1 tab bowel bladder mgm 06.08 - polaris groupstore.polaris-group.com/b&b toc 05.09.pdf · tab...
TRANSCRIPT

INDEX
TAB ONE Bowel and Bladder Management program
TAB TWO Sample forms
- Assessments - Voiding Patterns and Re-training tools - QA Tools
TAB THREE F-tag 315 Guidance to Surveyors and Investigative protocol.
Manual includes: Program CD –Bowel and Bladder Management --includes entire program, protocol, and forms.
PROCEDURES
How to use this manual: All systems and processes have key steps or components that are needed to achieve the desired outcome. For a clinical program, the desired outcomes include:
1. Compliance with regulations and best practices. 2. Provides for individualized assessment and care planning. 3. Monitors effectiveness of processes in achieving desired resident outcomes.
The QA Committee should review all outlined key components in this manual, then perform a gap analysis comparing current systems to recommended best practices recommended. Steps:
1. Evaluate current systems to key components outlined in this manual. 2. Define standards and key components for the health center. 3. Review F-tag 315 guidelines and protocols. Access clinical resources listed in guidance
as a resource for developing procedures. 4. Use text from the manual provided on CD to develop center specific procedures. 5. Finalize forms. 6. Provide education and training to staff. 7. Implement systems. 8. Develop ongoing QA to monitor effectiveness.
SAMPLE

Polaris Group (800) 275-6252 Page 1 of 2
BLADDER CONTINENCE ASSESSMENT
SEE INSTRUCTION ON BACK
RESIDENT: ROOM:
CRITERIA 0 1 2 3 SCORE
COGNITIVE STATUS
No LIMITATIONS Alert, oriented x3 decisions consistent and reasonable
SLIGHTLY IMPAIRED Occasional confusion; some difficulty in new situations only
MODERATERLY IMPAIRED Frequently confused and disoriented; decisions poor; requires cues and supervision
SEVERELY IMPAIRED Continual confusion; decisions never or rarely made/ also includes comatose resident
MEDICAL HISTORY * (over)
None 1 2 3 or more
MEDICATION HISTORY ** (over)
≤1 Group I No Group II, III
2 Group I; and/or 1 Group II; No Group III
3 Group I; and/or 2 Group II; and/or 1 Group III
>3 Group I; and/or ≤ 3 Group II; and/or ≤ 2 Group III
MOBILITY
INDEPENDENT Fully ambulatory; self-sufficiency once in W/C; able to transfer to and from toilet
LIMITED ASSISTANCE Ambulates with limited assistance (i.e. walker, cane) able to transfer to and from toilet with minimal assistance
EXTENSIVE ASSISTANCE Ambulates and transfers to and from toilet with moderate assistance
DEPENDENT Non weight bearing; unable to transfer without full staff assistance
BLADDER CONTROL STATUS
CONTINENT Aware of need to void; includes foley
USUALLY / OCCASIONAL Incontinent ≤ 1 per week; and/or ≤ 2 per week, but not daily
FREQUENTLY Daily incontinence, but some control present
INCONTINENT Inadequate control, multiple daily episodes
FLUID INTAKE GOOD ≤ 2000 cc daily
FAIR 1000 – 2000 cc daily
POOR 500 – 1000 cc daily
EXTREMELY POOR < 500 cc daily
TOTAL
DATE
0 – 3 = High restorative potential (retraining) 4 – 9 = Moderate restorative potential (habit/prompted) 10 – 14 =Low restorative potential (habit/prompted) 15 - 18 = Minimal restorative potential (Check Change)
INITIAL
INTL SIGNATURE INTL SIGNATURE INTL SIGNATURE
SAMPLE
Polaris Group (800) 275-6252 Page 2 of 2
COMPLETION OF THE BLADDER CONTINENCE ASSESSMENT
1. The licensed nurse will evaluate each resident for each of the six criteria, determine the description that most
closely approximates the condition of the resident, and record the numerical score in the scoring column at the far right.
2. Add the scores from the criteria and enter the total in the spaces provided to determine the nursing interventions for each resident.
3. The assessing nurse signs and dates the Bladder Continence Assessment. 4. Using the total score, implement the nursing interventions according to the scale listed.
0 – 3 = High restorative potential (retraining) 10 – 14 =Low restorative potential (habit/prompted) 4 – 9 = Moderate restorative potential (habit/prompted) 15 - 18 = Minimal restorative potential (CheckChange) 5. The Bladder Continence Assessment form should be placed in the medical record upon completion. * MEDICAL HISTORY: Refers to medical conditions that affect the restorative potential of the resident. Examples below are not all inclusive:
a. Cardiovascular - ASHD, CHF, Cardiac Dysrhythmia, HTN, PVD, CAD, Hypotension, Pacemaker b. Neurological - CVA, MS, CP, Huntington’s Chorea, Parkinson’s Disease, Peripheral Neuropathy,
Hemiplegia, Paraplegia, Quadriplegia, Hemiparesis, Seizure Disorder, Transient Ischemic Attach (TIA), Comatose, Aphasia
c. Musculoskeletal - Previous Fractures, Arthritis, Scoliosis, Pain, Skeletal Deformities, Kyphosis, Amputation (i.e. missing limb)
d. Pulmonary - Asthma, DOPD, Emphysema e. Sensor/Perceptual - Balance Abnormality, Dizziness, vertigo, Glaucoma, Cataracts, Blindness, Hearing Loss f. Cognitive - Alzheimer’s Disease, Dementia other than Alzheimer’s Disease g. Psychiatric - Depression, Anxiety Disorder, Manic Depressive (bipolar dx.) Psychosis, Neurosis h. Endocrine - Hypo/Hyperglycemia, Diabetes Mellitus, Hypo/Hyperthyroidism i. Genitourinary - Vitamin B12 Deficiency, High BUN or Creatinine, Atrophic Vaginitis, Rule Out UTI, Rule
Out Fecal Impaction, Rule Out Laxative Dependence, Cancer (i.e. Prostate), Hemorrhoids, Fissures/Fistulas, Rectal Bleeding
j. Other - Cancer (i.e. Brain), Explicit Terminal Prognosis ** MEDICATION HISTORY: refers to medications that affect the restorative potential of the resident. Review 24
hour regularly administered (scheduled & prn) medications. Examples below are not all inclusive:
GroupI a. Cardiac - Lanoxin, Inderal, Procardia, Calan, Nitrobid, Transderm-Nitro, Lopressor b. Antihypertensive/Diuretic - Lasix, capoten, Dyazide, HCTZ, Diuril, Catapres, Tenorectic c. Sedative/HypnoticsSedative - Restoril, Halcion, Dalmane, Benadryl Group II a. Antidepressants/Antianxiety –Valium, Librium, Sinequan, Elavil, Ativan, Desyrel, Xanax, Ludiomil,
Vistaril, Buspar b. Anticholingerics - Antivert, Dramamine, Compazine Group III a. Antipsychotic/Neuroleptics - Mellaril, Haldol, Stelazine, Thorazine, Prolixin, Trilaforn, Navane
b. Anticonvulsants/Neuromuscular – Phenobarbital, Artane, Dilantin, Moban, Tegretol, Depakene, Klonopin c. Anti-Parkinson - Levodopa, Sinemet, Eldepryl, Permax, Parlodel, Cogentin
SAMPLE

PRELIMINARY NURSING ASSESSMENT
RESIDENT:__________________________________ RM:_______MR#________ Page 1 of 4
Admit Date _____________ Admit time ______________ From _______________ Via __________________ Diagnosis __________________________________________ Allergies: ______________________________ T: ___________ P: ___________ R: ___________ BP: __________ HT: __________ WT: ______________ 1. COGNITIVE (CIRCLE) ALERT / ORIENTED TO: PERSON – PLACE – TIME MEMORY PROBLEMS / ACUTE CONFUSION /
LETHARGIC / SEMI COMATOSE / COMATOSE: DESCRIBE __________________________________________
CARE PLAN Y OR N 2. MOOD AND BEHAVIOR (CIRCLE)
ELOPEMENT POTENTIAL: Y or N __________________________ If yes, complete full Elopement Assessment tool
(Circle One) WITHDRAWN / PACING / VERBALLY ABUSIVE / CRYING / WEEPING / ANGRY / RESISTS CARE /
REPETITIVE BEHAVIORS / AGITATION/ OTHER: ____________________________________________________
CONDITION/DIAGNOSIS:_____________________________________________________CARE PLAN: Y OR N
RECEIVING: HYPNOTIC / ANTIPSYCHOTIC / ANTIANXIETY / ANTIDEPRESSANT: LIST MEDS: _______________________________________________________________________________________ If applies: BEHAVIOR MONITOR INITIATED: _____ REFERRED TO PHARMACY: _____ CONSENT SIGNED:_______SIDE EFFECT MON. STARTED:______ AIMS:__________ 3. COMMUNICATION (CIRCLE)
HOH / DEAF L R B HEARING AIDE L R B / OTHER:
COMMUNICATES: SPEECH / GESTURES / WRITES / OTHER APHASIC
CAN BE UNDERSTOOD Y OR N UNDERSTANDS Y OR N
CARE PLAN: Y OR N REFER TO THERAPY: Y OR N 4. VISION (CIRCLE)
ADEQUATE Y OR N GLASSES Y OR N BLIND Y OR N – L R B LENS IMPLANTS L R B
PROSTHESIS L R B GLAUCOMA / CATARACTS / FIELD CUT L R B CARE PLAN: Y OR N 5. PAIN (CIRCLE) VERBAL OR NONVERBAL EXPRESSION OF PAIN: PAIN: Yes No CARE PLAN Y OR N
COMPLETE PAIN SCREEN ON ALL RESIDENTS: IF SCORE IS GREATER THAN 3, COMPLETE FULL ASSESSMENT FORM.: Pain Screen Score: _______ Pain Scale: 1-10:_______
SAMPLE

Polaris Group (813) 886-6500 Page 1 of 1
ELIMINATION ASSESSMENT SUMMARY Summary of risk factors, environmental. Functional/adaptive device needs, & voiding pattern data: Bladder Risk Score: ___ Type of Incontinence: Urge___ Stress___ Mix___ Overflow___ Functional___ Other___ Unknown___
Implement Bladder or Bowel retraining program:
Implement Intermittent Catheterization: Implement [] Prompted [] Habit [] Scheduled toileting training program as the individualization scheduled toileting plan for:
Bladder Bowel OR Prior failed attempts at toileting schedules, implement Check and Change Describe toileting plan:
Remove Continue with Foley Catheter Justification: Infection Control in place: Fluid needs: Care Plan Completed
Assessment completed by: _________________________________________ Date_______________
ELIMINATION ASSESSMENT SUMMARY Summary of risk factors, environmental. Functional/adaptive device needs, & voiding pattern data: Bladder Risk Score:___ Type of Incontinence: Urge___ Stress___ Mix___ Overflow___ Functional___ Other___ Unknown___
Implement Bladder or Bowel retraining program:
Implement Intermittent Catheterization: Implement [] Prompted [] Habit [] Scheduled toileting training program as the individualization scheduled toileting plan for:
Bladder Bowel OR Prior failed attempts at toileting schedules, implement Check and Change Describe toileting plan:
Remove Continue with Foley Catheter - Justification: Infection Control in place: Fluid needs: Care Plan Completed
Assessment completed by: _________________________________________ Date_______________ Resident_______________________ Med Rec_______ Physician_______________ Rm_____________
SAMPLE

Resident: _____________________________________ MR#:_________ Rm #: ______ Page 2 of 3
1. INTIAL/QUARTERLY ELIMINATION ASSESSMENT SUMMARY Summary of risk factors, environmental. Functional/adaptive device needs, & voiding pattern data: Bladder Risk Score: ___ Type of Incontinence: Urge___ Stress___ Mix___ Overflow___ Functional___ Other___ Unknown___
Implement Bladder or Bowel retraining program:
Implement Intermittent Catheterization: Implement: [] Prompted [ ] Habit [] Scheduled toileting plan: Bladder Bowel Both Prior failed attempts at toileting schedules, implement Check and Change Describe plan:
Remove Continue with Foley Catheter Diagnosis: Infection Control precautions in place: Special Fluid needs: Care Plan revised/updated/current
Assessment completed by: _______________________________________ Date_______________
2. QUARTERLY ELIMINATION ASSESSMENT SUMMARY Summary of risk factors, environmental. Functional/adaptive device needs, & voiding pattern data: Bladder Risk Score: ___ Type of Incontinence: Urge___ Stress___ Mix___ Overflow___ Functional___ Other___ Unknown___
Implement Bladder or Bowel retraining program:
Implement Intermittent Catheterization: Implement: [] Prompted [ ] Habit [] Scheduled toileting plan: Bladder Bowel Both Prior failed attempts at toileting schedules, implement Check and Change Describe plan:
Remove Continue with Foley Catheter Diagnosis: Infection Control precautions in place: Special Fluid needs: Care Plan revised/updated/current
Assessment completed by: _______________________________________ Date_______________
SAMPLE

Page 1 of 2 CONTINENCE & CATHETER ASSESSMENT & RAP
FACTORS POTENTIALLY related to CONTINENCE STATUS Bowel and Bladder Risk Score: _______________________________________ (Complete as part of RAI process and after Voiding Pattern Data Collection has occurred)
Current DIAGNOSES Indicate MEDICATIONS currently taking: Antibiotics Disopyramide Diuretics Calcium channel blockers Antipsychotics Admit date:
Antianxiety Antispasmodics History of: Antidepressants Antihistamines
Urinary disorders Bladder disorders Kidney disease Edema Hypnotics Narcotics Prostate Problems Neurological problems U.T.I. Parkinsonism Antacids Other (describe) Pain Abnormal labs Drugs that stimulate or
block sympathetic nervous system
Stool softeners/laxatives Antidiarrheals
BOWEL ASSESSMENT (Complete at end of 3-day observation period) CONTINENT of STOOL: Yes No If incontinent: How long has resident been incontinent? _______________ Days Months Years Reason identified, if known: ___________________________________________________ Frequency of incontinence: Less than weekly Once a week 2-3 times a week All (or almost all) the time USUAL ELIMINATION PATTERN: Frequency: _______________________________________________ Time(s) of Day: Upon rising After meal(s): Bkfst Lunch Dinner No apparent pattern Other (describe): __________________________________________________ Amount: Small Med. Large Other: _________________ Perception of need to evacuate: Present Diminished Absent Prompting method: ________________________________________________________ History of impactions: No Yes, freq: ___________________ ________________________________________________________ Results of 3-day Observation: ________ % Continent Pattern: _________________________________________________ ________________________________________________________ ________________________________________________________
USUAL CONSISTENCY: Consistency: Hard Formed Soft Liquid Other: ____________ Color: Tarry Light/Medium Dark Brown Clay Other: _________ Flatulence: If known, caused by: ____________________________________________ Other (describe): _________________________________________________ Comments: _______________________________________________________________ ADDITIONAL PHYSICAL SYMPTOMS/PROBLEMS: Bowel Sounds: ________________________________________________ Comments: _____________________________________________________ ELIMINATION ASSISTS: None used Stool softeners, name, dose, freq: _________________________________ Laxatives, name, dose, freq: _____________________________________ Enemas, type, amount, freq: _____________________________________ Suppositories, type, amount, freq: ________________________________ Juice/Fiber, type, freq:__________________________________________ Comments: ______________________________________________________________ EXERCISE PATTERNS: Describe usual daily activities: _____________________________________ Is resident capable of increasing? Yes No, describe: ______________________________________________________________ Comments: ______________________________________________________________ ______________________________________________________________
Resident Name ID#
Room # Physician
No impairments impacting ability to toilet
Impaired physical ability to use: toilet commode bedpan/urinal call light Due to decline in: ROM transferability ambulation balance Fx cast bed mobility use of restraints
need for adaptive device lighting difficulty removing clothes
Impaired cognitive ability to use: toilet commode bedpan/urinal call light
Due to decline in: impaired memory comatose resistive to care
refusal of care inability to remember toileting tasks
Impaired sensory ability to use: toilet commode bedpan/urinal call light Due to decline in: vision blind hearing aphasic decline in communication skills
Environmental factors: location of toilet lighting location of commode
See RD Assessment regarding diet, fiber, fluid needs._______________________________________________________________________________
SAMPLE

Polaris Group (813) 886-6500 Page 1 of 1
FOLEY CATHETER ASSESSMENT AND MANAGEMENT
A resident is not to be catheterized unless his/her clinical condition demonstrated that catheterization was necessary. An indwelling catheter should only be used when there is a valid medical justification. In order to assess the need for catheterization the following questions need to be answered:
Y (Yes)
N (No)
Does the resident have a valid medical justification (supporting diagnosis) for use of the indwelling catheter? List:___________________________________________________
Does the resident have documented urinary retention that cannot be treated or corrected medically or surgically, for which alternative therapy is not feasible characterized by:
[ ] Documented post void residual (PVR) volumes in a range over 200ml. [ ] Inability to manage the retention/incontinence with intermittent catherization; and [ ] Persistent overflow incontinence, symptomatic infections, and/or renal dysfunction
Does the resident have supporting diagnostic testing or unsuccessful catheter-free trials documented?
Does the resident have contamination of Stage 3 or 4 pressure ulcer with urine which has impeded healing, despite appropriate personal care for the incontinence?
Does the resident have a terminal illness or severe impairment, which makes positioning or clothing changes uncomfortable or which is associated with intractable pain?
If any of the above questions in this section are answered “yes”, then indwelling catheterization may be medically necessary if benefits outweigh risks. Re-evaluation should occur at least quarterly or at time of a symptomatic UTI.
Catheter size: _____
Check the following practices: Y
(Yes) N
(No) Is the staff following the facility’s protocol and/or written procedures for catheterization? Do all personnel wash their hands before and after caring for the catheter/tubing/collecting bag ?
Is staff securing catheter to minimize injury and positioning bag to decrease risk of infection?
Is staff cleaning the catheter and providing bowel care per protocol? Fluid Needs addressed and met?
SUMMARY: [ ] Remove catheter and initiate bladder program [ ] Continue indwelling catheter _____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ RESIDENT: ______________________________________________________ ROOM: _______________ SIGNATURE: _____________________________________________________ DATE: _______________
SAMPLE
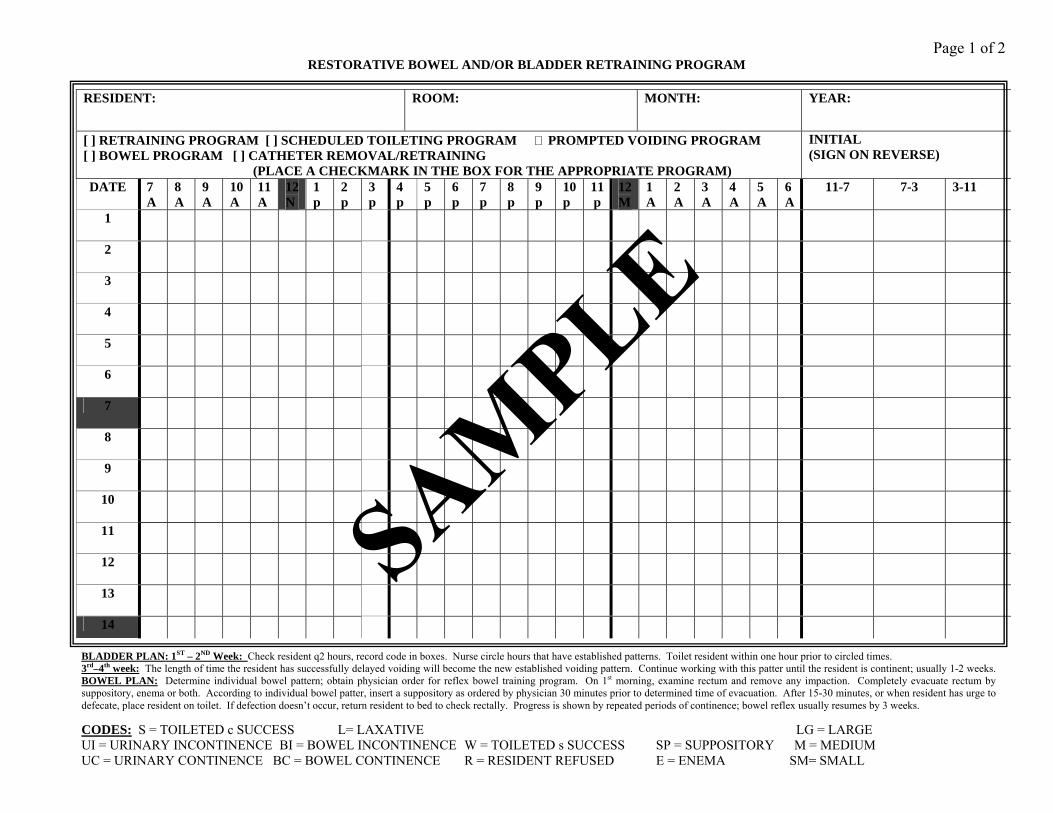
Page 1 of 2 RESTORATIVE BOWEL AND/OR BLADDER RETRAINING PROGRAM
BLADDER PLAN: 1ST – 2ND Week: Check resident q2 hours, record code in boxes. Nurse circle hours that have established patterns. Toilet resident within one hour prior to circled times. 3rd–4th week: The length of time the resident has successfully delayed voiding will become the new established voiding pattern. Continue working with this patter until the resident is continent; usually 1-2 weeks. BOWEL PLAN: Determine individual bowel pattern; obtain physician order for reflex bowel training program. On 1st morning, examine rectum and remove any impaction. Completely evacuate rectum by suppository, enema or both. According to individual bowel patter, insert a suppository as ordered by physician 30 minutes prior to determined time of evacuation. After 15-30 minutes, or when resident has urge to defecate, place resident on toilet. If defection doesn’t occur, return resident to bed to check rectally. Progress is shown by repeated periods of continence; bowel reflex usually resumes by 3 weeks.
CODES: S = TOILETED c SUCCESS L= LAXATIVE LG = LARGE UI = URINARY INCONTINENCE BI = BOWEL INCONTINENCE W = TOILETED s SUCCESS SP = SUPPOSITORY M = MEDIUM UC = URINARY CONTINENCE BC = BOWEL CONTINENCE R = RESIDENT REFUSED E = ENEMA SM= SMALL
RESIDENT: ROOM: MONTH: YEAR:
[ ] RETRAINING PROGRAM [ ] SCHEDULED TOILETING PROGRAM PROMPTED VOIDING PROGRAM [ ] BOWEL PROGRAM [ ] CATHETER REMOVAL/RETRAINING (PLACE A CHECKMARK IN THE BOX FOR THE APPROPRIATE PROGRAM)
INITIAL (SIGN ON REVERSE)
DATE 7A
8A
9A
10A
11A
12 N
1p
2p
3p
4p
5p
6p
7p
8p
9p
10p
11p
12M
1A
2A
3A
4A
5A
6A
11-7 7-3 3-11
1
2
3
4
5
6
7
8
9
10
11
12
13
14
SAMPLE
Polaris Group (813) 886-6500 Page 1 of 1
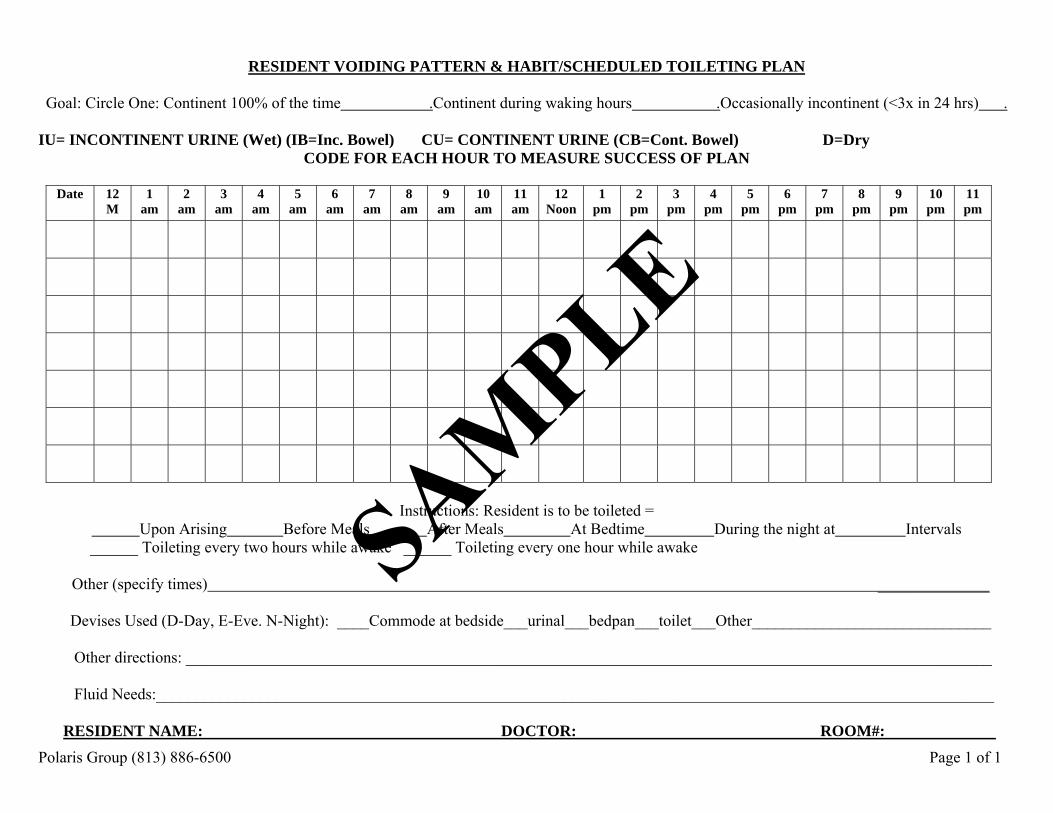
RESIDENT VOIDING PATTERN & HABIT/SCHEDULED TOILETING PLAN
Goal: Circle One: Continent 100% of the time .Continent during waking hours .Occasionally incontinent (<3x in 24 hrs) .
IU= INCONTINENT URINE (Wet) (IB=Inc. Bowel) CU= CONTINENT URINE (CB=Cont. Bowel) D=Dry
CODE FOR EACH HOUR TO MEASURE SUCCESS OF PLAN
Date 12 M
1 am
2 am
3 am
4 am
5 am
6 am
7 am
8 am
9 am
10 am
11 am
12 Noon
1 pm
2 pm
3 pm
4 pm
5 pm
6 pm
7 pm
8 pm
9 pm
10 pm
11 pm
Instructions: Resident is to be toileted =
Upon Arising Before Meals After Meals At Bedtime During the night at Intervals ______ Toileting every two hours while awake ______ Toileting every one hour while awake
Other (specify times) ______________
Devises Used (D-Day, E-Eve. N-Night): ____Commode at bedside___urinal___bedpan___toilet___Other______________________________ Other directions: _____________________________________________________________________________________________________ Fluid Needs:_________________________________________________________________________________________________________
RESIDENT NAME: DOCTOR: ROOM#:
SAMPLE

Polaris Group (813) 886-6500 Page 1 of 2
BLADDER RETRAINING FLOWSHEET Residents Name: Room#: MR#:
WEEK ONE: Record date. Initial in the appropriate box for each shift. Enter the code from the bottom in the box for the applicable time which best applies. Comments/Progress: Date/ Init 7-3 3-11 11-7 7
am 8
am 9
am 10 am
11 am
12 pm
1 pm
2 pm
3 pm
4 pm
5 pm
6 pm
7 pm
8 pm
9 pm
10 pm
11 pm
12 am
1 am
2 am 3 am 4
am 5 am 6 am
WEEK Two: Record date. Initial in the appropriate box for each shift. Enter the code from the bottom in the box for the applicable time which best applies. Comments/Progress: Date/Init 7-3 3-11 11-7 7
am 8
am 9
am 10 am
11 am
12 pm
1 pm
2 pm
3 pm
4 pm
5 pm
6 pm
7 pm
8 pm
9 pm
10 pm
11 pm
12 am
1 am
2 am
3 am
4 am
5 am
6 am
CODES: U Episode of urinary incontinence A Assisted to toilet with result C Resident found to be clean/dry N Resident not cooperative B Episode of bowel incontinence W Assisted to toilet without result T Toileted self/continent O Assisted to toilet with incontinent episodes
SAMPLE

QA SCREEN
Prevalence of Indwelling Catheter
Polaris Group (813) 886-6500 Page 1 of 1
Threshold = 90% or greater Directions: Audit 100% of residents with Prevalence of Indwelling Catheter if flagged at the 90th % or greater.
Y or X = Met NA = Not Applicable
Medical Record/Room Number Criteria/Questions
Comments
1. MDS items that trigger QI and risk status are accurate for observation period
2. Bowel and Bladder Assessment (RAP) upon admission, quarterly, and at time of change
3. Bladder and bowel patterns collected for three days upon admission and at time of decline in continence
4. Toileting plan documented: 1) Bladder/Bowel Retraining, 2) Scheduled Toileting,
3) Attends/diapers only, 4) Indwelling Catheter
5. Care plan addresses fluid needs and bowel routine as indicated
6. Care Plan addresses catheter care per facility policy
7. Observe provision of catheter care; infection control practices followed during care
8. Positioning of catheter in bed or chair maintains infection control best practices
9. Catheter and bag are covered to protect privacy per facility policy
Indwelling Catheter: Documentation supports continued use of Indwelling catheter An indwelling catheter must be justified per regulations F315: 1. Urinary Retention that a) is causing persistent overflow
incontinence, symptomatic infections, and/or renal dysfunction, b) Cannot be corrected surgically, c) Cannot be managed practically with intermittent catheter use.
2. Skin wounds, pressure sores or irritations that are being contaminated by urine
3. Terminal illness or severe impairment, which makes bed and clothing changes uncomfortable or disruptive.
SYSTEM: QIs printed out monthly; review and investigate if flagged at the 90th % or greater
Percentage of Compliance = # of Yes responses x100 Assessor: Total #of blocks: )the # of audits x’s the # of questions-exclude System and NA questions) Threshold Reached: Yes No
Percentage of Compliance (# yes divided by # blocks = % compliance)
Completed By: Title: Date:
SAMPLE