document1
DESCRIPTION
daftar pustakaTRANSCRIPT

Acute diarrhea in adults Updated 2014 Apr 24 03:14:00 PM: review of acute infectious diarrhea in
immunocompromised adults (N Engl J Med 2014 Apr 17) WGO practice guideline on acute diarrhea in adults and children (National Guideline
Clearinghouse 2014 Mar 24) view update review of acute diarrhea (Am Fam Physician 2014 Feb 1)
Overview
assess hydration status and initiate rehydration therapy as necessary o rehydration therapy, ideally oral rehydration therapy, recommended as first
step for treating acute diarrhea (AFP Grade C)o consider IV rehydration for severe dehydration or hypovolemic shock if oral
route not possible, as well as mild dehydration accompanied by vomiting that precludes adequate
intake of ORS risk of aspiration (for example, patients with decreased consciousness)
consider serious and life-threatening causes if bloody stools, abdominal pain or distention, bilious vomiting, recent antibiotic use, or clinical shock
laboratory tests usually not needed in cases of acute uncomplicated, transient gastroenteritis with watery diarrhea
o reserve stool cultures for patients with (AFP Grade C) bloody stool severe dehydration evidence of inflammatory disease symptoms durating > 3-7 days imunosuppression suspected nosocomial infections
o other tests to consider based on illness severity or suspicion of diagnoses other than transient gastroenteritis, include
measurement of serum electrolytes complete blood cell count blood cultures urinalysis abdominal computed tomography sigmoidoscopy/endoscopy/colonoscopy esophagogastroduodenoscopy proctoscopy
antidiarrheal medications o antimotility or antiperistaltic agents (including loperamide) may reduce stool
volume and frequency but are contraindicated in patients with bloody diarrhea immunocompromised patients patients at risk for septicemia elderly patients with chronic lung disease

o combination of loperamide-simethicone recommended over monotherapy for faster and more complete relief of acute nonspecific diarrhea and gas-related discomfort (AFP Grade B)
antimicrobial medications o antibiotics, typically a quinolone, reduce the duration and severity of traveler's
diarrhea (AFP Grade A)o routine antimicrobial use not recommended but may be indicated for patients
with severe cholera, shigellosis, typhoid, and paratyphoid fever severe dysenteric presentation of Campylobacter enterocolitis or
Nontyphoidal salmonellosis in immunocompromised patients severe invasive amebiasis severe symptomatic giardiasis
probiotics may reduce duration of acute diarrhea in adults (level 2 [mid-level] evidence )
in adults with gastroenteritis, diarrhea typically lasts 5-7 days
General Information
Description
change in normal bowel movement characterized by passage of unusually soft or liquid stools ≥ 3 times in 24 hours (or > 250 g unformed stool/day)(1, 3, 4, 7)
duration of diarrhea < 14 days(1, 3, 4, 7) most cases of acute diarrhea in adults are mild, with no signs of blood or mucus, and
are typically caused by enteric pathogens(2)
Types
World Health Organization (WHO) recognizes 2 clinical types of acute diarrhea(1) o acute watery diarrhea (includes cholera )o acute bloody diarrhea (also called dysentery)
Definitions
acute diarrhea - duration < 14 days(7) persistent diarrhea - duration 14-29 days(3, 7) chronic diarrhea - duration ≥ 30 days(3, 7) dysentery (also called acute bloody diarrhea) - infection of intestinal tract resulting in
diarrhea containing blood or mucus (does not include occult blood or streaks of blood on surface of formed stool)(1)
gastroenteritis - usually refers to self-limited, enteric infectious disorder resulting in acute watery diarrhea or vomiting(2)
dehydration - excessive intracellular water loss due to hypertonic extracellular/intravascular fluid
hypovolemia - decreased intravascular blood volume, also called volume depletion

Incidence/Prevalence
in United Stateso 179 million cases of acute diarrhea reported annually, resulting in about 0.6
diarrheal episodes per person/year(7) o 48 million foodborne diarrheal illness reported annually (about 36% of all
cases of diarrhea), resulting in 128,000 hospitalizations(6, 7)
Risk factors
camping or consumption of untreated water(6) foods commonly associated with foodborne illness include(6, 7)
o produce (reported in 46% of cases), particularly contaminated leafy green vegetables
o fried riceo raw ground beefo raw or undercooked poultry, pork, or beefo seed sproutso raw milko seafood, particularly raw or undercooked shellfish
exposure to day care centers(6, 7) HIV infection or immunosuppression(6, 7) travel to developing country(6, 7) exposure to animals (such as reptiles [may harbor Salmonella], or pets with diarrhea,
or recent visit to farm or petting zoo)(4) fecal-oral sexual contact(4, 6, 7) receptive anal intercourse, with or without rectal pain or proctitis(4, 6, 7)
Differential Diagnosis
Serious and life-threatening conditions
hemolytic-uremic syndrome o preceded by infectious illness, often gastrointestinal (GI) infectiono patients with Escherichia coli O157:H7 infection may be at increased risko indicated by triad of
microangiopathic hemolytic anemia thrombocytopenia acute renal failure
(pseudomembranous colitis)o diagnosis suspected if
recent antibiotic use and typical symptoms diarrhea abdominal cramps fever leukocytosis
diarrhea ≥ 3-4 days after being hospitalizedo confirmation based on positive C. difficile testing from stool sample
toxic shock syndrome

o may be associated with wound infection, tampon use, Clostridium infectiono may be indicated by
nonspecific muscle aches faintness clinical shock red nonspecific rash possible site of bacterial entry such as small burn or injury
toxic megacolono complication of inflammatory bowel disease, C. difficile colitis, and some GI
infectionso may be indicated by gastric distention on clinical examination or imagingo Reference - Am J Gastroenterol 2003 Nov;98(11):2363
conditions which may present as an acute abdomen may include(2) o diverticulitis o appendicitis o peritonitis secondary to bowel perforationo acute mesenteric ischemia
Gastrointestinal infection
gastrointestinal (GI) infection is common cause of acute diarrhea in adults and classified as noninflammatory or inflammatory(2, 6)
noninflammatory diarrheal syndromes (usually without bloody stool) are typically viral but can be bacterial or parasitic, including(4, 6)
o norovirus infection most common cause of diarrhea in United States reported to account for
50% of outbreaks 26% of diarrhea treated in emergency departments 13% of office visits for diarrhea
o rotavirus gastroenteritis o enterotoxigenic , associated with traveler's diarrhea o enteropathogenic o cholera o diarrhea o food poisoning o giardiasis o cyclosporiasis o Aeromonas infection - typically watery and self-limited, but some patients
may have bloody diarrhea (J Infect Dev Ctries 2008 Apr 1;2(2):81 full-text )o cryposporidiosis - bloody stool relatively rareo balantidiasis - may be watery or bloody (Clin Microbiol Rev 2008
Oct;21(4):626 full-text )o Dientamoeba fragilis may be an overlooked cause of diarrhea (CMAJ 2006
Aug 29;175(5):468 full-text ), correction can be found in CMAJ 2006 Sep 26;175(7):777
inflammatory diarrheal syndromes (often presenting with bloody stool) are typically caused by invasive or toxic-producing bacteria, including(4, 6)
o Nontyphoidal salmonellosis

o shigellosis o enterocolitis o enterocolitis o enterohemorrhagic , including O157:H7 Shiga toxin-producing E. coli o enteroinvasive - mainly watery, but small proportion of patients may present
with bloody diarrheao enteroaggregative E. coli infection - typically watery, but some patients may
present with bloody diarrhea (Interdiscip Perspect Infect Dis 2010;2010:254159 full-text )
o infection - mucoid stool, no nausea/vomitingo amebiasis o schistosomiasis o CMV colitis o hemorrhagic fevers like dengue , Crimean-Congo hemorrhagic fever, Lassa
fever, Venezuelan hemorrhagic fever (Lancet 1991 Oct 26;338(8774):1033 ) see also Traveler's diarrhea
Gastrointestinal disease
inflammatory bowel diseaseo ulcerative colitis o Crohn's disease o collagenous colitis (rare)o microscopic colitis (rare)
irritable bowel syndrome (IBS) celiac disease lactose intolerance ischemic colitis (rare) colorectal cancer malabsorption gastrinoma (Zollinger-Ellison syndrome) VIPoma (pancreatic cholera) bowel obstruction radiation proctitis (radiation enteritis) McKittrick-Wheelock syndrome is rare disorder of volume and electrolyte depletion
from diarrhea caused by colonic neoplasm (J Emerg Med 2012 Sep;43(3):e171 , Am J Emerg Med 2007 Nov;25(9):1083.e1 , Eur J Gastroenterol Hepatol 2006 May;18(5):557 )
Extraintestinal infection
diarrhea may be 1 manifestation of certain extraintestinal infections includingo meningitis o pneumonia o urinary tract infection o adnexitis(2)
Endocrine disease

hyperthyroidism adrenocortical insufficiency carcinoid tumors (rare) medullary thyroid carcinoma (rare)
Drug-associated enteritis
antibiotics(6, 7) lactulose or laxative abuse(6) magnesium- or calcium-based antacids(6) chemotherapy(6, 7) colchicine (6) less commonly(6)
o proton pump inhibitorso mannitol o nonsteroidal anti-inflammatory drugs (NSAIDs)o angiotensin-converting enzyme (ACE) inhibitorso cholesterol-lowering medicationso lithium
Other causes
alcohol pelvic radiation therapy(6) systemic lupus erythematosus , related to Salmonella bacteremia or protein-losing
enteropathy (J Clin Gastroenterol 2011 May-Jun;45(5):436 ), also called lupus protein-losing enteropathy (LUPLE) (Rheumatol Int 2011 Aug;31(8):995 )
acute panautonomic neuropathy (Nan Fang Yi Ke Da Xue Xue Bao 2010 Apr;30(4):900 [Chinese])
rarely graft versus host disease (GVHD) or posttransplant lymphoproliferative disorder (Liver Transpl 2005 Aug;11(8):881 full-text )
estuary-associated syndrome, related to toxin-forming dinoflagellates (Environ Health Perspect 2001 May;109(5):539 PDF )
History and Physical
History
most patients with acute diarrhea self-manage their symptoms and do not present for medical evaluation(7)
thorough history is critical for(1, 3, 4) o patients with significant diarrheal illness (profuse, dehydrating, febrile, or
bloody diarrhea)o immunocompromised patients
important clinical features(1, 2, 3, 4) o symptom onset (abrupt or gradual) and duration of diarrhea (food poisoning
often associated with acute onset)o severity of diarrhea - may be assessed by disturbance in daily activitieso stool characteristics (watery, bloody, mucus, purulent, greasy, or bilious)

o frequency of bowel movements and relative quantity of stool producedo dysenteric symptoms, including
fever (including duration and severity) tenesmus blood or pus in stool
o symptoms of dehydration, including thirst nausea or vomiting headache muscle cramps dizziness altered mental status
o other associated symptoms, including abdominal pain myalgias unexplained weight loss
o dietary factors including pre-illness feeding practices change in diet or relationship to meals recent oral intake possible exposure to tainted food (for example, raw or undercooked
meats, eggs or shellfish, unpasteurized milk or juices) ask about important epidemiological factors(4, 6, 7)
o exposure to daycare or senior-care centerso exposure to other ill personso consumption of untreated fresh surface water (such as while swimming or by
drinking lake or stream water)o exposure to animals (such as reptiles [may harbor Salmonella], or pets with
diarrhea, or recent visit to farm or petting zoo)o recent travel, including to developing areaso current or recent hospitalizationo recent or regular medication use (including antibiotics, antacids, antimotility
agents, chemotherapy, colchicine , laxatives, lactulose)o underlying medical conditions associated with acute and chronic diarrheal
illness including gastrointestinal (GI) disease HIV infection carcinoid tumors immunosuppressive medication use prior gastrectomy extremes of age
o sexual activity including receptive anal intercourse or oral-anal sexual contacto occupation as caregiver or food handlero history of radiation therapy to abdomen or pelvis
Physical
consider abnormal vital signs(2, 4) o fever

o orthostatic pulse and blood pressure changeso respiratory rateo tachycardia (may indicate moderate-to-severe dehydration)
look for (may be masked or absent in older adults)o dry mucous membraneso sunken-appearing eyeso increased capillary refill time
assessed by pressing fingernail for 5 seconds and releasing observe time required for color to return to normal capillary refill time of 1-3 seconds is normal
o decreased skin turgoro hypotensiono orthostatic changes - decrease in blood pressure and/or increase in heart rateo tachycardiao weak and thready peripheral pulseso flat neck veins in supine positiono oliguriao functional signs of dehydration (change in mental status or falls)o Reference - Nursing 2009 Apr;39(4):14 o see also Dehydration and hypovolemia in adults
also assess(2) o abdomen to exclude peritonitiso rectum to identify stool character and possible presence of blood
Diagnostic Testing
Testing to consider
testing usually not needed in adults with acute uncomplicated, transient gastroenteritis with watery diarrhea(1, 2, 6)
microbiological stool investigation o microbiological stool investigation not usually necessary , especially in
immunocompetent patients presenting within 24 hours after onset of acute, watery diarrhea
o no rapid stool studies (leukocytes, lactoferrin, or occult blood) appear to be useful in developing countries, but microscopy for fecal leukocytes might predict patients with bacterial gastroenteritis in developed countries (level 2 [mid-level] evidence )
o reserve stool cultures for patients with (AFP Grade C) bloody stool severe dehydration evidence of inflammatory disease symptoms durating > 3-7 days imunosuppression suspected nosocomial infections
other tests to consider based on illness severity or suspicion of diagnoses other than transient gastroenteritis, include
o measurement of serum electrolyteso complete blood cell count

o blood cultureso urinalysiso abdominal computed tomographyo sigmoidoscopy/endoscopy/colonoscopyo esophagogastroduodenoscopyo proctoscopy
Microbiological stool investigation
General information
microbiological stool investigation not usually necessary in immunocompetent patients presenting within 24 hours after onset of acute, watery diarrhea(3, 4)
indications for stool testingo consider microscopy of fresh stool in certain cases(2)
microscopic red blood cells and white blood cells > 20 cells per high power field may predict early cases of bloody diarrhea
may help distinguish shigellosis from amebiasis in patients with gross bloody diarrhea
positive dark-field microscopy for shooting bacteria suggests Vibrio species
o additional factors which may warrant microbiological stool investigation (including cultures and other tests)
acute diarrhea with fever ≥ 101.3 degrees F (38.5 degrees C)(7) elderly or immunocompromised patient, and/or systemic illness(3, 4, 7) dehydration(4) recent antibiotic use (testing only)(4, 6, 7) day care exposure(4, 7) patient employed as food handlers(7) patients in nursing home(7) persistent diarrhea durating ≥ 14 days(7) cholera-like watery diarrhea, dehydration, and dysentery(7) public outbreak of diarrhea(7)
if stool sample necessary(7) o single stool sample obtained by patient and evaluated by licensed laboratory is
usually sufficiento additional stool samples may be necessary for
patients with inflammatory bowel disease and possible Clostridium difficile associated diarrhea
patients with persistent diarrhea due to likely parasitic infection (requires 3 separate stool samples)
o stool sample should be processed within 4 hours after passage if using direct microscopic exam to detect
parasitic organisms within 12 hours after passage if using routine microbiological methods
Infectious Diseases Society of America (IDSA) recommends selective approach to microbiological fecal studies (IDSA Grade B-II)(4)
o if suspicion of community-acquired or traveler's diarrhea (especially if significant fever or bloody stool), culture or test for

Salmonella Shigella Campylobacter Escherichia coli O157:H7 (plus Shiga toxin if blood in stool) Clostridium difficile toxins A and B (if recent antibiotics or
chemotherapy)o if suspicion of nosocomial diarrhea (onset after > 3 days in hospital)
test for C. difficile toxins A and B if bloody stool or suspected nosocomial outbreak, add Salmonella,
Shigella, Campylobacter, and E. coli O157:H7 (plus Shiga toxin)o if duration of diarrhea > 7 days (especially if immunodeficiency), consider
testing for parasites - Giardia, Cryptosporidium, Cyclospora, Isospora belli
inflammatory screen (including fecal lactoferrin testing or microscopy for leukocytes)
in patients with HIV infection, test for Microsporidia (Gram-chromotrope), Mycobacterium avium complex, Salmonella, Shigella, Campylobacter, E. coli O157:H7 (plus Shiga toxin), and C. difficile toxins A and B
o consider noninfectious or extraintestinal causes if diagnostic evaluation fails to identify pathogen
culture confirmation of Shiga toxin enzyme immunoassay-positive specimens recommended
o E. coli O157:H7 and other strains of E. coli that produce Shiga toxin are collectively known as Shiga toxin-producing E. coli (STEC)
o specific strain identification allows tracing of source during outbreako culture confirmation can identify false-positive enzyme immunoassayo Reference - MMWR Morb Mortal Wkly Rep 2006 Sep 29;55(38):1042 full-
text microscopy appears more sensitive than ELISA for stool testing for
Cryptosporidium (level 2 [mid-level] evidence ) o based on cohort study without independent reference standardo 72 immunocompromised patients with acute or chronic diarrhea had stool
specimens tested by microscopy with modified Ziehl-Neelsen technique (acid fast staining) and by ELISA for detection of Cryptosporidial coproantigen
o microscopy was positive in 11 cases, of which ELISA was positive in 4 caseso compared to microscopy ELISA had 36% sensitivity, 100% specificity, 100%
positive predictive value, and 90% negative predictive valueo Reference - Indian J Med Microbiol 2008 Apr-Jun;26(2):203 full-text
Stool testing
Occult blood
diagnosis of inflammatory diarrhea more likely if positive fecal occult blood tests in addition to presence of fecal leukocytes or lactoferrin(6)
diagnostic performance of fecal occult blood testing for detecting inflammatory diarrhea in systematic review

o systematic review of 15 studies evaluating diagnostic accuracy of rapid stool studies in 7,161 patients with acute, community-acquired bacterial gastroenteritis ≤ 7 days
o diagnostic performance for detecting inflammatory diarrhea in developed counties
sensitivity 71% specificity 79%
o diagnostic performance for detecting inflammatory diarrhea in developing countries
sensitivity 44% specificity 72%
o Reference - Clin Infect Dis 2003 Aug 1;37(3):365 full-text
Fecal biomarkers
lactoferrin(6) o lactoferrin is marker for leukocytes released by deteriorating or damaged cells
which increases in response to bacterial infectionso lactoferrin testing is the preferred method (over testing for leukocytes) to
screen for leukocytes due to speed and simplicity of testingo immunoassay testing kits for lactoferrin reported to be more precise and less
variable compared with testing for fecal leukocyteso reported diagnostic efficacy of lactoferrin testing for detection of bacterial
infections sensitivity > 90% specificity > 70%
screening for leukocytes not commonly performed due to wide variability in sensitivity and specificity(6)
no rapid stool studies (leukocytes, lactoferrin, or occult blood) appear to be useful in developing countries, but microscopy for fecal leukocytes might predict patients with bacterial gastroenteritis in developed countries (level 2 [mid-level] evidence )
o based on systematic review limited by heterogeneityo systematic review of 15 studies evaluating diagnostic accuracy of rapid stool
studies in 7,161 patients with acute, community-acquired bacterial gastroenteritis ≤ 7 days
o in developed countries microscopy for fecal leukocytes in analysis of 6 studies, results limited
by significant heterogeneity sensitivity 0.73 (95% CI 0.33-0.94) specificity 0.84 (95% CI 0.5-0.96) positive likelihood ratio 4.56
fecal occult blood test in analysis of 3 studies sensitivity 0.71 (95% CI 0.36-0.91) specificity 0.79 (95% CI 0.4-0.96)
o in resource-poor countries lactoferrin test in analysis of 3 studies
sensitivity 0.95 (95% CI 0.48-1) specificity 0.29 (95% CI 0.17-0.46)

microscopy for fecal leukocytes in analysis of 8 studies sensitivity 0.5 (95% CI 0.33-0.67) specificity 0.83 (95% CI 0.74-0.89)
fecal occult blood test in analysis of 6 studies sensitivity 0.44 (95% CI 0.32-0.57) specificity 0.72 (95% CI 0.6-0.82)
o Reference - Clin Infect Dis 2003 Aug 1;37(3):365 full-text
fecal calprotectin appears more sensitive and more specific than fecal lactoferrin or fecal occult blood test for positive bacterial culture in patients with acute diarrhea (level 2 [mid-level] evidence )
o based on diagnostic case-control studyo 200 patients with acute diarrhea and positive bacterial stool cultures and
cytotoxins for C. difficile and were matched to 200 controls with acute diarrhea and negative cultures
o stool samples tested for calprotectin, lactoferrin, and guaiac-based fecal occult blood test
For Prediction of Positive Bacterial Culture: Sensitivity Specificity
Fecal calprotectin 83% 87%Fecal lactoferrin 78% 54%Fecal occult blood test 38% 85%
o Reference - Am J Med 2008 Dec;121(12):1099
Stool cultures
reserve stool culture for patients with (AFP Grade C)(6) o grossly bloody stoolo severe dehydrationo evidence of inflammatory diseaseo symptoms durating > 3-7 dayso imunosuppressiono Traveler's diarrheao diarrhea begins > 3 days after hospital admission and nosocomial outbreak
not generally recommended in adults with mild, watery diarrhea, especially if no dehydration and if presenting within first few days of onset(2)
stool cultures appear to have 30% yield in patients with acute diarrhea and bloody stools in United States (level 2 [mid-level] evidence )
o based on prospective cohort study without stool cultures collected in all patients
o at 11 emergency departments in United States, 873 consecutive patients with 877 episodes of bloody diarrhea (confirmed by Hemoccult testing) with > 3 loose stools per 24 hours for > 7 days
o 24.5% patients were < 5 years old

o among 549 episodes with stool specimen submitted for culture and/or Shiga-toxin assay
enteric pathogens identified in 168 (30.6%) Shigella in 15.3% Campylobacter in 6.2% Salmonella in 5.8% Shiga toxin producing E. coli in 2.6% other pathogens (Vibrio, Yersinia, Plesiomonas) in 1.6%
o Reference - Clin Infect Dis 2001 Feb 15;32(4):573 full-text
Other stool studies
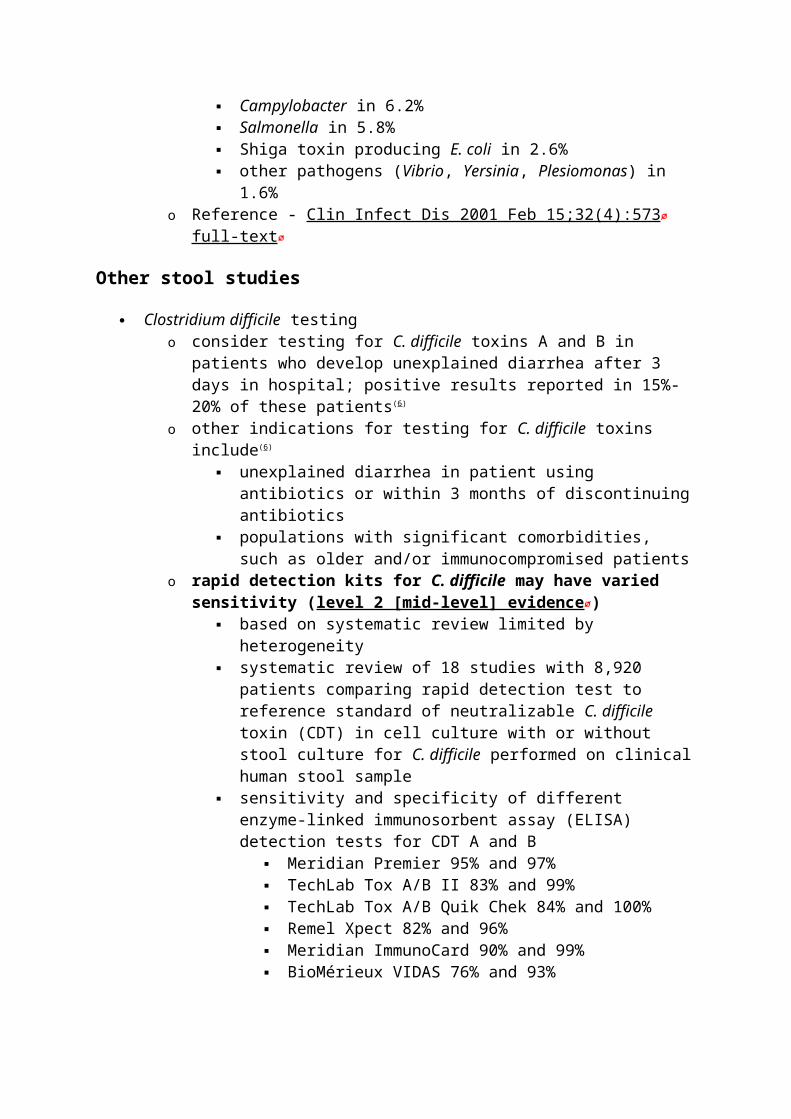
Clostridium difficile testingo consider testing for C. difficile toxins A and B in patients who develop
unexplained diarrhea after 3 days in hospital; positive results reported in 15%-20% of these patients(6)
o other indications for testing for C. difficile toxins include(6) unexplained diarrhea in patient using antibiotics or within 3 months of
discontinuing antibiotics populations with significant comorbidities, such as older and/or
immunocompromised patientso rapid detection kits for C. difficile may have varied sensitivity (level 2
[mid-level] evidence ) based on systematic review limited by heterogeneity systematic review of 18 studies with 8,920 patients comparing rapid
detection test to reference standard of neutralizable C. difficile toxin (CDT) in cell culture with or without stool culture for C. difficile performed on clinical human stool sample
sensitivity and specificity of different enzyme-linked immunosorbent assay (ELISA) detection tests for CDT A and B
Meridian Premier 95% and 97% TechLab Tox A/B II 83% and 99% TechLab Tox A/B Quik Chek 84% and 100% Remel Xpect 82% and 96% Meridian ImmunoCard 90% and 99% BioMérieux VIDAS 76% and 93%
Reference - Lancet Infect Dis 2008 Dec;8(12):777 routine testing for ova and parasites not recommended in developed countries except
for in high-risk patients, characterized by (AFP Grade C)(6) o diarrhea lasting > 7 days (especially if associated with infants in day care or
travel to mountain regions)o diarrhea in patients with AIDS or men who have sex with meno community waterborne outbreakso bloody diarrhea with few fecal leukocytes
Other testing to consider
indications for additional diagnostic tests include(4) o patients with severe illness

o more severe level of dehydrationo suspicion of diagnosis other than transient, watery acute diarrhea
additional testing may includeo blood tests, including
serum electrolytes(4) complete blood cell count(4) blood cultures(4)
o urinalysis(4) o abdominal computed tomography (CT)(4, 7)
may help detect mucosal thickening or other signs of ischemic, hemorrhagic, or inflammatory colitis
considered preferred diagnostic test when both intestinal and intra-abdominal diseases are included in differential diagnosis
considered particularly effective for detecting mucosal thickening and pericolonic stranding which may indicate fulminant Clostridium difficile-associated diarrhea
o sigmoidoscopy/endoscopy/colonoscopy routine flexible sigmoidoscopy or colonoscopy not recommended for
patients with acute diarrhea(7) flexible sigmoidoscopy may be useful for select case of acute diarrhea
with clinical colitis when diagnosis is unclear, including(2, 6, 7) suspected Clostridium difficile-associated diarrhea with toxin-
negative stool dysenteric diarrhea with negative results of toxin and
microbiologic tests, and negative for enterohemorrhagic on culture
no improvement despite empiric antibiotics for 3-5 days lower endoscopy may be especially useful for diagnoses of(6)
suspected tuberculosis or diffuse colitis (as in C. difficile colitis)
identifying non-infectious causes of acute diarrhea, such as inflammatory bowel disease ischemic colitis enteropathy related to nonsteroidal anti-inflammatory
drug use cancer
select bowel preparations prior to endoscopy to minimize mucosal change, and consider omitting bowel preparation in patients with severe diarrhea(7)
o esophagogastroduodenoscopy(7) may be useful in patients with persistent diarrhea and unclear results
on stool and serologic studies may help diagnose
giardiasis early-onset celiac disease histopathological changes in absorptive lining of small bowel bacterial overgrowth in small bowel
o proctoscopy exam may help diagnose proctitis in patients who have unprotected anal intercourse(7)

Treatment
Treatment overview
rehydration therapy , ideally oral rehydration therapy, recommended as first step for treating acute diarrhea (AFP Grade C)
antidiarrheal medicationso antimotility or antiperistaltic agents (including loperamide) may reduce stool
volume and frequency but are contraindicated in patients with bloody diarrhea immunocompromised patients patients at risk for septicemia elderly patients with chronic lung disease
o combination of loperamide-simethicone recommended over monotherapy for faster and more complete relief of acute nonspecific diarrhea and gas-related discomfort (AFP Grade B)
antimicrobial medications o antibiotics, typically a quinolone, reduce the duration and severity of traveler's
diarrhea (AFP Grade A)o routine antimicrobial use not recommended but may be indicated for patients
with severe cholera, shigellosis, typhoid, and paratyphoid fever severe dysenteric presentation of Campylobacter enterocolitis or
Nontyphoidal salmonellosis in immunocompromised patients severe invasive amebiasis severe symptomatic giardiasis
probiotics may reduce duration of acute diarrhea in adults (level 2 [mid-level] evidence )
Rehydration therapy
rehydration therapy, ideally oral rehydration therapy, recommended as first step for treating acute diarrhea (AFP Grade C)(2, 6)
o give 1.5-2 times volume of stool loss in 24 hours in addition to normal dietary intake
o encourage slow, steady intake of oral rehydration rather than drinking large amounts all at once
o considerations in elderly patients lower-sodium ORS may be suitable due to increased risk of sodium
abnormalities regularly assess serum electrolytes
IV rehydrationo consider IV rehydration for severe dehydration or hypovolemic shock if oral
route not possible, including(2, 6) mild dehydration accompanied by vomiting that precludes adequate
intake of ORS risk of aspiration (for example, patients with decreased consciousness)
o Ringer’s lactate solution recommended for adults with dehydration (with any form of diarrhea)(2)

o beware of volume overload in patients with cardiac problems, and avoid rapid correction of hyponatremia(5)
fluid replacement should cover maintenance needs and ongoing losses, plus replace 30%-50% deficit in first 24 hours(5)
o estimated 24-hour fluid maintenance needs total 1,500 mL plus 20 mL/kg for each kg > 20 kg in adults > 65 years old, use 30 mL/kg to estimate maintenance needs in febrile patients, add additional 10% of calculated water need for
each degree Celsius above normal estimated 24-hour maintenance needs sodium 3 mEq/100 mL water
and potassium 2 mEq/100 mL watero estimated fluid deficit in hypernatremic dehydration = {(serum sodium [in
mEq/L] - 140)/140} x (weight [in kg]) x (0.6 in men, 0.5 in adult women and elderly men, 0.45 in elderly women)
o ongoing losses from diarrhea determined by weighing or measuring stool if possible (particularly for very ill patients)(2)
rehydration therapy should maintain urine output ≥ 0.5 mL/kg/hour(5) among adults receiving oral rehydration salts for cholera, rice-based oral
rehydration salts associated with shorter duration of diarrhea than glucose-based oral rehydration salts (level 2 [mid-level] evidence )
o based on Cochrane reviewo systematic review of 34 randomized trials comparing polymer-based oral
rehydration salts (ORS) vs. glucose-based ORS in 4,214 patients with acute watery diarrhea (27 trials in children, 5 in adults, 2 in both children and adults)
o most trials compared polymer-based ORS vs. glucose-based ORS with osmolarity ≥ 310 mOsm/L
o polymers included rice, wheat, maltodextrin, maize, sorghum, or corn o trials in adults were limited to adults positive for Vibrio cholerae o in adults
rice-based ORS associated with greater reduction in duration of diarrhea (mean difference -7.11 hours, 95% CI -2.32 to -11.91 hours) in analysis of 4 trials with 228 patients
3 of these trials had unclear allocation concealment, the other trial did not have blinding
o Reference - Cochrane Database Syst Rev 2009 Apr 15;(2):CD006519 see Dehydration and hypovolemia in adults for additional information
Antidiarrheal medications
Indications and contraindications
antimotility or antiperistaltic agents (including loperamide ) may reduce stool volume and frequency but are contraindicated in(2)
o patients with bloody diarrheao immunocompromised patientso patients at risk for septicemiao elderly patients with chronic lung disease
long-term use of antimotility drugs may lead to physiologic dependence(2)

Loperamide
loperamide (Imodium, generic)o FDA-approved for control and symptomatic relief of acute nonspecific
diarrheao adult dose initially 4 mg, then 2 mg after each unformed stool up to maximum
16 mg/dayo do not use in patients with high fever or bloody diarrheao adverse effects include abdominal distention, abdominal discomfort,
constipation, drowsiness, fatigueo Pregnancy Category Bo see also Loperamide
loperamide appears more effective than bismuth subsalicylate for reducing symptoms of acute diarrhea (level 2 [mid-level] evidence )
o based on 2 randomized trials without blinding or intention-to-treat analysiso 219 adult students with acute nondysenteric traveler's diarrhea visiting 7
countries in Latin America randomized to loperamide (Imodium) vs. bismuth subsalicylate (Pepto-Bismol)
loperamide dose 4 mg, then 2 mg after each unformed stool (maximum 16 mg/day) for 2 days
bismuth subsalicylate dose 30 mL every 30 minutes for 3.5 hours on each of 2 days
if perception of symptom worsening after 12 hours students could stop study drug and start trimethoprim-sulfamethoxazole for 3-5 days
students taking < 75% of prescribed course of study drug and students missing or taking additional loperamide doses excluded from analysis
219 students completed the trial, number randomized and number excluded not reported
comparing loperamide vs. bismuth subsalicylate median number of unformed stools
between 0 and 4 hours 0.9 vs. 1.3 (p < 0.001) between 4 and 24 hours 1.5 vs. 2.4 (p < 0.002) between 24 and 48 hours 0.8 vs. 1 (p < 0.05)
constipation in 7.2% vs. 0.9% (p < 0.05, NNH 16) Reference - JAMA 1986 Feb 14;255(6):757
o 203 adult students in Mexico with acute diarrhea for up to 72 hours randomized to loperamide (Imodium A-D) liquid up to 8 mg/day vs. bismuth subsalicylate (Pepto-Bismol) liquid up to 4.9 g/day for 2 days
180 patients included in per-protocol analysis comparing loperamide vs. bismuth subsalicylate
mean number of unformed stools between 0 and 12 hours 0.9 vs. 2.3 (p = 0.0001)
mean number of unformed stools between 12 and 24 hours 0.4 vs. 0.8 (p = 0.01)
mean time to last unformed stool 9.9 hours vs. 17.3 hours (p < 0.001)
loperamide associated with improved overall subjective relief at 24 hours (p = 0.01)
no significant differences in mean number of unformed stools after 24 hours
Reference - Am J Med 1990 Jun 20;88(6A):15S
Loperamide-simethicone
chewable tablet containing loperamide 2 mg plus simethicone 125 mg available as Imodium Advanced Chewable Tablets
combination of loperamide-simethicone recommended over monotherapy for faster and more complete relief of acute nonspecific diarrhea and gas-related discomfort (AFP Grade B) (Am Fam Physician 2014 Feb 1;89(3):180 )
loperamide-simethicone combination chewable tablet may provide faster relief of acute nonspecific diarrhea and associated gas-related abdominal discomfort than loperamide alone (level 2 [mid-level] evidence )
o based on 2 randomized trials in Mexico with mixed results for magnitude of effect
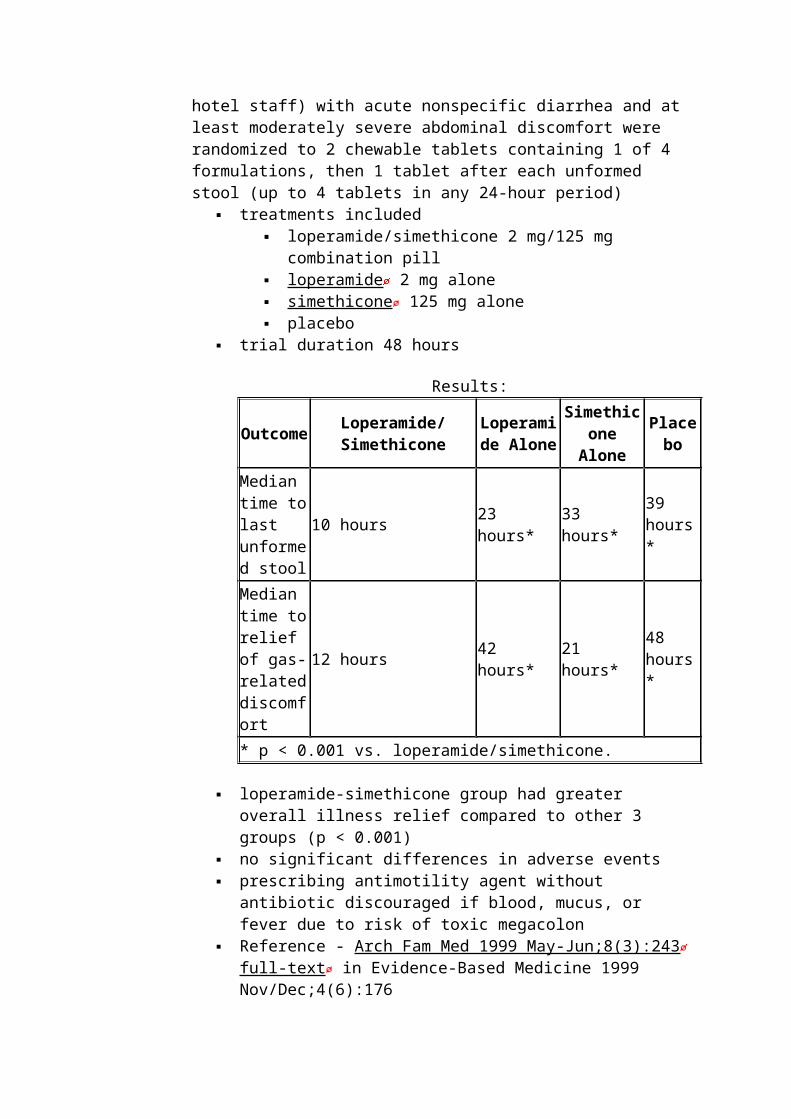
o 493 outpatients aged 18-63 years in Acapulco, Mexico (in ambulatory primary care practice or referred by hotel staff) with acute nonspecific diarrhea and at least moderately severe abdominal discomfort were randomized to 2 chewable tablets containing 1 of 4 formulations, then 1 tablet after each unformed stool (up to 4 tablets in any 24-hour period)
treatments included loperamide/simethicone 2 mg/125 mg combination pill loperamide 2 mg alone simethicone 125 mg alone placebo
trial duration 48 hours
Results:
Outcome Loperamide/Simethicone
Loperamide Alone
Simethicone Alone Placebo
Median time to last unformed stool
10 hours 23 hours* 33 hours* 39 hours*
Median time to relief of gas-related discomfort
12 hours 42 hours* 21 hours* 48 hours*
* p < 0.001 vs. loperamide/simethicone.
loperamide-simethicone group had greater overall illness relief compared to other 3 groups (p < 0.001)
no significant differences in adverse events prescribing antimotility agent without antibiotic discouraged if blood,
mucus, or fever due to risk of toxic megacolon

Reference - Arch Fam Med 1999 May-Jun;8(3):243 full-text in Evidence-Based Medicine 1999 Nov/Dec;4(6):176
DynaMed commentary -- trial funded by drug manufacturero 485 patients aged 18-78 years in Mexico (including local residents and
international travelers) with acute nonspecific diarrhea and gas-related abdominal discomfort were randomized to 2 chewable tablets containing 1 of 4 formulations, then 1 tablet after each unformed stool (up to 4 tablets in any 24-hour period)
treatments included loperamide/simethicone 2 mg/125 mg combination pill loperamide 2 mg alone simethicone 125 mg alone placebo
using strict definition of time to last unformed stool, any unformed stool after 24-hour period of formed stools, or no stools was considered continuance of original episode
using alternate definition of time to last unformed stool, any unformed stool after 24-hour period of formed stools, or no stools was considered a new episode
trial duration 48 hours
Results:
Outcome Loperamide/Simethicone
Loperamide Alone
Simethicone Alone Placebo
Median time to last unformed stool (strict definition)
8.7 hours 12.5 hours** 27 hours* 30.5
hours*
Median time to last unformed stool (alternate definition)
7.6 hours 11.5 hours* 26 hours* 29.4 hours*
Median time to complete relief of gas-related abdominal discomfort
12 hours 24 hours* 23.2 hours* 23.5 hours*
* p ≤ 0.023 vs. loperamide/simethicone.
** p = 0.071 vs. loperamide/simethicone.

no serious adverse events were reported Reference - Curr Med Res Opin 2007 May;23(5):1033 DynaMed commentary -- trial funded by drug manufacturer
Racecadotril
racecadotril is an enkephalinase inhibitor with antisecretory actions(6) o also called acetorphano available in parts of Europe, South America, and Asia but not Available in
United Stateso brand names include Hidrasec, Tiorfan, and Tiorfix
racecadotril may reduce acute diarrhea in adults by about 1 day or about 1 unformed stool per day (level 2 [mid-level] evidence )
o based on 2 randomized trials with allocation concealment not statedo 199 adults with acute diarrhea of presumed infectious origin (≤ 5 days)
randomized to racecadotril 100 mg vs. placebo tablets to be taken as 2 capsules initially then 1 capsule after each unformed bowel movement until recovery or maximum 10 days
5 patients did not take treatment or did not follow-up, 194 patients analyzed
comparing racecadotril vs. placebo recovery by day 4 in 75% vs. 37% (p < 0.001, NNT 3) mean total number of capsules taken 11.6 vs. 15.5 unformed stools at 30 days in 7.4% vs. 23.5% (p < 0.002, NNT
7); these patients not included in analysis of mean duration of diarrhea
mean duration of diarrhea 3.4 days vs. 4.4 days (p = 0.001) no significant differences in side effects
Reference - Gut 1992 Jun;33(6):753 PDF o 71 adults with acute diarrhea of presumed infectious origin (≥ 3 liquid or soft
stools/day for ≤ 5 days) randomized to racecadotril 100 mg vs. placebo orally 30 minutes before meals 3 times daily until no liquid or soft stools for 12 hours or for up to 6 days
1 patient lost to follow-up, 70 patients analyzed comparing racecadotril vs. placebo
mean stool weight on first day of treatment (primary efficacy outcome) 355 g vs. 499 g (p = 0.025)
mean number of diarrheal stools on first day of treatment 4.3 vs. 5.4 (p = 0.027)
at least 1 formed stool on day 2 in 15.6% vs. 5.3% (not significant)
duration of diarrhea not reported Reference - Aliment Pharmacol Ther 1999 Dec;13 Suppl 6:15 PDF
racecadotril appears as effective as loperamide for acute diarrhea in adults; racecadotril associated with lower rate of reactive constipation and abdominal distention (level 2 [mid-level] evidence )
o based on 4 randomized trials with allocation concealment not statedo 945 adults with acute watery diarrhea of presumed infectious origin (lasting 24
hours to 5 days) randomized to racecadotril 100 mg orally 3 times daily vs.

loperamide 2 mg orally 3 times daily until diarrhea resolved or maximum 7 days
countries included Brazil, Cameroon, Costa Rica, Guatemala, Indonesia, Ivory Coast, Kenya, Nigeria, Mexico, Morocco, Pakistan, Philippines, Tunisia, and Vietnam
trial described as single-blind, not clear if patient was blinded, allocation concealment not stated
comparing racecadotril vs. loperamide median duration of diarrhea (from time of first dose) 55 hours
vs. 55 hours 95% CI for difference in recovery rates at 72 hours -5% to +5% overall clinical response rate 92% vs. 93% (not significant) median duration of abdominal pain 11 hours vs. 10 hours (not
significant) median duration of abdominal distension 5.4 hours vs. 24.4
hours (p = 0.0001) adverse events 14.2% vs. 23.9% (p = 0.001, NNH 10 for
loperamide) abdominal distention in 1.7% vs. 6.1% (p = 0.03, NNH 22 for
loperamide) constipation (36 hours without passing stool) in 16% vs. 25%
(p = 0.001, NNH 11 for loperamide) Reference - Scand J Gastroenterol 2002 Jun;37(6):656
o 157 adults with acute diarrhea (≥ 3 soft or liquid stools for 1-5 days) randomized to racecadotril (100 mg initially then 100 mg before each meal) vs. loperamide (4 mg initially then 2 mg after each diarrheal stool) under double-blind conditions until recovery or maximum 7 days
10 patients (5 in each group) did not complete data correctly, 147 patients analyzed
comparing racecadotril vs. loperamide mean number of stools passed until recovery 3.5 vs. 2.9 (not
significant) mean duration of diarrhea 14.9 hours vs. 13.7 hours (not
significant) adverse events in 7.4% vs. 12% (not significant) rebound constipation (no stool for ≥ 2 days) in 9.8% vs. 18.7%
(NNH 11 for loperamide) Reference - Aliment Pharmacol Ther 1999 Dec;13 Suppl 6:21 PDF
o 69 adults with acute diarrhea of presumed infectious origin for ≤ 5 days randomized to racecadotril 100 mg vs. loperamide 1.33 mg capsules given as 2 capsules initially, 2 capsules in next 12 hours, then 1 capsule 3 times daily until absence of unformed stool or maximum 7 days
comparing racecadotril vs. loperamide mean duration of diarrhea 2.2 days vs. 2.3 days (not significant) recovery rate at 2 days 59.3% vs. 50% (not significant) mean duration of abdominal distension 1.1 days vs. 1.8 days (p
< 0.05) constipation after diarrhea resolution in 8.1% vs. 31.3% (p <
0.02, NNH 4 for loperamide) Reference - Scand J Gastroenterol 1993 Apr;28(4):352

o 62 adults with acute diarrhea of presumed infectious origin for 1-5 days randomized to racecadotril 100 mg orally 3 times daily vs. loperamide 2 mg orally twice daily until recovery or maximum 7 days
trial described as single-blind 48 patients (77%) completed the trial comparing racecadotril vs. loperamide in intention-to-treat analysis
mean duration of diarrhea 19.5 hours vs. 13 hours (not significant)
mean duration of abdominal pain 16 hours vs. 14 hours (not significant)
clinical success rate 87.1% vs. 87.1% adverse events in 25% vs. 22% (not significant)
Reference - World J Gastroenterol 2005 Mar 14;11(10):1540 full-text
racecadotril is more effective than loperamide for elderly nursing home patients with acute diarrhea (level 1 [likely reliable] evidence )
o based on randomized trialo 61 geriatric nursing home patients in Italy with acute diarrhea (≥ 3 liquid
stools in 24 hours) without severe dehydration or bacterial infection (blood or pus in stool) were randomized to racecadotril 100 mg orally every 8 hours vs. loperamide 2 mg then 1 tablet after each unformed stool up to 4 tablets in any 24-hour period
o treatment started after third diarrhea episode and stopped after 2 consecutive normal stools or no stool for 12 hours, treatment changed to other drug after 4 days without recovery
o comparing racecadotril vs. loperamide mean number of acute diarrhea episodes after enrollment 3.93 vs. 7.29 mean duration of abdominal pain 14 hours vs. 28 hours mean total stool output before recovery 120 g/kg vs. 150 g/kg (p <
0.01) treatment considered ineffective at 4 days in 0% vs. 50% (NNT 2 for
racecadotril) adverse effects in 12% vs. 60% (NNH 2 for loperamide), mainly
constipation no significant differences in oral or IV fluids given for rehydration
o Reference - Eur J Clin Pharmacol 2010 Feb;66(2):137 , commentary can be found in Eur J Clin Pharmacol 2010 Aug;66(8):839; author reply 841
Antimicrobial medications
Indications for antimicrobial therapy
antibiotics, typically a quinolone, reduce the duration and severity of traveler's diarrhea (AFP Grade A)(6)
universal routine antimicrobial use not recommended(1, 3, 4) o most adults with mild, nondehydrating cases of watery diarrhea generally do
not need antibiotics(2) o antibiotics ineffective against viruses (considered predominant cause of acute
diarrhea in especially in winter)(1, 3, 4)

o inappropriate use may lead to antimicrobial resistance, suprainfection, or induction of disease-producing phage by antibiotics (such as Shiga-toxin phage induced by quinolone antibiotics)(3)
o treating Shiga toxin-producing Escherichia coli (STEC) O157 with antimicrobials may increase risk of hemolytic-uremic syndrome (HUS) development(4)
routine antimicrobial use recommended in certain cases, including(3) o severe cholera , shigellosis , typhoid, and paratyphoid fevero severe dysenteric presentation of enterocolitis or Nontyphoidal salmonellosis
in immunocompromised patientso severe invasive amebiasis o severe symptomatic giardiasis
consider selective use of antimicrobials in certain cases, includingo patients ≥ 65 years old(2, 3) o immunocompromised patients(2, 3) o sepsis or septicemia, or at risk for septicemia(2) o parasitic infections(3) o infections with known pathogens such as(3)
shigellosis (IDSA Grade A-I)(4) Nontyphoidal salmonellosis enterocolitis (IDSA Grade B-II)(4) infection giardiasis amebiasis cholera (especially with severe dehydration)
o suspected traveler's diarrhea (enterotoxigenic E. coli or other bacterial pathogens may be likely cause) (IDSA Grade A-I)(3, 4)
o serious nonintestinal infections (such as pneumonia)(1, 3) o diarrhea lasting > 10-14 days(4)
Recommended antimicrobial therapy by underlying illness
Bacillary dysentery (shigellosis)
World Health Organization (WHO) recommendations for the management of shigellosis
o pivmecillinam, ceftriaxone , or azithromycin may be used when local strains of Shigella are known to be resistant to ciprofloxacin
World Health Organization 2005 Recommendations for Antimicrobial Treatment of Bacillary Dysentery :
Antimicrobial Dose
Route Frequency Duration Children Adults
First LineCiprofloxacin 15 mg/kg 500 mg Oral Twice daily 3 days
Second Line
Pivmecillinam 20 mg/kg 100 mg Oral 4 times daily 5 days

World Health Organization 2005 Recommendations for Antimicrobial Treatment of Bacillary Dysentery :
Antimicrobial Dose
Route Frequency Duration Children Adults
Ceftriaxone 50-100 mg/kg
No recommended dose
Intramuscular Once daily 2-5 days
Azithromycin 6-20 mg/kg 1-1.5 g Oral Once daily 1-5 days
o Reference - WHO guidelines for the control of shigellosis, including epidemics due to Shigella dysenteriae type 1 (WHO 2005 PDF or in French )
see Bacillary dysentery for additional information
Salmonellosis
nontyphoidal salmonellosis o Infectious Disease Society of America (IDSA) 2001 recommendations for
antibiotic therapy of nontyphoidal Salmonella diarrhea(4) in immunocompetent patients
antibiotics not routinely recommended (IDSA Grade E-1) in patients with severe disease (age < 6 months or > 50 years,
prostheses, valvular heart disease, severe atherosclerosis, malignancy, or uremia) recommended regimens include
ciprofloxacin 500 mg orally twice daily (IDSA Grade B-III)
co-trimoxazole (trimethoprim/sulfamethoxazole) 1 double-strength (DS) tablet twice daily (IDSA Grade B-III)
ceftriaxone 2 g IV every 24 hours in immunocompromised patients, extend duration of antibiotic
treatment to 14 days, or longer if symptoms relapseo see Nontyphoidal salmonellosis for additional information
enteric fever, bacteremic salmonellosis (including typhoid fever)(7) o give fluoroquinolone or IV cephalosporin for 7 dayso in immunocompromised patients, extend duration of antibiotic treatment to ≥
14 days chronic carriage of typhoidal salmonella(7)
o initial treatment is either of ciprofloxacin 750 mg twice daily for 4-6 weeks norfloxacin 400 mg twice daily for 4-6 weeks
o if treatment failure, assess for cholithiasis (gallstones ) and consider cholecystecomy
Clostridium difficile-associated diarrhea

Infectious Diseases Society of America/Society for Healthcare Epidemiology of America (IDSA/SHEA) recommendations for antibiotics for Clostridium difficile infection
o for initial episode
SHEA/IDSA Recommendations on First-Line Therapy for C. difficile infection in adults:
Initial Episode
Clinical Characteristics
Recommended First-Line Therapy Duration
Mild or moderate
Leukocytosis with a white blood cell count ≤ 15,000 cells/mcL AND
Serum creatinine level < 1.5 times premorbid level
Metronidazole 500 mg orally 3 times daily 10-14 days
Severe
Leukocytosis with a white blood cell count ≥ 15,000 cells/mcL OR
Serum creatinine level ≥ 1.5 times premorbid level
Vancomycin 125 mg orally 4 times daily 10-14 days
Severe, complicated
Hypotension or shock
Ileus Megacolon
Vancomycin 500 mg orally or by nasogastric tube 4 times daily PLUS
Metronidazole 500 mg IV every 8 hours
Consider rectal instillation of vancomycin if complete ileus
Stop oral or rectal antimicrobial therapy if colonic perforation demonstrated or colectomy imminent
Reference - SHEA/IDSA clinical practice guideline on C. difficile infection in adults (Infect Control Hosp Epidemiol 2010 May;31(5):431), commentary can be found in Infect Control Hosp Epidemiol 2010 Nov;31(11):1205, Infect Control Hosp Epidemiol 2011 Dec;32(12):1231.
o for recurrence if first recurrence, treat same as for initial episode stratified by disease
severity (IDSA Grade A-II) if second or later recurrence - use vancomycin in tapered and/or pulsed
regimen (IDSA Grade B-III); tapered regimen may be vancomycin 125
mg 4 times daily for 10-14 days, then 125 mg twice daily for 1 week, then 125 mg once daily for 1 week, then 125 mg/day every 2-3 days for 2-8 weeks
o Reference - Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA) (Infect Control Hosp Epidemiol 2010 May;31(5):431 )
o see infection for additional information
Traveler's diarrhea and enterotoxigenic E. coli diarrhea
in patients without fever or dysentery, either of(7) o rifaximin 200 mg 3 times/day for 3 dayso ciprofloxacin 500 mg twice daily (or 750 mg daily) for 1-3 days
in patients with fever and/or dysentery, azithromycin 1,000 mg orally in single dose(7)
antibiotics associated with shorter duration of diarrhea but increased risk of side effects in patients with traveler's diarrhea (level 2 [mid-level] evidence )
o based on Cochrane review of trials with methodologic limitationso systematic review of 20 randomized trials evaluating antibiotics in 3,157
patients ≥ 5 years old with traveler's diarrheao most trials evaluated patients with moderate-to-severe diarrheao causative organism unknown at time of allocationo all trials had unclear method of randomization sequence generation or lack of
intention-to-treat analysiso comparing antibiotics to placebo, antibiotics associated with
reduced duration of diarrhea in 10 trials with 1,935 patients (p < 0.05 for each trial, heterogeneity in statistics reporting precluded meta-analysis)
increased rate of clinical resolution of symptoms at 72 hours in analysis of 6 trials with 697 patients
odds ratio (OR) 5.9 (95% CI 4.1-8.6) NNT 3-4 with cure in 50% of controls
reduced number of unformed stools in analysis of 2 trials with 223 patients (p < 0.01 for each 24-hour period from 0 to 72 hours)
increased number of side effects in analysis of 5 trials with 862 patients
OR 2.4 (95% CI 1.5-3.8) NNH 4-21 with side effects in 11% of controls
o Reference - Cochrane Database Syst Rev 2000 Jul-Sep;(4):CD002242 (review updated 2003 Sep 8)
o consistent results in systematic review of 15 randomized trials, including 13 trials included in Cochrane review above (West J Med 2000 Jun;172(6):409 full-text )
see Traveler's diarrhea for additional information
Treatments for other underlying organisms
intestinal campylobacteriosis, either ofo azithromycin 500 mg once daily for 3-5 days(6, 7)

o erythromycin 500 mg 4 times/day for 5 days(7) noncholeraic vibrio diarrhea, either of(7)
o ciprofloxacin 750 mg once daily for 3 dayso doxycycline 300 mg in single dose
Vibrio cholerae infection (cholera ) , doxycycline 300 mg in single dose(6, 7) giardiasis , any of(7)
o tinidazole 2 g orally in single doseo metronidazole 250 mg 3 times/day for 5-7 dayso nitazoxanide 500 mg twice daily for 3 days
antibiotic therapy not indicated foro gastroenteritis, including norovirus infection and rotavirus gastroenteritis (7) o Shiga toxin-producing E. Coli diarrhea(6, 7)
Probiotics
probiotics may reduce duration of acute diarrhea in adults (level 2 [mid-level] evidence )
o based on Cochrane review with limited evidence in adultso systematic review of 63 randomized and quasi-randomized trials evaluating
probiotics in 8,014 patients with acute diarrhea proven or suspected to be of infectious origin
o 5 trials recruited adults (no separate analysis conducted in adult-only trials)o probiotics reduced
proportion of patients with diarrhea lasting ≥ 4 days in analysis of 29 trials with 2,853 patients
risk ratio 0.41 (95% CI 0.32-0.53) NNT 4-5 assuming diarrhea for ≥ 4 days in 45% of controls results limited by significant heterogeneity only 4 trials in adults included in analysis (3 of 4 trials found
significant effect; results pooled with largely child population) duration of diarrhea in analysis of 25 trials with 4,555 children
mean difference -24.76 hours, 95% CI -33.61 to -15.91 hours no trials in adults included in analysis
o probiotics with more supporting evidence (in children) include Lactobacillus casei strain GG, Enterococcus LAB SF68, Saccharomyces boulardii, and Escherichia coli strain Nissle 1917
o Reference - Cochrane Database Syst Rev 2010 Dec 8;(11):CD003048
Medications not recommended
World Health Organization (WHO) advises against the use of(1) o cardiac stimulantso blood or plasma (unless hypovolemia due to septic shock)o steroidso purgatives
Follow-up
encourage fluid intake after rehydration(2)

ensure adequate follow-up of hydration and nutritional status, especially in elderly patients(2)
Complications and Prognosis
Complications
dehydration and hypovolemia - prognosis generally good if successful rehydration(1, 2,
3) electrolyte disturbances (such as hypernatremia or hyponatremia ) hypovolemic shock reactive arthritis (following acute enteric infection by strains of salmonella, shigella,
and yersinia)(7) functional bowel disorders, including post-infectious irritable bowel syndrome (IBS)
(reported in 5%-10% of patients after infection by inflammatory bacterial pathogens and less commonly after infection by parasites and viruses)(7)
Guillain-Barre syndrome (reported in 1-2 per 10,000 patients with campylobacteriosis)(7)
Prognosis
general prognosiso acute, watery diarrhea typically lasts 5-7 days(1) o most cases resolve within 2 weeks(1)
mortality due to foodborne diarrheal illness reported in(6) o 2.5 million patients annually worldwideo 3,000 patients annually in United States
factors associated with poorer prognosis includeo bloody diarrhea(1, 2) o dehydration and hypovolemia (1) o hypovolemic shock(1) o repeated diarrheal attacks(1) o malnourishment(1) o immunodeficiency, including with HIV infection (1) o age > 65 years(2) o antibiotic-associated diarrhea(2) o hospital acquired or outbreak diarrhea(2) o signs of peritonitis (2)
Prevention general preventative measures include(6)
o good hygieneo hand washingo safe food preparationo access to clean water
prophylactic vaccines are available for(6) o rotavirus gastroenteritis

o typhoid fever o cholera
to contain disease outbreaks, report designated disease to public health authorities; in the United States, reportable diarrhea-causing illnesses include those caused by(6)
o Vibrio cholerae o Cryptosporidium o Giardia o Salmonella o Shigella o Shiga toxin-producing E. coli
Guidelines and Resources
Guidelines
International guidelines
WHO manual on treatment of diarrhea can be found at WHO 2005 PDF WHO Global Task Force on Cholera Control recommendation on first steps for
managing an outbreak of acute diarrhoea can be found at World Health Organization 2010 PDF
World Gastroenterology Organisation (WGO) practice guideline on acute diarrhea in adults and children can be found at WGO 2012 Feb PDF or at National Guideline Clearinghouse 2014 Mar 24:47569 or in J Clin Gastroenterol 2013 Jan;47(1):12
Bangkok World Congress of Gastroenterology guideline on management of acute diarrhea in adults can be found in J Gastroenterol Hepatol 2002 Feb;17 Suppl:S54
International Centre for Diarrheal Disease Research, Bangladesh/Swiss Tropical Institute (ICDDR,B/STI) cholera outbreak training and shigellosis program can be found at COTS PDF
United States guidelines
CDC recommendation on diagnosis of Shiga toxin-producing Escherichia coli infections by clinical laboratories can be found in MMWR Recomm Rep 2009 Oct 16;58(RR-12):1 full-text
CDC primer on diagnosis and management of foodborne illnesses can be found in MMWR Recomm Rep 2004 Apr 16;53(RR-4):1 full-text
American Society of Gastrointestinal Endoscopy (ASGE) guideline on role of endoscopy in management of patients with diarrhea can be found in Gastrointest Endosc 2010 May;71(6):887 PDF or at National Guideline Clearinghouse 2012 Nov 19:37860
Infectious Diseases Society of America (IDSA) practice guideline on management of infectious diarrhea can be found in Clin Infect Dis 2001 Feb 1;32(3):331 full-text , summary can be found in Am Fam Physician 2001 Sep 15;64(6):1065

American Gastroenterological Association (AGA) Institute position statement on use of gastrointestinal medications in pregnancy can be found in Gastroenterology 2006 Jul;131(1):278 , summary can be found in Am Fam Physician 2007 Mar 1;75(5):748
American Association of Clinical Endocrinologists medical guideline for clinical use of dietary supplements and nutraceuticals can be found in Endocr Pract 2003 Sep-Oct;9(5):417 PDF
Council to Improve Foodborne Outbreak Response (CIFOR) guideline on foodborne disease outbreak response can be found at CIFOR 2009 PDF
Asian guidelines
Japanese expert guideline on anaerobic infections (individual fields): antibiotic-associated diarrhea and enterocolitis can be found in J Infect Chemother 2011 Jul;17 Suppl 1:137
Review articles
review of acute diarrhea in adults can be found in Am Fam Physician 2008 Aug 15;78(4):503 full-text
review of acute infectious diarrhea can be found in N Engl J Med 2004 Jan 1;350(1):38 , commentary can be found in N Engl J Med 2004 Apr 8;350(15):1576
review of acute infectious diarrhea can be found in Am J Med 1999 Jun;106(6):670 review of acute bloody diarrhea can be found in Gastroenterology 2009
May;136(6):1887 PDF review of antibiotic-associated diarrhea can be found in Expert Opin Drug Saf 2006
May;5(3):361 review of interdisciplinary approach to antibiotic-associated diarrhea can be found in
Praxis (Bern 1994) 2003 Apr 16;92(16):751 review of diarrhea and hypovolemia in elderly can be found in Adv Stud Med 2005
Nov-Dec;5(10):528 PDF review of probiotics for prevention and treatment of diarrhea can be found in J Clin
Gastroenterol 2011 Nov;45 Suppl:S149 case presentation of acute diarrhea in adults can be found in BMJ 2009 Jun
15;338:b1877
Patient Information
Patient information
handout from National Digestive Diseases Information Clearinghouse PDF handout from British Society of Gastroenterology PDF handout from Patient UK PDF technical information from Patient Plus PDF handout from Mayo Clinic handout from Cleveland Clinic
ICD-9/ICD-10 Codes

ICD-9 codes
003.0 salmonella gastroenteritis 005.9 food poisoning; unspecified 008.8 intestinal infection due to other organism, not elsewhere classified (used for
viral gastroenteritis not otherwise specified) 009 ill-defined intestinal infections
o 009.0 infectious colitis, enteritis and gastroenteritiso 009.1 colitis, enteritis and gastroenteritis of presumed infectious origino 009.2 infectious diarrheao 009.3 diarrhea of presumed infectious origin
564.4 other postoperative functional disorders 564.5 functional diarrhea 787.91 diarrhea
ICD-10 codes
A02.0 salmonella enteritis A05.9 bacterial foodborne intoxication, unspecified A07.2 cryptosporidiosis A07.9 protozoal intestinal disease, unspecified A08 viral and other specified intestinal infections
o A08.0 rotaviral enteritiso A08.1 acute gastroenteropathy due to Norwalk agento A08.3 other viral enteritiso A08.4 viral intestinal infection, unspecified [viral gastroenteritis NOS]o A08.5 other specified intestinal infections
A09 diarrhoea and gastroenteritis of presumed infectious origin K52.0 gastroenteritis and colitis due to radiation K52.9 noninfective gastroenteritis and colitis, unspecified K59.1 functional diarrhoea
References
General references used
1. World Health Organization. The Treatment of Diarrhoea: a manual for physicians and other senior health workers. WHO 2005 PDF
2. Manatsathit S, Dupont HL, Farthing M, et al; Working Party of the Program Committee of the Bangkok World Congress of Gastroenterology 2002. Guideline for the management of acute diarrhea in adults. J Gastroenterol Hepatol. 2002 Feb;17 Suppl:S54-71
3. Farthing M, Salam MA, Lindberg G, Dite P, Khalif I, Salazar-Lindo E, Ramakrishna BS, Goh KL, Thomson A, Khan AG, Krabshuis J, LeMair A. World Gastroenterology Organization. Acute diarrhea in adults and children: a global perspective. J Clin Gastroenterol. 2013 Jan;47(1):12-20 or at WGO 2012 Feb PDF
4. Guerrant RL, Van Gilder T, Steiner TS, et al; Infectious Diseases Society of America (IDSA). Practice guidelines for the management of infectious diarrhea. Clin Infect Dis. 2001 Feb 1;32(3):331-51 full-text

5. Suhayda R, Walton JC. Preventing and managing dehydration. Medsurg Nurs. 2002 Dec;11(6):267-78
6. Barr W, Smith A. Acute diarrhea. Am Fam Physician. 2014 Feb 1;89(3):180-9 7. DuPont HL. Acute infectious diarrhea in immunocompetent adults. N Engl J Med.
2014 Apr 17;370(16):1532-40
Recommendation grading systems used
strength of recommendation ratings used in American Family Physician (AFP) clinical review articles
o Strength of recommendation A - based on consistent and good quality patient-oriented evidence
o Strength of recommendation B - based on inconsistent or limited quality patient-oriented evidence
o Strength of recommendation C - based on consensus, usual practice, expert opinion, disease-oriented evidence, or case series
o Reference - AFP guidelines for rating strength of recommendations in clinical review articles , also used in Journal of Family Practice
Infectious Diseases Society of America (IDSA) grades of recommendationo strength of recommendation grades
Grade A - good evidence to support recommendation for use Grade B - moderate evidence to support recommendation for use Grade C - poor evidence to support recommendation for or against use Grade D - moderate evidence to support recommendation against use Grade E - good evidence to support a recommendation against use
o quality of evidence ratings I - evidence from ≥ 1 properly randomized, controlled trial II - evidence from ≥ 1 well-designed clinical trial without
randomization, from cohort or case-controlled analytic studies (preferably from ≥ 1 center), from multiple time-series studies, or from dramatic results in uncontrolled experiments
III - evidence from opinions of respected authorities, based on clinical experience, descriptive studies, or reports of expert committees
o Reference - IDSA practice guidelines for management of infectious diarrhea (Clin Infect Dis 2001 Feb 1;32(3):331 full-text )
DynaMed editorial proces
DynaMed topics are created and maintained by the DynaMed Editorial Team . Over 500 journals and evidence-based sources (DynaMed Content Sources ) are monitored
directly or indirectly using a 7-Step evidence-based method for systematic literature surveillance . DynaMed topics are updated daily as newly discovered best available evidence is identified.
The participating members of the DynaMed Editorial Team have declared that they have no financial or other competing interests related to this topic.
The participating reviewers have declared that they have no financial or other competing interests related to this topic, unless otherwise indicated.

McMaster University is a partner that provides support in identifying Practice-Changing DynaMed Updates . Over 1,000 practicing physicians from 61 disciplines in 77 countries rate these articles to help you find the most useful new evidence affecting your practice.
F1000 is a partner that provides support in identifying Practice-Changing DynaMed Updates. Over 2,000 practicing clinicians from 20 disciplines in 60 countries rate these articles to help you find the most useful new evidence affecting your practice.
Special acknowledgements
Jeffrey L. Chamberlain, MD (Core Faculty and Clinical Instructor, Michigan State University Department of Family Medicine; Family Practice Doctor, Advantage Health; Urgent Care Provider, St. Mary's Health South West Urgent Care; Michigan, United States) provides peer review.
How to cite
For attribution in other publications see How to Cite Information from DynaMed .