1 in+care campaign webinar august 14, 2012. 2 ground rules for webinar participation actively...
TRANSCRIPT

1
in+care CampaignWebinar
August 14, 2012

2
Ground Rules for Webinar Participation
• Actively participate and write your questions into the chat area during the presentation(s)
• Do not put us on hold• Mute your line if you are not speaking
(press *6, to unmute your line press #6)• Slides and other resources are available
on our website at incareCampaign.org• All webinars are being recorded

3
Agenda
• Welcome & Introductions, 5min• Substance Abuse and Retention, 30min• The UCSF Story, 10min• Data Review and Discussion of
Retention Strategies Collected Through the Campaign, 15min
• Q & A Session, 5min• Updates & Reminders, 5min

Strategies to Improve Health Outcomes and Treatment Retention
in HIV+ Substance Users
Chinazo Cunningham, MD, MS
Albert Einstein College of Medicine
Montefiore Medical Center

Objectives
• To review poor health outcomes observed in HIV+ substance users
• To examine treatment strategies aimed at improving health outcomes and treatment retention – Outreach
– Case management
– Integration of HIV & substance abuse treatment
– Support groups
– Patient navigation
– Harm reduction framework

National estimates of drug-related ED visits 2004-2010
SAMHSA, OAS, DAWN

Poor outcomes in HIV+ substance users
• Less access to care
• Less retention in care
• Less access to antiretroviral therapy (ART)
• Worse adherence to ART
• Slower decline in morbidity and mortality
Turner 2001; Kalichman 2002; Shapiro 1999; Celentano 1998; Strathdee 1998; Arnsten 2002; Tucker 2003; Golin 2002; Chesney 2000; Lucas 1999; Bouhnik 2002; Knowleton 2001; Chitwood 1999 & 2001; Cronquist 2001

Possible Reasons for Poor Health Outcomes
• Substance users:- Lack of trust in health care system
- Competing needs (housing, food, benefits, etc.)
- Co-morbid illnesses (mental illness, Hepatitis C, TB)
- Intermittent incarceration
• Providers:- Discrimination (substance use, race/ethnicity, poverty, HIV, homeless)
- Lack of education/training around substance use
• System:- Fragmented system addressing HIV & substance abuse separately
- Lack of support to address needs
- Lack of flexibility to address needs
- Philosophical framework not conducive to drug users

Strategies to Improve Health Outcomes & Treatment Retention
• Outreach
• Case management
• Integration of HIV & substance abuse treatment
• Support groups
• Patient navigation
• Harm reduction framework

Outreach
• Project Bridge – Intense CM for HIV+ recently released prisoners
– At 1 year, 82% were retained in HIV care
• Yale Community Health Care Van – Mobile van visiting needle exchange sites
– At 9 months, 77% with undetectable VL
• Montefiore/CitiWide Program – Doctors with outreach team targeting HIV+ SRO hotel residents
– After outreach, regular HIV care provider and taking ART
• HRSA multi-site outreach initiative # of outreach visits associated with gap in HIV care
Rich 2001; Cunningham 2005; Altice 2003; Cabral 2007

Case Management• One of the most widely used services in HIV programs• Lack of uniform definition of CM• Studies examining CM
– Several observational studies examine association between CM and HIV outcomes
• CM assoc with HIV health care utilization
• CM assoc with ART utilization and adherence
– Few RCTs of CM with conflicting findings• CM with drug users & non-users = HIV care utilization
• CM with drug users = no change in HIV care utilization
Katz 2001; Cunningham 2007; Kushel 2006; Lo 2002; Messeri 2002; Harris 2003; Gardner 2005 ; Sorenson 2003

Integration of HIV & SA Treatment
• Benefits of integration– Easier to access/utilize services
– SA treatment associated with positive HIV health outcomes
– Single health care provider can closely monitor and reduce risk of drug-drug interactions
– Likely more efficient and less costly
• 2 ways of integration– HIV treatment into SA treatment
– SA treatment into HIV treatment
Samet 2001

Integration of HIV treatment into SA treatment
• Several studies examined integration of HIV treatment into methadone programs– Feasible HIV care utilization high risk behavior opioid use– Improvement in education & employment
Selwyn 1993; Keen 2003; Samet 2001; Fiellin 2001; Novick 1988, 1993 & 1994; Salsitz 2000

Integration of SA treatment into HIV treatment
• Several studies examined buprenorphine treatment in HIV clinic
• HRSA multi-site study• Feasible opioid use HIV care utilization ART initiation VL, CD4 count
• International studies with consistent findings
O’Connor 1998 & 1996; Vignau; 2001 Fiellin 2002 & 2012; Sullivan 2006; Cunningham 2011; Altice 2012; Lucas 2010; Roux 2009

Support Groups
• Support groups are widely accepted to address needs of drug users not addressed elsewhere
• Few studies explicitly examine support groups– Attending support groups associated with:
utilization ART utilization HIV care services
Kang 2006; Cunningham 2008

Patient Navigation
• Patient navigation = emerging strategy to improve outcomes of marginalized HIV+ individuals
• Few studies have examined patient navigation• Evaluation pooling data from 4 “navigation-like”
programs– Blend of CM, care coordination, accompaniment to appts
– Patients who received navigation (vs. no navigation) HIV care utilization VL
Bradford 2007

Harm Reduction
• Principles:– minimize harmful effects of drugs
– some ways of using drugs are safer than others
– success not necessarily cessation of drug use
– non-judgmental, low threshold services
– “meet drug users where they are at”

Harm Reduction
• System approach– Flexibility in appointments– Missed and “walk-in” appointments– Wait times (in person, by phone)
• Individual approach

The reality of caring for HIV+ substance users
• Difficult and challenging work, yet can be very gratifying
• Time and PATIENCE
• Acknowledge own judgments, personal beliefs
• TRUST is critical
• Addressing the “hidden agenda”

Harm Reduction Treatment
• Shift in traditional philosophy
• Take several steps back and assess harms
• Patient vs. provider agenda
• Concrete actions – Prescriptions for syringes
– Refer for case management
– Redefine health, goals, and success/failure

Redefine Health• Health is NOT the absence of disease
• Biopsychosocial model AND…– drugs – housing– support system – finances – violence – criminal justice issues…
• Life priorities of HIV+ IDUs– Only 37% ranked HIV as most important– Top priorities: housing, money, safety from violence
Mizuno 2003

Redefine Success
• Success is NOT just: – Undetectable viral load– Abstinence from drug use
• Success also includes:– Making it to appointments– Preventative care (PAP smears, OI prophylaxis, PPD)
– Less, safer, more controlled drug use– Improvement in non-medical areas (housing, support
system, criminal activity, etc.)

Why Adopt a Different Definition of Success?
• Recognizes that success is not only about taking medications
• Actively engages patients in health care and treatment• Values the health impacts of “non-medical”
interventions (e.g. controlled drug use, stable housing, social supports)
• Improves patients’ self-efficacy • Provides more opportunities for success
Conclusion
• Reviewed poor outcomes in HIV+ substance users
• Examined treatment strategies improve health outcomes and treatment retention – Outreach
– Case management
– Integration of HIV & substance abuse treatment
– Support groups
– Patient navigation
– Harm reduction framework

Support for Drug Users
Jacqueline Tulsky M.D.Professor of Medicine, UCSF/SFGH
Positive Health ProgramSF AETC

26
A Perspective on Addiction
“Most of us walk unseeing through the world, unaware alike of its beauties, its wonders and the strange and sometimes terrible intensity of the lives being lived about us.”
Rachel Carson (1907-1964)

27
“Gaining some control”
34 yo man opioid addicted in jail Frequent in and out, but during longer
stay is approached by targeted testing project and found HIV+, CD4 110.
Referred to methadone at release, but comes 3 days later. No slot that day, told to come back next day
Disappears and arrested 3 weeks later.

28

29
Continued -2
This time, HIV specialist in jail contacted us at the methadone program
Could we do intake while in jail and start patient on methadone?
Sheriff agreed, methadone agreed – pt started while in jail on 30mg methadone

30
Continued -3 On release, pt came to methadone next
day where methadone dose confirmed with jail and increased slowly
Referred to HIV primary care clinic in the methadone clinic who used Motivational Interviewing, social worker, drug counselor for ADAP, food, housing and support
Over 3 months, stabilized on methadone, identified cocaine as problem and wanted HIV treatment
31
Continued -4 Back in jail one more time, but
continued methadone through their program. Start HIV ART medications.
Arranged inclusion in methadone DOT program for HIV meds at when released from jail.
2 years later still struggles with cocaine, but no further jail stays, off street opioids, undetectable viral load.

32
Lessons Learned
Multi modality for true recovery in most complex pts (addiction/medical/social)
They can’t do it alone, and neither can you
Motivational Interviewing was very useful in identifying (and creating) the patient’s priorities

33
Lessons Learned
Connections between and across programs and providers are underutilized and often the only barrier is the lack of imagination, communication and persistence


35
Improvement Strategies Exercise
Michael Hager, MPH MANQC Manager

36
in+care Campaign National Data Snapshot
December – June Data as of 07/31/2012
Dec Average
(Patients)
Dec Sites
Feb Average
(Patients)
Feb Sites
Apr Average
(Patients)
Apr Sites
Jun Average
(Patients)
Jun Sites
Measure 1: Gap Measure 16.00% (122,473) 200 15.88%
(123,949) 191 14.74% (125,056) 197 15.33%
(106,837) 167
Measure 2: Visit Frequency Measure
64.40% (83,647) 151 65.47%
(83,996) 147 61.91% (99,496) 170 63.63%
(85,825) 154
Measure 3: New Patient Measure
57.23% (7,859) 190 58.19%
(8,641) 183 58.72% (8,227) 188 59.79%
(6,899) 163
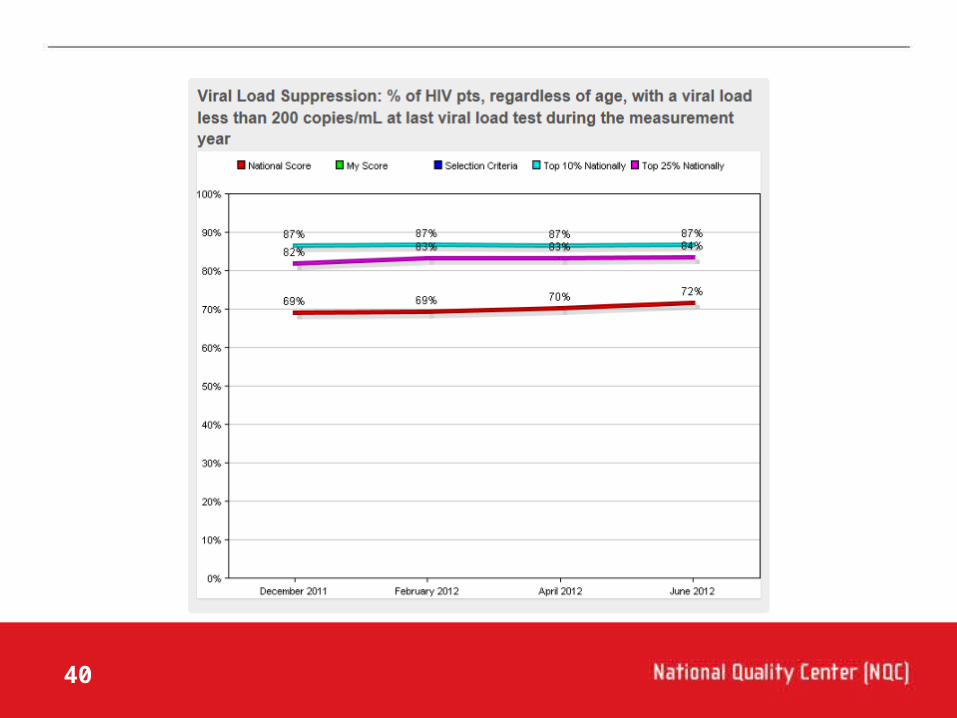
Measure 4: Viral Suppression Measure
69.14% (132,539) 192 69.39%
(143,625) 185 70.31% (148,134) 190 71.80%
(130,584) 168
Coming Soon – new analyses!

37

38

39
40

41
New Way to Submit Improvement Updates!

42
Improvement Update Discussion
A) Interventions Related to Substance Abuse• Patient navigation services• Van services to pick up and drop off patients where they
are (can be non-HIV specific to reduce stigma)• Health van services to treat patients where they are• Flexible appointment times or same day appointments• Case consultation at provider meetings• Interdisciplinary teams• Target substance abusing patients issues for intensive
reminders• Mention substance abusing patients in QM Plan – make
a program priority to address these needs

43
Improvement Update Discussion
B) Barriers Related to Substance Abuse• Health is often a lower priority for substance abusers• Can be difficult to communicate with patients• Very high no-show risk for on site appointments• Lots of supports are needed for these patients• Silo-ed funding streams for HIV and substance abuse
treatment• Patients often missing eligibility determination
paperwork• Intermittent incarceration makes finding patients
challenging• Declining local resources for substance abuse treatment

44
Improvement Update Discussion
C) Lessons Learned Related to Substance Abuse• Screen, screen, screen for substance abuse and relapse• Providing transportation for patients OR doctors to
improve patient access to care• Relying on community partnerships to bolster efforts• Relying on peers or someone relatable (navigator) to
slowly link patients into consistent HIV care• Working with Local/Regional Departments of Health to
create communities of learning and working groups• Tiered approach to outreach intensity based on
demonstrated patient need

45
Time for Questions and Answers

46
MedScape Retention in HIV Care Series
• Technical Working Group working on articles for a new Medscape Today News Series.
• Bruce Agins, MD MPH, New York State Department of Health AIDS Institute Medical Director, wrote the opening article in the series
• We recommend that you subscribe to HIV/AIDS MedPlus to be informed of new and exciting articles in this series!
• http://www.medscape.com/viewarticle/768102

47
Partners in+care
• Partners in+care Private Facebook Group is live! • Share tips, stories and strategies• Join a community of PLWH and those who love them• Email [email protected] for more
details
• Partners in+care website is live!• http://www.incarecampaign.net/index.cfm/77453 • Join our mailing list (a list-serv version of the FB
Group)

48
• Campaign Office Hours: Mondays & Wednesdays 4-5pm ET
• Data Collection Submission Deadline: August 1, 2012
• Next Campaign Webinar: Identifying Attrition Risk Patients To be announced
• Next Meet-the-Author Webinar: To be announced
• Next Partners in+care Webinar: To be announced
Upcoming Events and Deadlines

49
Campaign Headquarters:National Quality Center (NQC)90 Church Street, 13th floorNew York, NY 10007Phone [email protected]
incareCampaign.orgyoutube.com/incareCampaign