10 management of patient with hypoglycemic coma. management of patient with hyperglycemic...
TRANSCRIPT
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 1/59
CURATION OF PATIENTS WITH
HYPOGLYCEMIC AND HYPERGLYCEMIC COMA
Diabetes mellitus (DM) is a systemic disease that affects essentially every organ of
the body. The fatal outcome is related to the development of acute or chronic
complications.
Classification of acute complications of DM
1. Diabetic coma:
1) diabetic ketoacidisis (DKA);
2) nonketonic hyperglycemic-hyperosmolar coma (NKHHC);
3) Lactoacidosis (LA).
2. Hypoglycemic coma (HC).
DIABETIC KETOACIDISIS (DKA)
Before the area of insulin therapy, ketosis was the leading cause of death of
patients with DM. Since insulin deficiency worsens the clinical picture and leads to
metabolic abnormalities, the complication is more common in young diabetics.
Despite insulin usage, mortality remains high (6 - 10 %).
DKA results from grossly deficient insulin modulation of glucose and lipid
metabolism.
Predisposing factors
1) newly diagnosed diabetes (presenting manifestation);
2) inadequate administration of exogenous insulin;
3) increased requirements for insulin caused by the presence of an underlying
stressful condition:
an intercurrent infection (pneumonia, cholecyctitis);
a vascular disorder (myocardial infarction, stroke);
an endocrine disorder(hyperthyroidism, pheochromocytoma);
trauma;
pregnancy;
surgery.

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 2/59
Pathophysiology of DKA
Insulin deficiency
(absolute or relative)
↓ glucoseuptake
↑ proteolysis ↑ lipolysis
↑aminoa
cides
↑nitrogen
loss
Muscle break-
down
↑ glycerol
free fattyacids
weight
loss
↑ keto-
genesis
Weakn
ess
↑ keton-
emia
Hyperglycemia Gluconeogenesis+ glucogenolysis
↑ keton-uria
Glucosuria
Osmoticdiuresis
Electrolyte depletion
Hypotonic
losses
dehydration and acidosis
Diagnostic criteria
Diabetic ketosis
It is status which is characterized by increased level of ketones in blood, without
clinical signs of dehydration and can be corrected by diet (fat restriction) and regular
insulin injection.
DKA develops over a period of days or weeks.
Signs and symptoms
1. Polydipsia, polyuria and weakness are the most common presenting complaints.
2. Anorexia, nausea, vomiting, and abdominal pain may be present and mimic an
abdominal emergency.

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 3/59
3. Ileus and gastric dilatation may occur and predispose to aspiration.
4. Kussmaul breathing (deep, sighing respiration) is present as respiratory
compensation for the metabolic acidosis and is obvious when the pH is less than
7,1.
5. Symptoms of central-nervous-system involvement include headaches, drowsiness,
lassitude, stupor and coma (only 10 % patients are unconscious).
Physical examination
1. Hypothermia is common in DKA. A fever should be taken as strong evidence of
infection.
2. Hyperpnoea or Kussmaul respiration are present and related to degree of acidosis,
acetone may be detected on the breath (musty (fruity) odor to the breath).3. Tachycardia frequently is present, but blood pressure is usually normal unless
profound dehydration is present.
4. Poor skin turgor may be prominent depending on the degree of hydration.
5. Hyporeflexia (associated with low serum potassium) can be elicited.
6. Signs consistent with a “surgical abdomen” but which follow severe ketonemia
can confuse the clinical picture.
7. In extreme cases of DKA one can see hypotonia, stupor, coma, incoordination of
ocular movements, fixed dilated pupils, and finally death.
8. Other signs from a precipitating illness can be present.
Laboratory findings
1. The hallmark of DKA is the finding of:
- hyperglycemia;
- ketonemia;
- metabolic acidosis (plasma pH and bicarbonates are decreased.
2. A presumptive bedside diagnosis is justified if the urine is strongly positive for
both glucose and ketones.
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 4/59
3. Different changes of electrolyte levels in the blood can be observed and does not
reflect the actual total body deficits.
4. Serum amylase and transaminases can be elevated.
5. Leucocytosis occurs frequently in DKA and therefore cannot be used as a sole
indication of infectious process.Types of DKA:
- abdominal (diabetic pseudoperitonitis, false acute abdomen) is characterized by
acute abdomen pain, dyspeptic signs with vomiting, leucocytosis and look like
acute appendicitis or peritonitis;
- cardiovascular type (characterized by vascular collapse, tachycardia, cyanosis,
pain in the region of the heart, arterial fibrillation and is a result of decreased
blood circulating volume due to the dehydration, in old patients with coronary
arteries atherosclerosis);
- cerebral (encephalopathic) type (can be found in old patients with cerebral vessels
atherosclerosis, characterized by changing of Kussmaul breathing on superficial,
absence of corneal reflexes and is a result of intoxication and brain edema);
- renal (develops in patients with diabetic nephropathy and is characterized by
proteinuria, hematuria, azotemia);
- mixed.
Differential diagnosis
DKA must be distinguished from a variety of clinical conditions, particularly those in
which central-nervous system function is altered and also associated with metabolic
acidosis. The patient’s history and physical examination often are adequate diagnostic
techniques.
The nurse monitors for the signs and symptoms of DKA

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 5/59
• checks blood pressure, pulse and respirations every 15 min until stable
• records urine output, temperature and mental status every hour
• assesses central venous pressure (when central venous catheter has been
placed) usually every 30 minutes
Primary nursing measures are
• assessing the patients airway patence, level of consciousness, hydration status,
status of fluid and electrolyte replacement and levels of blood glucose
(laboratory or bedside glucose monitoring) – results of last indicate the efficacy
of insulin replacement and establish when to switch from saline to dextrose-
containing solutions
•
After stabilization of patient’s condition monitoring vital signs and recordingvalues every 4 hours is acceptable
Treatment
Treatment of diabetic ketosis
1. Inhibition of ketogenesis can be achieved by exclusion of fat from diet and
increasing quantity of high-calorie carbohydrates in meal.
2. Prescription only of short-acting insulin.
Treatment of diabetic ketoacidosis and coma
The most important factor to emphasize is the frequent monitoring of the patient
both clinically and chemically. Initially, laboratory data should be obtained every 1 –
3 hours and less frequently once clinical improvement is noted. If the patient is in
shock, stupor or coma, a nasogastric tube, especially if vomiting, and urinary catheter
are recommended.
Frequent assessment of potassium status is vital. A lead II electrocardiogram
(ECG) can be provide a rapid assessment of hyperkalemia (peaked T waves) and
hypokalemia (flat T waves and presence of U waves). Hyporeflexia and ileus are
clinical indications of potassium deficiency.
Careful observation of neurological status is vital to detect the infrequent but
devastating presence of cerebral edema.
The goals of therapy include:
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 6/59
1. Rehydratation.
2. Reduction of hyperglycemia.
3. Correction of: a) acid-base and b) electrolyte imbalance.
4. Investigation of precipitating factors, treatment of complications.
Rehydration
The average fluid deficit in adults with DKA is 3 to 5 l. A rapid infusion of 0,9
% sodium chloride (e.g., 1 l/h for the first 1 to 2 hours) is given and then reduced to
about 0,5 – 0,3 l/h if the blood pressure is stable and the urine follow is adequate.
After the initial infusion, intravenous fluid therapy must be adjusted individually on
the basis of urine output, clinical assessments of hydration and circulation,
determination of plasma electrolytes and glucose. When serum glucose level is about11 – 13 mmol/l administration of 5 % glucose with insulin can be performed (1 to 2
unites of insulin on each 100 ml of 5 % glucose solution). The addition of glucose to
the intravenous solution is necessary for correction of tissue lipolysis and acidosis.
The nurse checks for clinical indicators of fluid imbalance
• Edema occurs with excess interstitial fluid and is not usually apparent until the
interstitial volume has increased by at least 2 to 3 L. Daily weights provide a
good indication of fluid volume status. One kilogram of body weight equals 1
L of fluid.
• Volume overload can cause an increase in blood pressure to the point of
hypertension. This is true in patients with renal failure who cannot excrete the
extra volume. An increased jugular venous pressure occurs with volume
overload.
• Orthostatic hypotension is an indication of volume depletion. In volume
depletion, jugular venous pulsation may not be visible at a 45-degree angle. In
severe volume depletion, the jugular venous pulsation may not be visible even
with the patient lying flat (Toto, 1998).
Insulin treatment
DKA can be treated with low dose insulin regimens.
Initial intravenous administration of 10 to 14 units of short-acting insulin has to
be prescribed for the patient during first hour. Continuous intravenous infusion of
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 7/59
insulin in a dose 0,1 unit/kg/hour in 0,9 % sodium chloride infusion has to be given
after that.
This solution can be prepared in such way: 50 units of insulin have to be added to a 500 ml
bottle with 0,9 % sodium chloride solution, and as a result each 10 ml of solution will contain 1
Unite of insulin.
If the glucose level does not improve (decrease on 3,3- 5,5 mmol/l) after an hour
of infusion, the rate of insulin is doubled until a response is noted. But if there is a
tendency for quicker decreasing the level of glucemia we have to decrease the dose of
insulin in twice.
When the serum glucose concentration reaches 11-13 mmol/l, insulin can be
given subcutaneously (if plasma and urine persistently negative for ketones). Blood
glucose level should be maintained at about 11 mmol/l during intravenous therapy.
Improvement usually is noted in 8 – 24 hours. Following stabilization of the
clinical condition, patients are placed in insulin regimen consisting of five injections
of regular insulin.
Treatment of electrolyte disorders
Potassium should never be given until the state of renal function is known and
until the serum potassium concentration is available. In most patients the initial serum
potassium is high, normal or elevated, and the initiation of potassium replacement
usually can be given in 2 hours after beginning of rehydration and insulin therapy,
using hourly serum measurements as a guide (table 1).
Hypokalemia can lead to the disturbances of heart rhythm, weakness and
paralyses of intercostal muscles, atone of stomach and intestine, development of
hypakalemic coma.
Table 1. Correction of potassium balance
Serum potassium level Potassium deficiency 2 % potassium solution
< 3 mmol/l 3 gr. 150 ml
3 – 4 mmol/l 2 gr. 100 ml
4 – 5 mmol/l 1,5 gr. 75 ml
5 – 6 mmol/l 1 gr. 50 ml
> 6mmol/l - -
Potassium would to be infused during 3 – 5 hours.

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 8/59
Phosphate deficiency can be treated by potassium phosphate, magnesium
deficiency can be treated by 10 % solution of MgSO4 prescription (6 – 8 ml each 3
hour under the control of blood pressure).
Correction of metabolic acidosis
The metabolic acidosis occurs due to insulin deficiency and dehydration. So
ketone bodies are themselves metabolized to bicarbonate once proper therapy is
begun (fluids, electrolytes, insulin) and exogenous administration of bicarbonate can
overcorrect to alkalosis.
The use of bicarbonate can be recommended only in the following cases:
- if life-threatening hyperkalemia;
-
when severe lactic acidosis complicates DKA;- with severe acidosis (pH<7), especially when complicated by shock that is not
responsive to appropriate fluid resuscitative measures in an attempt to improve
cardiac output.
Bicarbonate would be to infuse at a rate of 100 to 300 ml of 2,5 % solution.
Prevention of hypokalemia can be made by intravenous droply infusion of 50 –
75 ml 2% potassium chloride solution on each 100 mmol of bicarbonate.
Other therapeutic consideration:
- since infection is one of the leading precipitating events of DKA, it should be
looked for and, if found, treated appropriately;
- vascular thrombosis (it is secondary to severe dehydration, high serum viscosity,
and low cardiac output) – heparin (5000 unites 4 times a day);
- vascular collapse can be treated by mesatone (1 – 2 ml); glucocorticoides
(dexametasone 4 mg two times a day). You must remember that development of
vascular collapse after initiation of therapy should suggest the presence of gram-
negative sepsis or silent myocardial infarction;
- cerebral edema (It is a rare and frequently fatal complication. Some physicians
believe that rapid osmotic reduction of plasma glucose should be avoided to
minimize rapid osmotic changes. Some patients have premonitory symptoms (e.g.,
sudden headache, rapid decrease in the level of consciousness), but in others acute
respiratory arrest is the initial manifestation. If cerebral edema is diagnosed,

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 9/59
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 10/59
The syndrome usually occurs in patients with type 2 DM, who are treated with a
diet or oral hypoglycemic agents, sometimes it is a complication of previously
undiagnosed or medically neglected DM (type 2).
In contrast to ketoacidosis, mortality in patients with HNC has been very high
(50 %) in most series. Mortality has been associated with convulsions, deep vein
thrombosis, pulmonary embolus, pancreatitis and renal failure. Death is usually due
to an associated severe medical condition and not to the hyperosmolality.
The pathophysiology of HNC is similar to that of ketoacidosis, except that
ketoacids do not accumulate in the blood. The reason of this phenomenon is unclear.
Initially it was thought that patients with HNC produced enough insulin to prevent
lipolysis and ketogenesis but not enough to prevent hyperglycemia. The concept wasinvalidated by finding similar inappropriately low plasma insulin concentrations in
patients with the two syndromes. The finding of lower plasma free fatty acids, as well
as cortisol and growth-hormone concentrations, in patients with ketoacidosis has
raised the possibility that the absence of ketosis may be the result of decreased
cortisol and growth-hormone effects on lipolysis. Suppression of lipolysis by
hyperosmolality also has been proposed.
HNC usually develops after a period of symptomatic hyperglycemia in which
fluid intake is inadequate to prevent extreme dehydration from the hyperglycemia-
induced osmotic diuresis.
Predisposing factors
1. HNC seems to occur spontaneously in about 5 – 7 % of patients.
2. In 90 % of patients some degree of renal insufficiency seems to coexist.
3. Infection (e.g., pneumonia, urinary tract infection, gram-negative sepsis) is
underlying frequent precipitating cause.
4. Use of certain drugs has been associated with this condition:
- steroids increase glucogenesis and antagonize the action of insulin;
- potassium-wasting diuretics (hypokalemia decreases insulin secretion), e.g.,
thiazides, furosemide;
- other drugs, e.g., propranolol, azathioprine, diazoxide.

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 11/59
5. Other medical conditions such as cerebrovascular accident, subdural hematoma,
acute pancreatitis, and severe burns have been associated with HNC.
6. Use of concentrated glucose solutions, such as used in peripheral
hyperalimentation or renal dialysis, has been associated with HNC.
7. HNC can be induced by peritoneal or hemodialysis, tube feeding.
8. Endocrine disorders such as acromegaly, Cushing disease, and thyrotoxicosis have
also been associated with HNC.
Diagnostic criteria
Signs and symptoms
1. Polyuria, polydipsia, weight loss, weakness and progressive changes in state of
consciousness from mental cloudiness to coma (present in 50 % of patients) occurover a number of days to weeks.
2. Because other underlying conditions (such as cerebrovascular accident and
subdural hematoma) can coexist, other causes of coma should be kept in mind,
especially in the elderly.
3. Seizures occur in 5 % of patients and may be either focal or generalized.
Physical examination
1. Severe dehydration is invariably present.
2. Various neurologic deficits (such as coma, transient hemiparesis, hyperreflexia,
and generalized areflexia) are commonly present. Altered states of consciousness
from lethargy to coma are observed.
3. Findings associated with coexisting medical problems (e.g., renal disease,
cardiovascular disease) may be evident.
Laboratory findings
1. Extreme hyperglycemia (blood glucose levels from 30 mmoll/l and over are
common.
2. A markedly elevated serum osmolality is present, usually in excess of 350
mOsm/l. (Normal = 290 mOsm/l). The osmolality can be calculated by the
following formula: mOsm/l = 2(Na + K) = blood glucose/18 + BUN/2.8.
3. The initial plasma bicarbonate averaged.
4. Serum ketones are usually not detectable, and patients are not acidic.

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 12/59
5. Serum sodium may be high (if severe degree of dehydration is present), normal, or
high (when the marked shift of water from the intracellular to the extracellular
space due to the marked hyperglycemia is present).
6. Serum potassium levels may be high (secondary to the effects of hyperosmolality
as it draws potassium from the cells), normal, or low (from marked urinary losses
from the osmotic diuresis). But potassium deficiency exists.
Treatment
This condition is a medical emergency and the patient should be placed in an
intensive care unit.
Many of the management techniques recommended for a patient with DKA are
applicable here as well.The goals of therapy include:
- rehydration;
- reduction of hyperglycemia;
- electrolytes replacement;
- investigation of precipitating factors, treatment of complications.
Rehydration
The average fluid deficit is 10 liters, and acute circulatory collapse is a common
terminal event in HNC. The immediate aims of treatment are to rapidly expand the
contracted intravascular volume in order to stabilize the blood pressure, improve the
circulation, and improve the rate of urine production.
It is important to remember that it is the severe hyperglycemia and the concomitant obligatory
shift of water from the intracellular to the intravascular compartment that prevents this latter space
from collapsing at the time of severe fluid depletion. With too rapid a correction of hyperglycemia,
potential hypovolimic shock (as fluid moves from the extracellular space back into the intracellular
space) may occur.
Treatment is starting by infusion 1 to 2 liters of 0,9 % sodium chloride over 1 to
2 hours; if this suffices to stabilize the blood pressure, circulation and restore good
urine flow, the intravenous fluid can be changed to 0,45 % sodium chloride to
provide some free water. 0,45 % sodium chloride is used at a rate of 150 to 500
ml/hour depending on the state of hydration, previous clinical response and the
balance between fluid input and output. The aim of this phase of intravenous fluid
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 13/59
therapy is not to attempt to rapidly correct the total fluid deficit or the
hyperosmolality, but rather to maintain stable circulation and renal function and to
progressively replenish water and sodium at rates that do not threaten or cause acute
fluid overload.
Generally, half of the loss is replaced in the first 12 hours and the rest in the
subsequent 24 hours.
Insulin therapy
Insulin treatment in HNC is started by 10 to 20 unites of regular insulin
intravenously as a bolus dose prior to starting the insulin infusion and then giving
intravenously regular insulin in a dose of 0,05 – 0,10 unites/kg/hour (many
authorities routinely use the same insulin treatment regimens as for treating DKA,other authorities recommend smaller doses of insulin, because they believe that
patients with type 2 DM are offer very sensitive to insulin, but this view is not
universally accepted, and many obese type 2 diabetics with NHC require larger
insulin doses to induce a progressive decrease in their marked hyperglycemia.
It is important to remember that because of insulin therapy causes blood glucose levels to
fall, water shifts into the cells and existing hypotension and oliguria can further aggravated. Thus,
initially some advocate delaying insulin therapy while infusion normal saline until vital signs have
improved.
When the plasma glucose reaches the range 11 – 13 mmoll/l, 5 % glucose
should be added to the intravenous fluids to avoid the risk of hypoglycemia.
Following recovery the acute episode, patients are usually switched to adjusted doses
of subcutaneous regular insulin at 4 to 6-hour intervals. When they are able to eat,
this is changed to a 1 or 2 injection regimen.
Treatment of electrolyte disorders
Once urine flow has been reestablished, potassium should be added to begin
repletion of the total body deficits.
Potassium replacement is usually started by adding 20 mmoll/l to the initial liter
of the intravenously-infused 0,45 % sodium chloride with careful serum potassium
and ECG monitoring.

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 14/59
LACTIC ACIDOSIS (LA)
DM is one of the major causes of LA, a serious condition characterized by
excessive accumulation of lactic acid and metabolic acidosis.
The hallmark of LA is the presence of tissue hypoxemia, which leads to
enhanced anaerobic glycolysis and to increased lactic acid formation.
Pyruvic acid Lactic acid
NADH NAD
Acetoacetic Beta-hydroxybutyric
Piruvic acid is converted into lactic acid by lactic dehydrogenase (LDH) in the
presence of reduced nicotinamide adenine dinucleotide (NADH), which, in turn, is
converted into NAD. The reaction is reversible and involves LDH in both
directions. The conversion of acetoacetic acid into beta-hydroxybutyric acid also
requires the oxydation of NADH. LA results from decreased availability of NAD
caused by lack of oxygen. Likewise, the deficiency of NAD impairs the conversion
of beta-hydroxybutyric into acetoacetic acid. Thus, LA predisposes to
accumulation of beta-hydroxybutyric acid, which does not react with acetest tablet,
so, the reaction for ketone bodies may be negative or slightly positive. The normal
blood lactic acid concentration is 1mmol/l, and the pyruvic to lactic ratio is 10:1.
An increase in lactic acid without concomitant rise in pyruvate leads to LA of
clinical importance.
Predisposing factors
1. Heart and pulmonary failure (which leads to hypoxia).
2. Usage of bigyanids, pheformin therapy.
3. Alcohol intoxication.
4. Ketoacidosis (it is important to have a very high index of suspection with respect
to presence of LA).
Diagnostic criteria

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 15/59
Signs and symptoms
1. Kussmaul breathing (deep, sighing respiration) is present as respiratory
compensation for the metabolic acidosis and is obvious when the pH is less than
7.2.
2. Symptoms of central-nervous-system involvement include headaches, drowsiness,
lassitude.
3. Anorexia, nausea, vomiting, and abdominal pain may be present.
4. Myalgia is common.
Physical examination
1. Acrocyanosis is common.
2.
Tachycardia frequently is present, blood pressure is decreased.3. Poor skin tugor and dry skin may be prominent.
4. Hypothermia is common in LA.
5. Hyperpnea or Kussmaul respiration are present and related to degree of acidosis.
4. Findings associated with coexisting medical problems (e.g., renal disease,
cardiovascular disease) may be evident.
Laboratory findings
1. Blood glucose level is not high
2. Glucosurea is absent.
3. Blood lactic acid is high.
Treatment of LA
LA is treated by correcting the underlying cause.
In severe cases, bicarbonate therapy should be used (intravenously-infused 2,5 %
sodium bicarbonates 1 to 2 l/day).
LA can be treated with low dose insulin regimens with 5 % glucose solution infusion.
Volume expanders and oxygen therapy are helpful treatment as well.
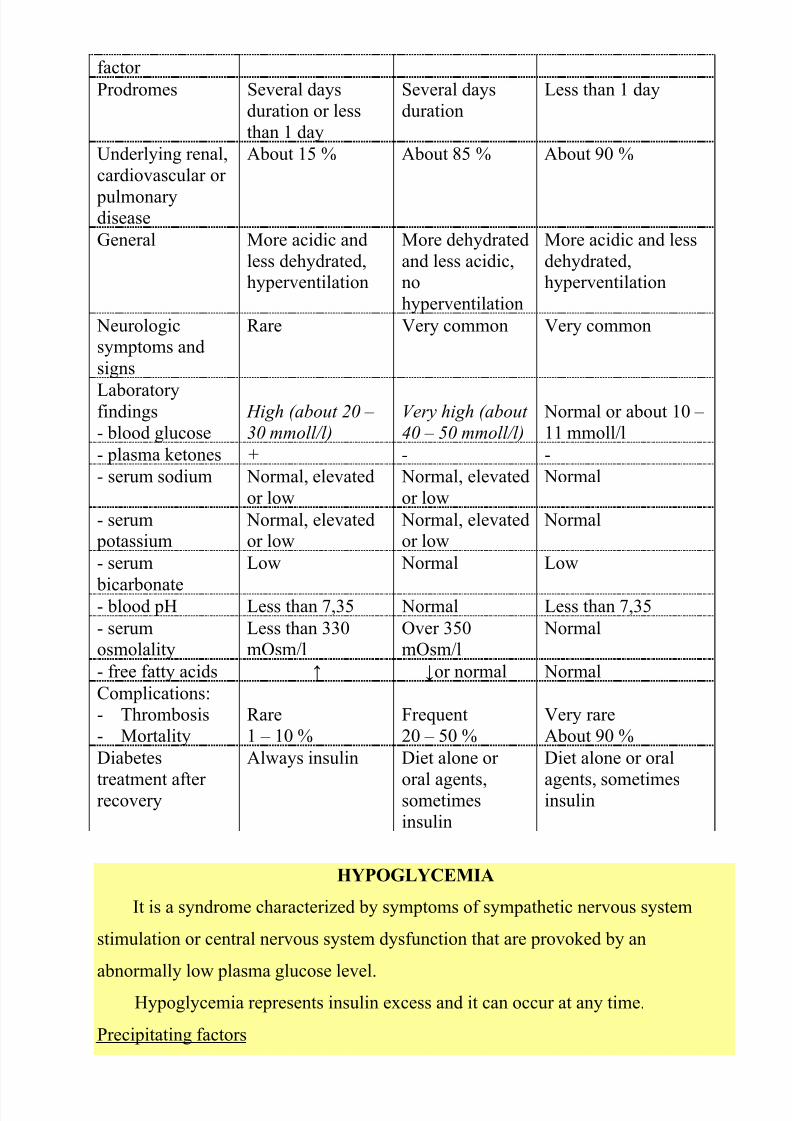
Diagnostic criteria of different hyperglycemic coma are shown in table 2.
Table 2. Comparison of DCA, HNC and LA.
DKA HNC LA
Age Below 40 Above 40 Above 40Type of DM Type 1 > type 2 Type 2 Type 2
Predisposing Insulin deficiency Dehydration Hypoxia
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 16/59
factor
Prodromes Several days
duration or less
than 1 day
Several days
duration
Less than 1 day
Underlying renal,
cardiovascular or
pulmonarydisease
About 15 % About 85 % About 90 %
General More acidic and
less dehydrated,hyperventilation
More dehydrated
and less acidic,no
hyperventilation
More acidic and less
dehydrated,hyperventilation
Neurologicsymptoms and
signs
Rare Very common Very common
Laboratoryfindings
- blood glucose
High (about 20 –
30 mmoll/l)
Very high (about
40 – 50 mmoll/l)
Normal or about 10 –
11 mmoll/l
- plasma ketones + - -
- serum sodium Normal, elevated
or low
Normal, elevated
or low
Normal
- serum potassium
Normal, elevatedor low
Normal, elevatedor low
Normal
- serum
bicarbonate
Low Normal Low
- blood pH Less than 7,35 Normal Less than 7,35
- serumosmolality
Less than 330mOsm/l
Over 350mOsm/l
Normal
- free fatty acids ↑ ↓or normal Normal
Complications:
- Thrombosis
- Mortality
Rare
1 – 10 %
Frequent
20 – 50 %
Very rare
About 90 %
Diabetes
treatment afterrecovery
Always insulin Diet alone or
oral agents,sometimes
insulin
Diet alone or oral
agents, sometimesinsulin
HYPOGLYCEMIA
It is a syndrome characterized by symptoms of sympathetic nervous system
stimulation or central nervous system dysfunction that are provoked by an
abnormally low plasma glucose level.
Hypoglycemia represents insulin excess and it can occur at any time.
Precipitating factors

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 17/59
- irregular ingestion of food;
- extreme activity;
- alcohol ingestion;
- drug interaction;
- liver or renal disease;
- hypopituitarism and adrenal insufficiency.
Diagnostic criteria
Signs and symptoms
Two distinct patterns are distinguished:
1) adrenergic symptoms (they are attributed to increased sympathetic activity and
epinephrine release):- sweating,
- nervousness,
- tremulousness,
- faintness,
- palpitation,
- and sometimes hunger;
2) cerebral nervous system manifestations: confusion, inappropriate behavior (which
can be mistaken for inebriation); visual disturbances, stupor, coma or seizures.
(Improvement in the cerebral nervous system manifestations will be with a rise in
blood glucose.)
A common symptom of hypoglycemia is the early morning headache, which is
usually present when the patient awakes.

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 18/59
Patients should be familiar with the symptoms of the hypoglycemia but some of
them are not heralded by symptoms.
Physical examination
1. The skin is cold, moist.
2. Hyperreflexia can be elicited.
3. Hypoglycemic coma is commonly associated with abnormally low body
temperature
4. Patient may be unconsciousness.
Laboratory findings
1. Low level of blood glucose
Treatment
Insulin – treated patients are advised to carry sugar lumps, candy, or glucosetablets at all time.

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 19/59
If the symptoms of hypoglycemia develop, the patients have to drink a glass of
fruit juice or water with 3 tbsp. of table sugar added or to eat candy, and to teach their
family members to give such treatment if they suddenly exhibit confusion or
inappropriate behavior:
1) glucagon 0,5 – 1 unit (0,5 – 1 ml) s/c, i/m or i/v with next fruit juice or candy
taken. If the patient does not respond to 1 unit of glucagon within 25 minutes,
further injections are unlikely to be effective, and are not recommended;
Glucagon
2) an i/v injection of 20 or 100 ml of 40 % glucose, followed by a continuous
infusion of 5 % glucose (10 % glucose may be needed) until it clearly can bestopped safely;
3) glucocorticoids and adrenaline are helpful as well.

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 20/59
We recommended you to repeat general information about diabetes mellitus.
Anatomy and physiology of pancreatic gland
Pancreatic gland is located in the upper abdomen, with the head lying
immediately adjacent to the end the body and tail extending across the midline nearly
to the spleen. In adults, most of the pancreatic tissue is devoted to exocrine function,
in which digestive enzymes are secreted via the pancreatic ducts into the duodenum.
The endocrine pancreas consists of the islets of Langerhans (named for the 19th-
century German pathologist Paul Langerhans). There are approximately one million
islets that weigh about 1 gram Approximately 75% of the cells in each islet are
insulin-producing beta cells, which are clustered centrally in the islet. The remainder
of each islet consists of alpha, delta, and F (or PP) cells (table 1) and are located atthe periphery of the islet. Each islet is supplied by one or two very small arteries
(arterioles) that branch into numerous capillaries. These capillaries emerge and
coalesce into small veins outside the islet. The islets also contain many nerve endings
(predominantly involuntary, or autonomic, nerves that monitor and control internal
organs).
Table 1. Production of hormones by pancreatic glands
Cell type Endocrine product
Alpha cells (A cells) glucagon
Beta cells (B cells) insulin
Delta cells (D cells) somatostatin
F (or PP) cells pancreatic polypeptide
Insulin is an anabolic hormone (promotes the synthesis of carbohydrates,
proteins, lipids and nucleic acids (table 2)). The most important target organs for
insulin action are: the liver, muscles and adipocytes. The brain and blood cells are
unresponsive to insulin.
Table 2. Biological effects of insulin
Type of metabolism The effects of insulin
carbohydratemetabolism
stimulation of glucose transport across muscle and adipose
cell membranes
regulation of hepatic glycogen synthesis inhibition of glucose formation – from glycogen
(glycogenolysis) and – from amino-acid precursors
(glyconeogenesis)

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 21/59
The result of these actions is a reduction in blood glucose
concentration
Protein metabolism the transfer of amino acids across plasma membranes
stimulation of protein synthesis
inhibition of proteolysis
Lipid metabolism incorporation of fatty acids from circulating triglyceride
into adipose triglyceride stimulation of lipid synthesis
inhibition of lipolisis
Nucleic acids
metabolism stimulation of nucleic acid synthesis by stimulating the
formation of adenosine triphosphate (ATP), DNA and RNF
Other effects of insulin:
1) stimulation of the intracellular flew of potassium, phosphate and magnesium in
the heart;
2) inhibition of inotropic and chronotropic action (unrelated to hypoglycemia).
The action of insulin can be decreased by contra-insulin hormones (table 3).
Table 3. Action of contra-insulin hormones
Hormone Action
glucagon stimulates glycogenolysis
stimulates glyconeogenesis
somatostatin inhibits secretion of insulin
regulates glucose absorption from alimentary tract into blood
glucocorticoids decrease of glucose utilization by tissues
stimulate glycogenolysis
stimulate glyconeogenesis
increase lipogenesis (in patients with insulin resistance)
catecholamines inhibits β-cells secretion
stimulates glycogenolysis
stimulates ACTH secretion
somatotropin stimulates α-cells (which secret glucagon) increases activity of enzymes which destroy the insulin
stimulates glyconeogenesis
increases of glucose exit from the liver veins into blood
decreases of glucose utilization by tissues
ACTH stimulates glucocorticoides secretion and β-cells secretion
thyroid hormones increase glucose absorption into blood
stimulate glycogenolysis
inhibit fat formation from the carbohydrates
DIABETES MELLITUS
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 22/59
Epidemiology. It is probably fair to state that about 4 to 7 percentage of the world
population is affected with diabetes mellitus (DM). The disease is more common in
persons after age 45, in obese individuals, in certain ethnic groups, and in those with
a positive family history of DM: for a child, born from the mother with type 1
diabetes, risk to get diabetes is 1:50, and from the sick father – 1:15. Each 12-15
years the quantity of diabetics increases twice.
The term diabetes mellitus refers to the excretion of large quantities of sweet
urine. Diabetes is an old word for siphon and means “dieresis”, mellitus means
“sweet”. The clinical syndrome known as DM comprises a wide variety of
symptoms, physical findings and laboratory abnormalities, in which multiple
etiologic factors are involved, the pathophysiology is partly understood and treatmentis unsatisfactory. The hallmark of DM is hyperglycemia.
Diabetes mellitus – is an endocrine – metabolic disease, which develops due to
absolute or relative insulin insufficiency and characterized by chronic hyperglycemia,
changes of different systems and organs of patient.
Absolute insulin insufficiency means that pancreas produce insulin in very low
quantities or doesn’t produce it at all (due to destruction of beta-cells by
inflammation, autoimmune process or surgery).
Relative insulin insufficiency means that pancreas produces or can produce
insulin but it doesn’t “work”. (The pathologic process can be on the next levels:
beta cells: they can be not sensitive for the high level of glycemia;
insulin: abnormal insulin, insulin antibodies, excessive quantity of contra-insulin
hormones, absence of enzyme, which converts proinsulin into insulin, etc;
receptors: decreased quantity of receptors or diminished binding of insulin.
Stages of diabetes mellitus development
1. Prediabetes (risk factors or predispose factors):
obesity;

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 23/59
positive family history of DM;
persons which were born with weight more than 4,0 kg;
women in which: = were born children with weight more than 4,0 kg; =had
abortions and dead child in anamnesis;
- persons with:
= atherosclerosis, hypertension;
= autoimmune diseases;
= furunculous;
= rubella, mumps, Coxsackie virus, infectious hepatitis, cytomegalovirus,
infection mononucleosis.
2. Impaired glucose tolerance (latent DM).
3. Clinical manifestation of DM.
Etiologic classification of DM (WHO recommendations, 1999)
I. Type 1* of DM (destruction of β-cells which mostly leads to absolute insulin
insufficiency):
autoimmune;
idiopathic.

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 24/59
II. Type 2 of DM (resistance to insulin and relative insulin insufficiency or defect
of insulin secretion with or without resistance to insulin).
III. Other specific types:
genetic defects of β-cells function (MODY-1; MODY-2; MODY-3; etc);
genetic defects of insulin action (insulin type A resistance, lipoatrophic
diabetes, Rabson-Mendenchole syndrome, leprechaunism, etc);
diseases of the exocrine pancreas (pancreatitis; trauma, pancreatectomy;
neoplasia; cystic fibrosis, fibrocalculosis; hemochromatosis);
endocrinopathies (acromegaly; Cushing’s syndrome; pheochromocytoma;
glucagonoma, thyrotoxicosis, aldosteroma, somatostatinoma)
drug- or chemical-induced (Vacor**; Pentamidine; Nicotinic acid;
Glucocorticoids; Thyroid hormone; Diazoxide; Beta-adrenergic agonists;
Thiazides; Phenytoin; Alfa-interferon);
infections (Congenital rubella; Cytomegalovirus)
Uncommon forms of immune-mediated diabetes (“stiff -man, antibodies for
insulin, antibodies for insulin’ receptors)
Other genetic syndromes sometimes associated with diabetes (Down
syndrome; Klinefelter's syndrome; Turner's syndrome; Wolfram syndrome;
Friedreich's ataxia; Huntington's chorea; Lawrence-Moon Beidel syndrome;
Myotonic dystrophy; Porphyria; Prader-Willi syndrome; etc)
IV. Gestation diabetes.
*- Arabic numerals are specifically used in the new system to minimize the occasional confusion of
type “II” as the number “11”
**- Vacor is an acute rodenticide that was released in 1975 but withdrawn as a general-use pesticidein 1979 because of severe toxicity. Exposure produces destruction of the beta cells of the pancreas,
causing diabetes mellitus in survivors.
Type 1 is characterized by pancreatic islet beta cell destruction and absolute
insulinopenia.
Current formulation of the pathogenesis of type 1 DM includes the following:
1. A genetic predisposition, conferred by diabetogenic genes on the short arm of
chromosome C, either as part of it or in close proximity to the major
histocompatibility complex (MMHC) region (more than 95 % of type 1 diabetes
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 25/59
individuals are HLA DR 3, DR 4 or DR 3/DR 4; on the other hand, HLA DR 2 confers
protection against the development of type 1 DM);
2. Putative environmental triggers (possibly viral infections (Coxsackie B, rubella)
or chemical toxins (nitrosourea compounds)) that in genetically susceptible
individuals might play a role in initiating the disease process.
3. An immune mechanism gone awry, either initiation of immune destruction or loss
of tolerance, leading to slow, progressive loss of pancreatic islet beta cells and
eventual clinical onset of type 1 diabetes.
Stages of type 1 DM development (by Flier, 1986)
I. A genetic predisposition or changes of immunity.
II.
Putative environmental triggers.III. Active autoimmune insulities with β-cells destruction.
IV. Progression of autoimmune insulities with destruction of >50 % of β-cells.
V. Development of manifest DM (table 1).
VI. Total β-cells destruction.
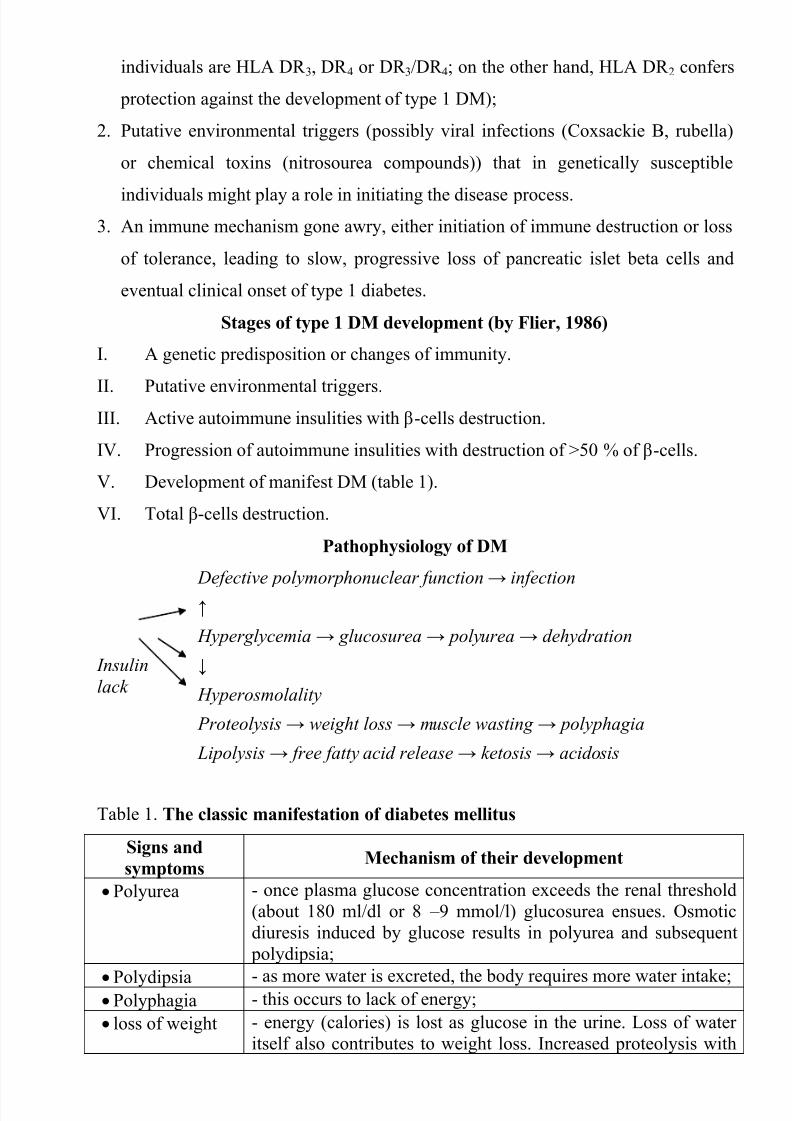
Pathophysiology of DM
Insulin
lack
Defective polymorphonuclear function → infection
↑
Hyperglycemia → glucosurea → polyurea → dehydration
↓
Hyperosmolality
Proteolysis → weight loss → muscle wasting → polyphagia
Lipolysis → free fatty acid release → ketosis → acidosis
Table 1. The classic manifestation of diabetes mellitus
Signs and
symptomsMechanism of their development
Polyurea - once plasma glucose concentration exceeds the renal threshold
(about 180 ml/dl or 8 – 9 mmol/l) glucosurea ensues. Osmotic
diuresis induced by glucose results in polyurea and subsequent
polydipsia;
Polydipsia - as more water is excreted, the body requires more water intake; Polyphagia - this occurs to lack of energy;
loss of weight - energy (calories) is lost as glucose in the urine. Loss of water
itself also contributes to weight loss. Increased proteolysis with
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 26/59
mobilization of aminoacids leads to enhancement of protein
catabolism and loss of weight, notably in muscle mass;
fatigue and
weakness
- probably occur as a result of decreased glucose utilization and
electrolyte abnormalities;
acidosis - develops due to increased lipolysis which cause the release of
free fatty acids, which are metabolized to ketones by the liver.
Individuals with type 1 DM are ketosis prone under basal conditions. The onset
of the disease is generally in youth, but it can occur at any age. Patients have
dependence on daily insulin administration for survival.
Type 2 DM is the most common form of diabetes, accounting for 95 – 90 % of
the diabetic population. Most investigators agree that genetic factors underlie 2 DM,
but it is probably not caused by defects at a single gene locus. Obesity, diet, physical
activity, intrauterine environment, and stress are among the most commonly
implicated environmental factors which play a role in the development of the disease.
Presenting signs and symptoms of type 2 DM include polyurea, polydipsia,
polyphagia; the majority of individuals (80 – 85 %) are obese, but it can also occur in
lean persons.
Patients with DM are at risk of chronic complications developing (Chapter ????
tablers???). Long-term complications of diabetes include retinopathy with potentialloss of vision; nephropathy leading to renal failure; peripheral neuropathy with risk of
foot ulcers, amputations, and Charcot joints; and autonomic neuropathy causing
gastrointestinal, genitourinary, and cardiovascular symptoms and sexual dysfunction.
Patients with diabetes have an increased incidence of atherosclerotic cardiovascular,
peripheral arterial, and cerebrovascular disease. Hypertension and abnormalities of
lipoprotein metabolism are often found in people with diabetes.
Physical examination
Skin
The skin is a common target of DM. Many lesions can be observed, but none isspecific to the disease, with the possible exception of necrobiosis lipoidica
diabeticorum (it consists of skin necrosis with lipid infiltration and is also
characteristically found in the pretibial area. The lesions resemble red plaques with
distinct borders).

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 27/59
The most common skin lesion is diabetic dermopathy (it is characterized by
brown, atrophic, well-demarcated areas in the pretibial region which resemble sears),
besides patients sometimes have xanthoma diabeticorum, which is usually located on
the buttocks, elbows and knees, look like eruptions (but is not really diabeticorum
since it occurs in the patients with lipoprotein abnormalities, particularly
hyperchylomicronemia, whether or not patient has DM).
The skin is dry and itches. Infections of the skin by bacteria and fungi,
candidiasis of the external female genitalia, hyperkeratosis, and nail disorders are
common in the patients with DM but nothing is specific with regard to their
development.
Subcutaneous adipose tissueThe abdomen type of obesity is common in patients with type 2 DM. Sometimes
generalized subcutaneous adipose tissue atrophy can be observed in diabetics.
Bones
Osteoporosis and osteoarthropaphy can be finding in patients with DM.
Gastrointestinal tract
Paradontosis, gastritis with decreased secretion ability, gastroduodenitis,
hepatosis and diarrhea are common in patients with DM.
Cardiovascular system (CVS)
Involvement of CVS, particularly the coronary circulation, is common in
patients with DM.
The heart, arteries, arterioles, and capillaries can be affected. Cardiovascular
changes tend to occur earlier in patients with DM when compared with individuals of
the same age, in the same quantity cases in both sexes. Atypical (painless) forms of
ischemic heart disease are common in diabetics. Several factors play a role in the
high incidence of coronary artery disease seen in patients with DM. These include
age of the patient, duration and severity of the diabetes, and presence of other risk
factors such as hypertension, smoking and hyperlipoproteinemia. It has been
suggested that in some patients with DM, involvement of the small vessels of the
heart can lead to cardiomyopathy, independent of narrowing of the major coronary
arteries. Myocardial infarction is responsible for at least half of deaths in diabetic
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 28/59
patients, and mortality rate for the diabetics is higher than that for nondiabetics of the
same age who develop this complication.
Hypertension is common in patients with DM, particularly in the presence of
renal disease (as a result of atherosclerosis, destruction of juxtaglomerular cells,
sympathetic-nervous-system dysfunction and volume expansion).
Atherosclerosis of femoral, popliteal and calf larger arteries may lead to the
diabetic macroangiopathy of lower extremities, which presents as intermittent
claudication, cold extremities, numbness, tingling and gangrene. Diabetic
microangiopathy of lower extremities can be on patients also.
Respiratory system Mucomycosis of the nasopharinx, sinusitis, bronchitis, pneumonia, tuberculosis
are more common in patients with diabetes than in nondiabetics.
Kidneys and urinary tract
Renal disease include diabetic nephropathy, necrosing renal papillitis, acute
tubular necrosis, lupus erythematosus, acute poststreptococcal and
membranoproliferative glomerulonephritis, focal glomerulosclerosis, idiopathic
membranous nephropathy, nonspecific immune complex glomerulonephrities,
pyelitis, pyelonephritis, cystitis and others. Obviously, these abnormalities, with
exception of diabetic nephropathy, are not at all peculiar to DM and can be observed
in many other conditions. Diabetic nephropathy can develop in patients with DM.
Eyes
Complications of the eyes include: diabetic retinopathy ceratities, retinitis,
chorioretinitis, and cataracts. The last one occurs commonly in the patients with long-
standing DM and may be related to uncontrolled hyperglycemia (glucose metabolism
by the lens does not require the presence of insulin. The epithelial cells of the lens
contain the enzyme aldose reductase, which converts glucose into sorbitol. This sugar
may be subsequently converted into fructose by sorbitol dehydrogenase. Sorbitol is
retained inside the cells because of its difficulty in transversing plasma membranes.
The rise in intracellular osmolality leads to increased water uptake and swelling of
the lens).
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 29/59
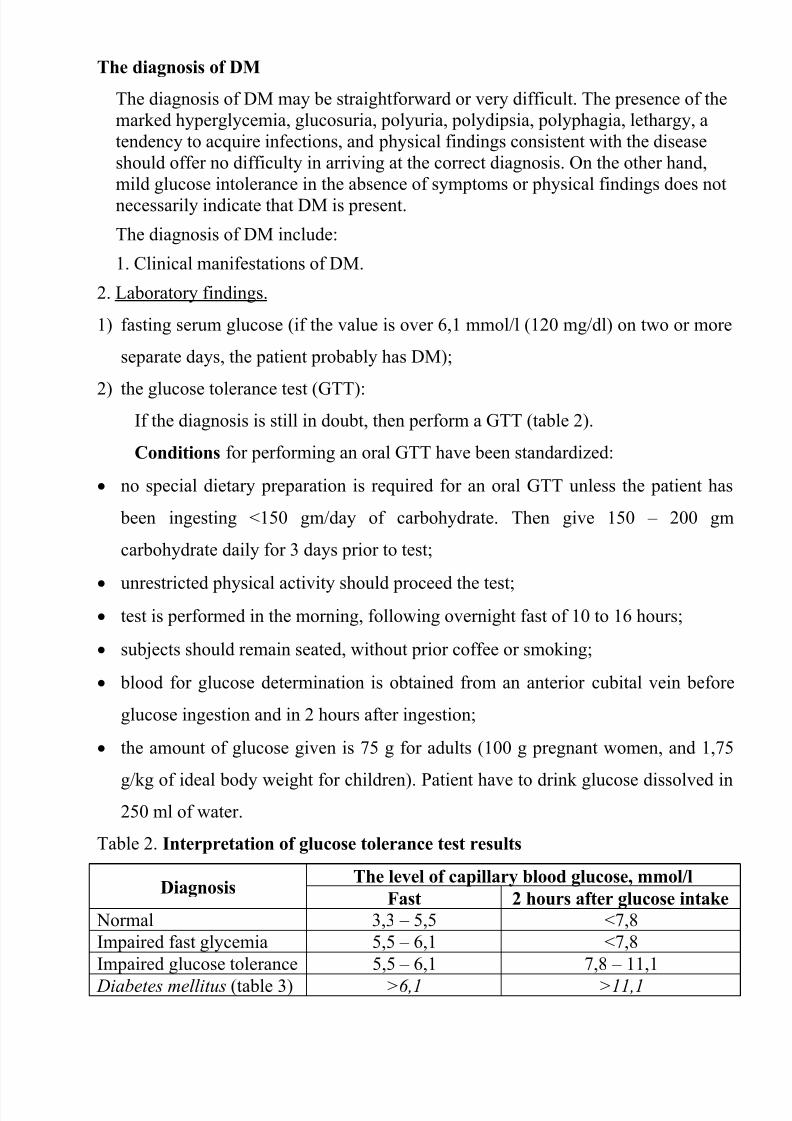
The diagnosis of DM
The diagnosis of DM may be straightforward or very difficult. The presence of the
marked hyperglycemia, glucosuria, polyuria, polydipsia, polyphagia, lethargy, a
tendency to acquire infections, and physical findings consistent with the disease
should offer no difficulty in arriving at the correct diagnosis. On the other hand,
mild glucose intolerance in the absence of symptoms or physical findings does not
necessarily indicate that DM is present.
The diagnosis of DM include:
1. Clinical manifestations of DM.
2. Laboratory findings.
1) fasting serum glucose (if the value is over 6,1 mmol/l (120 mg/dl) on two or more
separate days, the patient probably has DM);
2) the glucose tolerance test (GTT):If the diagnosis is still in doubt, then perform a GTT (table 2).
Conditions for performing an oral GTT have been standardized:
no special dietary preparation is required for an oral GTT unless the patient has
been ingesting <150 gm/day of carbohydrate. Then give 150 – 200 gm
carbohydrate daily for 3 days prior to test;
unrestricted physical activity should proceed the test;
test is performed in the morning, following overnight fast of 10 to 16 hours;
subjects should remain seated, without prior coffee or smoking;
blood for glucose determination is obtained from an anterior cubital vein before
glucose ingestion and in 2 hours after ingestion;
the amount of glucose given is 75 g for adults (100 g pregnant women, and 1,75
g/kg of ideal body weight for children). Patient have to drink glucose dissolved in250 ml of water.
Table 2. Interpretation of glucose tolerance test results
DiagnosisThe level of capillary blood glucose, mmol/l
Fast 2 hours after glucose intake
Normal 3,3 – 5,5 <7,8
Impaired fast glycemia 5,5 – 6,1 <7,8
Impaired glucose tolerance 5,5 – 6,1 7,8 – 11,1
Diabetes mellitus (table 3) >6,1 >11,1

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 30/59
The major indication for an oral GTT is to exclude or diagnose DM (mostly type
2) in those suspected of having diabetes although fasting or symptomatic
hyperglycemia is absent; e.g., in patients with a clinical condition that might be
related to undiagnosed DM (e.g., polyneuropathy, retinopathy). Various conditions
(other than DM) and drugs can cause abnormalities in the oral GTT. The criteria of
DM do not apply to patients treated with drugs that can impair glucose tolerance
(e.g., thiazids, glucocorticoids, indometacin, nicotinic acid, oral contraceptives
containing synthetic estrogenes) or to patients who develop nausea, sweating,
faintness or pallor during the test, or to have infections, hepatic, renal and endocrine
disease that impairs glucose tolerance.
3) glycohemoglobin (HbA1c)
(This test is an indicator of blood sugar control during the previous 2-to-3-month
period. The level of HbA1c >6,5% estimate diagnosis of DM and may be alternative
method of DM diagnostic criteria in compare to GGT);
4) islet cell antibody levels will be positive prior to any insulin administration in 60 –
80 % of patients with type 1 DM;
5) C-peptide (it is not affected by antibodies to exogenous insulin and is used to
distinguish type 1 and 2 DM if there is still a need after clinical determination);
6) glucose level in urine;
7) acetonurea;
8) blood lipids and others.
3. Instrumental investigations usually are used to diagnose chronic complications of
DM.
Table 3. Differential diagnosis of type 1 and type 2 DM
Signs Type 1 DM Type 2 DM
1. Age Young (under 40) Old, moderate (over 40)
2. Beginning of disease Acute Gradual
3. Duration Labile Stable
4. Ketosis, ketoacidosis Often develops Rare develops
5. Body weight Decreased or normal Obesity in 80-90%of patients
6. Treatment Insulin, diet Diet, oral hypoglycemic

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 31/59
agents or insulin
7. Degrees of severity
(table 4)
Moderate, severe Mild, moderate, severe
8. Season of disease
beginning
Frequently autumn-winter
period
Absent
9. Connection with HBA-
system
Present Absent
10. Level of insulin and C- peptide
Decreased or absent Frequently normal level
11. Antibodies to β-cells Present in 80-90% of
patients on first year
Absent
12. Late complications Microangiopathies Macroangiopathies
13. Mortality Less than 10% More than 20%
14. Spreading 10-20% 80-90%
Table 4. Degrees of severity of DM
CriteriaDegree of severity
mild moderate Severe
compensation can
be achieved by
Diet oral hypoglycemic
agents (in patients
with type 2 DM) or
insulin (in patientswith type 1 DM)
by insulin or oral
hypoglycemic
agents
fast serum glucose
level, mmol/l
8,4 8,4 – 14,0 14,0
Glucosuria 20 gr. /l (2 %) 20 to 40 gr. /l (2 – 4
%)
40 gr. /l (4 %)
C o m p l i c a t i o n s
Acute
complications
proneness to
ketosis does not
occur
ketosis can occur ketosis is common,
frequent
hypoglycemia
long-term(chronic)
complications
are rare or onlyfunctional stages
can be observed
complications can beobserved (but not last
stages*)
last stages of long-term (chronic)
complications are
present**
* - nonproliferative stage of diabetic retinopathy, diabetic nephropathy on stage of
microalbuminurea, diabetic neuropathy, etc;
** - preproliferative or proliferative stages of diabetic retinopathy, diabetic
nephropathy on stage of proteinurea or chronic renal failure, autonomic diabetic
neuropathy, diabetic foot syndrome, postinfarction cardiosclerosis, stroke, etc.
Stages of compensations:
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 32/59
1. Compensation.
2. Subcompensation.
3. Decompensation.
Criteria of compensative stage
1. Patient hasn’t new complains.
2. Fast serum glucose level is normal (but can be under 7.0 mmol/l in old patients or
which have cardiovascular disorders) (table 5).
3. Glucose in urine is absent.
4. Glucose level fluctuation is under 4.4-5.5 mmol/l during the day .
5. HbA1c <7,0%
6.
Comatose and precomatose statuses are absent.Criteria of subcompensative stage
1. Patient may have new complains.
2. Fast serum glucose is high.
3. Glucosuria is present.
4. Glucose level fluctuation is over 4.4-5.5 mmol/l during the day.
5. HbA1c 7,1 – 7,5%.
6. Comatose or precomatose statuses are absent.
Table 5. Criteria of carbohydrate metabolism compensation in patients with DM
Criteria compensation subcompensation decompensation **
HBA1c, % <7,0 7,1 – 7,5 >7,5
Fast glucemia* 5,0 – 6,0 6,1 – 6,5 >6,5
Postprandial glucemia (in 2hours after meal intake)
7,5 – 8,0 8,1 – 9,0 >9,0
Glucemia at bedtime 6,0 – 7,0 7,1 – 7,5 >7,5*The level of glucose in capillary blood, mmol/l
**Criteria of decompensate stage:
1. Comatose or precomatose status are present.
Duration of DM
1. Stabile (glucose level fluctuation is under 4.4-5.5 mmol/l during the day and
comatose or precomatose status are absent).

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 33/59
2. Labile (glucose level fluctuation is over 4.4-5.5 mmol/l during the day or
comatose and precomatose status are present).
Mechanism of formulation of diagnosis is shown in table 6.
Table 6. Formulation of diagnosis
Disease Peculiarity Type, stage or degree
Diabetes
mellitus
type
or as a result of
- 1
- 2- or to show a cause (in a case of another types of DM)
degree of severity - mild
- moderate
- severe
stage - compensation
- subcompensation
- decompensationdiabetic microangiopathy - nephropathy (stage)
- retinopathy (stage on each eye)
- angiopathy of lower extremities (stage)
diabetic neuropathy - peripheral
- autonomic (type)
- central
diabetic macroangiopathy - ischemic heart disease (type)
- heart failure (stage according NYHA)
- angiopathy of lower extremities (stage)syndrome of diabetic foot - ischemic
- neuropathic
- mixed
arterial hypertension degree
dyslipidemia in a case of presence
concomitant diseases
Example of diagnosis.
Diabetes mellitus type 1, severe degree, stage of subcompensation. Diabetic
peripheral neuropathy. Diabetic preproliferative retinopathy. Diabetic nephropathy IVstage. Secondary arterial hypertension, II stage, moderate degree.
Chronic (long – term) complications
The long-term degenerative changes in the blood, vessels, the heart, the kidneys,
the nervous system, and the eyes as responsible for the most of the morbidity and
mortality of DM. There is a causal relationship and the level of the metabolic control.
Classification of chronic (long-term) complications of DM
I. Diabetic angiopathy:
1. Microangiopathy:
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 34/59
1) retinopathy;
2) nephropathy;
3) angiopathy of lower extremities.
2. Macroangiopathy:
1) ischemic heart disease;
2) angiopathy of lower extremities.
II. Diabetic neuropathy.
1) peripheral;
2) visceral (autonomic);
3) central.
Diabetic retinopathyDibetics need careful ophthalmologic examination (at least yearly) by
ophthalmologist experienced with diabetes.
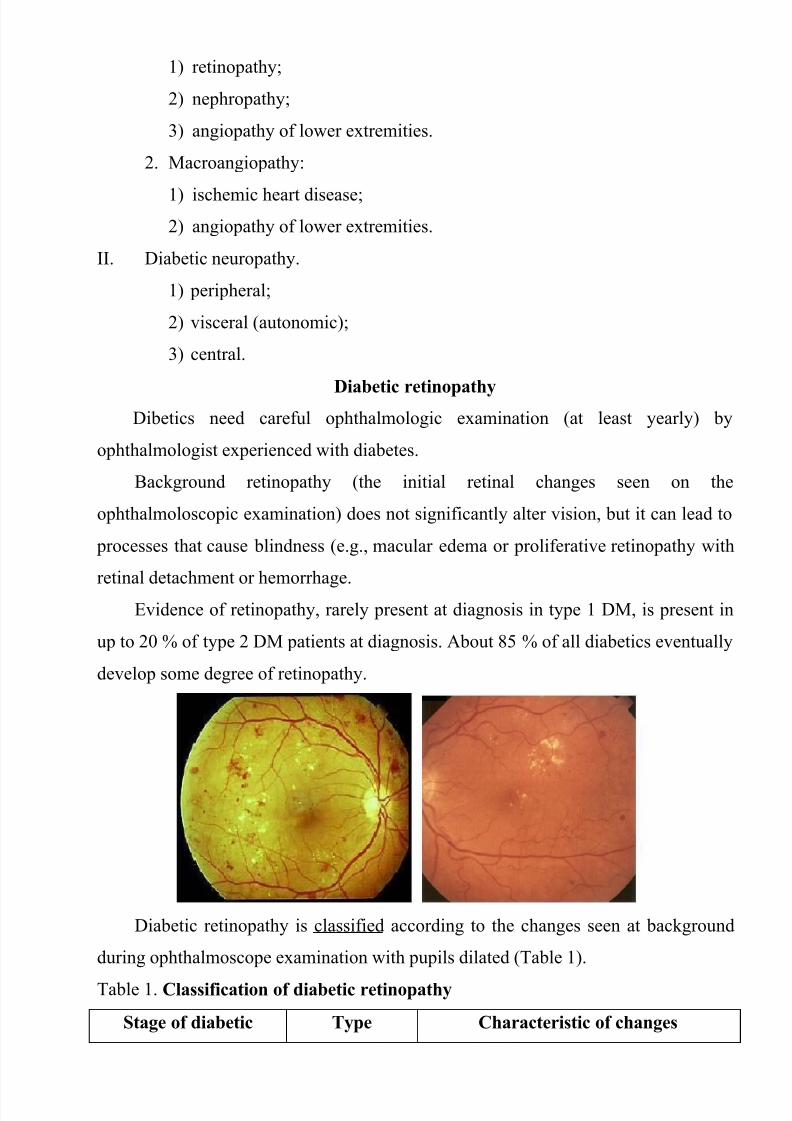
Background retinopathy (the initial retinal changes seen on the
ophthalmoloscopic examination) does not significantly alter vision, but it can lead to
processes that cause blindness (e.g., macular edema or proliferative retinopathy with
retinal detachment or hemorrhage.
Evidence of retinopathy, rarely present at diagnosis in type 1 DM, is present in
up to 20 % of type 2 DM patients at diagnosis. About 85 % of all diabetics eventually
develop some degree of retinopathy.
Diabetic retinopathy is classified according to the changes seen at background
during ophthalmoscope examination with pupils dilated (Table 1).
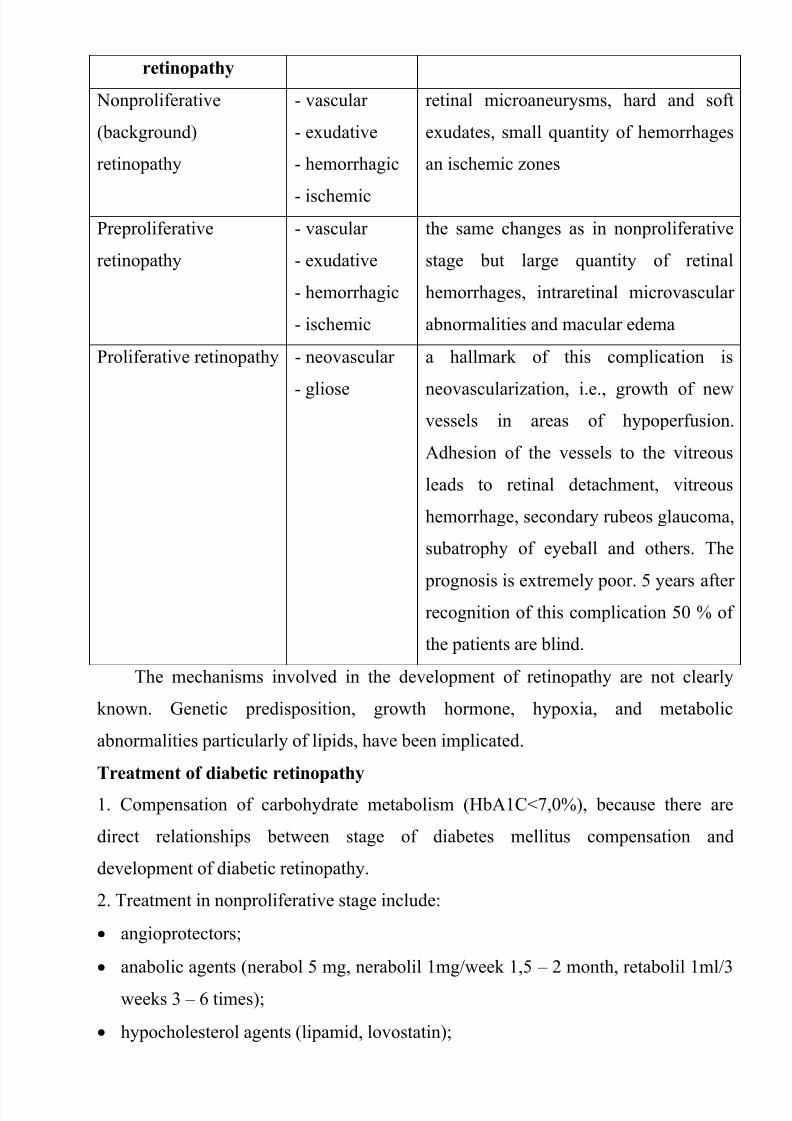
Table 1. Classification of diabetic retinopathy
Stage of diabetic Type Characteristic of changes
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 35/59
retinopathy
Nonproliferative
(background)
retinopathy
- vascular
- exudative
- hemorrhagic
- ischemic
retinal microaneurysms, hard and soft
exudates, small quantity of hemorrhages
an ischemic zones
Preproliferative
retinopathy
- vascular
- exudative
- hemorrhagic
- ischemic
the same changes as in nonproliferative
stage but large quantity of retinal
hemorrhages, intraretinal microvascular
abnormalities and macular edema
Proliferative retinopathy - neovascular
- gliose
a hallmark of this complication is
neovascularization, i.e., growth of newvessels in areas of hypoperfusion.
Adhesion of the vessels to the vitreous
leads to retinal detachment, vitreous
hemorrhage, secondary rubeos glaucoma,
subatrophy of eyeball and others. The
prognosis is extremely poor. 5 years afterrecognition of this complication 50 % of
the patients are blind.
The mechanisms involved in the development of retinopathy are not clearly
known. Genetic predisposition, growth hormone, hypoxia, and metabolic
abnormalities particularly of lipids, have been implicated.
Treatment of diabetic retinopathy
1. Compensation of carbohydrate metabolism (HbA1C<7,0%), because there are
direct relationships between stage of diabetes mellitus compensation and
development of diabetic retinopathy.
2. Treatment in nonproliferative stage include:
angioprotectors;
anabolic agents (nerabol 5 mg, nerabolil 1mg/week 1,5 – 2 month, retabolil 1ml/3
weeks 3 – 6 times);
hypocholesterol agents (lipamid, lovostatin);
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 36/59
antioxydative therapy (emoxipin, trental);
vitamins B ,A, E, PP;
anticoagulants.
3. Laser photocoagulation (local, focal, panretinal), criocoagulation or vitrectomy
with endolazercoagulation, which have to performed by ophthalmologist in
preproliferative and proliferative stage of retinopathy.
1) nonproliferative retinopathy:
Diabetic nephropathy
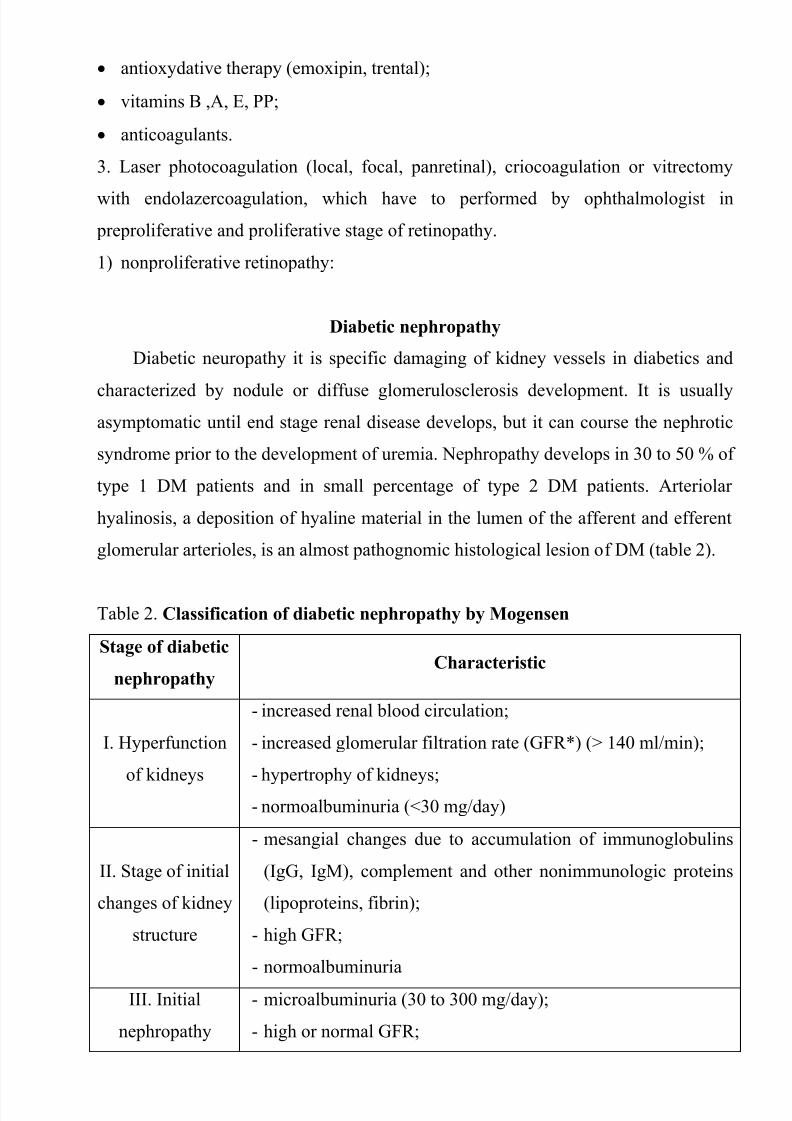
Diabetic neuropathy it is specific damaging of kidney vessels in diabetics and
characterized by nodule or diffuse glomerulosclerosis development. It is usually
asymptomatic until end stage renal disease develops, but it can course the nephrotic
syndrome prior to the development of uremia. Nephropathy develops in 30 to 50 % of
type 1 DM patients and in small percentage of type 2 DM patients. Arteriolar
hyalinosis, a deposition of hyaline material in the lumen of the afferent and efferent
glomerular arterioles, is an almost pathognomic histological lesion of DM (table 2).
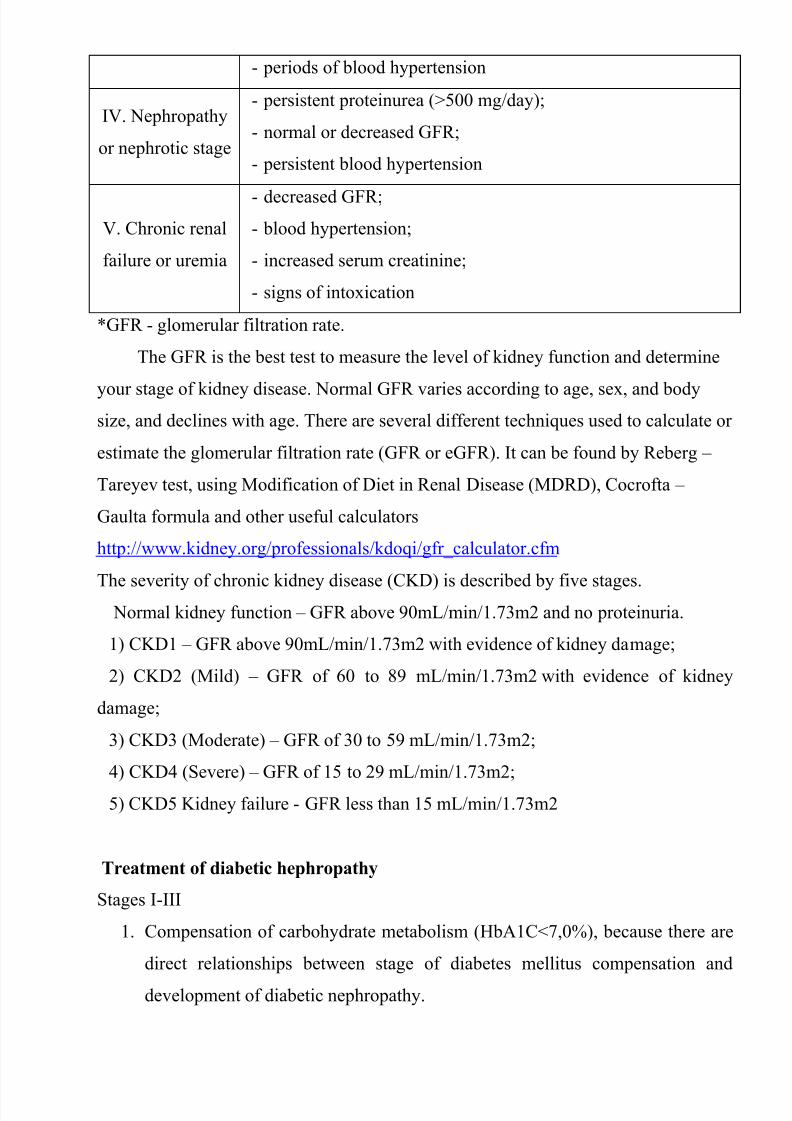
Table 2. Classification of diabetic nephropathy by Mogensen
Stage of diabetic
nephropathyCharacteristic
I. Hyperfunction
of kidneys
- increased renal blood circulation;
- increased glomerular filtration rate (GFR*) (> 140 ml/min);
- hypertrophy of kidneys;
- normoalbuminuria (<30 mg/day)
II. Stage of initial
changes of kidney
structure
- mesangial changes due to accumulation of immunoglobulins
(IgG, IgM), complement and other nonimmunologic proteins
(lipoproteins, fibrin);
- high GFR;
- normoalbuminuria
III. Initial
nephropathy
- microalbuminuria (30 to 300 mg/day);
- high or normal GFR;
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 37/59
- periods of blood hypertension
IV. Nephropathy
or nephrotic stage
- persistent proteinurea (>500 mg/day);
- normal or decreased GFR;
- persistent blood hypertension
V. Chronic renal
failure or uremia
- decreased GFR;
- blood hypertension;
- increased serum creatinine;
- signs of intoxication
*GFR - glomerular filtration rate.
The GFR is the best test to measure the level of kidney function and determine
your stage of kidney disease. Normal GFR varies according to age, sex, and bodysize, and declines with age. There are several different techniques used to calculate or
estimate the glomerular filtration rate (GFR or eGFR). It can be found by Reberg –
Tareyev test, using Modification of Diet in Renal Disease (MDRD), Cocrofta –
Gaulta formula and other useful calculators
http://www.kidney.org/professionals/kdoqi/gfr_calculator.cfm
The severity of chronic kidney disease (CKD) is described by five stages. Normal kidney function – GFR above 90mL/min/1.73m2 and no proteinuria.
1) CKD1 – GFR above 90mL/min/1.73m2 with evidence of kidney damage;
2) CKD2 (Mild) – GFR of 60 to 89 mL/min/1.73m2 with evidence of kidney
damage;
3) CKD3 (Moderate) – GFR of 30 to 59 mL/min/1.73m2;
4) CKD4 (Severe) – GFR of 15 to 29 mL/min/1.73m2;
5) CKD5 Kidney failure - GFR less than 15 mL/min/1.73m2
Treatment of diabetic hephropathy
Stages I-III
1. Compensation of carbohydrate metabolism (HbA1C<7,0%), because there are
direct relationships between stage of diabetes mellitus compensation and
development of diabetic nephropathy.
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 38/59
2. ACE-inhibitors or ARA in suppressive doses in patients with normal blood
pressure and therapeutic while it more than 130/80 mm.Hg. (contraindicated
during pregnancy).
3. Correction of dyslipedemia (while present).
4. Moderate restriction of animal protein in diet (≤ 1gr/1 kg of patient’s weight).
Stage IV
1-3 - as in stage I-III.
4. Restriction of animal protein in diet (≤ 0,8gr/1 kg of patient’s weight).
5. Correction of secondary anemia.
Stage V
1-5 – as in stage IV.6. Correction of electrolyte’s level: potassium, calcium, phosphorus.
7. Enterosorbtion.
Terminal stage
1. Extracorporal renal replacement therapy: hemodialysis, peritoneal dialysis.
2. Transplantation of kidney.
Indications for extracorporal renal replacement therapy:
- GFR< 15 ml/min;
- serum potassium > 6,5 mmol/l;
- severe hyperhydration with risk of lung edema development;
- increasing of protein – energy insufficiency.
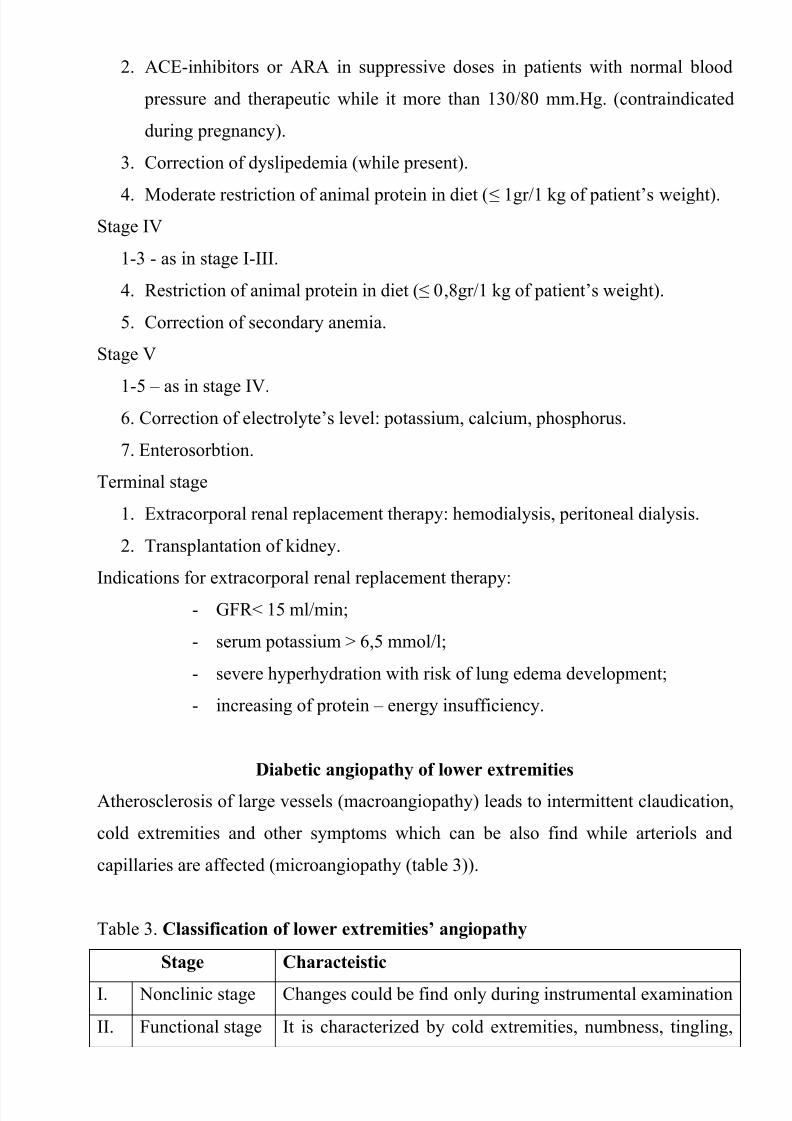
Diabetic angiopathy of lower extremities
Atherosclerosis of large vessels (macroangiopathy) leads to intermittent claudication,
cold extremities and other symptoms which can be also find while arteriols and
capillaries are affected (microangiopathy (table 3)).
Table 3. Classification of lower extremities’ angiopathy
Stage Characteistic
I. Nonclinic stage Changes could be find only during instrumental examination
II. Functional stage It is characterized by cold extremities, numbness, tingling,

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 39/59
pain during physical examination
III. Organic stage It is characterized by trophyc changes: dry skin, hypo- or
atrophy of muscles, ulcers, gangrene
Treatment of diabetic angiopathy of lower extremities
Patient have to be educated in foot care; early detection of risk factors, ulcers,
infections, calluses, exposed nails, diminished pulses, deformities
Medicaments therapy
1. Compensation of carbohydrate metabolism (HbA1C<7,0%).
2. Smoking.
3. Correction of hypertension.4. Treatment of dislipidemia.
5. Decreasing of extremities ischemia:
- vasodilators;
- anticoagulants and antiaggregative preparations (under the control of
coagulogram and retina).
6.
Antibacterial therapy (in a presence of ulcers).Surgical therapy (in specialized department).
Peculiarities of ischemic heart disease in diabetics
1. Cardiovascular changes tend to occur earlier in patients with DM when compared
with individuals of the same age.
2. Frequency of myocardial infarction (MI) and mortality is higher in diabetics than
that in nondiabetics of the same age.
3. The prognosis is even worse if ketoacidosis, or other complications of DM are
present.
4. Diabetic patients have more complications of MI (arrhythmias, cardiogenic shock
and others) than nondiabetic ones.
5. Often can observe atypical forms (without pain).
6. Male: female = 1:1 (nondiabetics = 10:1).
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 40/59
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 41/59
- involvement of the bowel (It is characterized by diarrhea (mostly at night time,
postural diarrhea), constipation, malabsorption and fecal incontinence;
2) urinary tract:
- neurogenic vesicle dysfunction (It is characterized by insidious onset and
progression of bladder paralysis with urinary retention.);
3) sexual disorders:
- retrograde ejaculation (which is caused by dysfunction of the pelvic autonomic
nervous system);
- impotence, and sometimes decreased libido;
4) cardiovascular system (diabetic cardioneuropaty):
-
orthostatic hypotension (It is characterized by dizziness, vertigo, faintness, andsyncope upon assumption of the upright posture and is caused by failure of
peripheral arteriolar constriction);
- tachycardia (but it does not occur in response to hypotension because of
sympathetic involvement).
Treatment of diabetic neuropathy
1. Compensation of carbohydrate metabolism (HbA1C<7,0%).
2. Sulfate-containing preparations: ɑ- lipoid acid (dialipon, berlition, tiogama-
turbo), unitiol, sodium thiosulfate, gabapentyn.
3. Vitamin B-complex.
4. Vasodilators.
5. Symptomatic therapy (, non-steroid anti-inflammatory drugs, analgetics, etc).
6. Inhibitors of aldose reductase (sorbinil), multivitamins, phenytoin,
carbamazepin (Tegretol), amitriptyline.
7. In patients with encephalopathy nootropil, piracetam have to be prescribed/
8. Physiotherapy (inductotermia, magnitolazerotherapy and others).
Diabetic foot
Appearance of diabetic foot is caused by a combination of vascular
insufficiency, neuropathy, and infection.
Diabetic foot is divided on three types:

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 42/59

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 43/59
The treatment of patients with DM is very important and may be difficult
because of problems in achieving of normal glucose control. Because there is good
evidence that hyperglycemia conveys risks for all of the common long-term
complications of DM, which are the major cases of excess morbidity and mortality in
diabetics.
The main principles of DM therapy.
1. Maintenance of metabolic status at normal level or as close to normal as possible
(especially blood glucose and lipid concentration). Achievement of DM
compensation.
2. Achievement and maintenance of normal or reasonable body weight.
3.
Maintenance (preservation) of working capacity.4. Prophylaxis of acute and chronic complications.
Treatment of DM has to be individualized and includes such methods:
1. Diet.
2. Oral hypoglycemic agents or insulin (indications for each vary with the type of
DM and severity of the disease).
3. Exercise program.
4. Phytotherapy (plant’s therapy).
5. Nontraditional methods of treatment.
6. Education of the patients about the nature of the disease, the importance of its
control, all aspects of self-management and routine practices to minimize the
development or severity of the diabetes’ complications. Physician has to educate,
motivate and monitor progress. Patient must understand the importance of
differing life-style.
Diet is the keystone of the treatment of the DM.
The main principles of diet.
1. Balanced diet (diet should include physiologic meal components: carbohydrate
comprises 50 – 60 % of total calories, fat – 24 – 25 % and protein – 16 – 15 %).
2. Normal-calorie diet in patients with type 1 DM (35-50 kcal/kg of ideal weight
(weight = height – 100)) and low-calorie diet in obese persons (mostly in patients
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 44/59
with type 2 DM (20 – 25 kcal/kg of ideal weight)). We try to decrease weight in
obese patients on 1-2 kg/month by such diet. (Obesity leads to insensitivity of
muscle and adipose tissue to insulin, presumable as the result of decreased binding
of insulin to its plasma membrane receptor. Hyperglycemia is the face of
increased insulin secretion and hyperlipoproteinemia are secondary to this
abnormality. The defect in insulin binding and secretion is corrected by weight
reduction.)
3. Regimen has to be consist of 4 – 5 – 6 small feedings a day. (The most frequent
regimen consists of 4 feedings a day, in which breakfast comprises 30 % of total
calories, dinner – 40 %, lunch – 10 %, supper – 20 %. Sometimes patients need
second breakfast (when they have a tendency to develop hypoglycemia). In suchcase it comprises15 % of the total calories and we decrease the quantity of calories
of the first breakfast and dinner).
4. Exclusion of high-calorie carbohydrates (sugar, biscuits, white bread, alcohol).
5. Increasing the quantity of high fiber-containing foods (fruits (exclusion: banana,
grapes), vegetables, cereal grains, whole grain flours, bran. Patients need 40 g
fibers per day.
6. Limiting of meat fat, butter, margarine in diet, decrease red and brown meats,
increase poultry and fish, encourage skim milk-based cheeses. Should be used
skim or low-fat milk, not more than 2 – 3 eggs weekly.
7. Alcohol should be avoided as much as possible because it constitutes a source of
additional calories, it may worsen hyperglycemia, and it may potentiate the
hypoglycemic effects of insulin and oral hypoglycemic agents.
Sometimes (mostly in obese diabetics) achievement and maintenance of normal body
weight may be enough to eliminate the need for oral hypoglycemic agents or insulin.
So, the diet should be planned in such way that the patient can follow it for the rest of
his or her life without starving or becoming malnourished.
Oral hypoglycemic agents.
Inadequate control of hyperglycemia by the diet and exercises interventions
suggests the need for a good glucose-lowering agent.
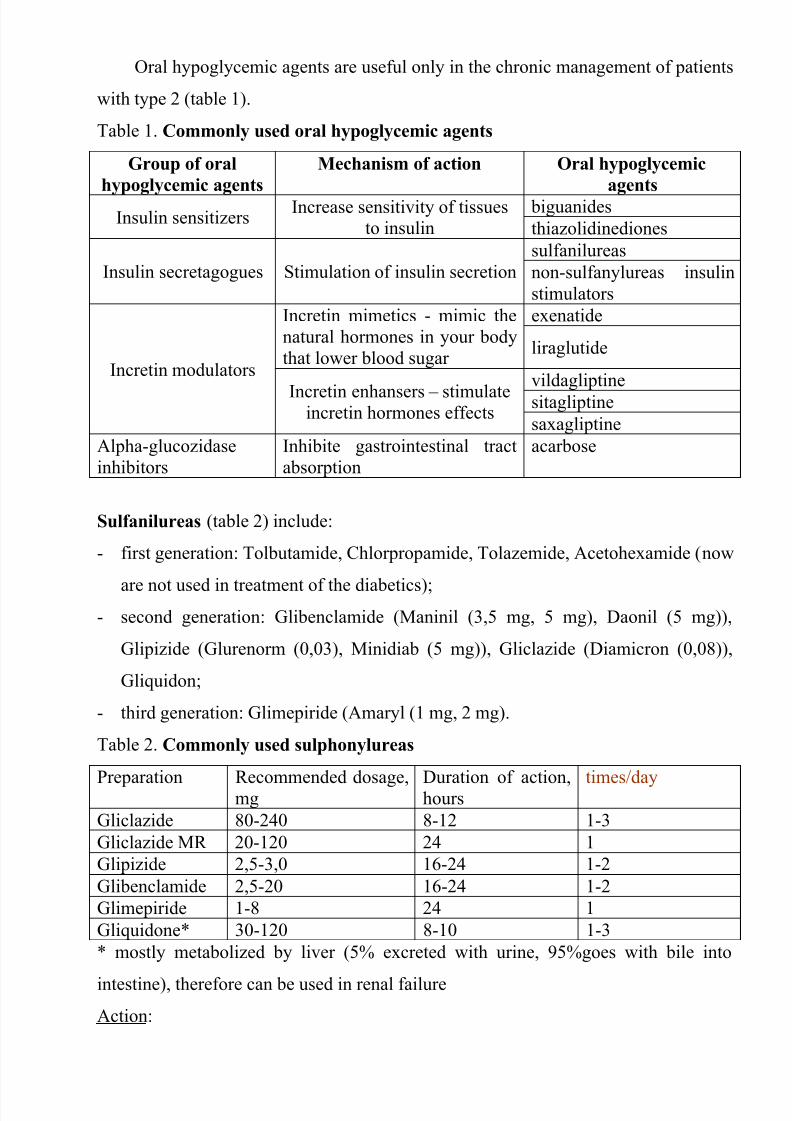
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 45/59
Oral hypoglycemic agents are useful only in the chronic management of patients
with type 2 (table 1).
Table 1. Commonly used oral hypoglycemic agents
Group of oral
hypoglycemic agents
Mechanism of action Oral hypoglycemic
agents
Insulin sensitizersIncrease sensitivity of tissues
to insulin
biguanides
thiazolidinediones
Insulin secretagogues Stimulation of insulin secretion
sulfanilureas
non-sulfanylureas insulin
stimulators
Incretin modulators
Incretin mimetics - mimic the
natural hormones in your body
that lower blood sugar
exenatide
liraglutide
Incretin enhansers – stimulateincretin hormones effects
vildagliptine
sitagliptine
saxagliptine
Alpha-glucozidase
inhibitors
Inhibite gastrointestinal tract
absorption
acarbose
Sulfanilureas (table 2) include:
- first generation: Tolbutamide, Chlorpropamide, Tolazemide, Acetohexamide (now
are not used in treatment of the diabetics);- second generation: Glibenclamide (Maninil (3,5 mg, 5 mg), Daonil (5 mg)),
Glipizide (Glurenorm (0,03), Minidiab (5 mg)), Gliclazide (Diamicron (0,08)),
Gliquidon;
- third generation: Glimepiride (Amaryl (1 mg, 2 mg).
Table 2. Commonly used sulphonylureas
Preparation Recommended dosage,mg Duration of action,hours times/day
Gliclazide 80-240 8-12 1-3
Gliclazide MR 20-120 24 1
Glipizide 2,5-3,0 16-24 1-2
Glibenclamide 2,5-20 16-24 1-2
Glimepiride 1-8 24 1
Gliquidone* 30-120 8-10 1-3
* mostly metabolized by liver (5% excreted with urine, 95%goes with bile into
intestine), therefore can be used in renal failure
Action:
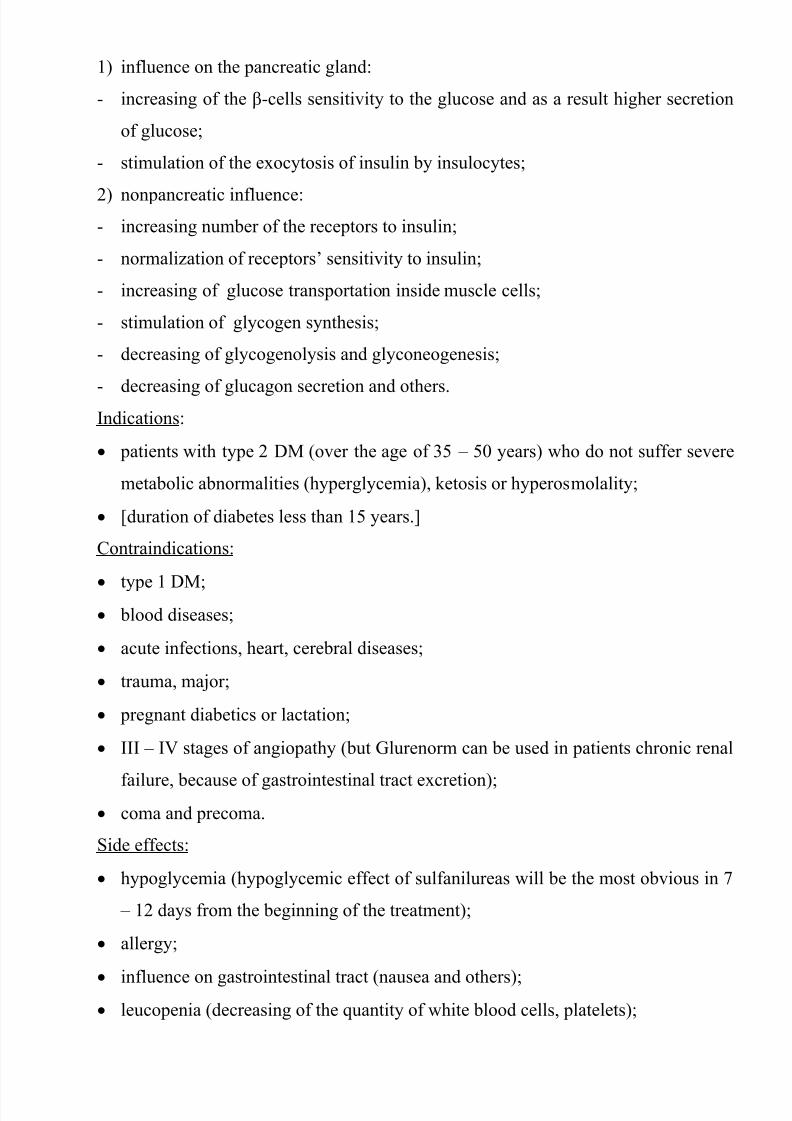
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 46/59
1) influence on the pancreatic gland:
- increasing of the β-cells sensitivity to the glucose and as a result higher secretion
of glucose;
- stimulation of the exocytosis of insulin by insulocytes;
2) nonpancreatic influence:
- increasing number of the receptors to insulin;
- normalization of receptors’ sensitivity to insulin;
- increasing of glucose transportation inside muscle cells;
- stimulation of glycogen synthesis;
- decreasing of glycogenolysis and glyconeogenesis;
-
decreasing of glucagon secretion and others.Indications:
patients with type 2 DM (over the age of 35 – 50 years) who do not suffer severe
metabolic abnormalities (hyperglycemia), ketosis or hyperosmolality;
[duration of diabetes less than 15 years.]
Contraindications:
type 1 DM;
blood diseases;
acute infections, heart, cerebral diseases;
trauma, major;
pregnant diabetics or lactation;
III – IV stages of angiopathy (but Glurenorm can be used in patients chronic renal
failure, because of gastrointestinal tract excretion); coma and precoma.
Side effects:
hypoglycemia (hypoglycemic effect of sulfanilureas will be the most obvious in 7
– 12 days from the beginning of the treatment);
allergy;
influence on gastrointestinal tract (nausea and others); leucopenia (decreasing of the quantity of white blood cells, platelets);

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 47/59
primary or secondary failure. (Primary failure defined as an inadequate response
during the first month of treatment with maximum dosage, occurs in
approximately 5 % of patients. Secondary failure is defined as a recurrence of
hyperglycemia after an initial satisfactory response. Secondary failure may be due
to nonadherence to eihter diet or sulfanilurea therapy, to disease progression, or to
loss of efficacy of the agent.)
Biguanides (table 3):
Metformine (Siofor 500, 850 mg), Adebit, Bufarmin.
(The usual starting dose is 500 mg 12 – hourly with meal increasing gradually to max
1 g 8-hourly.)Table 3 . Commonly used biguanides
Preparation Recommended dosage,
mg
Duration of action,
hours
times/day
metformine 500-3000 8-12 3
Action:
inhibition of gastrointestinal glucose absorption;
decreasing of glyconeogenesis, lipogenesis; enhancing glucose transport into muscle cells;
increasing the quantity of insulin’s receptors;
stimulation of anaerobic and partly aerobic glycolis;
anorrhexogenic effects.
Indications:
Obese patients with type 2 DM, with middle severity of the disease without ketosis.They can be used with the combination of sulfanilureas when sulfonylureas alone
have proved inadequate to treat DM.
Contraindications:
heart and lung disease with their insufficiency (chronic heart and lung failure);
status with hypoxemia;
acute and chronic liver and kidney diseases with decreased function;
pregnant diabetics, lactation;
old age;
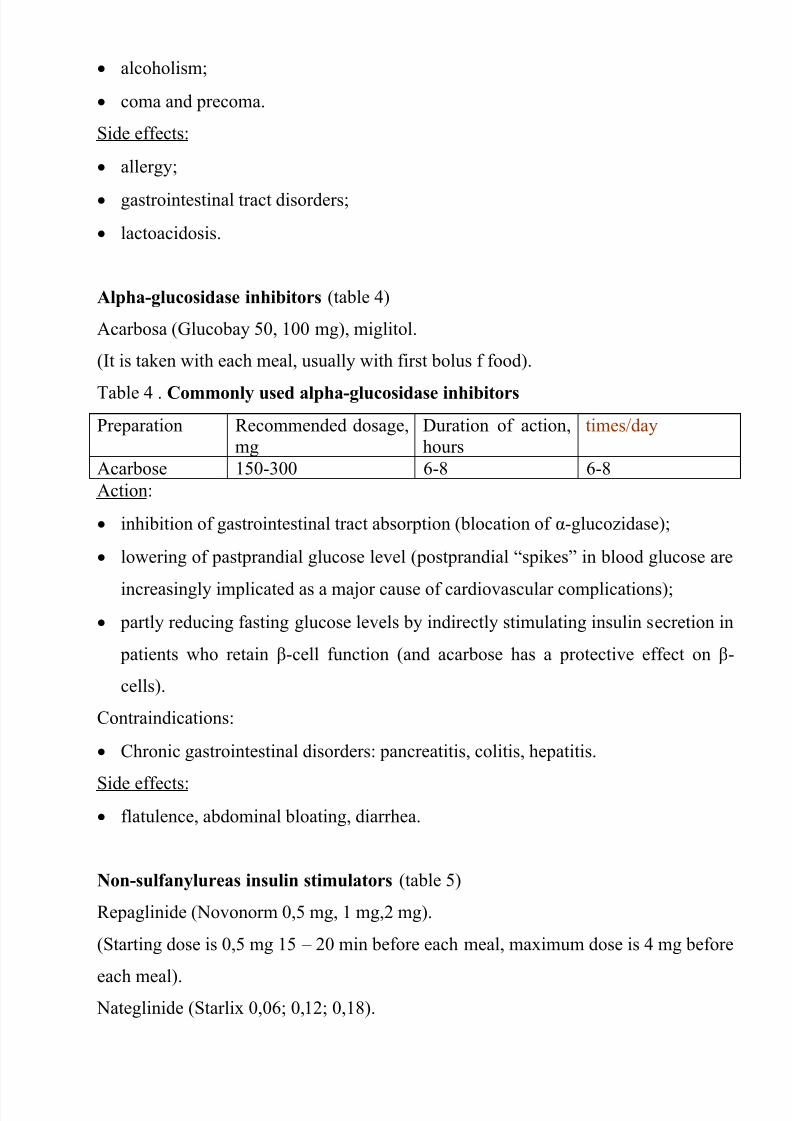
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 48/59
alcoholism;
coma and precoma.
Side effects:
allergy;
gastrointestinal tract disorders;
lactoacidosis.
Alpha-glucosidase inhibitors (table 4)
Acarbosa (Glucobay 50, 100 mg), miglitol.
(It is taken with each meal, usually with first bolus f food).
Table 4 . Commonly used alpha-glucosidase inhibitors
Preparation Recommended dosage,
mg
Duration of action,
hours
times/day
Acarbose 150-300 6-8 6-8
Action:
inhibition of gastrointestinal tract absorption (blocation of α-glucozidase);
lowering of pastprandial glucose level (postprandial “spikes” in blood glucose are
increasingly implicated as a major cause of cardiovascular complications);
partly reducing fasting glucose levels by indirectly stimulating insulin secretion in
patients who retain β-cell function (and acarbose has a protective effect on β-
cells).
Contraindications:
Chronic gastrointestinal disorders: pancreatitis, colitis, hepatitis.
Side effects:
flatulence, abdominal bloating, diarrhea.
Non-sulfanylureas insulin stimulators (table 5)
Repaglinide (Novonorm 0,5 mg, 1 mg,2 mg).
(Starting dose is 0,5 mg 15 – 20 min before each meal, maximum dose is 4 mg before
each meal). Nateglinide (Starlix 0,06; 0,12; 0,18).

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 49/59
Table 5 . Commonly used non-sulfanylureas insulin stimulators
Preparation Recommended dosage,
mg
Duration of action,
hours
times/day
Repaglinide 0,5-16 3-4 3-4
Nateglinide 120-480 3-4 3-4
Action:
these drugs stimulates insulin production at meal times;
very rapidly absorbed from the intestine and metabolized in liver;
plasma half0life is less than 1 hour/
Indications:
can be used in elderly with type 2 DM (due to short half-life) and in renal
impairment (because it is metabolized in liver).
Side effects:
hypoglycemia;
transient elevation of liver enzymes;
rash;
visual disturbances.
Thiozolidindiones (table 6)
Pioglitazon (Actos, Pionorm) Dose in 1 tabl. 0,015; 0,03; 0,045.
Rosiglitazon is not used due to side effects
Table 6 . Commonly used thiozolidindiones
Preparation Recommended dosage,
mg
Duration of action,
hours
times/day
pioglitozon 15-45 16-24 1
Action of thiozolidindiones
Agonist to the receptors of the nucleus PPAR γ of the fat, muscle tissues and the
liver;
Increasing of the glucose passage to these tissues;
Increasing of insulin synthesis in the b-cells;
Increasing of the insulas amount;
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 50/59
Increasing of glycogen synthesis in the liver;
Decreasing of gluconeogenesis;
Decreasing of triglycerides;
Indications to thiozolidindiones usage
DM type 2, when diet and exercises are no effective;
Using with sulfanilureas, biguanides, insulin in case of their insufficient efficacy
Contraindications to thiozolidindiones usage
Diabetic coma, precoma, ketoacidosis;
Acute and chronic diseases of the liver;
Heart failure;
Pregnancy, lactation;
Children, teenagers;
Allergic reactions to the drug.
Side effects of thiozolidindiones
Hypoglycemic conditions (rarely);
Peripheral edema;
Anemia;
Obesity.
Incretin mimetics
Exenatide (Byetta), liraglutide (Victoza) – subcutaneous injection daily.
Action:
“incretin effect” is attributed to the insulinotropic action of gut hormones, specifically
glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide
(GIP).
Allows pancreas to release insulin. This drug lowers blood sugar levels only
when they rise too high.
Prevents the pancreas from giving out glucagon.
Helps to slow the rate at which stomach empties after eating. This may make
feel less hungry and more satisfied after a meal.

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 51/59
Indications:
can be used in type 2 DM patients.
Side effects:
nausea (is usually worse during the first few weeks of treatment and gets better
over time);
diarrhea;
stomch pain;
pancreatitis;
weight loss.
Incretin enhansers (table 7)
Onglyza 5 mg
Galvus 50 mg
Yanuvia 25 mg, 50 mg, 100 mg
Table 7 . Commonly used inhibitors of DPP IV
Preparation Recommended dosage,
mg
Duration of action,
hours
times/day
saxagliptine
(onglyza)
5 24 1
vildagliptine
(galvus)
50-100 10-12 2
sitagliptine(yanuvia)
100-200 16-24 2
Action:
Suppress the degradation of a variety of bioactive peptides, including GLP-1,
thereby extending their period of action by inhibing of dipeptydpeptidase IV (DPP-
IV).
Indications:
can be used in type 2 DM patients.
Side effects:
nasopharyngitis;
mild headache;

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 52/59
cough.
Combined preparates
Glibomet consists of Maninil 2,5 mg and Siofor 400 mg
Plant’s therapy (phytotherapy).
1) hypoglycemic action;
2) treatment of chronic diabetics complications;
3) influence on the immune reactivity.
Insulin
Insulin has been available for the treatment of patients with DM since 1921. Formany years, the most commonly used preparations consisted of a combination of
pancreatic bovine and porcine insulin. Contamination of small amounts (to 2 %) of
other pancreatic hormones, such as glucagon, proinsulin, C peptide, somatostatin,
and pancreatic polypeptide, was the rule. Subsequent purification have yielded
purer (almost 100 %) preparations of beef insulin, pork insulin, or combination of
two, with a biologic activity of 26 to 28 units/mg as compared to 22 to 24 units/mg
for the older preparations. The most recent development has been the preparation
of biosynthetic human insulin. Two procedures have been utilized. In the first,
alanine in the 30 position of the B chain of pork insulin is substituted
enzymatically by threonine. The resulting “humanized pork” insulin has the amino
acid sequence of human insulin (Actrapid, Monotard made by Novo-Nordisk). The
second approach involves synthesis by Escherichia coli (E. Coli) by recombinant
DNA technology. The hormone can be produced by single fermentation in which
proinsulin is made first and then cleaved into insulin and C peptide, or by separate
fermentation in which A and B peptide are synthesized first and then joined into
insulin (Humulin, Lilly). Synthetic human insulin does not have great advantages
over purified pork insulin, except for slightly faster onset of the action.
Hypokalemia, C-peptide suppression, and secretion of epinephrine, cortisol,
growth hormone and prolactine may be reduced with human insulin. The synthetic
hormone has the potential to be less antigenic than the pork insulin. Causes of

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 53/59
potential use for human insulin include resistance to exogenous insulin, beef or
pork insulin allergy, lipodystrophy, gestation diabetes. Anticipated short-term
administration, and newly diagnosed young diabetic patients.
A multitude of insulin preparations and insulin analogues are available, and the
major difference in their duration of action (Table 8, 9). Figures on onset, peak and
duration of action are applicable to normal non-insulin-treated subjects.
Only short-acting insulins should be given intravenously; all the types can be
injected only subcutaneously.
Table 8. Insulin preparations
Group Preparations Onset, h Peak ofaction, h Duration ofaction, h
Short-acting Humodar R
Actrapid HM
Iletin
0,5 – 1,0 1 – 4 5 – 8
Intermediate-
acting
Humodar B
Protaphan HM
Humulin L
Monotard MC
1 - 3 6 – 12 18 – 26
Long-acting Ultratard HMUltralong 4 - 8 14 – 20 20 – 36
Combined
preparations
Humodar C-
15
Mixtard 30
HMMonodar C-30
0,5 Depends on quantity of
components
Table 9. Insulin analogues
Group Preparations Onset, h Peak of
action, h
Duration of
action, h
Ultra-short- acting
(insulin analogues
for rapid onset of
insulin action)
Humalog
Hovorapid
Epaidra
5 - 10
min.
0,5 – 2,5 3 - 4
Long-acting inulin Lantus
Levemir
Detmir
1 nonpeaked 24
Indications for insulin therapy

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 54/59
1. All patients with type 1 DM.
2. Some patients with type 2 DM:
uncontrolled diabetes by diet or oral hypoglycemic agents;
ketoacidosis, coma;
acute and chronic liver and kidneys disease with decreased function;
pregnancy and lactation;
II – IV stages of angiopathy;
infection diseases;
acute heart and cerebral diseases;
surgery.
Initiation and modification of insulin therapy to achieve diabetic control.
The daily insulin requirement in patients:
- on the first year of the disease is 0,3 – 0,5 unite of insulin per kilogram of body
weight (0,5 – if the patient with ketosis or DKA);
- on the next years is 0,6 – 0,8 – 1,0 unite/ kg of body weight. We can use
traditional or multiple component insulin program. The last is better. It using three
or four shots of short-acting insulin (1/3 of total daily dose) plus intermediate-
acting (2/3 of total daily dose) insulin daily is started as soon as possible in an
attempt to “rest” the damaged islet cells and help to “induce” a remission
(“honeymoon” phase). Other advantages include the following:
- hypoglycemic reactions may be decreased or prevented because smaller doses of
insulin are needed;- more physiologic match of insulin to meals is achieved.
2/3 of the total daily dose we give before lunch, 1/3 in the evening and then make
correction due to the glucose blood level. Insulin doses should be given 30 minutes
before meals to allow for adequate absorption of regular insulin.
(Other commonly used insulin treatment algorithms:
1. Single prebreakfast injection of intermediate-acting insulin.
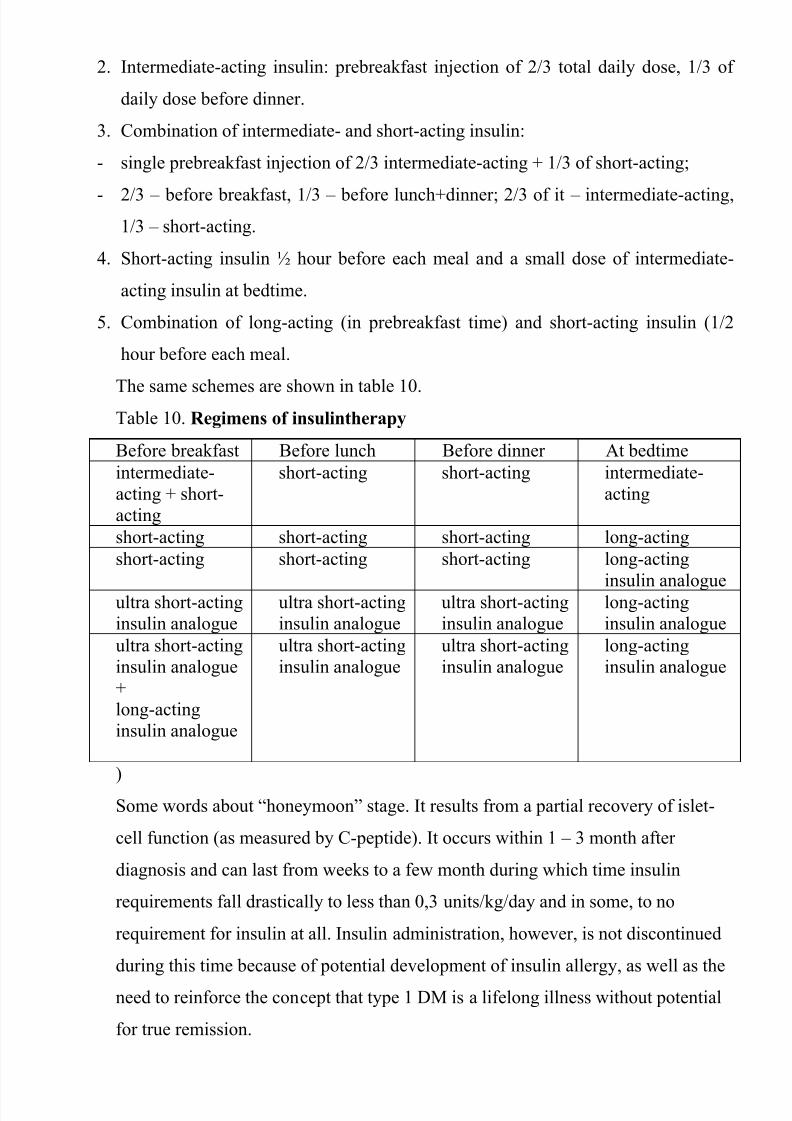
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 55/59
2. Intermediate-acting insulin: prebreakfast injection of 2/3 total daily dose, 1/3 of
daily dose before dinner.
3. Combination of intermediate- and short-acting insulin:
- single prebreakfast injection of 2/3 intermediate-acting + 1/3 of short-acting;
- 2/3 – before breakfast, 1/3 – before lunch+dinner; 2/3 of it – intermediate-acting,
1/3 – short-acting.
4. Short-acting insulin ½ hour before each meal and a small dose of intermediate-
acting insulin at bedtime.
5. Combination of long-acting (in prebreakfast time) and short-acting insulin (1/2
hour before each meal.
The same schemes are shown in table 10.Table 10. Regimens of insulintherapy
Before breakfast Before lunch Before dinner At bedtime
intermediate-
acting + short-
acting
short-acting short-acting intermediate-
acting
short-acting short-acting short-acting long-acting
short-acting short-acting short-acting long-acting
insulin analogueultra short-acting
insulin analogue
ultra short-acting
insulin analogue
ultra short-acting
insulin analogue
long-acting
insulin analogue
ultra short-acting
insulin analogue
+
long-acting
insulin analogue
ultra short-acting
insulin analogue
ultra short-acting
insulin analogue
long-acting
insulin analogue
)
Some words about “honeymoon” stage. It results from a partial recovery of islet-
cell function (as measured by C-peptide). It occurs within 1 – 3 month after
diagnosis and can last from weeks to a few month during which time insulin
requirements fall drastically to less than 0,3 units/kg/day and in some, to no
requirement for insulin at all. Insulin administration, however, is not discontinued
during this time because of potential development of insulin allergy, as well as the
need to reinforce the concept that type 1 DM is a lifelong illness without potential
for true remission.
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 56/59
Some particularities of insulin therapy:
1) insulin acts faster when is administrated intravenously;
2) subcutaneous and intramuscular absorption of insulin is decreased in the
dehydrated or hypotensive patients;
3) it is necessary to change the insulin injection site (because the absorption is more
rapid from the new sites);
4) the most rapid absorption from the abdomen;
5) exercise accelerates insulin absorption (before planned exercise program patient
has to decrease insulin dose or take more caloric diet).
Insulin is stable at room temperature, but refrigeration of the vial while not in useis recommended.
Future directions in improving glycemic control:
nasal insulin preparations;
pancreatic transplantation;
islet replacement therapy;
genetically engineered pseudo-beta-cells.
Side effects (complications) of insulin therapy.
1. Hypoglycemia.
This complication represents insulin excess and it can occur at any time (frequently
at night (common symptom: early-morning headache)).
Precipitating factors:
irregular ingesting of food;
extreme activity;
alcohol ingestion;
drug interaction;
liver or renal disease;
hypopituitarism;
adrenal insufficiency.
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 57/59
Treatment (preventing coma):
to eat candy or to drink sweet orange juice (when the symptoms develop);
to receive intravenous glucose;
1 mg of glucagon administrated subcutaneously;
gradual reduction of insulin dose in future.
Somogyi effect (Somogyi phenomenon, rebound effect)
It is caused by overinsulinization: hyperglycemia proceeded by insulin – induced
hypoglycemia. Hypoglycemia causes an increase in the secretion of the
counterregulatory hormones (glucagon, epinephrine, cortisol, growth hormone),
which inhibit insulin secretion and increase glucose output by the liver (as a result
of the stimulation of glucogenolysis and glucogenesis).
Treatment: gradual reduction of insulin dose.
Dawn phenomenon
Many patients with type I DM demonstrate an early morning (4 – 8 a.m.) rise in
glucose levels, because of activation of counterregulatory hormones. It may be
confused with the Somogyi phenomenon. Sampling of glucose levels throughout
the night might help differentiate the two conditions.Treatment: some have recommended an earlier injection in the morning (5 – 6
a.m.), and most suggest a late evening (before bedtime) injection of intermediate-
acting insulin.
2. Allergic reactions.
These include burning and itching at the site of insulin injection; skin rash;
vasculaties; purpura and anaphylactic reaction.
Treatment:
antihistamines;
changing of standard insulin to pure pork insulin or to human insulin;
in extreme cases – glucocorticoids.
3. Insulin resistance.
Clinical status characterized by insulin resistance:
obesity;
therapy with oral contraceptives;
8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 58/59
glucocorticoid therapy;
acromegaly;
Cushing’s syndrome;
acanthosis nigricans;
chronic liver or renal disease.
Non-true insulin resistance may be caused by long-time injections of insulin into
the one site.
4. Lipodystrophy
It is atrophy or hypertrophy of the adipose tissue, which occur at the site of insulin
injection.
Treatment:
changing the site of injection;
the usage of human insulin.
Exercise program.
Exercise is an excellent adjunct to diet therapy, but it is very ineffective when
used as the sole weight-reducing modality.
Exercises must be clearly planned and depend on patient’s abilities and the
physical condition, exclusion of the competition’s elements.
Exercises may be valuable adjunct to the management of the DM by:
- lowering blood glucose concentration;
-
decreasing insulin requirements;- potentiation the beneficial effects of diet and other therapy.
To prevent hypoglycemia, patients should carefully monitor glucose level and
taking of insulin. Mostly they need to reduce the insulin dosage by 20 – 25 % on the
day that strenuous exercises is planned.
Patient’s education.
1) the nature of DM and importance of metabolic control;
2) the principles and importance of good nutrition and reasonable exercise program;

8/13/2019 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) …
http://slidepdf.com/reader/full/10-management-of-patient-with-hypoglycemic-coma-management-of-patient-with 59/59
3) the principles of adequate foot, dental and skin care;
4) treatment of DM during the periods of illness;
5) techniques of insulin administration and measurement of urine and blood glucose
level (if taking insulin);
6) recognition of hypoglycemia, its causes and methods of prevention;
7) the importance of general and specific measures to minimize in the best possible
way diabetic complications and maintain of good overall health.
There are several specialized sanatoriums in Truscavets, Myrgorod, Odessa with
specialized school for diabetics
Literature:
1. Textbook of Endocrinilogy/ edited by prof. Petro M. Bodnar/ Vinnytsya “Nova
Knyha”, 2008 – 496 p.
2. Davidson’s Essentials of Medicine /edited by J. Alastair Innes, Edinburg, UK ,
Elsevier, 2009 – P.329 – 414.
3. The Merck Manual of Diagnosis and Therapy (eighteenth Edition)/ Robert
Berkow and others. – published by Merck Research Laboratories, 2006 – P. 1926 –
2058.
B. Additional.
1. Mohammad Inam Danish Short Textbook of Medical Diagnosis and
Management (Third Edition). – Pakistan, 2002 – 653 p.