1 using evidence based interventions stephen brazill, ma, mac
TRANSCRIPT
1
Using Evidence Based
Interventions
Stephen Brazill, MA, MAC
Agenda
Brief History Some things about research EBTs Implementation Resources
2

3
History
Where Have We Been?
4
History
Mid 1930s Alcoholics Anonymous
1950s Narcotics Anonymous
The 1970s Hughes Act Research was scarce Knowledge mostly folk science For severe and chronic clients
5
History
1980s Drug Free Workplace Act EAPs Inpatient centers grew and prospered
1990s Institute of Medicine report Disconnect between research and
practice Bridging the Gap

6
Today
Building the bridge Evidence-based treatments Outpatient treatment Continuum of addictive behaviors
None Mild Moderate Severe
7
Now and Future
Ongoing research in academic and community settings
Improving dissemination of innovation
Improving implementation of evidence-based treatments
Client driven Outcome driven Maintenance vs. acute model
8
Now and Future Increased intervention via non-
specialist systems Health systems Social systems
The barber shop? Dentist? Religious communities Schools systems
New(er) Delivery systems Internet (meetings, chat room, Second
Life, etc.) Cell phone
9
Does Treatment Work?
Wrong
Questi
on
10
What Treatments Work?
11
What Does “Work” Mean?
Abstinence? Reduced use? Reduced psychiatric problems? Reduced incarceration? Increased employment? Reduced medical problems? Improved family functioning?
12
What Treatments Work?
For what clients?At what time?
Delivered by who?
13
How Do We Tell If Treatments
Work?
14
Levels of Evidence
Randomized clinical trials Quasi-experimental studies Correlational studies Anecdotal case reports, professional
opinion, best practice guidelines developed by consensus
15
Research Definitions
Efficacy Effectiveness
16
Problems With Research
Uni-directional Chosen by researchers Controlled settings Specific populations Individual counseling
17
Problems With Research
Training (cost, time, follow-through, drift)
Dissemination Less than 50% of programs are using
proven psychosocial interventions 10-17 years for dissemination
18
Solutions
Practice to research Clinical Trials Network Outcome research in community
programs Leadership focus on evidence-based
program development and training
19
How Research Helps Us Help
Others

20
What Research Does For Us
Helps clarify, guide and inform practice
Answers questions Improves outcomes Helps correct for human self-
deception “Addictive personality” Confrontation Victim impact panels
21
What Research Does For Us
Dispels myths such as…… Nothing works One approach is superior to another Everything works equally well
22
Why Use Evidence-Based Treatments?
Ethical and humanitarian considerations
Public interest and moral obligation Particularly when treatment is
coerced
23
Absence of Studies Does Not
Mean That a Treatment Does
Not Work
24
Respect Research, But
Do Not Revere It

EBTs Vs. EBP
Evidence Based Treatment Motivational Interviewing
Evidenced Based Practice Allowing mothers to take kids with
them to treatment Hiring empathic counselors
25

26
A Brief Review of Some Research
Findings
27
Miller & Hester 1995: Alcohol
Top Brief intervention Social skills training Motivational enhancement Community reinforcement approach Behavior contracting
Bottom Relaxation training Confrontation Psychotherapy General alcoholism counseling Education

28
Miller & Hester 2003: Alcohol (adapted post
COMBINE)Top
Brief intervention Motivational enhancement Community reinforcement approach Self-change manual Opiate Antagonists (Naltrexone) BSCT
Bottom Relaxation training Confrontation Psychotherapy General alcoholism counseling Education
29
Miller, Zweben & Johnson 2005
Cognitive-behavioral treatment Community reinforcement approach Motivational interviewing Relapse prevention Social skills training
JSAT 29 (2005)

30
Overview of Treatment Methods
Build client motivation, readiness and engage
Cognitive and behavior skills Increasing positive rewards for non-
use Involve family and social networks
Think outside the skin Appropriate medications
A Resource
Understanding Research Concepts: A Guide for Counselors
http://www.danya.com/dlc/courselist.asp
31
Building Motivation, Readiness,Engaging
32
33
Important Client Factors
Goals Values Experiences Expectations Strengths Cultural, ethnic and spiritual
background Biology Motivation & readiness
Assessi
ng and
Utilizin
g
34
Stages of Change
Precontemplation Contemplation Preparation Action Maintenance
Prochaska, Norcross, DiClemente
Relapse
35
Stages of Change
80% of substance abusers are in precontemplation or contemplation
Define success by the movement from one stage to the next

36
Predicting Change
in Clients

37
Predicting Change
Adherence to change efforts Self-efficacy Self-reported motivation Engagement and retention Quality of counseling relationship Client speech
38
Counselors and Helpers
39
HARPWhat We Believe and Do Matters
40
Building Motivation
41
Influencing Motivation:What Doesn’t Work
Enlightenment Education Insight-oriented persuasion
Confrontation Punishment
42
Building Motivation:What Works
43
Helper Traits That Help...…
A Lot Accurate empathy Genuine Unconditional positive regard
44
Appears that the counselor to whom one is assigned makes considerably more difference than the specific treatment employed*
*Najavits & Weiss, 1994
45
Interpersonal Influence
Referral from your office 2X Call or handwritten note 2X Missed session/letter ½
drop out AA w/member support 100% AC reminder calls/calendar 2X
46
Motivation
Is not a static client trait Affected greatly by relationship with
counselor It is interpersonal Measured by client language and
observed behavior

47
Change Talk
D = Desire for Change (want, wish, like) A = Ability to Change (could, can) R = Reasons for Change (if……then…..) N = Need for Change (need, have to, got to)
C = Commitment to Change (intention, decision)A = Activation (ready, prepared, willing)T = Taking Steps (tossed out cigarettes)
Motivational Interviewing Is…..
Motivational interviewing is a collaborative, person-centered, form of guiding
to elicit and strengthen motivation for change
Miller & Rollnick (2009)
Motivational Interviewing
Helps increase client change and commitment talk
Helps reduce resistance Helps engage clients Plays well with other treatments
Synergistic effects
50
Community Reinforcement Approach
52
Community Reinforcement Approach
(CRA) Broad spectrum behavioral
treatment Creating ways to reward sober
behavior Positive reinforcement
Utilizing social, recreational, familial and vocational reinforcers
Changing the person’s sources of reinforcement in the community
CRA Components
Job Finding Behavioral marital
therapy Social/leisure
counseling Social club Medication Problem-solving Sober buddy
system
Motivational counseling
Sobriety sampling Drink refusal Immediate
disulfiram administration
Relaxation training
53
54
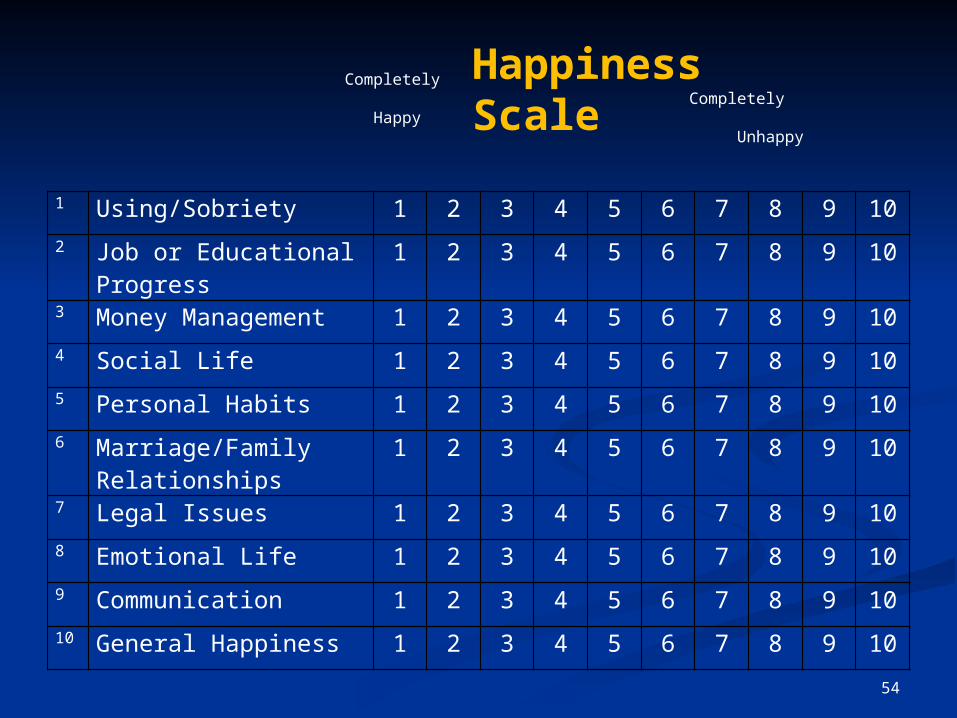
1 Using/Sobriety 1 2 3 4 5 6 7 8 9 10
2 Job or Educational Progress 1 2 3 4 5 6 7 8 9 10
3 Money Management 1 2 3 4 5 6 7 8 9 10
4 Social Life 1 2 3 4 5 6 7 8 9 10
5 Personal Habits 1 2 3 4 5 6 7 8 9 10
6 Marriage/Family Relationships
1 2 3 4 5 6 7 8 9 10
7 Legal Issues 1 2 3 4 5 6 7 8 9 10
8 Emotional Life 1 2 3 4 5 6 7 8 9 10
9 Communication 1 2 3 4 5 6 7 8 9 10
10 General Happiness 1 2 3 4 5 6 7 8 9 10
Completely Completely Happy Unhappy
Happiness Scale

55
Thinking Outside
The Skin
56
Systemic View For every individual with an alcohol
problems, 5 others suffer directly Violence & verbal aggression Unpredictable & embarrassing
behavior Stealing from family Depressed mood, lowered self-
confidence Physical complaints
57
Motivation Individuals with substance abuse
problems often report that their decision to enter treatment was prompted by direct influence of CSOs or CSOs acting in concert with others
Success rates for treatment entry when CSOs are directed by professionals:
24% to 86%

Community Reinforcement and Family Training: CRAFT

59
Community Reinforcement and
Family Training (CRAFT) Outgrowth of CRA Assumes that CSOs can play a
powerful role in effecting change Does not assume that CSOs are
responsible for use’s behavior CSOs can benefit from assistance in
learning to take better care of themselves
60
Unique Components
Emphasis on safety issues Reliance on functional analysis Identifying and utilizing reinforcers
for both the drinker and CSO Emphasis on personal lifestyle
changes Skills training from CRA
61
The Other Benefits
CRAFT-trained CSO functioning from baseline to 3 months showed decreased: anger anxiety depression
Regardless of whether or not the substance user had entered treatment
62
CRAFT Procedures
Domestic violence precautions Functional analysis Communication training Use of positive reinforcement Time out from positive
reinforcement
Natural consequences for using Reinforcers for the CSO Suggestion of treatment Rapid intake procedures
The Numbers
Randomized into: Ala-non 13% Johnson Institute intervention 23% CRAFT 67%/76%

Promoting Awareness of Motivational Incentives
Seven Principles Target behavior Choice of target population Choice of reinforcer Incentive magnitude Frequency of incentive distribution Timing of the incentive: Duration of the intervention
65
What Do You Get…..
When you take an effective
intervention and implement it in an ineffective way?
66
67
The Joy of Implementation

Stages of Implementation
Exploration and adoption Program installation Initial implementation Full operation Innovation Sustainability
Implementation Research: A Synthesis of the Literature
Fixsen, et. al. 68
69
Considerations
Provider, agency or system culture and readiness
Buy-in on multiple levels Delivery systems (in-person, manual-
driven, etc.) Staff selection Training design and systems Follow through Supervision, mentoring and
coaching
70
Considerations
Costs Mandated use of EBTs??? Policy or mission statements

A Few Resources(more are in the resources
handout)
71

Big Picture View
Rethinking Substance Abuse: What the Science Shows and What We Should Do About It
William R. Miller and Kathleen M. CarrollGuilford Press 2006
72
EBTs
http://www.nrepp.samhsa.gov/index.asp
http://www.drugabuse.gov/blending/
73
Implementation
http://www.fpg.unc.edu/~nirn/resources/detail.cfm?resourceID=31
Fixsen, et. al.
74

Summary
Anything goes is gone No superior approach for all
individuals Variety of approaches work Different people respond to different
approaches Therapeutic relationship is of GREAT
importance Client goals, values, experiences and
cultural background are important75
76
Summary
Treatment programs should offer a variety of evidence-based treatments
Staff should receive training in evidence-based treatments and their work should be observed
Programs need to measure their outcomes
Effective implementation is vital and often overlooked in the process of putting EBTs into practice
77
What Really Matters…..
Its is not the amount or setting of treatment
as much as the method of treatment who provides it and how they relate
From W.R. Miller: “Motivation for Change: 25 Years of Unexpected Findings and Their Implications for Treating Addictions”

Thanks for playing along….
Stephen Brazill, MA, MACRiverside Group, LLC
316 304-5272sbrazill@riversidegroupconsul
ting.com
78