1 introduction making musculoskeletal diagnosis v3
Upload: department-of-anesthesiology-faculty-of-medicine-hasanuddin-university
Post on 23-Jan-2018
17 views
TRANSCRIPT
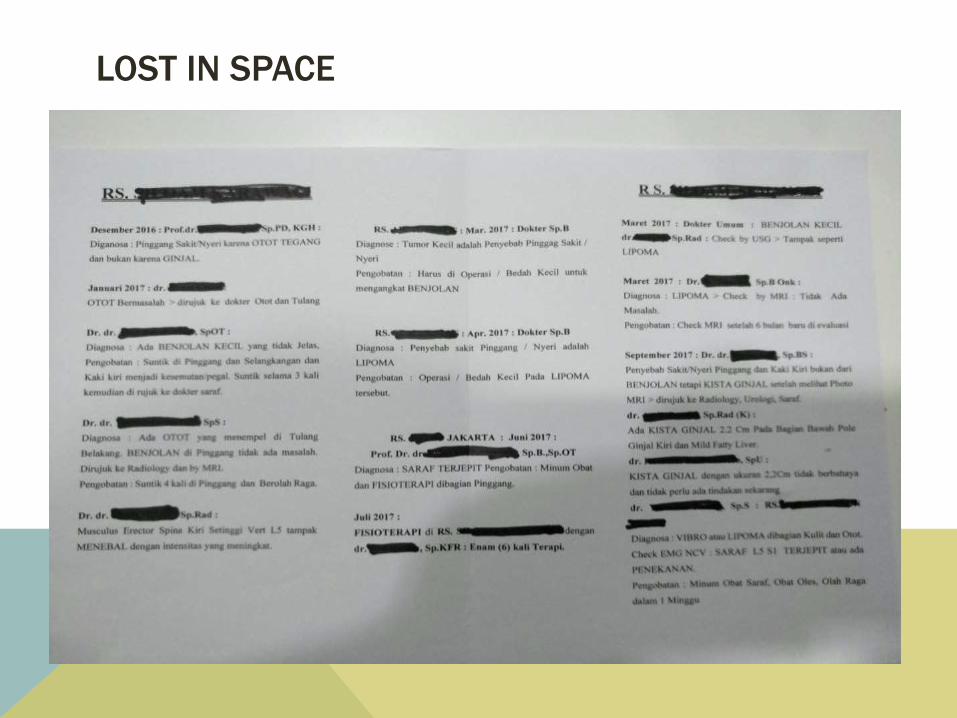
LOST IN SPACE
When thoughts become silent,
The soul finds peace...
In it’s own source
I N T R O D U C T I O N
• Pain medicine
relieving pain
• Diagnosis based
care
H I S T O R Y
TA K I N G
• Adequate time
• Listen carefully
• Empathetic
• Trust building
• Do not intervere
• Pschosocioeconomic & spiritual
codition
• - quantity: VAS
- quality: nociceptive
- mode of onset and location
- duration & chronicity
- provocating & relieving factors
- special character
- timing of pain
- relation with posture
- associated complaints
CONT..
Rule out red flags or warning signs: inf, trauma, tumor
Past history: DM, inflamatory disorder, op, trauma
Psychosocial assessment history: occupation, vocation, sos
economic status, depression, sleep habit
Family history: RA, FM
Treatment history
GENERAL EXAMINATION
Sign of distress: wincing, sweating, protecting
Facial appearance: anxious, depressed, moon face
Gait and posture: antalgic, trendelenburg, waddling, stooped
Mental status: orientation, calculation, memory, speech,
comprehension
Built, nutrition
State of clothing
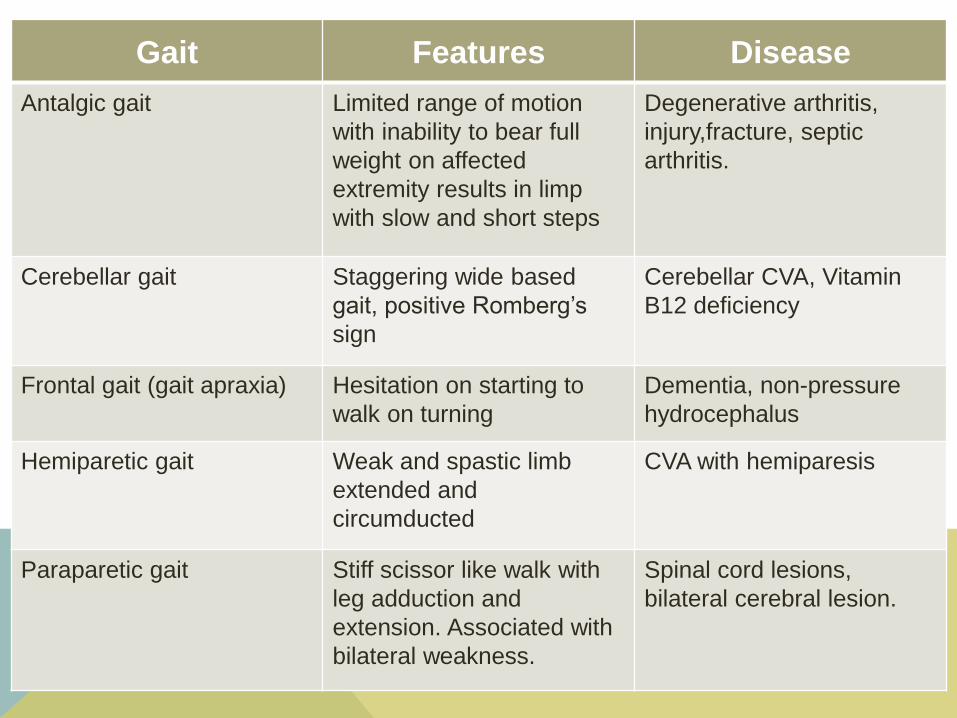
Gait Features Disease
Antalgic gait Limited range of motion
with inability to bear full
weight on affected
extremity results in limp
with slow and short steps
Degenerative arthritis,
injury,fracture, septic
arthritis.
Cerebellar gait Staggering wide based
gait, positive Romberg’s
sign
Cerebellar CVA, Vitamin
B12 deficiency
Frontal gait (gait apraxia) Hesitation on starting to
walk on turning
Dementia, non-pressure
hydrocephalus
Hemiparetic gait Weak and spastic limb
extended and
circumducted
CVA with hemiparesis
Paraparetic gait Stiff scissor like walk with
leg adduction and
extension. Associated with
bilateral weakness.
Spinal cord lesions,
bilateral cerebral lesion.
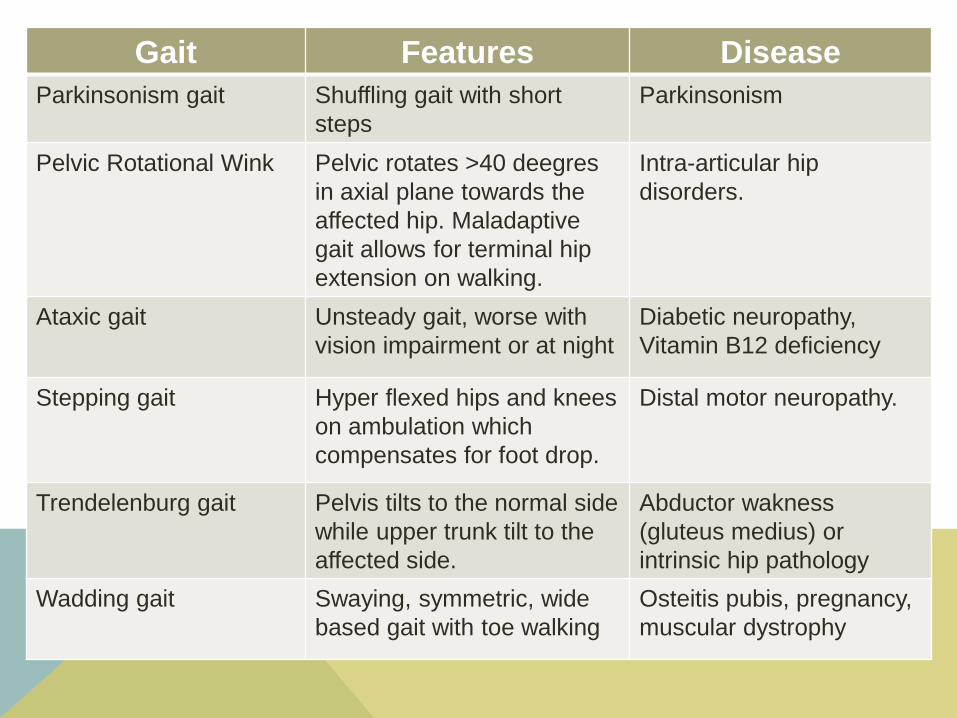
Gait Features Disease
Parkinsonism gait Shuffling gait with short
steps
Parkinsonism
Pelvic Rotational Wink Pelvic rotates >40 deegres
in axial plane towards the
affected hip. Maladaptive
gait allows for terminal hip
extension on walking.
Intra-articular hip
disorders.
Ataxic gait Unsteady gait, worse with
vision impairment or at night
Diabetic neuropathy,
Vitamin B12 deficiency
Stepping gait Hyper flexed hips and knees
on ambulation which
compensates for foot drop.
Distal motor neuropathy.
Trendelenburg gait Pelvis tilts to the normal side
while upper trunk tilt to the
affected side.
Abductor wakness
(gluteus medius) or
intrinsic hip pathology
Wadding gait Swaying, symmetric, wide
based gait with toe walking
Osteitis pubis, pregnancy,
muscular dystrophy
GENERAL EXAM CONT.
Vital signs incl pain
BH, BW, BMI (Normal 18-25)
Complete exam from head to toe if needed
Tender points
Extremities:
o Oedema:
o Swelling: heberdens node (DIP OA), Bouchard node (PIP
OA), Rheumatoid nodule
o Deformities: Swan neck, Buttonier def, ulnar dev, Dupuytren
contracture, trophic changes (ulcer, burn), genu valgus/varus
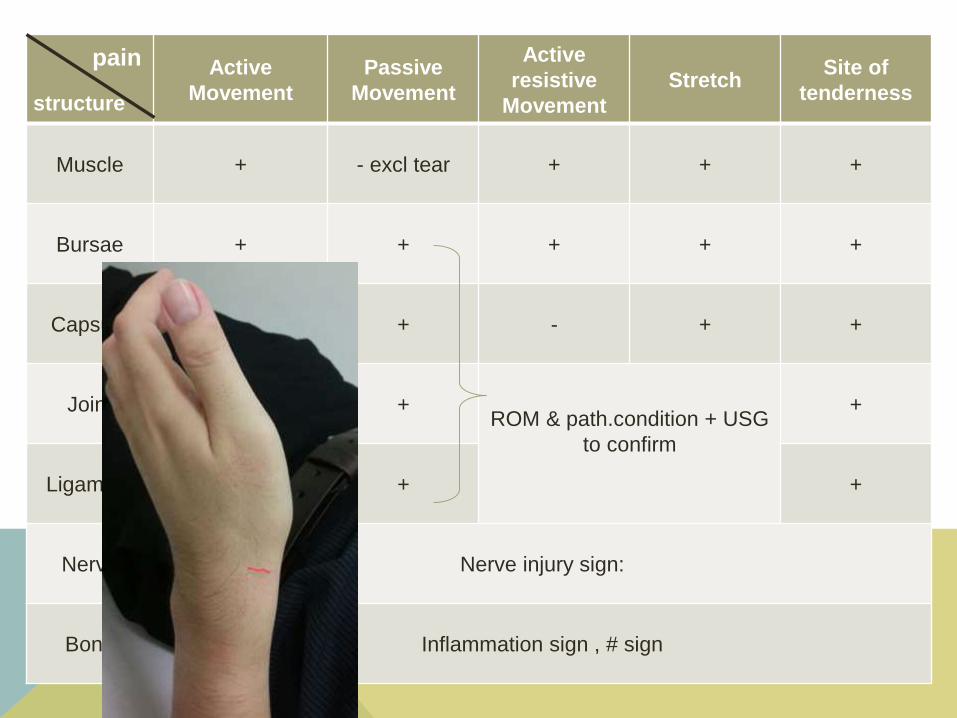
Active
Movement
Passive
Movement
Active
resistive
Movement
StretchSite of
tenderness
Muscle + - excl tear + + +
Bursae + + + + +
Capsule + + - + +
Joint + +ROM & path.condition + USG
to confirm
+
Ligament + + +
Nerve Nerve injury sign:
Bone Inflammation sign , # sign
pain
structure
SUPPORTING EXAMINATION
- USG
- Plain Radiograph
- MRI
DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
TREATMENT