(14.09.2012 final with isbn) uganda - whopromind · dr sebastiana da gama nkomo, acting regional...
TRANSCRIPT
WHO MIND Mental Health in Development
WHO proMIND: Profiles on
Mental Health in Development
Republic of Uganda
WHO MIND Mental Health in Development
Mental Health Policy and Service Development
Department of Mental Health and Substance Abuse
World Health Organization

WHO Library Cataloguing-in-Publication Data WHO proMIND: profiles on mental health in development: Uganda.
1.Mental health. 2.Mental health services. 3.Health policy. 4.Uganda. I.World Health Organization. ISBN 978 92 4 150419 5 (NLM classification: WM 140)
© World Health Organization 2012
All rights reserved. Publications of the World Health Organization are available on the WHO web site (www.who.int) or can be purchased from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press through the WHO web site (http://www.who.int/about/licensing/copyright_form/en/index.html).
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use. The named authors alone are responsible for the views expressed in this publication.
.
Suggested Citation: Ndyanabangi S. Funk M. Ssebunnya J. Drew N. Dhillon S. Sugiura K. Skeen S. WHO Profile on mental health in development (WHO proMIND): Republic of Uganda. Geneva, World Health Organization, 2012. This and other profiles on mental health in development can be sourced from: http://www.who.int/mental_health/policy/country/countrysummary/en/index.html For feedback or suggestions for the improvement of this publication, please email Dr Michelle Funk ([email protected])

Republic of Uganda
"A population that has access to a comprehensive and well coordinated system of care that promotes mental wellness and recovery from mental, neurological and substance abuse disorders." Acknowledgements This publication has been produced as part of the World Health Organization's (WHO) profiles on mental health in development (WHO proMIND), and has been written and edited by:
Dr Sheila Ndyanabangi, Mental Health Department, Ministry of Health Headquarters, Kampala, Republic of Uganda Dr Michelle Funk, Coordinator, Mental Health Policy and Service Development, Department of Mental Health and Substance Abuse, WHO, Geneva Dr Joshua Ssebunnya, Department of Mental Health and Community Psychology, Makerere University, Kampala, Republic of Uganda Ms Natalie Drew, Technical Officer, Mental Health Policy and Service Development, Department of Mental Health and Substance Abuse, WHO, Geneva Ms Sonia Dhillon, Mental Health Policy and Service Development, Department of Mental Health and Substance Abuse, WHO, Geneva Dr Kanna Sugiura, Technical Officer, Mental Health Policy and Service Development, Department of Mental Health and Substance Abuse, WHO, Geneva Ms Sarah Skeen, Technical Officer, Mental Health Policy and Service Development, Department of Mental Health and Substance Abuse, WHO, Geneva The preparation of this profile would not have been possible without the support of the following staff from WHO:
Dr Joaquim Saweka, The WHO Representative for the Republic of Uganda, Kampala Dr Sebastiana da Gama Nkomo, Acting Regional Advisor for Mental Health and Substance Abuse, WHO Regional Office for Africa, Brazzaville, Republic of Congo Mrs Carina Ferreira-Borges, Technical Officer for Mental Health and Substance Abuse, WHO Regional Office for Africa, Brazzaville, Republic of Congo (WHO proMIND): Republic of Uganda Potential partners interested in finding out more about mental health in the Republic of Uganda should also contact project partners based in-country (contact details on page 8). WHO proMIND Potential partners and donors interested in supporting or funding WHO proMIND projects should contact Dr Michelle Funk ([email protected]), Coordinator, MHP, Department of Mental Health and Substance Abuse, WHO, Geneva, Switzerland. More information about WHO MIND and WHO proMIND projects is available on the website: http://www.who.int/mental_health/policy/en/


WHOproMIND: Republic of Uganda | 1
THE PROJECT
"A population that has access to a comprehensive and well coordinated system of care that promotes mental wellness and recovery from mental, neurological and substance abuse disorders."
WHOproMIND: Republic of Uganda | 2
KEY ACHIEVEMENTS FOR MENTAL HEALTH IN UGANDA
� 100% Regional Referral Hospitals with functional mental health units achieved in 2007/8
� Community access to mental health services increased from 20% in 2005/06 to 75% in 2009/10
� Proportion of Health Centre IVs with Psychiatric Nurses or other mental health staff increased from 30% in 2005/06 to 75% in 2009/10
� Draft “Mental health, Neurological and substance abuse policy” presented to Senior Management Committee at the Ministry of Health and under review
� Draft mental health bill ready to present to parliament
� National Alcohol policy ready to present to Cabinet
� Media programmes held to educate the public on mental health, epilepsy and substance abuse control (1)
� In service training of 600 selected primary care health workers in providing Mental Health care in the community
� Reviewed Essential Medicines List to include more options including some atypical medicines
� Reviewed HMIS to include more conditions such as Dementia
NEXT STEPS FOR UGANDA
� Finalize and adopt mental health policy
� Devise and implement a mental health strategic plan
� Update and finalize mental health law

WHOproMIND: Republic of Uganda | 3
OVERVIEW
Health Sector reforms in the 1990s began a process of deinstitutionalizing mental health services and integrating mental health services into primary care. A number of strategies have been put in place to strengthen mental health services in Uganda under the strong leadership and commitment of the Ministry of Health of Uganda. In 1999, The National Health Policy was formulated and included a package of minimum health services (UMHCP) of which mental health was a component. This led to the training of general health care workers in mental health at all levels (pre-service and in-service training as well as the creation of a budget for mental health within the overall national health budget). Additional developments have been:
� Decentralization of mental health services alongside general health services from central government to district levels. This has been in an attempt to bring services closer to the population.
� Integration of mental health into general health care up to the community level.
� Attempts to reduce stigma by providing outpatient mental health services at Mulago National Hospital and outpatient general services at Butabika National mental Hospital.
� Provision of kitchen and sleeping facilities for relatives accompanying mental health
patients at all Regional Hospital mental health units to encourage family involvement in mental health patient care through direct participation in care.
Challenges to mental health service delivery are constrained by inadequate finances, human resources, and available supplies of essential medicines. Also, lack of awareness among patients and negative attitudes towards mental health among health workers are barriers to more effective service delivery. The Ministry of Health has reviewed the Mental Health Policy to ensure comprehensive care for Mental, Neurological and Substance abuse related conditions. In the next two years the Ministry is planning to:
� increase provision of kitchen and sleeping facilities for relatives accompanying mental health patients at all Regional Hospital mental health units to encourage family involvement in mental health patient care through direct participation in care
� develop an action plan for implementation of the global strategy for reduction of harmful use of Alcohol
� finalize drafting of drug control masterplan
� participate in a research project on integration of Mental Health in Primary Health Care
under the PRIME project
WHOproMIND: Republic of Uganda | 4
HISTORY AND MILESTONES
1996
The Ministry of Health started a process of strengthening mental health services and integrating them into primary care. Standards and guidelines for mental health were developed for the care of epilepsy and the mental health of children and adults, from community to tertiary level. Health workers began to receive training in detection and management of mental and neurological conditions and a new referral and supervision support network was established.
1999
The National Health Policy was formulated and included a package of minimum health services (UMHCP) of which mental health was a component.
2000
A draft mental health policy was developed and was informally adopted leading to significant reforms in the country.
2001
Health Sector Strategic Plan (HSSP I) was released covering a period from 2000/01 -2004/05. This document provided for the building and furnishing of modern mental health units at 6 of the 10 regional referral hospitals. The implementation of this plan led to improved access to health services, a rise in use of health care services and the abolishment of user-fees.
2002
Review of staffing norms and inclusion of mental health nurses at health centre level. 2003
African Development Bank (ADB) funds the Re-development of Butabika Hospital with 450 bed capacity (reduced from 1000) and 6 Regional mental health units with 35 bed capacity.
2005
Health Sector Strategic Plan II (HSSP II) released covering a time period from 2005 - 2010. The HSSP II set a range of targets for mental health including functional Mental Health Units at all regional hospitals, increasing community access to mental health services by 50% and establishing a community strategy for the prevention of mental health problems.
2007
The HSSP II target to construct mental health units at 100% Regional Referral Hospitals was achieved.
2008
Findings from a situational analysis of Uganda’s mental health care system by the Mental Health and Poverty Project, a 5 year DFID funded study on mental health policy and service delivery, established the need for an officially endorsed mental health policy. Consequently, various stakeholders lobbied the Ministry of Health, including the top management committee and the heads of departments for mandate and support. A multi-disciplinary drafting committee was formed to revise the policy draft based on consultation with a wide range of stakeholders.

WHOproMIND: Republic of Uganda | 5
2010
The draft mental health policy was submitted to the Policy Analysis Unit of the Ministry of Health for revision, and has recently been sent to the Senior and Top Management Committees for discussion and approval. Extensive discussion with these committees has taken place. On approval, the policy will be widely disseminated to all stakeholders and is expected to contribute significantly towards structuring and improving mental health services in the country. Development of a specific mental health strategic plan based on the policy is also under way. A drafting committee was established to review current mental health legislations and WHO support materials to inform required revisions to the 1964 legislation. This was followed by a series of consultative meetings with key stakeholders, including health professionals, policy-makers, and a range of government ministries, NGOs and service users. These consensus-building meetings helped to identify weaknesses in drafts, develop the contents of the Bill, obtain varying opinions and gain ongoing support for the drafting and adoption processes. The drafting committee referred to mental health legislations in other countries of similar socio-economic contexts such as Kenya and South Africa to improve the draft.

WHOproMIND: Republic of Uganda | 6
Timeline
1996 2000 2001 2002
2008
Initiation of Mental Health Reforms to decentralise services
Review of staffing norms and inclusion of mental health nurses at health centre level.
Drafting committee for new mental health policy established and process commenced
2005 Health Sector Strategic Plan target achieved: 100% Regional Hospitals with Mental Health Units
2007
Health Sector Strategic Plan I released with set targets for mental health and abolishment of user fees in Public Health facilities
2010
Approval process of draft Mental Health Policy ongoing
Drafting committee for new mental health legislation established and process commenced to review 1964 Mental Health Act
Minimum health package included mental health as a component
1999
Development of draft Mental Health Policy

WHOproMIND: Republic of Uganda | 7
OFFICIAL DOCUMENTS
DEVELOPMENT AND POVERTY REDUCTION POLICIES, STRATEGIES AND PROGRAMMES
� Uganda Poverty Reduction Strategy Paper, National Development Plan 2010/11-2014/15, Republic of Uganda and International Monetary Fund http://www.imf.org/external/pubs/ft/scr/2010/cr10141.pdf
HEALTH AND MENTAL HEALTH POLICIES, PLANS AND PROGRAMMES
� Health Sector Strategic Plan III, 2010/11 – 2014/15, Government of Uganda, Ministry of Health, http://www.health.go.ug/docs/HSSP_III_2010.pdf
� The Uganda Draft Mental Health Policy (2000-2005) LEGISLATION
� Mental Treatment Act 1964 SITUATIONAL ANALYSES
� Mental Health and Poverty Project, 2008, Uganda Country Report, http://workhorse.pry.uct.ac.za:8080/MHAPP/public/public/resources/Uganda_report

WHOproMIND: Republic of Uganda | 8
MAIN PARTNERS
NATIONAL LEADING PARTNERS
Dr Sheila Ndyanabangi (Mental Health Department, Ministry of Health Headquarters, Kampala, Uganda) Email: [email protected] Joshua Ssebunnya (Department of Mental Health and Community Psychology, Makerere University, Kampala, Uganda) Email: [email protected]
WHO COUNTRY OFFICE
Dr Joaquim Saweka (WHO Representative, WHO Country Office, Kampala, Uganda) Email: [email protected] WHO REGIONAL OFFICE FOR AFRICA Dr Sebastiana da Gama Nkomo (Acting Regional Advisor, Mental Health and Substance Abuse) Brazzaville, Republic of Congo Email: [email protected] Mrs Carina Ferreira-Borges (Technical Officer for Mental Health and Substance Abuse) Email: [email protected] WHO HEADQUARTERS
Dr Shekhar Saxena, Director, Department of Mental Health and Substance Abuse (MSD) Email: [email protected]
Dr Michelle Funk, Coordinator, Mental Health Policy and Service Development, MSD Email: [email protected]
Ms Natalie Drew, Technical Officer, Mental Health Policy and Service Development, MSD Email: [email protected]
Dr Kanna Sugiura, Technical Officer, Mental Health Policy and Service Development, MSD Email: [email protected]
Ms Sarah Skeen, Technical Officer, Mental Health Policy and Service Development, MSD Email: [email protected]
OTHER
Dr Frances Hughes, WHO PIMHnet Facilitator, Email: [email protected]: [email protected]

WHOproMIND: Republic of Uganda | 9
THE CONTEXT

WHOproMIND: Republic of Uganda | 10
1. COUNTRY DEMOGRAPHIC AND SOCIOECONOMIC PROFILE
Figure 1 Map of Uganda
Source: reference (2)
GEOGRAPHY AND CLIMATE
Uganda is located in East Africa, sharing its borders with Kenya on the east, Sudan on the north, Democratic Republic of Congo on the west, Rwanda on the south-west and Tanzania on the south (figure 1). The country capital is Kampala. Uganda has a total area of 241,038 square kilometres. Just less than 30% is arable land, 11% permanent cropland and 17% forest (3). DEMOGRAPHICS
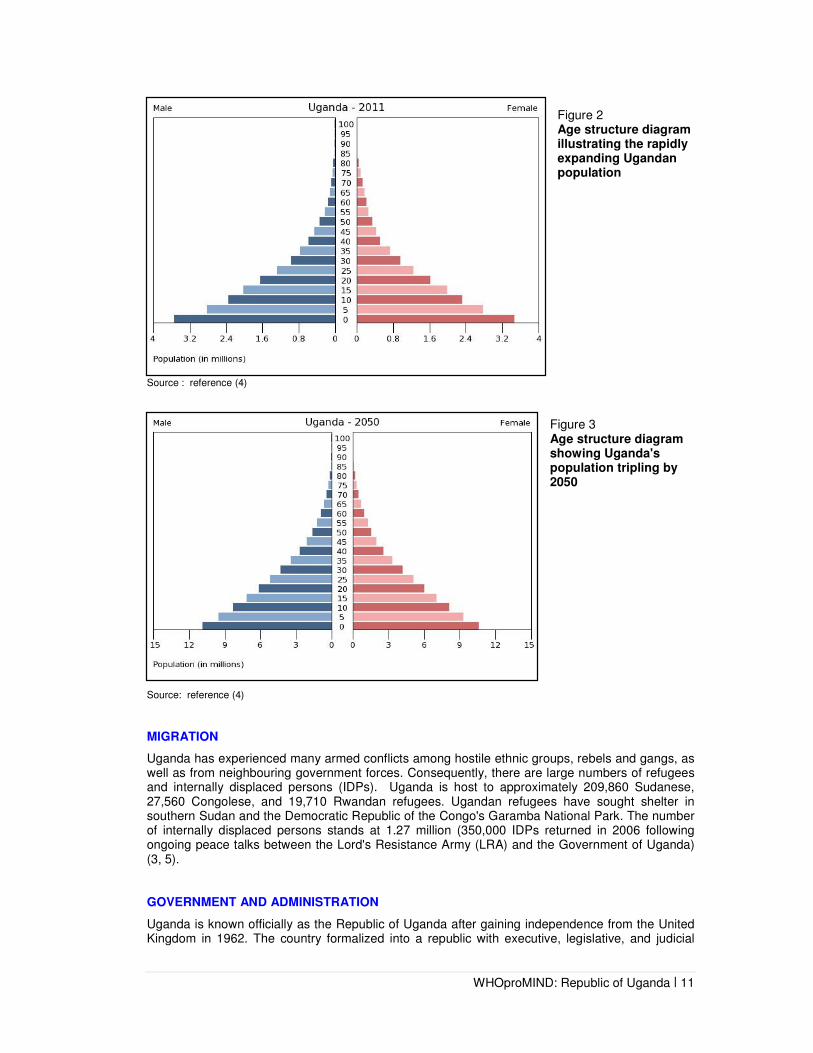
The population of Uganda in 2011 was 33 million (Population secretariat). Population growth is estimated at 3.4% per year, making it the third fastest-growing population in the world. The population by2050 is estimated to be 1.2 million. The median age is 15.1 years, with 49.9% of the population aged between 0-14 years, 48.1% aged between 15-64 years and 2.1% aged 65 years and above. Figures 2 and 3 illustrate the age distribution of Uganda's population by sex and shows that the populations expected triple by 2050.
WHOproMIND: Republic of Uganda | 11
Figure 2 Age structure diagram illustrating the rapidly expanding Ugandan population
Source : reference (4)
Figure 3 Age structure diagram showing Uganda's population tripling by 2050
Source: reference (4)
MIGRATION
Uganda has experienced many armed conflicts among hostile ethnic groups, rebels and gangs, as well as from neighbouring government forces. Consequently, there are large numbers of refugees and internally displaced persons (IDPs). Uganda is host to approximately 209,860 Sudanese, 27,560 Congolese, and 19,710 Rwandan refugees. Ugandan refugees have sought shelter in southern Sudan and the Democratic Republic of the Congo's Garamba National Park. The number of internally displaced persons stands at 1.27 million (350,000 IDPs returned in 2006 following ongoing peace talks between the Lord's Resistance Army (LRA) and the Government of Uganda) (3, 5). GOVERNMENT AND ADMINISTRATION
Uganda is known officially as the Republic of Uganda after gaining independence from the United Kingdom in 1962. The country formalized into a republic with executive, legislative, and judicial

WHOproMIND: Republic of Uganda | 12
branches after establishing its constitution in 1995. Uganda is divided into 112 administrative districts with distinct roles for central ministries and district level local governments (3). DEVELOPMENT INDICATORS The Human Development Index (HDI) is a measure of well-being and provides a composite measure on three basic dimensions of human development: health, education and income. Figure 4 shows that Uganda's HDI as of 2010 was 0.422, ranking 43 out of 169 countries. This places Uganda below the world average (HDI score 0.619), but above the regional average for Sub-Saharan Africa (HDI score 0.389) (6). Figure 4 Comparison of trends in HDI scores in Uganda with rest of world and Sub-Saharan region averages
Source: reference (4)
HDI score components for income, health and education in Uganda are illustrated in Figure 5 below. Uganda has witnessed overall improvements across all three development indicators from the 1970's to 2010. While Income and Health index scores showed decline during the 1980's and 1990's there has been gradual recovery of these indices since the mid to late 1990s. Progress in education has shown continuous improvement with a sharp increase from 0.249 in the 1970's to 0.661 in 2010.

WHOproMIND: Republic of Uganda | 13
Figure 5 Comparison of Income Index, Health Index and Education Index for Uganda with other Sub-Saharan Countries
Source: reference (4)
The Development Diamond below shows the four key indicators of life expectancy, GNI/capita, Gross primary enrolment and access to improved water source in Uganda compared to that of the 0low-income group average. As Figure 6 reveals, Uganda has slightly higher gross primary school enrolment and slightly lower GNI per capita compared to other lower-income countries. Figure 6 Development diamond of Uganda
Source: reference (7)
Income Index (Sub-Saharan Africa (RBI))
Health Index (Sub-Saharan Africa (RBI))
Education Index (Sub-Saharan Africa (RBI))

WHOproMIND: Republic of Uganda | 14
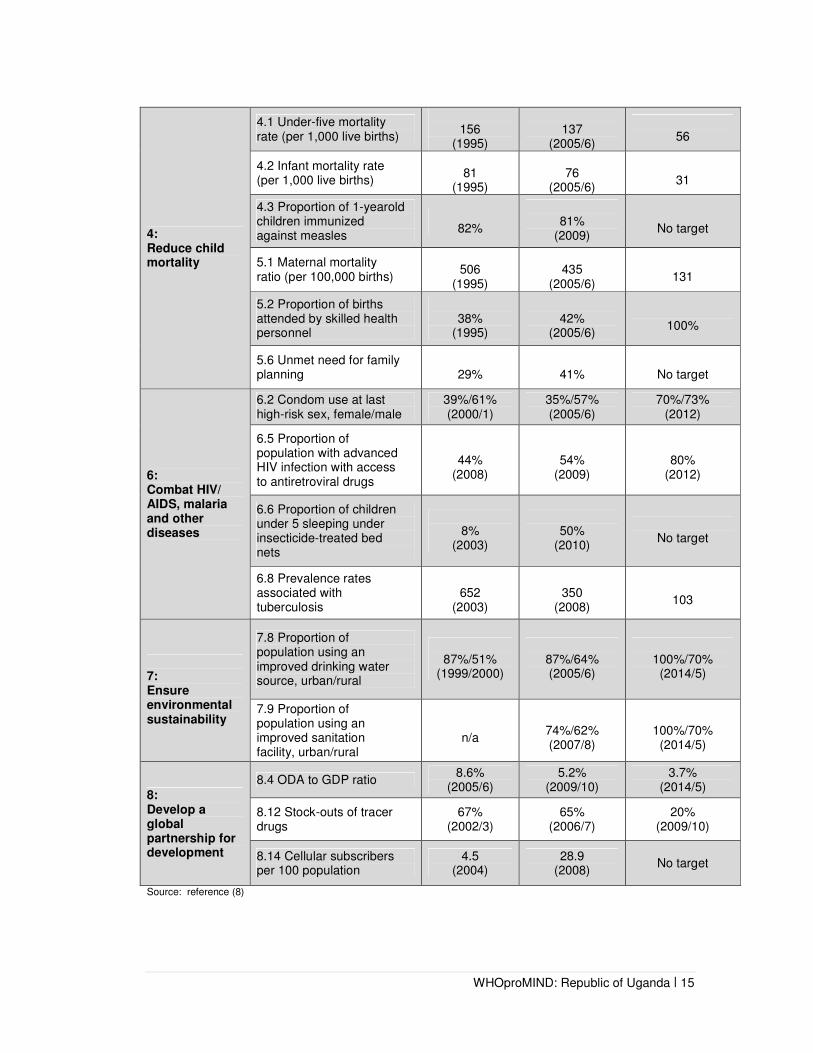
PROGRESS TOWARD THE MILLENNIUM DEVELOPMENT GOALS (8)
In 2010, Uganda reported important progress towards achieving many of the MDG targets (Table 1). The target of gender parity in primary education has been achieved and the country is on track to meet the targets for access to HIV/AIDS treatment and access to safe water. There has been good progress in reducing the share of the population living in poverty and with hunger. Some progress has been seen in gender equality, women’s rights, ensuring debt relief and sustainability and expanding access to information and communication technology. However, progress to improve reproductive health and reduce the incidence of malaria and other diseases has been more modest. There is unequal distribution of available resources, even though there has been overall progress towards many of the MDGs. In rural areas, levels of poverty are more than twice as high compared to urban areas. In the northern and eastern areas, poverty levels remain even higher.
Table 1 Summary table of MDG indicators of Uganda
MDG Indicator Baseline Current Status
2015 target
1: Eradicate extreme poverty and hunger
1.1 Proportion of population below national poverty line
56%
(1992/3)
31%
(2005/6)
25%
1.2 Poverty gap 21
(1992/3) 9
(2005/6) No target
1.8 Prevalence of underweight children under-five years of age (percentage below -2 standard deviations of weight for age)
26%
(1995)
16%
(2005/6)
10%
2: Achieve universal primary education
2.1Net enrolment ratio in primary education Boys Girls
(all 2000)
86% 89% 82%
(all 2009)
93% 96% 90%
100% 100% 100%
2.2 Primary completion Rate Boys Girls
(2001)
63% n/a n/a
(all 2009)
52% 55% 48%
100% 100% 100%
2.3 Literacy rate of 15-24 year-olds
(all 2002/3)
81%
(all 2008)
88% No target
3: Promote gender equality and empower women
3.1 Ratios of girls to boys in primary/secondary/ tertiary education
(all 2000)
0.93/0.79/0.58
(all 2009)
1.00/0.84/0.79
1.00/1.00/1.00
3.3 Proportion of seats held by women in national parliament
18%
(2000)
30%
(2006)
No target
WHOproMIND: Republic of Uganda | 15
4: Reduce child mortality
4.1 Under-five mortality rate (per 1,000 live births)
156
(1995)
137
(2005/6)
56
4.2 Infant mortality rate (per 1,000 live births)
81
(1995)
76
(2005/6)
31
4.3 Proportion of 1-yearold children immunized against measles
82%
81%
(2009)
No target
5.1 Maternal mortality ratio (per 100,000 births)
506
(1995)
435
(2005/6)
131
5.2 Proportion of births attended by skilled health personnel
38%
(1995)
42%
(2005/6)
100%
5.6 Unmet need for family planning
29%
41%
No target
6: Combat HIV/ AIDS, malaria and other diseases
6.2 Condom use at last high-risk sex, female/male
39%/61% (2000/1)
35%/57% (2005/6)
70%/73% (2012)
6.5 Proportion of population with advanced HIV infection with access to antiretroviral drugs
44%
(2008)
54%
(2009)
80%
(2012)
6.6 Proportion of children under 5 sleeping under insecticide-treated bed nets
8%
(2003)
50%
(2010)
No target
6.8 Prevalence rates associated with tuberculosis
652
(2003)
350
(2008)
103
7: Ensure environmental sustainability
7.8 Proportion of population using an improved drinking water source, urban/rural
87%/51%
(1999/2000)
87%/64% (2005/6)
100%/70%
(2014/5)
7.9 Proportion of population using an improved sanitation facility, urban/rural
n/a
74%/62% (2007/8)
100%/70%
(2014/5)
8: Develop a global partnership for development
8.4 ODA to GDP ratio 8.6%
(2005/6) 5.2%
(2009/10) 3.7%
(2014/5)
8.12 Stock-outs of tracer drugs
67% (2002/3)
65% (2006/7)
20% (2009/10)
8.14 Cellular subscribers per 100 population
4.5 (2004)
28.9 (2008)
No target
Source: reference (8)

WHOproMIND: Republic of Uganda | 16
2. CONTEXTUAL FACTORS INFLUENCING MENTAL HEALTH NEEDS AND SERVICES
HIV/AIDS
Approximately 68% of those living with HIV/AIDS in the world reside in Sub Saharan Africa and 76% of the AIDS related deaths in 2007 alone occurred in this region. Several social determinants of health such as poverty, underdevelopment and illiteracy play major roles in exacerbating the HIV epidemic. Individuals living with HIV/AIDS may face physical and psychological stresses that negatively impact their well-being. The social ramifications of HIV/AIDS have challenged development initiatives at individual, local and national levels. Financial resources are often depleted in caring for the sick and household incomes may be threatened, either from disability or because household members must care for ailing family members. Uganda was among the first countries devastated by the HIV/AIDS epidemic. In 1992, the national disease prevalence was approximated at 18.3% and as high as 30% in some areas. From the mid 1990s through 2002 there was a steady decline in prevalence to approximately 6%. This was attributed to favourable prevention policies. The country has since experienced stabilizing prevalence of HIV/AIDS over the last several years. The 2004/05 National HIV/AIDS survey by the Ministry of Health Surveillance Unit estimated about 915,400 adults and children were living with HIV/AIDS in 2005. Prevalence among adults aged 15-49 was estimated at 6.4%, 0.7% among children less than 5 years, and 5.8% among those aged 50-59. The Ministry of Health estimated 132,500 new infections in 2005 alone. The survey revealed regional, rural/urban, and gender variations in HIV prevalence. Overall infection rates were higher in urban areas compared to rural areas. Women living in urban settings had a disease prevalence almost twice as high (13%) as those living in rural areas (7%). As of 2007, adult HIV Prevalence in Uganda was 5.4% (9). REFUGEES AND INTERNALLY DISPLACED PERSONS
Uganda is host to a large number of refugees from neighbouring countries, particularly the Democratic Republic of the Congo and Sudan. Steady improvement in the political relationship between Uganda and its neighbours has seen most of the refugees from South Sudan returning to their homeland. IDPs in Northern and North-eastern Uganda have been a major focus for the country’s government. Improved security has encouraged spontaneous return by IDPs from the domicile camps to satellite camps closer to their locations of origin. The majority of internally displaced people in Northern and Eastern Uganda have returned to their homes with a few vulnerable people remaining in camps. The government has initiated interventions to help them resettle (5). MIGRATION OF SKILLED WORKERS
Ugandan doctors and nurses have sought employment in Botswana, South Africa, Swaziland, Rwanda, the UK, Canada, USA, and elsewhere. According to Hagopian et al (2004) (10), there were 175 Ugandan doctors living and practicing in the U.S compared to 722 in the whole of Uganda. According to the MoH, between the years 2003-2009, 500 Ugandan doctors and thousands of nurses went to work abroad. This phenomenon of emigrating skilled personnel imposes severe economic and social costs on home countries, especially when the number of skilled local personnel is limited.

WHOproMIND: Republic of Uganda | 17
POVERTY
Poverty and mental health conditions interact in a negative cycle. People living in poverty not only lack financial resources to maintain basic living standards, but may also have fewer educational and employment opportunities. These individuals may face hazardous living environments with poor sanitation, limited or no access to water and restricted access to effective health care. The stress associated with hazardous living environments may impair psychological well-being. People with mental health conditions sometimes are unable to work because of their symptoms. Due to discrimination, others are denied work opportunities or lose employment. Many have no means to pay for needed treatment. In other instances, money is spent on costly mental health care. If this care is ineffective or inappropriate, the end result may be even worse, as individuals would have not only expended their financial resources, but also failed to get better (11). The proportion of people living below the poverty line has significantly declined from 52% in 1992 to 31% in 2005. Despite this reduction, poverty still remains a significant problem for Uganda. Uganda remains one of the poorest countries, ranking 145 on the global Human Development Index.

WHOproMIND: Republic of Uganda | 18

WHOproMIND: Republic of Uganda | 19
MENTAL HEALTH PROBLEMS AND TREATMENT IN UGANDA

WHOproMIND: Republic of Uganda | 20
3. BURDEN OF DISEASE AND TREATMENT GAP
PREVALENCE AND BURDEN OF DISEASE IN COUNTRY
There is no recent and reliable data on the prevalence of mental illness in Uganda because few epidemiological studies have been conducted in the field of mental health. One 2004 study estimated that 35% of Ugandans suffer from some form of mental disorder (Basangwa, 2004; as cited by Kigozi et al 2008), however this is much greater than the generally accepted estimate of 13% global prevalence rate (3% severe mental illness, 10% mild to moderate mental illness) (12). Anecdotal evidence suggests an increase in the incidence of mental disorders. According to UBOS (2006)(13), an estimated 7% of the households in the country had disabled members, of which 58% had at least one person with a mental disorder. This implies that about 4% of the households had at least one member with a mental disability. TREATMENT AND SERVICE UITLIZATION DATA
In the financial year 2009/2010, Butabika provided inpatient mental health care to 4,394 first time admissions and 1,752 readmissions. This suggests that there were at least 6,146 admissions for mental disorders at the tertiary level in one year. At the 13 regional referral hospitals, the number of available psychiatric beds range between 16 and 40 beds each and average length of stay for a patient is 2 to 3 weeks. In those hospitals, between 170 and 360 patients are seen in inpatient services a year and between 748 and 2500 patients are seen in outpatient's services of the different facilities a year. For detailed numbers for each hospital please refer to Table 2. There is very little reliable data on treatment rates or service utilization at district general hospital level and health centre level. TREATMENT GAP
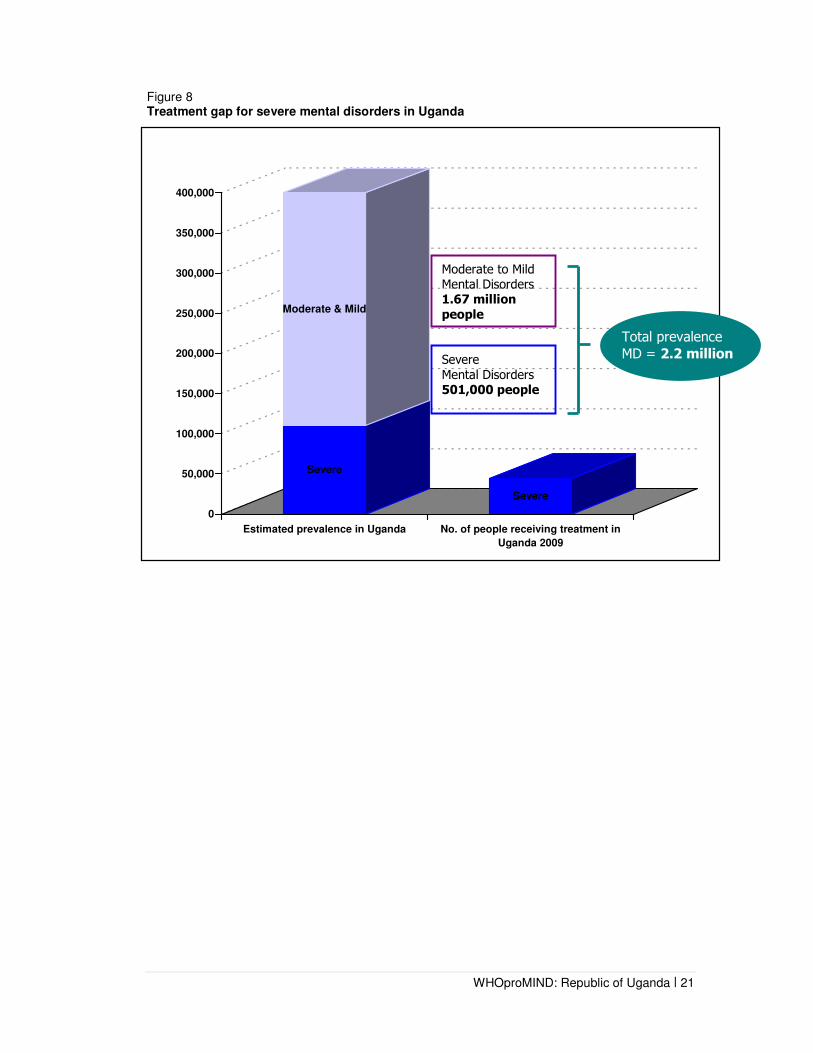
Given that there is no reliable national level data for population-based prevalence rates of mental illness in Uganda, the treatment gap has been estimated from a conservative perspective using the global rate of 13% prevalence (as opposed to the higher estimate of 35% reported above). Based on global prevalence rates we can estimate that about 2.2 million people in Uganda (13% of the 16.7 million adult population) have had a mental disorder in the previous year, and about 501,000 (3% of the adult population) have had a severe form. In Table 2 (below) it is estimated that approximately 7540 people were treated in inpatient services in the tertiary or secondary care hospitals and 37221 people were treated in outpatient services at the same facilities. In total, it is thus estimated that 44 219 people were treated in the past year. If we assume that most new people in Uganda who were treated had a severe mental disorder, then the treatment gap for severe mental disorders would be 91.1%. This estimated treatment gap is illustrated in Figure 8, below:
WHOproMIND: Republic of Uganda | 21
Figure 8 Treatment gap for severe mental disorders in Uganda
Severe
Moderate & Mild
Severe
0
50,000
100,000
150,000
200,000
250,000
300,000
350,000
400,000
Estimated prevalence in Uganda No. of people receiving treatment in
Uganda 2009
Severe
Mental Disorders
501,000 people
Moderate to Mild
Mental Disorders
1.67 million
people
Total prevalence
MD = 2.2 million

WHOproMIND: Republic of Uganda | 22
Table 2. Service Utilization in Uganda (Health Management Information System 2010)
GENERAL HEALTH
MENTAL HEALTH INPATIENT MENTAL HEALTH OUTPATIENT
Facility/Level Total Number
of Beds Total Number
Beds Average length of
stay
Number of Individual Patients
seen per year
Number of contacts per year
(i.e. number of total consultations)
Number of Individual
patients seen per year
Number of contacts per year
(i.e. number of total
consultations)
TERTIARY LEVEL CARE
Mulago Hospital
Total 1700 50 12 days 165 364 416 795
Butabika Hospital
Total 550 3 weeks 4394 6146 21240 95106
SECONDARY LEVEL CARE
Regional Referral Hospitals
TOTAL 3824 337 2-3 weeks 2981 8497 15565 76805
Lira 322 28 3 weeks 240 900 1,200 5500
Mbarara 295 20 2 weeks 220 720 1,300 7,200
Soroti 260 35 2 weeks 144 445 542 5,950
Mubende 100 20 2 weeks 300 420 800 3,200
Mbale 440 22 2 weeks 340 850 748 4,460
Hoima 240 20 2 weeks 185 650 1100 4,200
Gulu 432 30 2 weeks 355 792 1,850 8,440
Moroto 133 16 2 weeks 110 320 495 2,750
Jinja 396 40 2 weeks 170 620 2,500 6,500
Arua 319 40 3 weeks 360 700 1,030 7000
Masaka 302 20 2 weeks 210 750 2,400 9,000
Kabale 254 26 2 weeks 185 645 780 6,955
Fortportal 331 20 2 weeks 162 685 820 5,650
TOTAL ALL LEVELS OF CARE
5524 937 2-3 weeks 7540 15007 37221 172706

WHOproMIND: Republic of Uganda | 23

WHOproMIND: Republic of Uganda | 24
MENTAL HEALTH WITHIN THE GENERAL HEALTH SYSTEM
WHOproMIND: Republic of Uganda | 25
4. MENTAL HEALTH WITHIN THE GENERAL HEALTH SYSTEM
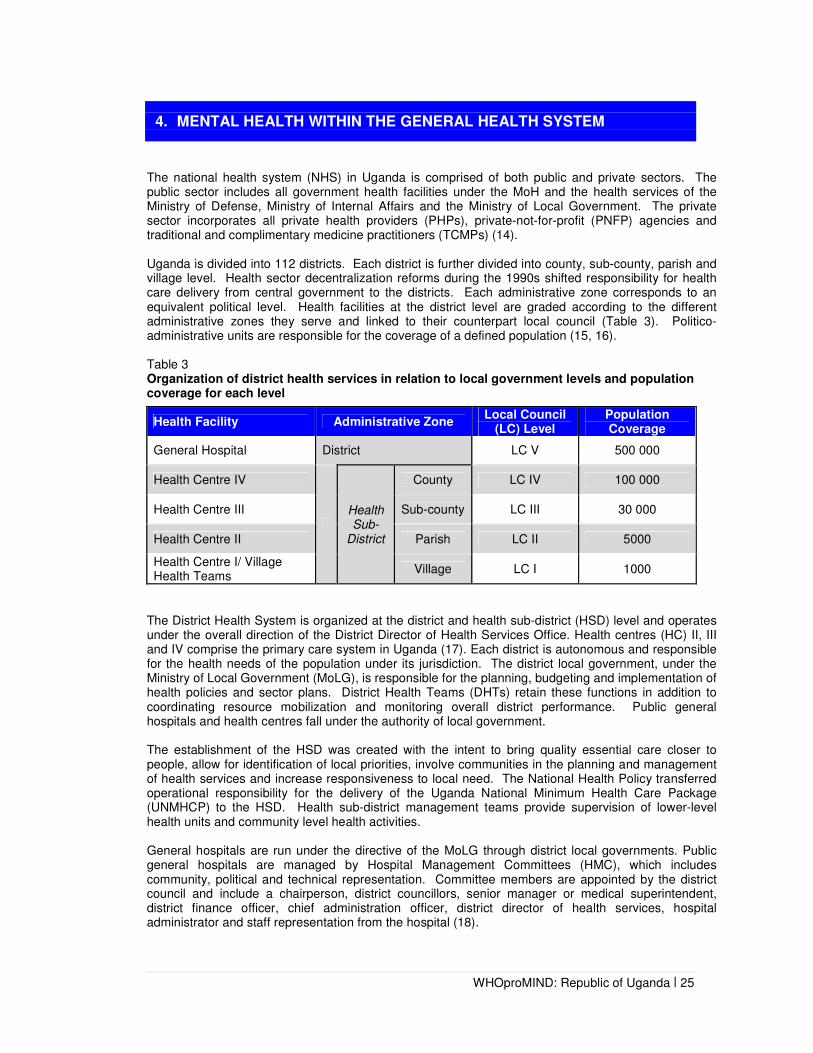
The national health system (NHS) in Uganda is comprised of both public and private sectors. The public sector includes all government health facilities under the MoH and the health services of the Ministry of Defense, Ministry of Internal Affairs and the Ministry of Local Government. The private sector incorporates all private health providers (PHPs), private-not-for-profit (PNFP) agencies and traditional and complimentary medicine practitioners (TCMPs) (14). Uganda is divided into 112 districts. Each district is further divided into county, sub-county, parish and village level. Health sector decentralization reforms during the 1990s shifted responsibility for health care delivery from central government to the districts. Each administrative zone corresponds to an equivalent political level. Health facilities at the district level are graded according to the different administrative zones they serve and linked to their counterpart local council (Table 3). Politico-administrative units are responsible for the coverage of a defined population (15, 16). Table 3 Organization of district health services in relation to local government levels and population coverage for each level
Health Facility Administrative Zone Local Council
(LC) Level Population Coverage
General Hospital District LC V 500 000
Health Centre IV
Health Sub-
District
County LC IV 100 000
Health Centre III Sub-county LC III 30 000
Health Centre II Parish LC II 5000
Health Centre I/ Village Health Teams
Village LC I 1000
The District Health System is organized at the district and health sub-district (HSD) level and operates under the overall direction of the District Director of Health Services Office. Health centres (HC) II, III and IV comprise the primary care system in Uganda (17). Each district is autonomous and responsible for the health needs of the population under its jurisdiction. The district local government, under the Ministry of Local Government (MoLG), is responsible for the planning, budgeting and implementation of health policies and sector plans. District Health Teams (DHTs) retain these functions in addition to coordinating resource mobilization and monitoring overall district performance. Public general hospitals and health centres fall under the authority of local government. The establishment of the HSD was created with the intent to bring quality essential care closer to people, allow for identification of local priorities, involve communities in the planning and management of health services and increase responsiveness to local need. The National Health Policy transferred operational responsibility for the delivery of the Uganda National Minimum Health Care Package (UNMHCP) to the HSD. Health sub-district management teams provide supervision of lower-level health units and community level health activities. General hospitals are run under the directive of the MoLG through district local governments. Public general hospitals are managed by Hospital Management Committees (HMC), which includes community, political and technical representation. Committee members are appointed by the district council and include a chairperson, district councillors, senior manager or medical superintendent, district finance officer, chief administration officer, district director of health services, hospital administrator and staff representation from the hospital (18).

WHOproMIND: Republic of Uganda | 26
Regional referral hospitals in Uganda have been granted self-accounting status but are still managed under the MoH. Both national referral hospitals Mulago and Butabika are fully autonomous (19).
Table 4 illustrates hospital resources by sector and facility in 2009-2010. Table 5 illustrates district hospital data based on HMIS from 2009-2010. An essential feature of the role of the Ministry of Health is providing leadership and coordination of the overall sector by bringing together stakeholders at the central, district and community level. Core functions include policy analysis, formulation and dialogue; strategic planning; setting standards and quality assurance; resource mobilization; advising other ministries, departments and agencies on health-related matters; capacity development and technical support supervision; provision of nationally coordinated services including health emergency preparedness and response and epidemic prevention and control; coordination of health research; and monitoring and evaluation of the overall health sector performance. Many of these functions are delegated to autonomous National institutions serving under the direction of MoH headquarters. Table 4 Hospitals in Uganda by sector and facility financial year 2009/10
Source: reference (1) - Annual Health Sector Performance Report 2009/10, PNHP
Table 5 District hospital data based on HMIS from 69 Hospitals Financial Year 2009/10
Source: reference (1) - Hospital submissions for AHSR 2009/10

WHOproMIND: Republic of Uganda | 27
Decentralization
The present structure and delivery of health services in Uganda is best understood in light of major decentralization reforms during the 1990s that decentralized government and service delivery from central government to district councils. The policy, which is within the 1995 Constitution and 1997 Local Government Act, impacted most sectors including health (20). In 1999 the Ministry of Health developed the National Health Policy (1999-2010) and Health Sector Strategic Plan I (2000/01-2004/05), which reflect Primary Health Care (PHC) as the guiding philosophy and strategy for health, in line with WHO and the Alma-Ata Declaration of Health for All strategy. The National Health Policy 1999 devolved health service delivery to local government with central government maintaining a stewardship function. Against this backdrop, mental health services have been fully decentralized and are being integrated into general health care (21). As a means for improving the management and delivery of healthcare services in Uganda, decentralization has yet to fulfil its potential (20). Figure 9 illustrates the Ministry of Health Structure. Figure 10 illustrates a map of the mental health services within the general health system.

WHOproMIND: Republic of Uganda | 28
Figure 9. Ministry of Health Organogram
Commissioner Commissioner Commissioner Commissioner NursingNursingNursingNursing
Office of the MinisterOffice of the MinisterOffice of the MinisterOffice of the Minister Permanent SecretaryPermanent SecretaryPermanent SecretaryPermanent Secretary
Director GeneralDirector GeneralDirector GeneralDirector General Health Services Health Services Health Services Health Services CommissionCommissionCommissionCommission
ResourcResourcResourcResource e e e CentreCentreCentreCentre Policy Analysis UnitPolicy Analysis UnitPolicy Analysis UnitPolicy Analysis Unit Department of Department of Department of Department of Finance and Finance and Finance and Finance and AdministrationAdministrationAdministrationAdministration
Directorate of Clinical and Directorate of Clinical and Directorate of Clinical and Directorate of Clinical and Community Health ServicesCommunity Health ServicesCommunity Health ServicesCommunity Health Services Directorate of Planning and Directorate of Planning and Directorate of Planning and Directorate of Planning and DevelopmentDevelopmentDevelopmentDevelopment Department of Department of Department of Department of National National National National Disease Disease Disease Disease Department of Department of Department of Department of Community Community Community Community HealthHealthHealthHealth Department ofDepartment ofDepartment ofDepartment of Clinical ServicesClinical ServicesClinical ServicesClinical Services Department Department Department Department of Planningof Planningof Planningof Planning Department of Department of Department of Department of Quality Quality Quality Quality AssuranceAssuranceAssuranceAssurance MENTAL HEALTH SECTIONMENTAL HEALTH SECTIONMENTAL HEALTH SECTIONMENTAL HEALTH SECTION Office of the National Mental Office of the National Mental Office of the National Mental Office of the National Mental Health CoordinatorHealth CoordinatorHealth CoordinatorHealth Coordinator

WHOproMIND: Republic of Uganda | 29
Figure 10. Mental Health Services within the General Health System
MoH HQ
Public Health System
Level/ Population
coverage Population–wide including army, police and
National Referral Hospital 2 national referral hospitals: Butabika and Mulago
National 30 000 000
Regional 2 000 000
HC IV 9 Health Centre
HC III 157 Health
HC II 391 Health
HC IV 3 Health Centre
HC III 10 Health
HC II 257 Health
General Hospital
General Hospital
District 500 000
County 100 000
Sub-county 20 000
Parish 5000
Village 1000
District General Hospital 144 general hospitals
HC IV 188 Health Centre IVs
HC III 1182 Health Centre IIIs
HC II 3517 Health Centre IIs
HC I/ Village Health Team
District Health Services HQ
Regional Referral Hospital 13 regional hospitals.
Total of 13 mental health units at regional level. Each regional referral hospital has one mental health
unit.
Health
Su
b-d
istric
t
Private health Services
Private-not-for-profit
WHOproMIND: Republic of Uganda | 30
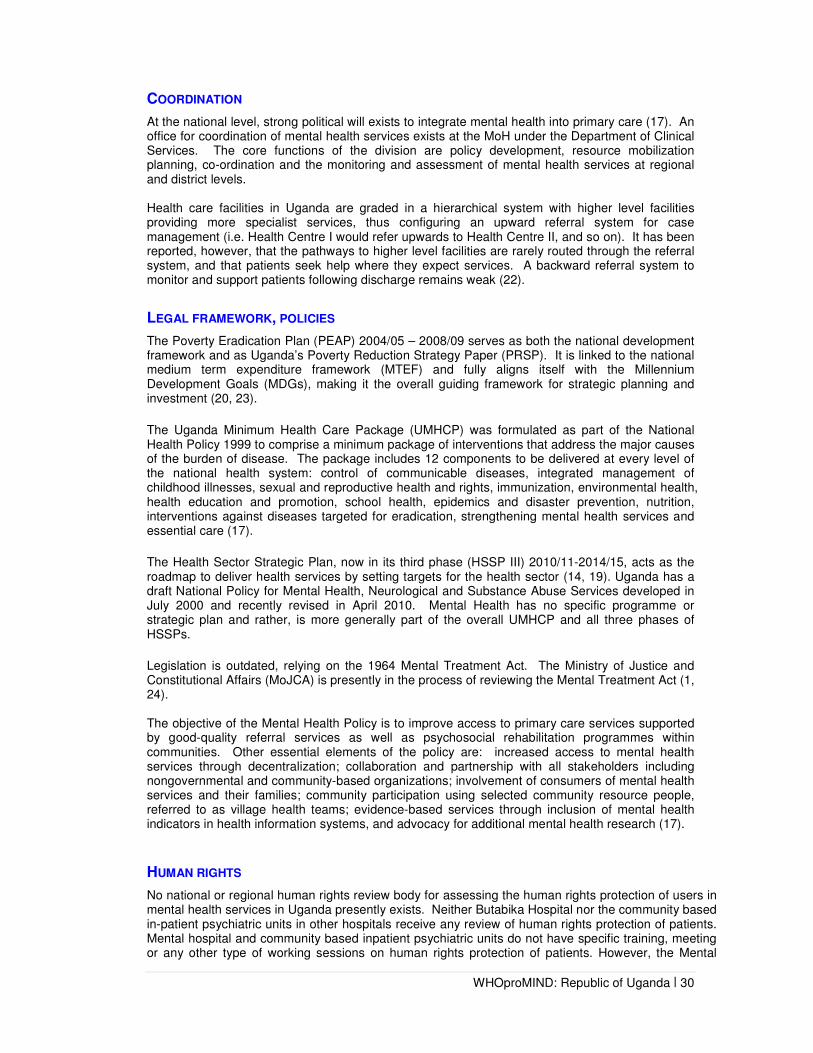
COORDINATION
At the national level, strong political will exists to integrate mental health into primary care (17). An office for coordination of mental health services exists at the MoH under the Department of Clinical Services. The core functions of the division are policy development, resource mobilization planning, co-ordination and the monitoring and assessment of mental health services at regional and district levels. Health care facilities in Uganda are graded in a hierarchical system with higher level facilities providing more specialist services, thus configuring an upward referral system for case management (i.e. Health Centre I would refer upwards to Health Centre II, and so on). It has been reported, however, that the pathways to higher level facilities are rarely routed through the referral system, and that patients seek help where they expect services. A backward referral system to monitor and support patients following discharge remains weak (22).
LEGAL FRAMEWORK, POLICIES
The Poverty Eradication Plan (PEAP) 2004/05 – 2008/09 serves as both the national development framework and as Uganda’s Poverty Reduction Strategy Paper (PRSP). It is linked to the national medium term expenditure framework (MTEF) and fully aligns itself with the Millennium Development Goals (MDGs), making it the overall guiding framework for strategic planning and investment (20, 23). The Uganda Minimum Health Care Package (UMHCP) was formulated as part of the National Health Policy 1999 to comprise a minimum package of interventions that address the major causes of the burden of disease. The package includes 12 components to be delivered at every level of the national health system: control of communicable diseases, integrated management of childhood illnesses, sexual and reproductive health and rights, immunization, environmental health, health education and promotion, school health, epidemics and disaster prevention, nutrition, interventions against diseases targeted for eradication, strengthening mental health services and essential care (17). The Health Sector Strategic Plan, now in its third phase (HSSP III) 2010/11-2014/15, acts as the roadmap to deliver health services by setting targets for the health sector (14, 19). Uganda has a draft National Policy for Mental Health, Neurological and Substance Abuse Services developed in July 2000 and recently revised in April 2010. Mental Health has no specific programme or strategic plan and rather, is more generally part of the overall UMHCP and all three phases of HSSPs. Legislation is outdated, relying on the 1964 Mental Treatment Act. The Ministry of Justice and Constitutional Affairs (MoJCA) is presently in the process of reviewing the Mental Treatment Act (1, 24). The objective of the Mental Health Policy is to improve access to primary care services supported by good-quality referral services as well as psychosocial rehabilitation programmes within communities. Other essential elements of the policy are: increased access to mental health services through decentralization; collaboration and partnership with all stakeholders including nongovernmental and community-based organizations; involvement of consumers of mental health services and their families; community participation using selected community resource people, referred to as village health teams; evidence-based services through inclusion of mental health indicators in health information systems, and advocacy for additional mental health research (17).
HUMAN RIGHTS
No national or regional human rights review body for assessing the human rights protection of users in mental health services in Uganda presently exists. Neither Butabika Hospital nor the community based in-patient psychiatric units in other hospitals receive any review of human rights protection of patients. Mental hospital and community based inpatient psychiatric units do not have specific training, meeting or any other type of working sessions on human rights protection of patients. However, the Mental

WHOproMIND: Republic of Uganda | 31
Health and Poverty Project (2006) found that some of the health workers have had some general training on human rights issues as part of their overall training. At the same time, violation of the rights of the people with mental disability was reported to be a fairly common practice (25).

WHOproMIND: Republic of Uganda | 32
4. RESOURCES FOR MENTAL HEALTH
FINANCING
The bulk of public sector service delivery for health is financed from the Government of Uganda (GoU) budget including donor support and project funding (table 6). The resource envelope for health covers the Ministry of Health, national hospitals, regional referral hospitals, primary health care, NGO health units, Uganda Aids Commission and the Health Services Commission. Funds are allocated in line with Uganda's Budget Framework Paper (BFP) which takes into account the National Health Policy (NHP), Health Sector Strategic Plan (HSSP) and annual sector priorities set by the National Health Assembly and Joint Review Mission. The Ministry of Finance, Planning and Economic Development (MoFPED) is responsible for releasing funds to the various ministries, agencies and facilities in consultation with the Medium Term Expenditure Framework (MTEF) (14, 26). Both Mulago and Butabika national hospitals and all regional referral hospitals in Uganda hold self-accounting status whereby they have a direct relationship with MoFPED regarding financial matters. Local councils receive grants directly from MoFPED for district health care service delivery at local council level 5, which is then allocated to the lower levels However, drugs are procured centrally (18). Table 6 Budget allocation to health providers in Uganda Financial Year 2007-2008 )
Source: reference (22) The total public expenditure on health for the financial year 2009/10 was Ugshs 737.6 of which GoU funding was Ugshs 435.8. An upward trend of government financing for health care has been witnessed, but fluctuations in donor project funding resulted in a general decline of total public expenditure on health between the years 2005/06-2007/08. The resource envelope for health however has since been increasing. This is reflected in per capita expenditure which has steadily increased from 2006/07. However, taking into consideration the growing population, per capita expenditure in 2009/11 was still less than 2005/06. Insufficient funding to deliver the UNMHCP remains a challenge to health care coverage. The health budget for 2008/09 was USD 10.4 per capita whilst the estimated per capita cost was USD 41.2, illustrating a shortfall of almost USD 31 USD (19). In addition, GoU allocation to health as a proportion of the total GoU budget for the financial year 2009/10 continues to remain below the Abuja target of a minimum of 15% of total government spending at 9.6%.

WHOproMIND: Republic of Uganda | 33
Table 7 MTEF allocation to the Health Sector during the HSSP II period
FY GoU Funding
Donor Project Funding
Total Per capita expenditure
in USD
GoU expenditure
on health as % of total
GoU expenditure
2005/06 229.86 268.38 498.24 14.8 8.9%
2006/07 242.63 139.23 381.86 7.8 9.6% 2007/08 277.36 141.12 418.48 8.4 9.6%
2008/09 375.38 253.08 628.46 10.4 8.3% 2009/10 435.8 301.8 737.6 11.1 9.6 Source: reference (14)
The total budget for mental health in 2005 was approximately 4% of the total Ministry of Health Budget. However, financing for mental health is mostly donor-driven with a significant proportion of this total being made up of funding from the African Development Bank (ADB). At present, about 2% of the Ministry of Health budget is directed towards mental health, although it is difficult to assess the exact proportion due to the integrated nature of mental health services. In the absence of a predetermined budget for mental health funds are drawn from within the general primary health care budget for mental health services at this level. Table 7 represents MTEF allocation to the Health Sector during the HSSP II period. Despite the abolition of user fees in 2001 for minimum package services in GoU health units, household contributions through either out-of-pocket expenditure or health insurance equates to almost half of the total national health expenditure. It is estimated that nearly 5% of households in Uganda are experiencing catastrophic payments, while 2.3% are impoverished by medical bills. Household expenditure for people with mental illness may be up to 57 USD per year on mental health care. Relative to the per capita income of 89 USD this is a substantial amount. Mental disorders are not covered by existing social insurance schemes and it is unknown whether they will be covered under the proposed National Health Insurance Scheme (NHIS) (1, 19, 25). HUMAN RESOURCES Human resources for health (HRH) Management falls under the directive of two key divisions in the MoH, namely the Human Resource Development Division (HRDD) and Human Resources Management Division (HRMD). The primary functions of the HRDD are to develop policy, strategies and plans for HRH in addition to setting standards for the training of health specialists in collaboration with professional councils, local governments and the Ministry of Education and Sports (MoES). The role of the HRMD is to lead in the development of personnel management strategies and processes. Each division whist exclusive, often work together to contribute to effective delivery of the UNMHCP. The Health Service Commission (HSC) is an autonomous institution working on behalf of the MoH. It is responsible for recruitment and deployment of HRH and conditions of service. The recruitment of health workers for MoH HQ, National and Regional Referral Hospitals, Specialized Institutions under MoH and health workers for prison health services also fall under the jurisdiction of HSC. The function for district level health service delivery is carried out by the District Service Commissions (DSC) under the mandate of the 1997 Local Government Act. However, under the HSSP III, the MoH plans to lobby and promote further recentralisation of the recruitment and deployment of staff at district level, particularly the deployment of key health workers such as Medical Officers (1, 19).
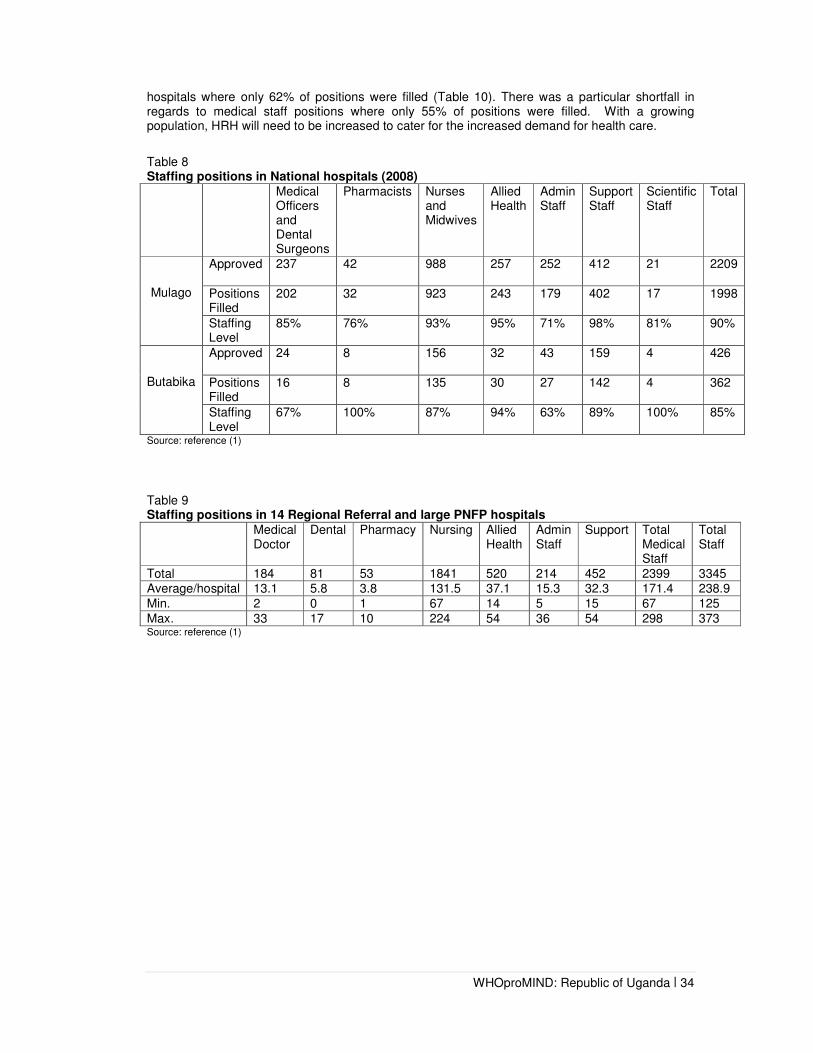
It can be seen from the table 8, 9, and 10 that overall there is a shortfall between staffing norms and actual positions filled within the health system. Table 8 reports staffing at national hospitals, table 6 reports at staffing regional referral hospitals, and Table 10 reports staffing at district hospitals. The shortfall of staffing was particularly evident at the 14 regional and large PNFP
WHOproMIND: Republic of Uganda | 34
hospitals where only 62% of positions were filled (Table 10). There was a particular shortfall in regards to medical staff positions where only 55% of positions were filled. With a growing population, HRH will need to be increased to cater for the increased demand for health care.
Table 8 Staffing positions in National hospitals (2008)
Medical Officers and Dental Surgeons
Pharmacists Nurses and Midwives
Allied Health
Admin Staff
Support Staff
Scientific Staff
Total
Mulago
Approved 237 42 988 257 252 412 21 2209
Positions Filled
202 32 923 243 179 402 17 1998
Staffing Level
85% 76% 93% 95% 71% 98% 81% 90%
Butabika
Approved 24 8 156 32 43 159 4 426
Positions Filled
16 8 135 30 27 142 4 362
Staffing Level
67% 100% 87% 94% 63% 89% 100% 85%
Source: reference (1)
Table 9 Staffing positions in 14 Regional Referral and large PNFP hospitals
Medical Doctor
Dental Pharmacy Nursing Allied Health
Admin Staff
Support Total Medical Staff
Total Staff
Total 184 81 53 1841 520 214 452 2399 3345 Average/hospital 13.1 5.8 3.8 131.5 37.1 15.3 32.3 171.4 238.9
Min. 2 0 1 67 14 5 15 67 125
Max. 33 17 10 224 54 36 54 298 373 Source: reference (1)

WHOproMIND: Republic of Uganda | 35
Table 10 Staffing positions in general hospitals. Data is based on HMIS reporting from 69 District Hospitals
Medical Doctor
Dental Pharmacy Nursing Allied Health
Admin Staff
Support Total Medical Staff1
Total Staff
Local Govt. Staffing Norms
7 4 3 116 28 14 13 158 185
Total in Post (data based on 63 hospitals)
261 120 86 3928 1041 603 1245 5436 7284
Average/hospital 4.1 1.9 1.4 62.3 16.5 9.6 19.8 86.3 115.6
Min. 0 0 0 2 0 1 0 12 23
Max. 12 6 6 192 40 29 123 216 272
Expected Total 441 252 189 7308 1764 882 819 9954 11655
Staff Gap (data based on 63 hospitals)
-180 -132 -103 -3380 -723 -279 426 -4518 -4371
% in post 2009/10
59% 48% 46% 54% 59% 68% 152% 55% 62%
Source: reference (1)
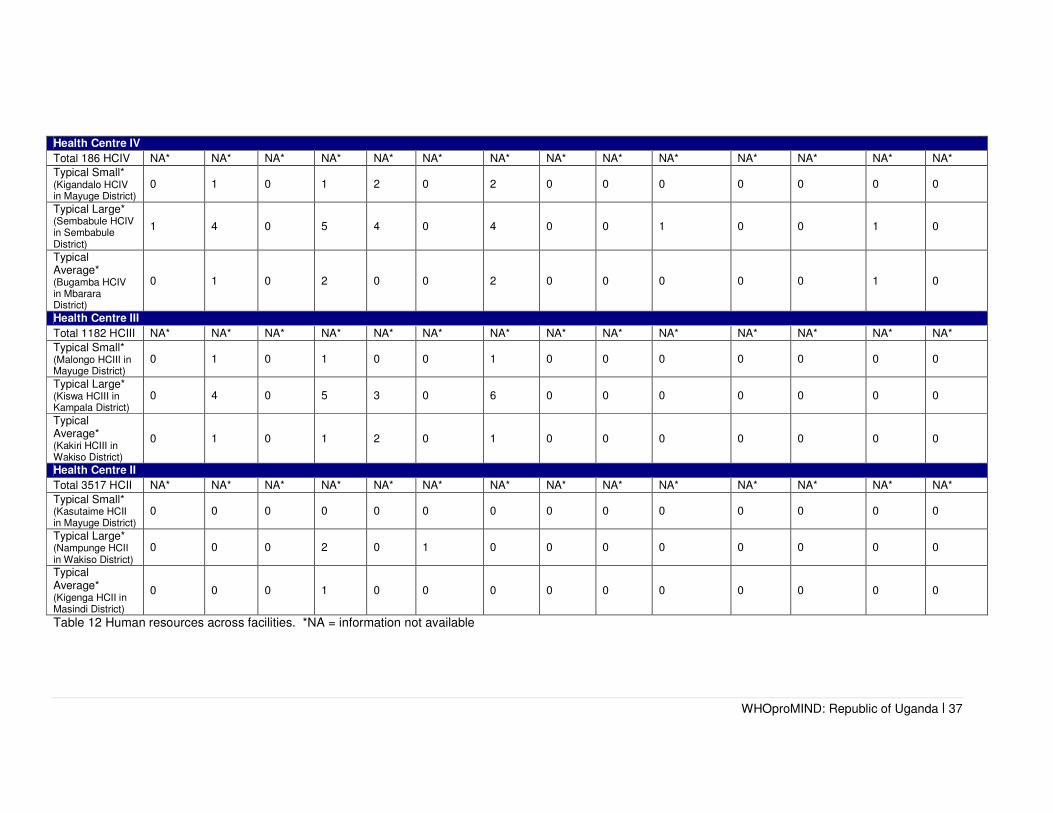
Table 11 shows the number of health workers across Uganda and specifically in the mental health sector. It is hard to clearly establish the total number of health workers based in the private sector and those in the public sector since many health workers are working in both. There are many nurses and midwives in the country who are not officially registered with the council. There are also many who are registered but are not practicing in the country. Registered nurses have higher nursing skills compared to enrolled nurses and they can prescribe wider medication. Psychiatric social workers are all working in the teaching hospitals. Table 12 reports and compares mental health and general health workers by facility level from the tertiary care level through to the health centre level. Both tables 11 and 12 show how few health workers are working in mental health compared to the entire health sector. Table 12, also demonstrates sparse human resources for mental health at lower levels of the health system. However at the same time Table 12 demonstrates the huge potential to integrate mental health into primary care at all health service levels. Table 11 Staffing levels of key general health and mental health cadres across Uganda (2010)
Medical Doctor
Clinical Officer
Pharmacist Nurse (27)
Social Worker
Clinical Psychologist
Occupational Therapist
Numbers working in general health
3624
Not
available
277
18,960 (enrolled)**
11,097 (registered)**
6
Not
applicable
53
Numbers working in mental health
36
216
(insert their
correct name)
0
997 (enrolled)**
997 (registered)** Insert name/title
4***
Psychiatric social worker
20
0
Source: reference (28)
1 Total Medical staff only excludes nursing assistants, admin staff and support staff
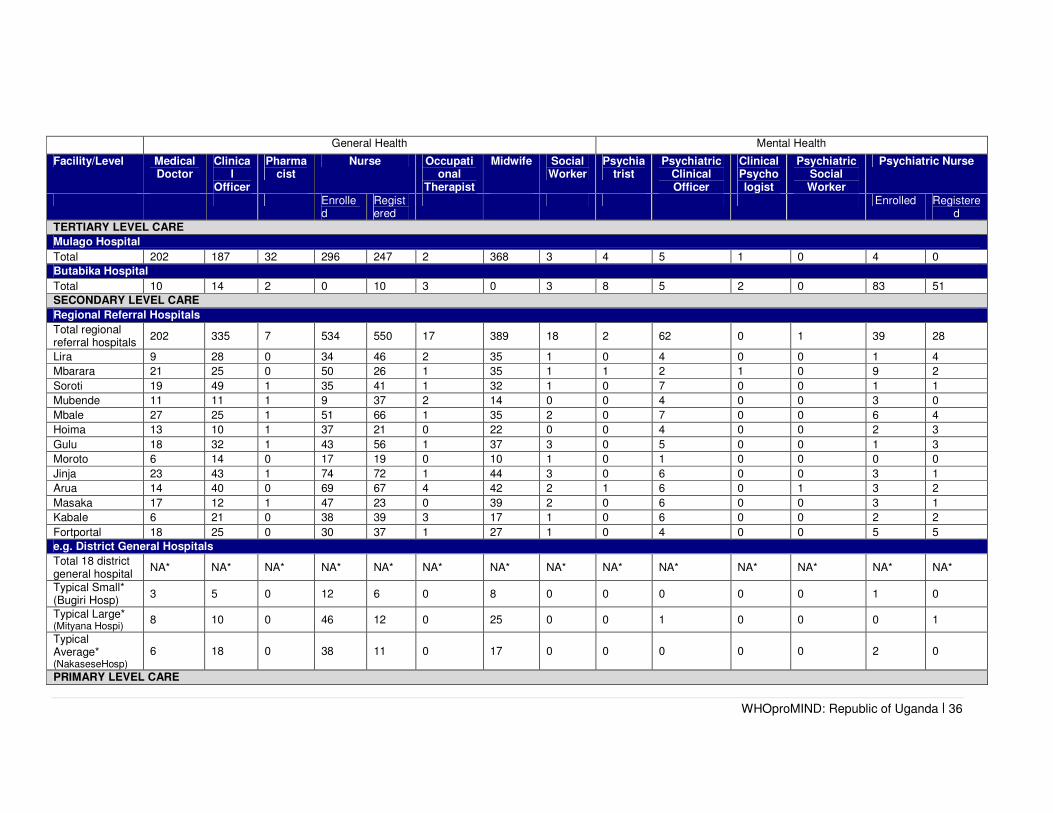
WHOproMIND: Republic of Uganda | 36
General Health Mental Health
Facility/Level Medical Doctor
Clinical
Officer
Pharmacist
Nurse Occupational
Therapist
Midwife Social Worker
Psychiatrist
Psychiatric Clinical Officer
Clinical Psychologist
Psychiatric Social Worker
Psychiatric Nurse
Enrolled
Registered
Enrolled Registered
TERTIARY LEVEL CARE
Mulago Hospital
Total 202 187 32 296 247 2 368 3 4 5 1 0 4 0
Butabika Hospital
Total 10 14 2 0 10 3 0 3 8 5 2 0 83 51
SECONDARY LEVEL CARE
Regional Referral Hospitals
Total regional referral hospitals
202 335 7 534 550 17 389 18 2 62 0 1 39 28
Lira 9 28 0 34 46 2 35 1 0 4 0 0 1 4
Mbarara 21 25 0 50 26 1 35 1 1 2 1 0 9 2
Soroti 19 49 1 35 41 1 32 1 0 7 0 0 1 1
Mubende 11 11 1 9 37 2 14 0 0 4 0 0 3 0
Mbale 27 25 1 51 66 1 35 2 0 7 0 0 6 4
Hoima 13 10 1 37 21 0 22 0 0 4 0 0 2 3
Gulu 18 32 1 43 56 1 37 3 0 5 0 0 1 3
Moroto 6 14 0 17 19 0 10 1 0 1 0 0 0 0
Jinja 23 43 1 74 72 1 44 3 0 6 0 0 3 1
Arua 14 40 0 69 67 4 42 2 1 6 0 1 3 2
Masaka 17 12 1 47 23 0 39 2 0 6 0 0 3 1
Kabale 6 21 0 38 39 3 17 1 0 6 0 0 2 2
Fortportal 18 25 0 30 37 1 27 1 0 4 0 0 5 5
e.g. District General Hospitals
Total 18 district general hospital
NA* NA* NA* NA* NA* NA* NA* NA* NA* NA* NA* NA* NA* NA*
Typical Small* (Bugiri Hosp)
3 5 0 12 6 0 8 0 0 0 0 0 1 0
Typical Large* (Mityana Hospi)
8 10 0 46 12 0 25 0 0 1 0 0 0 1
Typical Average* (NakaseseHosp)
6 18 0 38 11 0 17 0 0 0 0 0 2 0
PRIMARY LEVEL CARE
WHOproMIND: Republic of Uganda | 37
Table 12 Human resources across facilities. *NA = information not available
Health Centre IV
Total 186 HCIV NA* NA* NA* NA* NA* NA* NA* NA* NA* NA* NA* NA* NA* NA*
Typical Small* (Kigandalo HCIV in Mayuge District)
0 1 0 1 2 0 2 0 0 0 0 0 0 0
Typical Large* (Sembabule HCIV in Sembabule District)
1 4 0 5 4 0 4 0 0 1 0 0 1 0
Typical Average* (Bugamba HCIV in Mbarara District)
0 1 0 2 0 0 2 0 0 0 0 0 1 0
Health Centre III
Total 1182 HCIII NA* NA* NA* NA* NA* NA* NA* NA* NA* NA* NA* NA* NA* NA*
Typical Small* (Malongo HCIII in Mayuge District)
0 1 0 1 0 0 1 0 0 0 0 0 0 0
Typical Large* (Kiswa HCIII in Kampala District)
0 4 0 5 3 0 6 0 0 0 0 0 0 0
Typical Average* (Kakiri HCIII in Wakiso District)
0 1 0 1 2 0 1 0 0 0 0 0 0 0
Health Centre II
Total 3517 HCII NA* NA* NA* NA* NA* NA* NA* NA* NA* NA* NA* NA* NA* NA*
Typical Small* (Kasutaime HCII in Mayuge District)
0 0 0 0 0 0 0 0 0 0 0 0 0 0
Typical Large* (Nampunge HCII in Wakiso District)
0 0 0 2 0 1 0 0 0 0 0 0 0 0
Typical Average* (Kigenga HCII in Masindi District)
0 0 0 1 0 0 0 0 0 0 0 0 0 0

WHOproMIND: Republic of Uganda | 38
TRAINING
Training for health workers in Uganda involves both the Ministry of Health (MoH) and the Ministry of Education and Sports (MoES). The MoES is essentially responsible for pre-service training of health workers. The MoH addresses education and training of the existing health workforce to improve skills and technical competencies, quality performance, and productivity through basic, post-basic, post-graduate, and in-service training. The MoH works collaboratively with the MoES and other key HRH education and training stakeholders to effectively plan for and develop the required numbers and competences of HRH. It retains a role in defining standards to guide the MoES in specific health cadres and numbers of health workers to be trained (1, 15). The Uganda Nurses and Midwives Council is the statutory professional body responsible for regulation of the Nursing and Midwifery professions in the country. The basis of the training for all health staff is provided in table 13. It is a requirement for all doctors to renew their registration for practice every year and three years for nurses. There is a minimum required number of Continuing Medical Training Sessions per year before registration. These regulations apply to MH workers too (1). Post registration continuing professional development is/is not required. Table 13 Training requirements of key general health and mental health professionals
Gen
era
l H
ealt
h
Cadre of Staff Undergraduate Training ( years)
Postgraduate Training ( years)
Total Duration of Training ( years)
Any post Continuing Professional Development Required?
Number students entered training in [2010]
Number of students graduated in [2010]
Medical Doctor
5
Not applicable
No 164 149
Clinical Officer
3 No
Pharmacist 5 No 32 23
Nurse Enrolled 2 No NA* NA*
Registered 3 No NA* NA* Occupational Therapist
3 No NA* NA*
Social Worker 3 No NA* NA* Midwife 2.5 No NA* NA*
Neurologists 5 3 8 No NA* NA* Neurosurgeons
5 3 8 No NA* NA*
Men
tal
Healt
h
Psychiatrist 5 3 8 No 2 2 Psychiatric Clinical Officer
Clinical Officer (3 years)
2 years Full-time residential Diploma in Mental Health
5 CPD required if chance arises
14 21
Clinical Psychologist
3 2 5 - 0 2
Psychiatric Social Worker
3 3 6 3 0
Psychiatric Nurse
Enrolled 2.5 - - CPD required if chance arises
126
Registered 4.5 - - CPD required if chance arises
45
(NA = data not available)

WHOproMIND: Republic of Uganda | 39
The total number of professionals who graduated in 2005 from academic and educational institutions in Uganda was 162 general medical doctors, 4 psychiatrists, 13 psychologists with at least one year training in mental health and 1491 nurses registered with the nurses and midwives council (25). There are 2 neurologists in the country and one of them was trained outside the country. There are 5 neurosurgeons in the country and all of them were trained outside. One of the key functions of Butabika National Referral Hospital is to provide mental health training to students in mental health care. During the financial year 2009/2010 a total of 1812 students were trained at Butabika hospital from various institutions (Makerere University – School of Health Science, Kampala University, Kampala International University, Uganda Christian University, Aga Khan University, Paramedical Schools: School of Psychiatric Clinical Officers Butabika, Medicare Health Professional College Mengo, Health Tutors’ College and Nurses Training Schools of Masaka, Matany, Mengo, Mulago, Kalong, Rakai, Rubaga, Kiwoko, Kibuli, Nsambya and Butabika) (1). Table 14 summarizes the mental health training and seminar activities at one hospital. Mulago hospital has a department of Psychiatry that shares teaching activities with Butabika hospital. However, key challenges to the effective delivery and roll-out of training on mental health for health workers remain including the critical shortages of tutors, inadequate infrastructure and shortages in funding. After a review of curricula for medical training in Ugandan education institutions, the number of hours of exposure to mental health issues was increased (17). Medical doctors now receive minimum of 4 weeks training at medical schools and are evaluated on examination at the end of their rotations. Clinical Officers receive lectures and are required to go through three week rotations in mental health but the post of Psychiatric Clinical Officer necessitates a two-year full-time residential Diploma in mental health. There are two courses for Psychiatric Nurse training in Uganda namely enrolled and registered. All Psychiatric Nurses are trained at Butabika Hospital. General nurses, midwives, occupational therapists and health care workers with the authority to write prescriptions receive orientation training in mental health with a component for recognition and referral. Each health worker must spend time at Butabika or a regional referral hospital in a mental health unit during rotations. All health care workers receive a written examination paper on mental health. Social workers receive some lectures and do a 2 weeks placement at mental hospitals, but this is optional. All village health teams are trained in the delivery of the 12 areas of the UNMHP of which mental health is one such unit. A training manual developed by the Department for Health Promotion and Education exists for village health teams with a module on mental health, which describes the causes of mental disorders and the advice they should provide to patients and their carers (29). There are nursing assistants formerly known as nurse aides. They are not formally trained or qualified, however, do play vital roles especially at Health Centre II and I. Table 14 Summary of mental health training and seminar activities at Butabika Hospital
Source: reference (1)

WHOproMIND: Republic of Uganda | 40
MEDICATIONS
The National Therapeutic Drug Policy was formulated in 1993. The policy was reviewed in 1996 and 2001. The financing of medicines and health supplies has recently undergone change effective financial year 2009/2010 when the GoU shifted financing away from decentralized primary health care through the recurrent wage grant and essential medicines account credit line. The NMS is now the official sole supplier for Essential Medicines and Health Supplies (EMHS) to all GoU facilities. MoFPED pays NMS a standard handling fee based on the value of commodities procured: 18% on EMHS, 7% Artemisinin Combination Therapies (ACTs), and Antiretroviral Drugs (ARVs). The increasing contribution of global health initiatives such as Global Fund, PEPAR, CHAI and GAVI are not included (1). Access to essential psychotropic medicines in all public health facilities in Uganda is free. However, frequent drug stock outs result in either no access to essential drugs or out-of-pocket payment estimated at 37% of the daily minimum wage needed to pay for one anti-psychotic drug and 7% of the daily minimum wage to pay for one-day dose of antidepressant medication. Only some physician based primary health care clinics (21-50%) had at least one psychotropic medicine in each therapeutic category (anti-depressant, anti-psychotic, mood stabilizers, anxiolytic and anti-epileptic) compared to non-physician based primary health care clinics (1-20%). At the health centre IV level, only 30% had the supply of at least one anti-psychotic, one anti-depressant and one anti-epileptic drug in stock at the same time. Inadequate financing, lack of human resources and poor management of medicines at the health unit level continue to hinder the delivery of access to medicines at health facilities. As of the 2009-2010 financial year, the situation improved due to the fact that the Ugandan government doubled the budget for psychotropic medications and NMS became involved in their distribution. Subsequently, most HC IVs have at least one anti psychotic and antidepressant (25, 30, 31). Table 15 summarizes psychotropic medication availability at various health centres. Table 15 Psychotropic medication availability at different health centre levels
Source: reference (1)
All trained health workers, including general doctors, nurses and midwives, are permitted to prescribe psychotropic medication on the Uganda Essential Drug List. The Ministry of Health’s guidelines allow general health workers to prescribe and administer psychotropic medicines for chronic patients, after the treatment has been initiated by a mental health professional. General health workers are usually not allowed to prescribe injectable psychotropic medicines or newer atypical antipsychotic medication, however injections are permitted to control highly aggressive patients (17). Table 16 compares the recommended psychotropic medications, official policy and practical availability in Uganda.

WHOproMIND: Republic of Uganda | 41
Table 16 Comparison of recommended psychotropic medications, official policy and practical availability in Uganda, see Appendix for more detail on WHO EPM List
INFORMATION SYSTEMS
Uganda's Health Monitoring Information System (HMIS) is managed by the MoH to monitor and evaluate health sector performance and trends. A revised HMIS tool was introduced in 2006 to monitor district level health care delivery. As part of the HMIS, reporting by the district health manager was reported to be done to the Ministry of Health headquarters on a monthly basis. The proportion of districts submitting HMIS monthly returns on time for the financial year 2009/10 is 84% and thus below the HSSP II target of 100%. However, a positive trend in data reporting can be seen due to efforts of training district managers in HMIS systems. A great improvement in reporting, in the area of mental health was observed following the recruitment of mental health staff and orientation of general health workers in mental health. Currently routine HMIS reports are available on 6 conditions namely schizophrenia, depression, mania, childhood mental disorders, anxiety disorders, alcohol and drug abuse, epilepsy and other mental health disorders. Data from HIMS reports from 2008 to 2011 show an increase in new patients treated for mental health (see table 17 below) (1, 14, 25).
Drug
WHO Essential Psychotherapeutic Medicines 2009 (32)
UGANDA National Essential
Medicines List (33)
Chlorpromazine � �
Haloperidol � �
Fluphenazine � �
Amitriptyline � �
Fluoxetine � �
Diazepam � �
Clomipramine � X
Carbamazepine � �
Sodium Valproate � �
Lithium Carbonate � �
Methadone � X
Nicotine replacement therapy � �

WHOproMIND: Republic of Uganda | 42
Table 17 HIMS Data on mental health from the Annual Health Sector Performance Report FY 2010/2011
Diagnosis
2008/20009 2009/2010 2010/2011
No. % of total OPD
No %of total OPD
No. % of total OPD
Epilepsy 176,851 0.6% 185,709 0.55 194,018 0.6%
Other forms of mental illness
24,257 0.08% 29,147 0.08% 32,578 0.09%
Anxiety disorders 20,456 0.06% 21,448 0.06% 23,693 0.075
Depression 18,744 0.06% 20,523 0.06% 22,069 0.06%
Mania 13,591 0.04% 12,546 0.03% 17,290 0.05%
Schizophrenia 10,272 0.03% 9,429 0.03% 13,722 0.04%
Alcohol and drug abuse 9,508 0.03% 8,632 0.02% 12,361 0.04%
Total 237,709 0.9% 287,434 0.78% 315,731 0.95%
Source: reference (34)
WHOproMIND: Republic of Uganda | 43
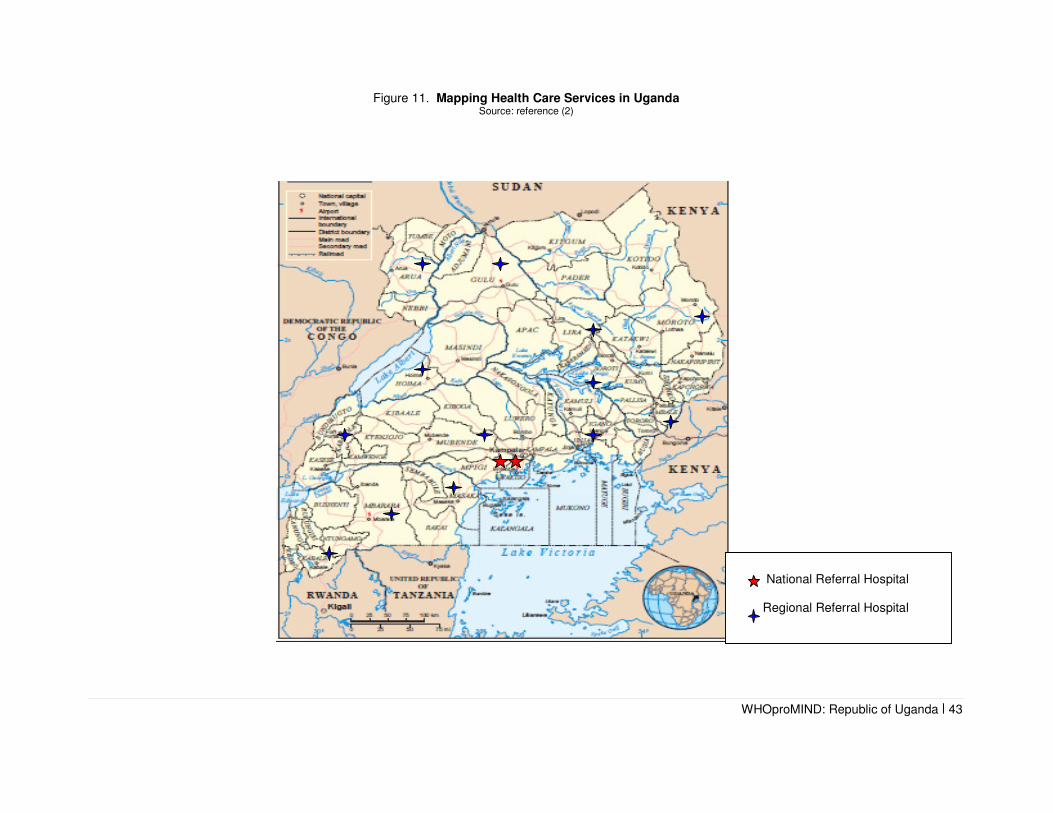
Figure 11. Mapping Health Care Services in Uganda Source: reference (2)
National Referral Hospital Regional Referral Hospital

WHOproMIND: Republic of Uganda | 44
FACILITIES AND SERVICES
The organization of services is schematically represented in Figure 12(a) and (b), and described below.
Long stay facilities and specialist services
Butabika National Referral Hospital was established in 1955 and is the only National Mental Health Hospital in Uganda. Butabika is also a teaching and research hospital in the field of mental health. The total bed capacity is 550 patients. There are no beds reserved specifically for children, adolescents and elderly. In addition, General Outpatient services (in addition to mental health services) are provided to people from the local population within a 10km surrounding area in an effort to combat mental health related stigma. In the financial year 2009/2010, Butabika provided inpatient mental health care to 4 394 first time admissions and 1 752 readmissions. All 80 forensic beds in Uganda are located within Butabika Hospital with 0.42 beds per 100 000 population. 10% of the beds are occupied by mentally-ill offenders. This category is for long-stay patients with a few spending 5 years in the unit (1, 29). There is 1 alcohol and drug rehabilitation centre at Butabika Hospital and 3 at private facilities. Butabika hospital also has a day treatment centre for child psychiatry. Multidisciplinary teams consisting of psychiatrists, clinical psychologists, psychiatric social workers, psychiatric clinical officer, psychiatric clinical nurses and occupational therapists staff the hospital.
Mulago Hospital is also a national referral hospital and provides out patients and inpatients mental health services, teaching and researches. It also has multidisciplinary teams consisting of psychiatrists, clinical psychologists, psychiatric social workers, psychiatric clinical officer, and psychiatric clinical nurses. Like Butabika hospital, it also has a day treatment centre for child psychiatry.
There is a psychiatric service within prison health services and this is where most patients who have been involved in crimes are seen.
Psychiatric services within general hospitals
There are 13 regional referral hospitals and as of the financial year 2007/08, they all have mental health units (Figure 11). In addition they provide outreach services, outpatients, and inpatient services. These services are provided by psychiatric clinical officers and psychiatric nurses. Three of the 13 regional hospitals have resident psychiatrists. In the remaining 10 regional hospitals, psychiatrists provide supervisory visits every 3 months. There are 144 district general hospitals. They provide in-patient mental health services as part of general wards and also provide a liaison psychiatry service. In addition they are responsible for providing weekly mental health clinics and outreach services to the communities. At most of the large district hospitals there are psychiatric clinical officers or a registered psychiatric nurse who provides mental health services under supervision of the regional hospitals and visiting psychiatrists who visit there every 3 months. An average sized district hospital might be staffed by a couple of enrolled psychiatric nurses, and a small sized district hospital might be staffed by one enrolled nurse (see table 12).
Formal community mental health services
There are no community services such as day care centres, work employment programs, rehabilitation programs, or crisis programs in the communities.
Mental health services through primary health care
There are 188 Health Centre IV and each covers 100,000 population. At HC IV, medical doctors, clinical officers and registered nurses are providing general health care. Weekly outpatient clinics, outreach services in the communities, and admissions to general wards are provided. Approximately 70% of HC IV has 1 psychiatric enrolled nurse and are providing basic mental health services. The service includes diagnosing and managing common mental disorders such as depression, bipolar disorder, anxiety disorders and also psychosis and epilepsy. The psychiatric nurses also provide brief intervention for alcohol abuse and attend HIV/AIDS clinics.

WHOproMIND: Republic of Uganda | 45
There are 1182 Health Centre III and it covers 20,000 population each. At HC III, for patients with psychiatric disorders emergency treatments and referrals are provided and for patients with epileptic disorders follow up care is provided based on diagnosis that has been made at higher
levels. Health education and awareness raising on mental health in the communities are also provided. These services are usually provided by 1 general clinical officer and registered nurses. In some districts like Kisoro district, only a psychiatric nurse provides the services. 20% of health care providers at HC III have received intensive service training from Ministry of Health and NGOs such as Basic Needs and TPO Uganda. The basic minimum package that is used at HCV III includes psychiatric drugs such as chlorpromazine, amitrytptylline, phenytoin, phenobarbitone and diazepam and they are used to treat psychosis, depression, epilepsy and anxiety disorders.
There are 3517 Health Centre II and it covers 5000 population each. At HC II, services such as follow up care for patients diagnosed at higher level, treatment of epilepsy without complications, sedation of violent patients in preparation for referral, and organizing outreach services for higher level are available. The same basic kit as HCV III is available here. The majority of HC II is served by 1enrolled nurse. Also nursing assistants or nursing aides is serving at HC II even though they are not qualified nurses.
Table 18 shows that the number of people with mental disorders seen at Ntete Health Centre II. The Health Centre started its mental health service in 2004 and the number of people accessing treatment and care has increased over time.
Table 18 Number of people seen at Ntete Health Centre II for different mental disorders ( 2003-2007)
2003 2005 2006 2007
Schizophrenia 0 16 10 17
Bipolar Disorder 0 18 12 22
Depression 0 8 6 13
Alcohol Abuse 0 2 1 1
Epilepsy 0 283 343 262
Total 0 327 369 315
Each Health Centre I covers 1000 population. At HC I (Village Health Team), the services such as identification and referral of psychiatric cases, receiving patients for resettlement and psycho education to patients and families are provide. These services are provided by VHT members or community health workers. It is estimated that 20% of VHT member has gone through some type of mental health training in their districts.
Informal community care
Traditional healers
Traditional healers were reported to be key health care providers in the provision of mental health services. It was found that traditional healers were often the first source of help for patients with mental health problems, especially in communities where mental health professionals are not readily available.
It has been estimated that approximately 60% of Uganda’s population seek care from TCMPs before visiting the formal sector. Most TCMPs have no functional relationship with public and private health providers. This results into late referrals, poor management of various medical, surgical, obstetric conditions and high morbidities and mortalities. A regulatory bill and policy framework for TCMPs is awaiting cabinet approval (25).

WHOproMIND: Republic of Uganda | 46
A study in north and north-east Uganda indicated that 59% of respondents went to religious leaders for help with depression, compared with 0.6% who went to traditional healers, and 2.3% who went to health facilities (17).
Non-government organizations (NGOs)
NGO involvement with mental health in the country exists. NGOs are mainly involved in advocacy, promotion, prevention, treatment and rehabilitation. There is some increase in NGO participation in capacity building and primary mental health care provision. Consumer support groups for mental health are also emerging. They are involved particularly with psychosocial care to war-afflicted populations. NGOs are also carrying out research in mental health (30). NGO services working in mental health in Uganda include Basic Needs and the Transcultural Psychosocial Organization. Basic Needs Uganda is an NGO working with mentally ill people, communities, partner organizations and primary health care workers to improve the quality of life of mentally ill persons by ensuring that basic needs and rights of mentally ill persons are met. Basic Needs work spans research, capacity building, and improving access to community based-treatment for mentally ill persons, poverty reduction, and targeting stigma associated with mental illness. The Transcultural Psychosocial Organization (TPO Uganda) provides psychosocial support and mental health care to communities, families and individuals in conflict and post conflict settings. TPO services are delivered through a community oriented intervention model, which mainly focuses on identifying existing community support structures, traditional circles of support and building their capacity to identify and participate in supporting the psychosocial and mental health needs of; children in need of protection, survivors of gender based violence, children and families infected and affected by HIV/AIDs and families whose socio –economic wellbeing has been debilitated by conflict and/or any other disaster.
Private Not-For-Profit Sub-Sector (PNFPs): The PNFP sector in Uganda is prominently present in rural areas. The PNFP sub-sector is divided into two categories: Facility-Based (FB-PNFPs) and the Non-Facility Based PNFPs (NFB-PNFPs). The FB-PNFPs provide both curative and preventive services. The FB-PNFPs account for 41% of the hospitals and 22% of the lower level facilities complementing government facilities especially in rural areas. NFB-PNFPs mainly provide preventive, palliative, and rehabilitative services. After several years of expansion in number and scope of their facilities, the subsector has now opted for a phase of consolidation of its services. The NFB-PNFP sub-sector is diverse and less structured comprising of hundreds of NGOs and Community Based Organizations (CBOs) that mainly provide preventive health services which include health education, counselling, health promotion and support to community health workers. PNFPs currently operate 70% of health training institutions. More than seventy five percent (75%) of the FB-PNFPs exist under 4 umbrella organizations: the Uganda Catholic Medical Bureau (UCMB), the Uganda Protestant Medical Bureau (UPMB), the Uganda Orthodox Medical Bureau (UOMB) and the Uganda Muslim Medical Bureau (UMMB) (19). Not all PNFP’s provide mental health services. Kisizi Hospital which is under Protestant Medical Bureau has a well-organized and facilitated mental health services in the country fully equipped with a ward and out- patient facilities.
Faith-based organizations
It has been reported that faith-based organizations are an important source of help for people with mental health problems in the community as they provide counselling and advice as well as making appropriate referrals (25).
Mental health services users or family associations
In total, Uganda has 2225 consumers who are members of user associations. The precise number of family membership to family associations is unknown. However, in relation to the total number of consumers who are members of user associations, only a few mental health facilities interact with such organizations. Consumer associations have been involved in formulation and implementation of the mental health policy and plan to some extent and are involved in current review of Mental Health Act (1).

WHOproMIND: Republic of Uganda | 47
Self-care and family-care
Mental health units in regional referral hospitals strongly encourage a relative to participate in the care of admitted mental health patients. Accommodation and kitchen facilities are provided at each regional mental health unit to for use by accompanying carers of admitted patients. However, concern has been raised that no specific budget for food for unaccompanied mental health patients exists except at a few hospitals. Figure 12 illustrates the WHO pyramid of ideal care versus the current state of care in Uganda.
Briefing sessions on patient care including drug administration are organized for relatives to promote family participation in the mental health care of the patient in an effort to reduce stigma and abandonment of family members at mental health facilities (29).

WHOproMIND: Republic of Uganda | 48
Figure 12. The WHO Pyramid of Care and the reality in Uganda Source: reference (35)
Figure 12a showing the ideal structure for mental health care in any given country.
Figure 12b illustrates the reality of mental health care in Uganda. The levels of care that are non-existent, poorly developed or inappropriate have been removed from the pyramid of care.

WHOproMIND: Republic of Uganda | 49
BIBLIOGRAPHY
INTERNET RESOURCES
Mental health and development: Targeting people with mental health conditions as a vulnerable group http://www.who.int/mental_health/policy/mhtargeting/en/index.html Improving health systems and services for mental health http://www.who.int/mental_health/policy/services/mhsystems/en/index.html WHO/Wonca joint report: Integrating mental health into primary care - a global perspective http://www.who.int/mental_health/policy/Integratingmhintoprimarycare2008_lastversion.pdf WHO Resource Book on Mental Health, Human Rights and Legislation. http://www.who.int/mental_health/policy/legislation/Resource%20Book_Eng2_WEB_07%20%282%29.pdf The WHO Mental Health Policy and Service Guidance Package http://www.who.int/mental_health/policy/essentialpackage1/en/index.html � The mental health context � Mental health policy, plans and programmes - update � Organization of services � Planning and budgeting to deliver services for mental health � Mental health financing � Mental health legislation & human rights � Advocacy for mental health � Quality improvement for mental health � Human resources and training in mental health � Improving access and use of psychotropic medicines � Child and adolescent mental health policies and plans � Mental Health Information Systems � Mental health policies and programmes in the workplace � Monitoring and evaluation of mental health policies and plans World Health Report 2001: New Understanding, New Hope. http://www.who.int/whr/2001/en/index.html
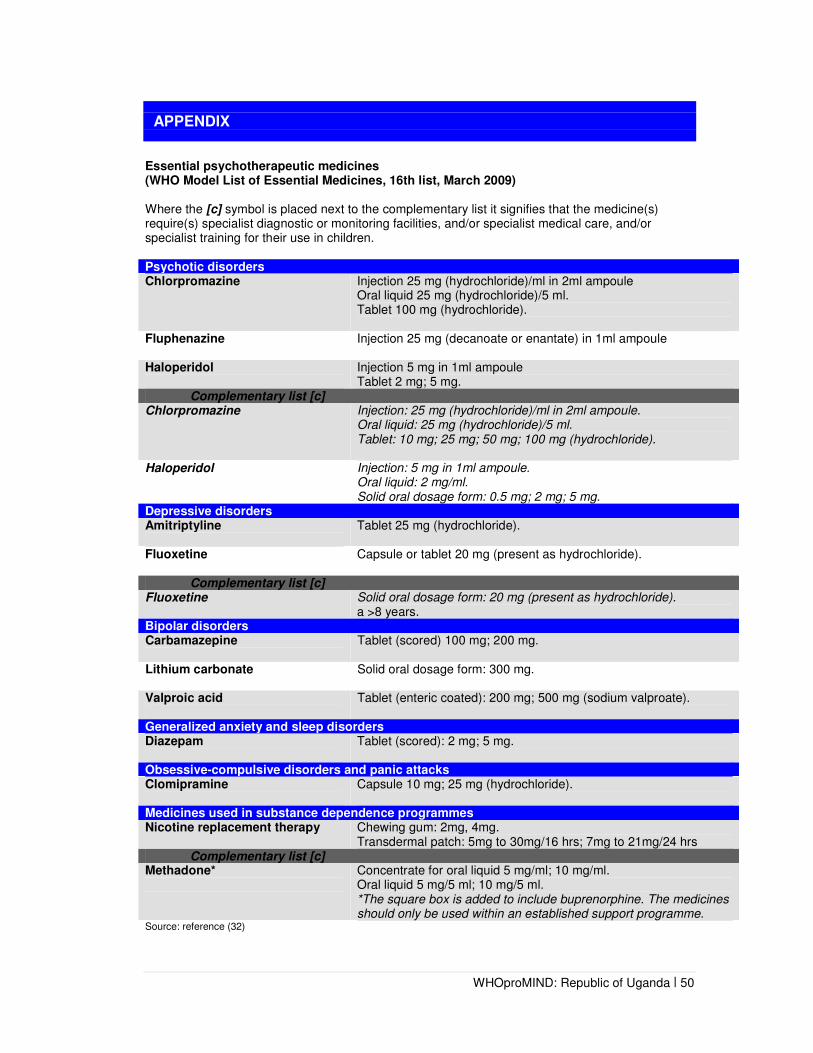
WHOproMIND: Republic of Uganda | 50
APPENDIX
Essential psychotherapeutic medicines (WHO Model List of Essential Medicines, 16th list, March 2009) Where the [c] symbol is placed next to the complementary list it signifies that the medicine(s) require(s) specialist diagnostic or monitoring facilities, and/or specialist medical care, and/or specialist training for their use in children. Psychotic disorders Chlorpromazine
Injection 25 mg (hydrochloride)/ml in 2ml ampoule Oral liquid 25 mg (hydrochloride)/5 ml. Tablet 100 mg (hydrochloride).
Fluphenazine Injection 25 mg (decanoate or enantate) in 1ml ampoule
Haloperidol
Injection 5 mg in 1ml ampoule Tablet 2 mg; 5 mg.
Complementary list [c] Chlorpromazine Injection: 25 mg (hydrochloride)/ml in 2ml ampoule.
Oral liquid: 25 mg (hydrochloride)/5 ml. Tablet: 10 mg; 25 mg; 50 mg; 100 mg (hydrochloride).
Haloperidol Injection: 5 mg in 1ml ampoule. Oral liquid: 2 mg/ml. Solid oral dosage form: 0.5 mg; 2 mg; 5 mg.
Depressive disorders Amitriptyline
Tablet 25 mg (hydrochloride).
Fluoxetine
Capsule or tablet 20 mg (present as hydrochloride).
Complementary list [c] Fluoxetine Solid oral dosage form: 20 mg (present as hydrochloride).
a >8 years. Bipolar disorders Carbamazepine
Tablet (scored) 100 mg; 200 mg.
Lithium carbonate
Solid oral dosage form: 300 mg.
Valproic acid
Tablet (enteric coated): 200 mg; 500 mg (sodium valproate).
Generalized anxiety and sleep disorders Diazepam
Tablet (scored): 2 mg; 5 mg.
Obsessive-compulsive disorders and panic attacks Clomipramine
Capsule 10 mg; 25 mg (hydrochloride).
Medicines used in substance dependence programmes Nicotine replacement therapy Chewing gum: 2mg, 4mg.
Transdermal patch: 5mg to 30mg/16 hrs; 7mg to 21mg/24 hrs Complementary list [c]
Methadone*
Concentrate for oral liquid 5 mg/ml; 10 mg/ml. Oral liquid 5 mg/5 ml; 10 mg/5 ml. *The square box is added to include buprenorphine. The medicines should only be used within an established support programme.
Source: reference (32)

WHOproMIND: Republic of Uganda | 51
REFERENCES
1. Government of Uganda, Ministry of Health. Annual health sector performance report, financial
year: 2009/10. Available from: http://www.health.go.ug/docs/AHSPR09.pdf.
2. United Nations Cartographic Section. Available from: http://www.un.org/depts/Cartographic/english/htmain.htm.
3. U.S. Department of State. Background notes on Uganda. 2011; Available from: http://www.state.gov/p/af/ci/ug/.
4. United Nations Development Programme. International human development indicators. Available from: http://hdr.undp.org/en/statistics/.
5. International Organization for Migration (IOM). Uganda: facts and figures. Available from: http://www.iom.int/jahia/Jahia/uganda.
6. United Nations Development Programme. Human development report. 2011; Available from: http://hdrundp.org/en/.
7. World Bank. Data Catalog. Available from: http://data.worldbank.org/data-catalog.
8. Uganda Ministry of Finance, Planning and Economic Development. Millenium development goals report for Uganda. 2010. Available from: http://planipolis.iiep.unesco.org/upload/Uganda/UgandaMDGReport2010.pdf.
9. Uganda Aids Commission. Available from: http://www.aidsuganda.org/.
10. Hagopian A, et al. The migration of physicians from sub-saharan Africa to the United States of America: Measures of African brain drain. Human Resources for Health, 2004, 2(17):2-10.
11. World Health Organization, Mental Health and Poverty Project. Mental health and development: targeting people with mental health conditions as a vulnerable group. 2010. Available from: http://whqlibdoc.who.int/publications/2010/9789241563949_eng.pdf.
12. The WHO World Mental Health Survey Consortium. Prevalence, severity, and unmet need for treatment of mental disorders in the World Health Organization Mental Health Surveys. The Journal of the American Medical Association, 2004, 291(21):2581-2590.
13. Uganda Bureau of Statistics. Available from: http://www.ubos.org/.
14. The Republic of Uganda, Ministry of Health. Health sector strategic plan II, 2005/06 – 2009/10 Volume I. Available from: http://www.who.int/rpc/evipnet/Health%20Sector%20Strategic%20Plan%20II%202009-2010.pdf.
15. Uganda National Tuberculosis Strategic Plan, 2006/07- 2010/11. Available from: https://country-matrix-repository.box.net/shared/8ege6g3yus#/shared/8ege6g3yus/1/42638103/434497025/1.
16. The Republic of Uganda Ministry of Health, World Health Organization. Service availability mapping. 2006. Available from: http://www.who.int/healthinfo/systems/samreportuganda.pdf.
17. World Health Organization, World Organization of Family Doctors. Integrating mental health into primary care: a global perspective. 2008. Available from: http://www.who.int/mental_health/policy/Integratingmhintoprimarycare2008_lastversion.pdf.
18. Hanson K, et al. Towards improving hospital performance in Uganda and Zambia: reflections and opportunities for autonomy. Health Policy, 2002, 61(1):73-94.
19. Government of Uganda, Ministry of Health. Health sector strategic plan III, 2010/11 – 2014/15. Available from: http://www.health.go.ug/docs/HSSP_III_2010.pdf.
20. World Health Organization Regional Office for Africa. WHO country cooperation strategy at a glance. 2008. Available from: http://www.afro.who.int/en/uganda/country-cooperation-strategy.html.
21. Kigozi F. Integrating mental health into primary health care – Uganda’s experience. South African Psychiatry Review, 2007, 10:17-19.
22. The Republic of Uganda, Ministry of Health. Annual health sector performance report, financial year 2006/7. Available from: http://www.health.go.ug/docs/AHSPR06.pdf.

WHOproMIND: Republic of Uganda | 52
23. World Health Organization Regional Office for Africa. WHO country cooperation strategy 2009-2014. 2009. Available from: http://www.afro.who.int/en/uganda/country-cooperation-strategy.html.
24. Uganda Ministry of Health. National Policy for Mental Health, Neurological and Substance Abuse Services (draft). 2010.
25. Mental Health and Poverty Project. Uganda country report. 2008. Available from: http://workhorse.pry.uct.ac.za:8080/MHAPP/public/public/resources/Uganda_report.
26. Uganda Debt Network. Uganda's poverty reduction strategy papers and resource allocation to the health sector. 2004.
27. The Uganda Nurses and Midwives Council. 2010.
28. The District Health Office, Uganda Ministry of Health. 2010.
29. Ndyanabangi S. Personal communication with Sheila Ndyanabangi: Mental Health Department, Ministry of Health Headquarters, Kampala, Uganda. 2011.
30. World Health Organization. Mental health atlas index. 2005; Available from: http://www.who.int/mental_health/evidence/mhatlas05/en/index.html.
31. World Health Organization, Ministry of Health Republic of Uganda. WHO AIMS report on mental health system in Uganda. 2006. Available from: http://www.who.int/mental_health/uganda_who_aims_report.pdf.
32. World Health Organization. WHO model list of essential medicines. 2009. Available from: http://whqlibdoc.who.int/hq/2009/a95055_eng.pdf.
33. Uganda Ministry of Health. Essential medicines list for Uganda. 2007. Available from: http://www.who.int/selection_medicines/country_lists/uga_eml_2007.pdf.
34. Government of Uganda, Ministry of Health. Annual health sector performance report, financial year: 2010/11. Available from: http://www.kampala.cooperazione.esteri.it/utlkampala/download/REPORT%20BOOK%202010-2011.pdf.
35. World Health Organization, World Organization of Family Doctors. WHO service organization pyramid for an optimal mix of services for mental health. In: Integrating mental health into primary care: a global perspective. 2008. p. 16.

WHOproMIND: Republic of Uganda | 53

WHOproMIND: Republic of Uganda | 54

WHOproMIND: Republic of Uganda | 55