12-immunopathology_part_2.pdf
TRANSCRIPT

8/10/2019 12-Immunopathology_Part_2.pdf
http://slidepdf.com/reader/full/12-immunopathologypart2pdf 1/25

8/10/2019 12-Immunopathology_Part_2.pdf
http://slidepdf.com/reader/full/12-immunopathologypart2pdf 2/25

8/10/2019 12-Immunopathology_Part_2.pdf
http://slidepdf.com/reader/full/12-immunopathologypart2pdf 3/25
Dr. Samir Ayad 3
Etiology:
(1) Genetic factors: - familial incidence
- HLA-DR2 and DR3
(2) Immunological factors:
- deficiency of suppresor T-cells- hyperactive helper T-cells
- abnormal B-cells
(3) Drugs - induced (e.g. hydralazine, procainamide)
(4) Viral infection
(5) Sex hormones (exacerbations in pregnancy)

8/10/2019 12-Immunopathology_Part_2.pdf
http://slidepdf.com/reader/full/12-immunopathologypart2pdf 4/25
Dr. Samir Ayad 4
Mechanism:
(a) Autoimmune disease: antinuclear antibodies
(ANAs) against several nuclear antigens (DNA,
RNA, nucleoproteins) react with nuclei of
damaged cells (cannot penetrate intact cells)
(b) Formation of immune complexes and their
deposition in different tissues
(c) Activation of complement inflammatory lesions
(type III hypersensitivity
)

8/10/2019 12-Immunopathology_Part_2.pdf
http://slidepdf.com/reader/full/12-immunopathologypart2pdf 5/25
Dr. Samir Ayad 5
Antinuclear antibody test, homogenous pattern,fluorescence microscopy
Here is a positive ANA, homogenous or diffuse staining
reflecting antibodies to chromatin, histones, and double-stranded DNA.

8/10/2019 12-Immunopathology_Part_2.pdf
http://slidepdf.com/reader/full/12-immunopathologypart2pdf 6/25
Dr. Samir Ayad 6
Antinuclear antibody test, rim pattern, fluorescencemicroscopy
Sometimes when performing the ANA test, the cells
demonstrate particular patterns of staining rim or peripheralstaining, indicative of AB to double stranded DNA. This is theso-called "rim" pattern that is more characteristic of SLE.

8/10/2019 12-Immunopathology_Part_2.pdf
http://slidepdf.com/reader/full/12-immunopathologypart2pdf 7/25Dr. Samir Ayad 7
Antinuclear antibody test, nucleolar pattern, fluorescencemicroscopy
This is the so-called "nucleolar pattern" of staining in which
the bright fluorescence is seen within the nucleoli of the cells.This pattern is more suggestive of progressive systemicsclerosis.

8/10/2019 12-Immunopathology_Part_2.pdf
http://slidepdf.com/reader/full/12-immunopathologypart2pdf 8/25Dr. Samir Ayad 8
Pathological changes:
(1) Blood vessels:(acute necrotizing vasculitis)
- acute vasculitis of small arteries and arteriolesdue to deposition of immune complexes
- necrosis & fibrinoid deposits within vessel wall
- later, fibrous thickening with luminal narrowing-perivascular lymphocytic infilterate
(2) Heart:
- pericarditis - myocarditis
- endocarditis (Libman-Sacks):
multiple, small, sterile, flat vegetations,
detachable embolization

8/10/2019 12-Immunopathology_Part_2.pdf
http://slidepdf.com/reader/full/12-immunopathologypart2pdf 9/25Dr. Samir Ayad 9
Libman-Sacks endocarditis, gross
Here are flat, pale tan, spreading vegetations over the mitral
valve surface and even on the chordae tendineae. This patient
has SLE. Thus, these vegetations that can be on any valve or even on endocardial surfaces are consistent with Libman-
Sacks endocarditis. These vegetations appear in about 4% of
SLE patients.

8/10/2019 12-Immunopathology_Part_2.pdf
http://slidepdf.com/reader/full/12-immunopathologypart2pdf 10/25Dr. Samir Ayad 10
(3) Kidneys: Normal (in few cases):
(i) Mesangial glomerulonephritis (10%):
increased cellularity of mesangial matrix
(ii) Focal proliferative glomerulonephritis (30%):
hypercellularity, but not all (focal) glomeruli, due to
proliferation of endothelial and mesangial cells. Presentwith hematuria, proteinuria, mild renal insufficiency.
(iii) Diffuse proliferative glomerulonephritis(45-50%):
Most serious, all glomeruli involved. Hematuria, proteinuria, hypertension, & renal insufficiency
(iv) Membranous glomerulonephritis (10%):
Thickening of capillary wall massive proteinuria

8/10/2019 12-Immunopathology_Part_2.pdf
http://slidepdf.com/reader/full/12-immunopathologypart2pdf 11/25

8/10/2019 12-Immunopathology_Part_2.pdf
http://slidepdf.com/reader/full/12-immunopathologypart2pdf 12/25Dr. Samir Ayad 12
Rapidly progressive glomerulonephritis with crescents, microscopic
Seen here within the glomeruli are crescents composed of proliferating
epithelial cells. Crescentic glomerulonephritis is known as rapidly
progressive glomerulonephritis (RPGN) because this disease is very
progressive. There are several causes, and in this case is due to SLE.
Note in the lower left glomerulus that the capillary loops are markedly
thickened (the so-called "wire loop" lesion of lupus nephritis).

8/10/2019 12-Immunopathology_Part_2.pdf
http://slidepdf.com/reader/full/12-immunopathologypart2pdf 13/25Dr. Samir Ayad 13
Lupus nephritis, kidney, microscopic
Here is a glomerulus with thickened pink capillary
loops, the so-called “wire loops", in a patient with
lupus nephritis. The surrounding renal tubules are
unremarkable.

8/10/2019 12-Immunopathology_Part_2.pdf
http://slidepdf.com/reader/full/12-immunopathologypart2pdf 14/25Dr. Samir Ayad 14
Lupus nephritis, electron micrograph
The thickened basement membrane (arrow) that
results from immune complex deposition in the
glomerular capillary loop is prominent in this electron
micrograph. The dark immune deposits are located
mainly in a subendothelial position.

8/10/2019 12-Immunopathology_Part_2.pdf
http://slidepdf.com/reader/full/12-immunopathologypart2pdf 15/25Dr. Samir Ayad 15
(4) Skin:
- deposition of immune complexes along thedermo-epidermal junction
- activation of complement inflammation
skin rash
- erythema, maculopapular rash
- malar regions of the face and bridge of nose( butterfly rash, photosensitivity to UVR)

8/10/2019 12-Immunopathology_Part_2.pdf
http://slidepdf.com/reader/full/12-immunopathologypart2pdf 16/25

8/10/2019 12-Immunopathology_Part_2.pdf
http://slidepdf.com/reader/full/12-immunopathologypart2pdf 17/25Dr. Samir Ayad 17
Vasculitis with marked inflammation, skin, patient with SLE,
microscopic
Here is a more severe inflammatory skin infiltrate in the upper
dermis of a patient with SLE in which the basal layer isundergoing vacuolization, and there is purpura with RBC's in
the upper dermis (which are the reason for the rash).

8/10/2019 12-Immunopathology_Part_2.pdf
http://slidepdf.com/reader/full/12-immunopathologypart2pdf 18/25Dr. Samir Ayad 18
(5) Joints:
- arthritis (most common presenting symptom)
resembles rheumatoid arthritis but:
- involves large and small joints
- mild (rarely causes destruction of cartilage)
(6) C.N.S:
- vasculitis hemorrhages, ischemia, infarcts
(7) Lung:
- pleurisy with pleural effusion
- alveolitis and fibrosis

8/10/2019 12-Immunopathology_Part_2.pdf
http://slidepdf.com/reader/full/12-immunopathologypart2pdf 19/25Dr. Samir Ayad 19
(8) Serosal cavities:
- Inflammation ( pleurisy, pericarditis, peritonitis)with serous effusion or fibrinous exudation inacute cases to fibrous opacification in chronic
cases.
(8) Spleen:
- enlarged slightly- capsule is thickened
- follicular hyperplasia

8/10/2019 12-Immunopathology_Part_2.pdf
http://slidepdf.com/reader/full/12-immunopathologypart2pdf 20/25Dr. Samir Ayad 20Complications of systemic lupus erythematosus.
8/10/2019 12-Immunopathology_Part_2.pdf
http://slidepdf.com/reader/full/12-immunopathologypart2pdf 21/25Dr. Samir Ayad 21
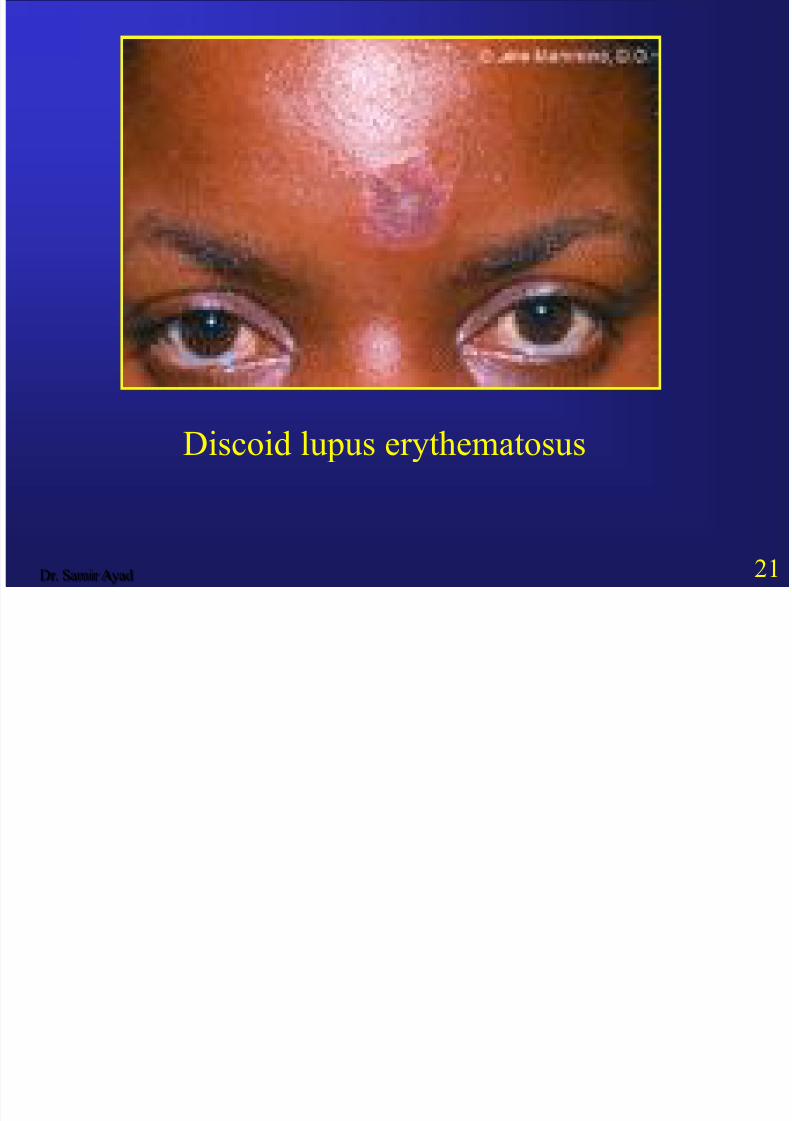
Discoid lupus erythematosus

8/10/2019 12-Immunopathology_Part_2.pdf
http://slidepdf.com/reader/full/12-immunopathologypart2pdf 22/25
Dr. Samir Ayad 22
Discoid lupus erythematosus

8/10/2019 12-Immunopathology_Part_2.pdf
http://slidepdf.com/reader/full/12-immunopathologypart2pdf 23/25
Dr. Samir Ayad 23
Clinical features:
- females
- arthritis (larger joints)
- fever
- skin eruption (butterfly rash over face)
- hypertension
- hematuria, albuminuria, nephrotic syndrome
Di i

8/10/2019 12-Immunopathology_Part_2.pdf
http://slidepdf.com/reader/full/12-immunopathologypart2pdf 24/25
Dr. Samir Ayad 24
Diagnosis :
- antinuclear antibodies (ANAs) in the serum
- presence of LE cells (nuclear debris ingested by blood neutrophils)
Prognosis:- chronic course with repeated exacerbations and
remissions
- survival rate is 90% at 10 years (death mostly due
to renal failure)
LE ll ti i i

8/10/2019 12-Immunopathology_Part_2.pdf
http://slidepdf.com/reader/full/12-immunopathologypart2pdf 25/25
25
LE cell preparation, microscopic
Here is the famous "LE cell" test which has value only in
demonstrating how the concept of autoantibodies work. The
pink blobs are denatured nuclei. Here are two, with one seen being phagocytozed in the center by a PMN.