16 th croi, montreal, 2009. hotel ac forum, barcelona – february 20 th 2009 16 th croi, montreal,...
TRANSCRIPT
16th CROI, Montreal, 2009.Hotel AC Forum, Barcelona – February 20th 2009
16th CROI, Montreal, 2009.Hotel AC Forum, Barcelona – February 20th 2009
José M. MiróInfectious Diseases Unit - ICMiD
Hospital Clinic - IDIBAPS University of Barcelona
Barcelona (Spain)
José M. MiróInfectious Diseases Unit - ICMiD
Hospital Clinic - IDIBAPS University of Barcelona
Barcelona (Spain)
Summary: Opportunistic Infections HCV/HBVCo-Infections &Tumors
Summary: Opportunistic Infections HCV/HBVCo-Infections &Tumors
E-mail address: [email protected] address: [email protected]
Tuberculosis Other opportunistic infections IRIS HBV & HCV co-infections Cirrhosis & liver transplantation Tumors
Tuberculosis Other opportunistic infections IRIS HBV & HCV co-infections Cirrhosis & liver transplantation Tumors
OIs, Hepatitis Coinfections & Tumors
OIs, Hepatitis Coinfections & Tumors
N= 44
N= 19
N= 11
N= 77
N= 5
N= 17
N= 44
N= 19
N= 11
N= 77
N= 5
N= 17
~173 abstracts in 20 min. !~173 abstracts in 20 min. !
http://www.retroconference.org/2009http://www.retroconference.org/2009
Tuberculosis Other opportunistic infections IRIS HBV & HCV co-infections Cirrhosis & liver transplantation Tumors
Tuberculosis Other opportunistic infections IRIS HBV & HCV co-infections Cirrhosis & liver transplantation Tumors
OIs, Hepatitis Coinfections & Tumors
OIs, Hepatitis Coinfections & Tumors
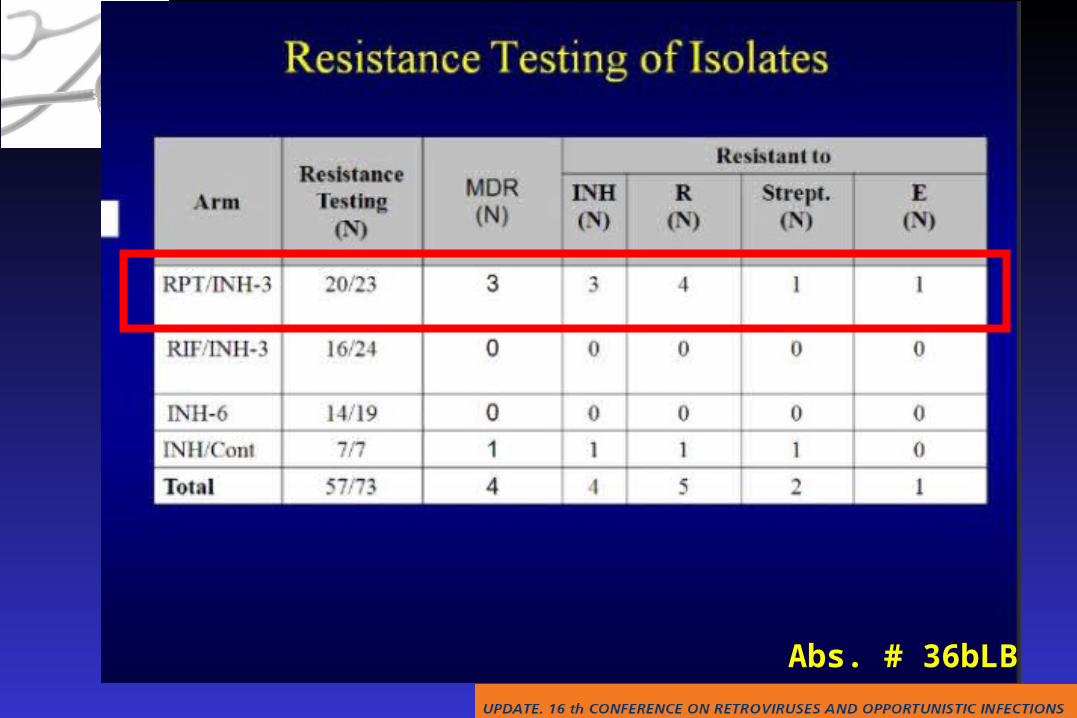
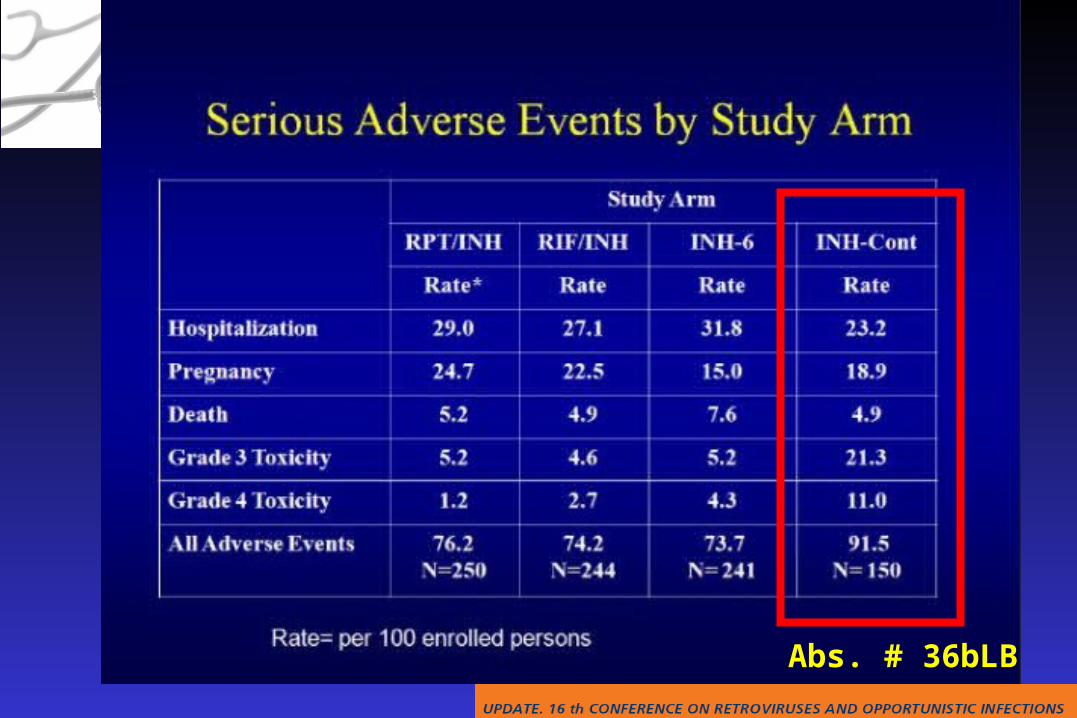
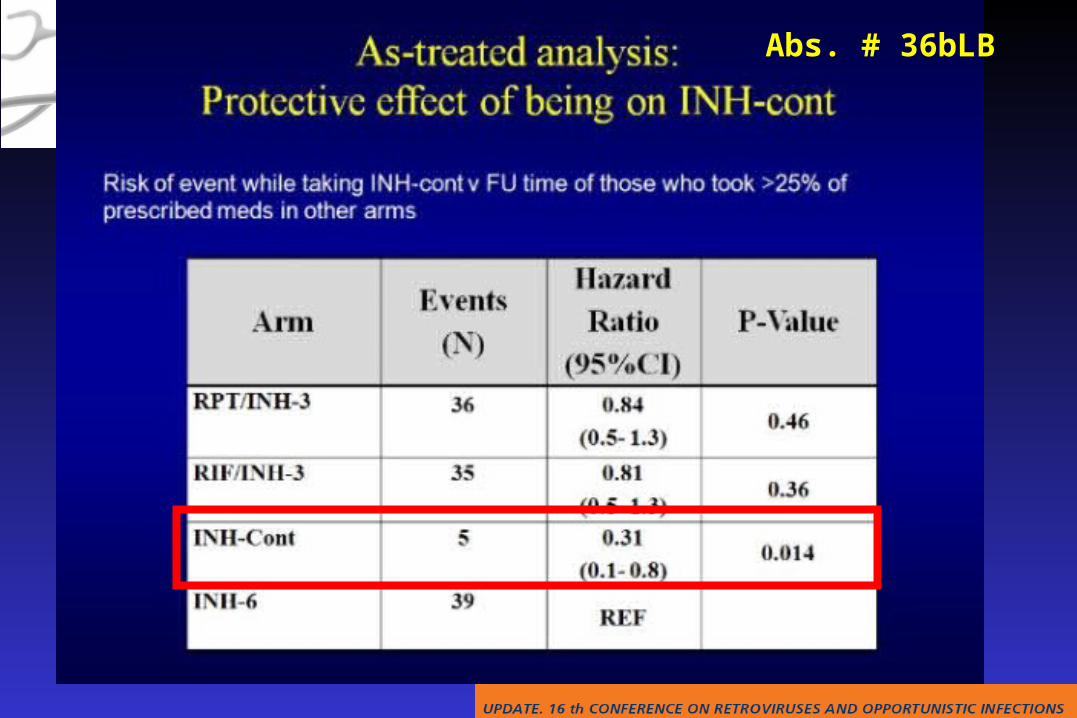
Abs. # 36bLB
Abs. # 36bLB
Abs. # 36bLB
Abs. # 36bLB
Abs. # 36bLB
Abs. # 36bLB
Abs. # 36bLB
Abs. # 36bLB
Abs. # 36bLB
Abs. # 35Abs. # 35
Abs. # 35Abs. # 35

Abs. # 35Abs. # 35
Abs. # 35Abs. # 35
Abs. # 35Abs. # 35
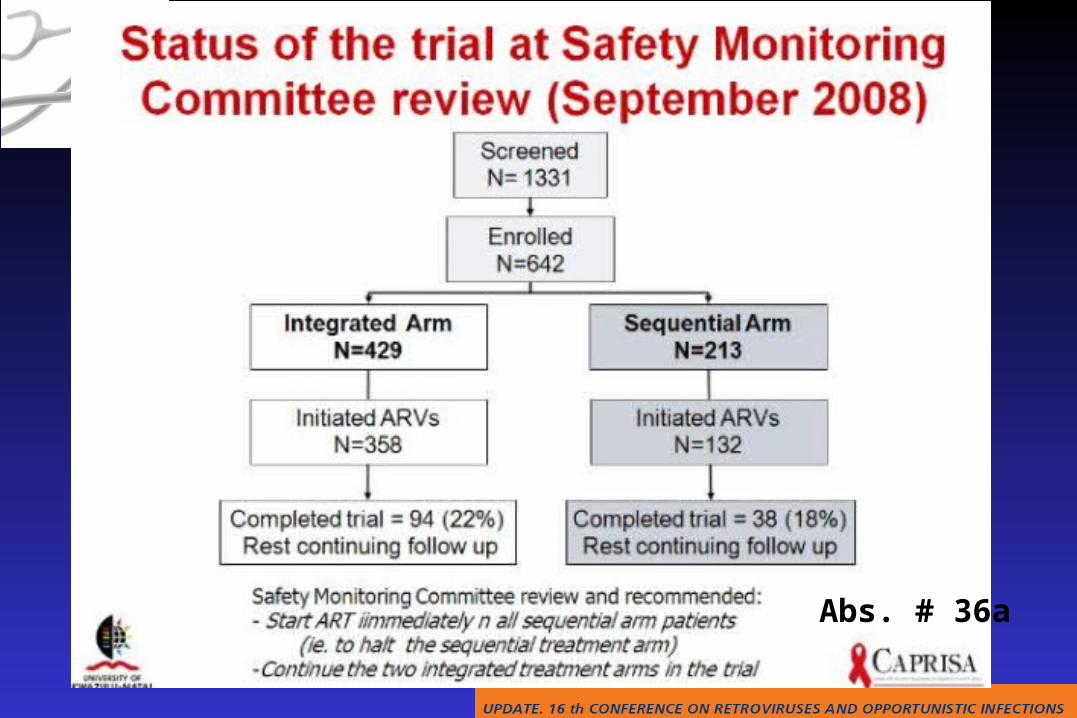
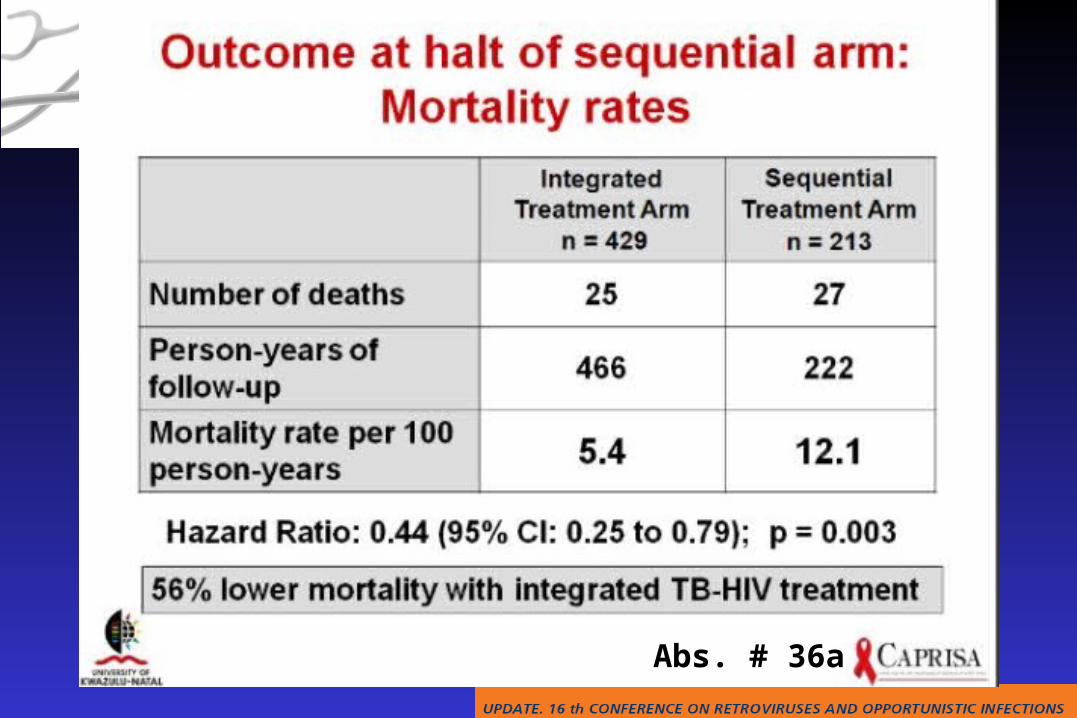
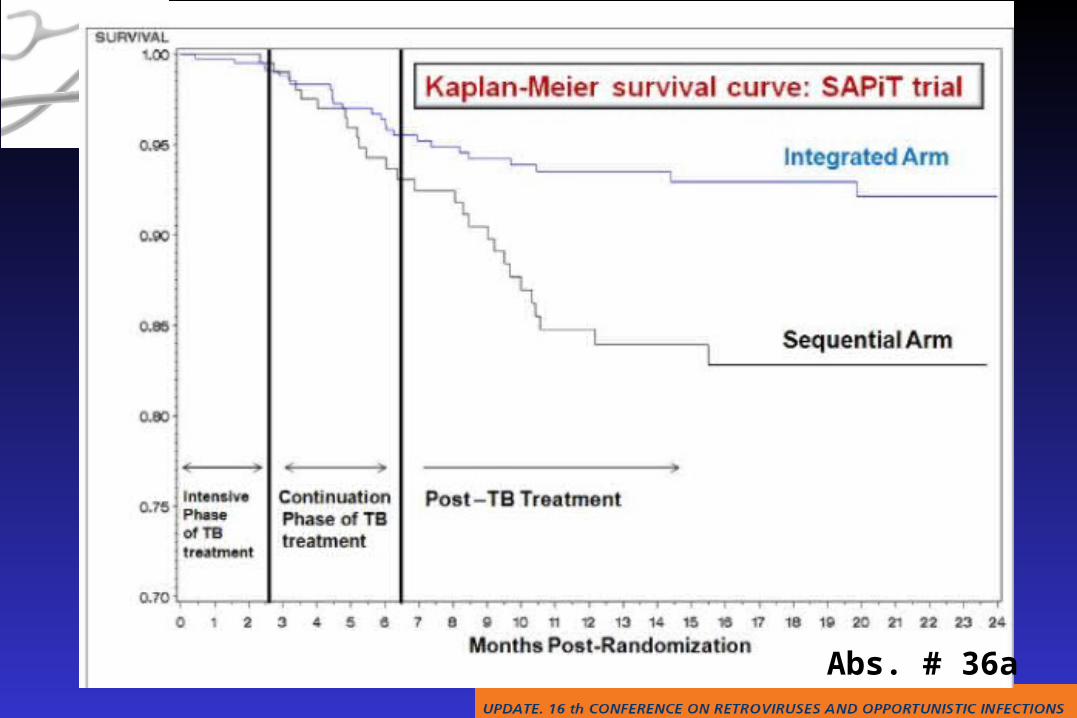
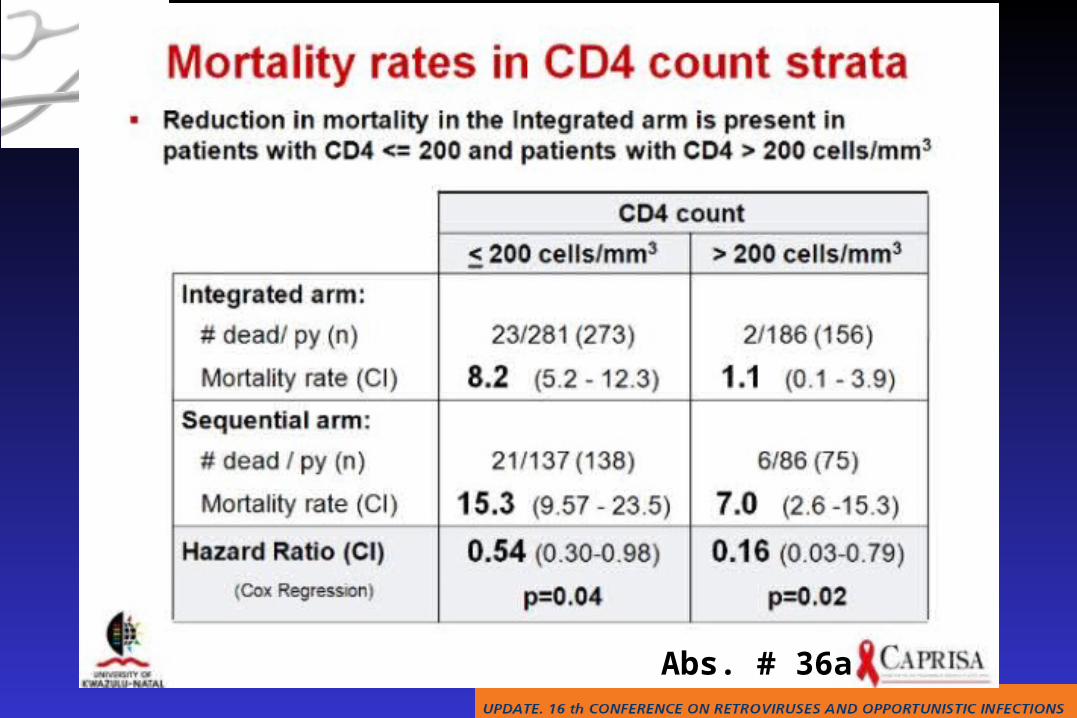
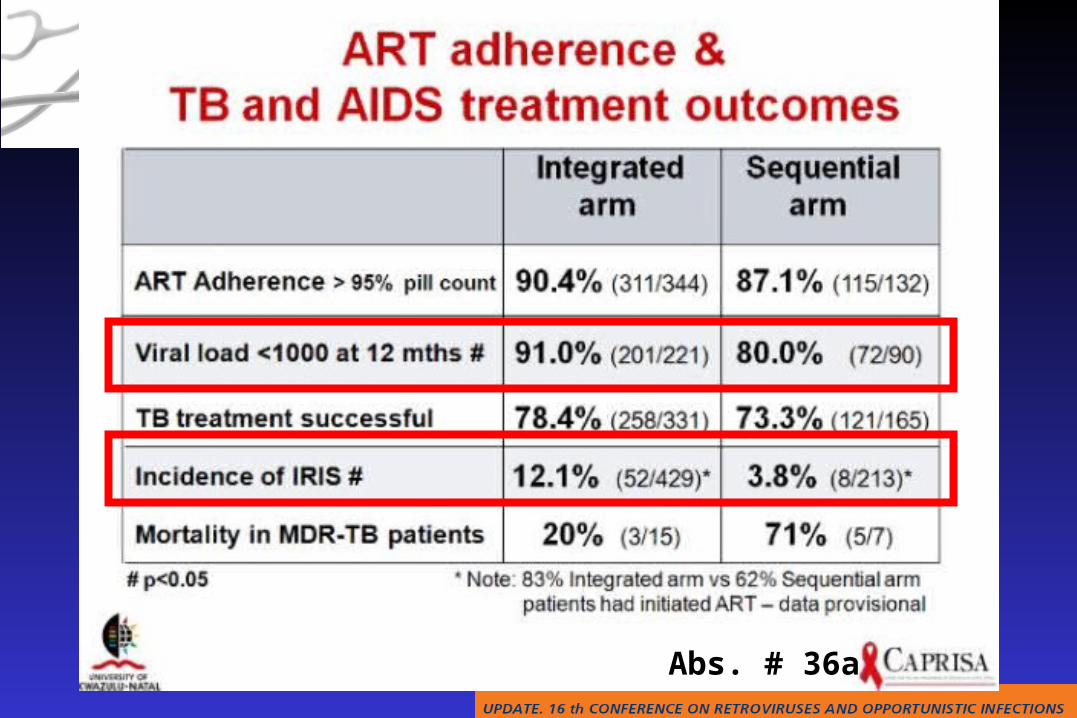
Abs. # 36a
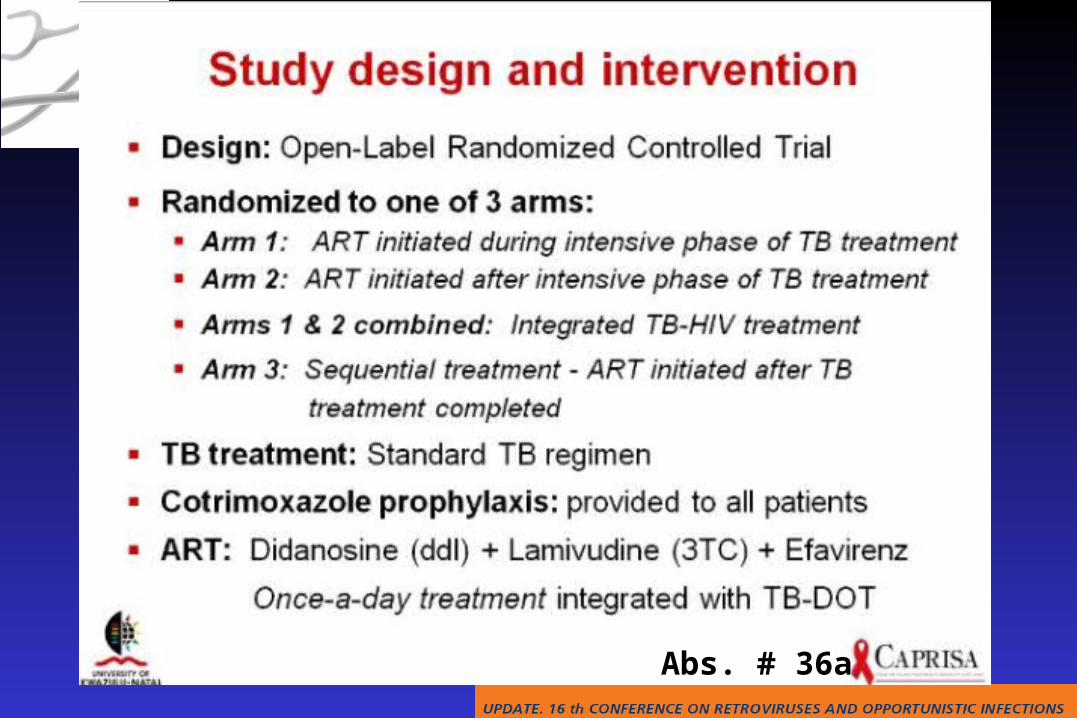
Abs. # 36a
Abs. # 36a
Abs. # 36a
Abs. # 36a
Abs. # 36a
Abs. # 36a
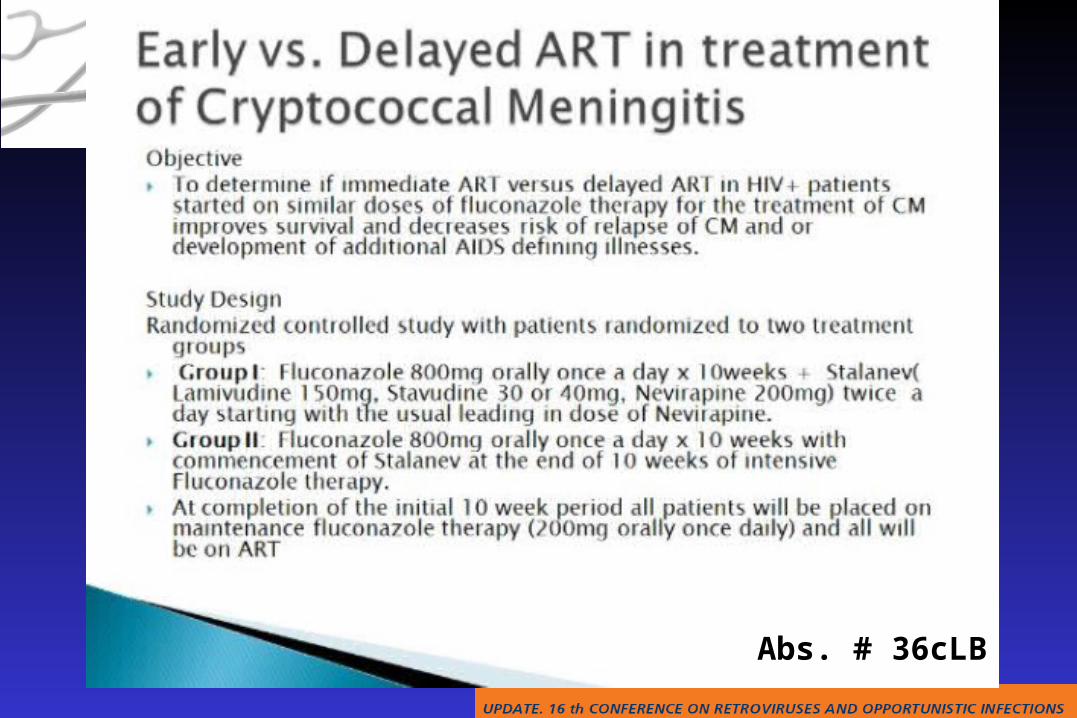
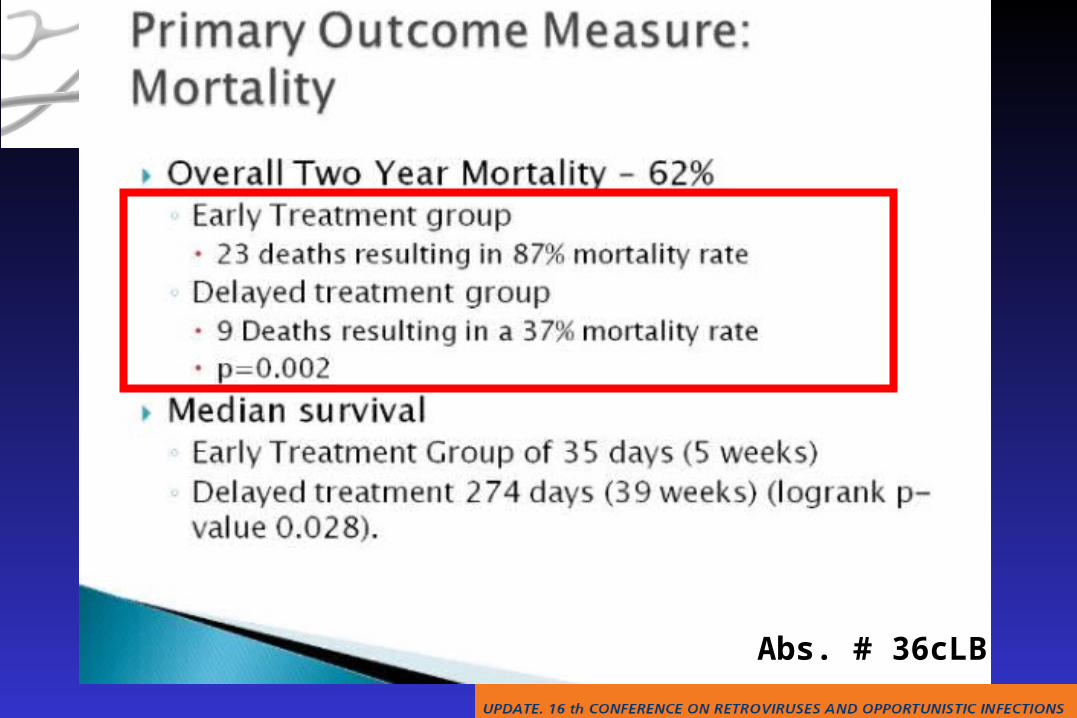
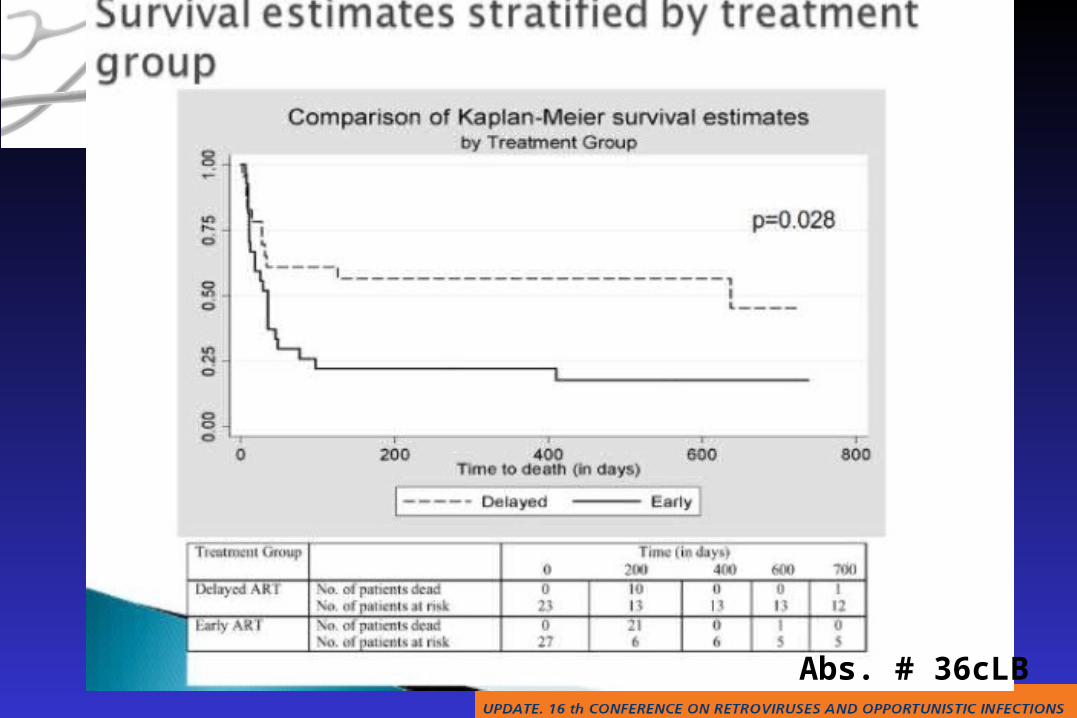
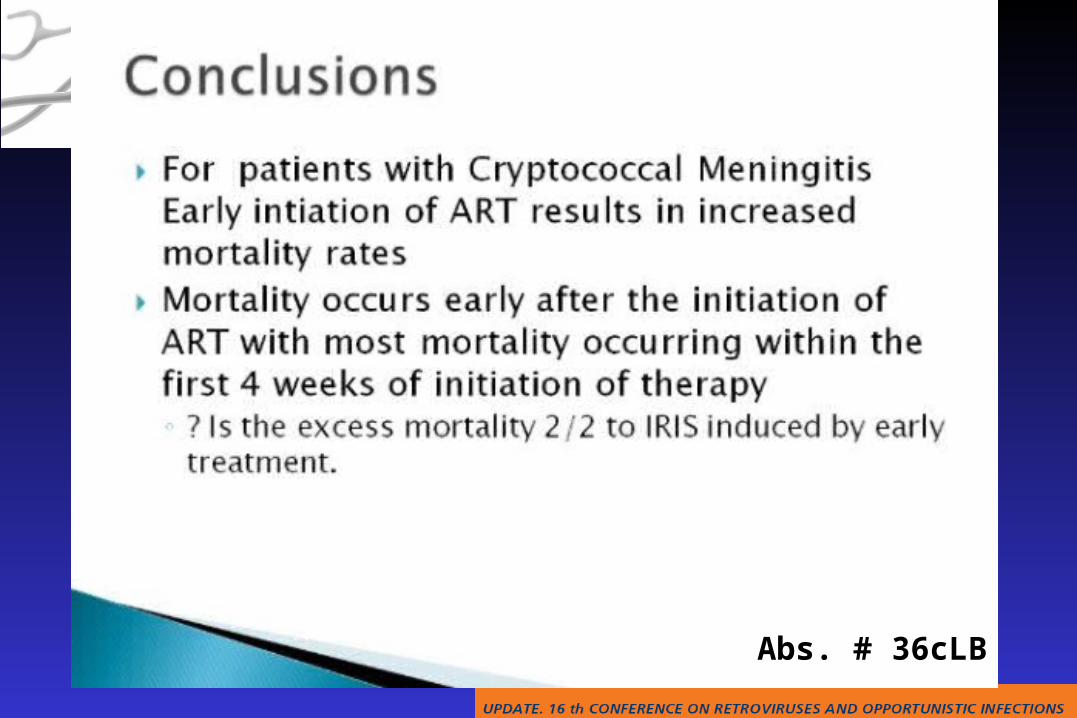
Abs. # 36cLB
Abs. # 36cLB
Abs. # 36cLB
Abs. # 36cLB
Abs. # 36cLB
Tuberculosis Other opportunistic infections IRIS HBV & HCV co-infections Cirrhosis & liver transplantation Tumors
Tuberculosis Other opportunistic infections IRIS HBV & HCV co-infections Cirrhosis & liver transplantation Tumors
OIs, Hepatitis Coinfections & Tumors
OIs, Hepatitis Coinfections & Tumors
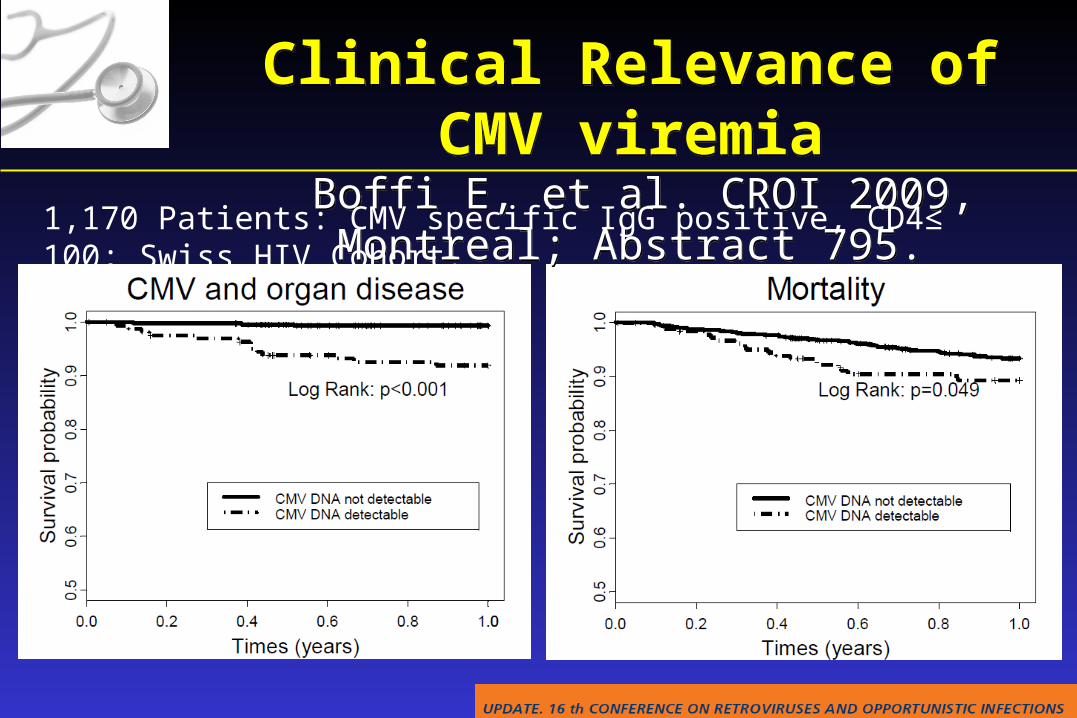
Clinical Relevance of CMV viremia Boffi E, et al. CROI 2009, Montreal; Abstract 795.Clinical Relevance of CMV viremia Boffi E, et al. CROI 2009, Montreal; Abstract 795.
1,170 Patients: CMV specific IgG positive, CD4≤ 100; Swiss HIV Cohort.
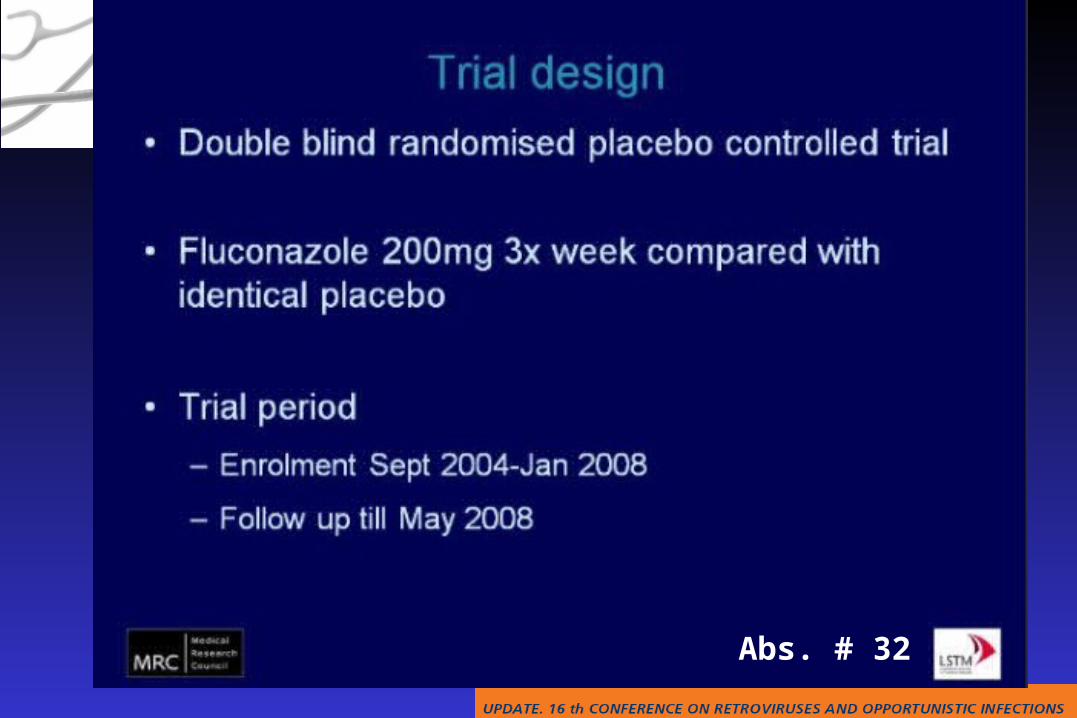
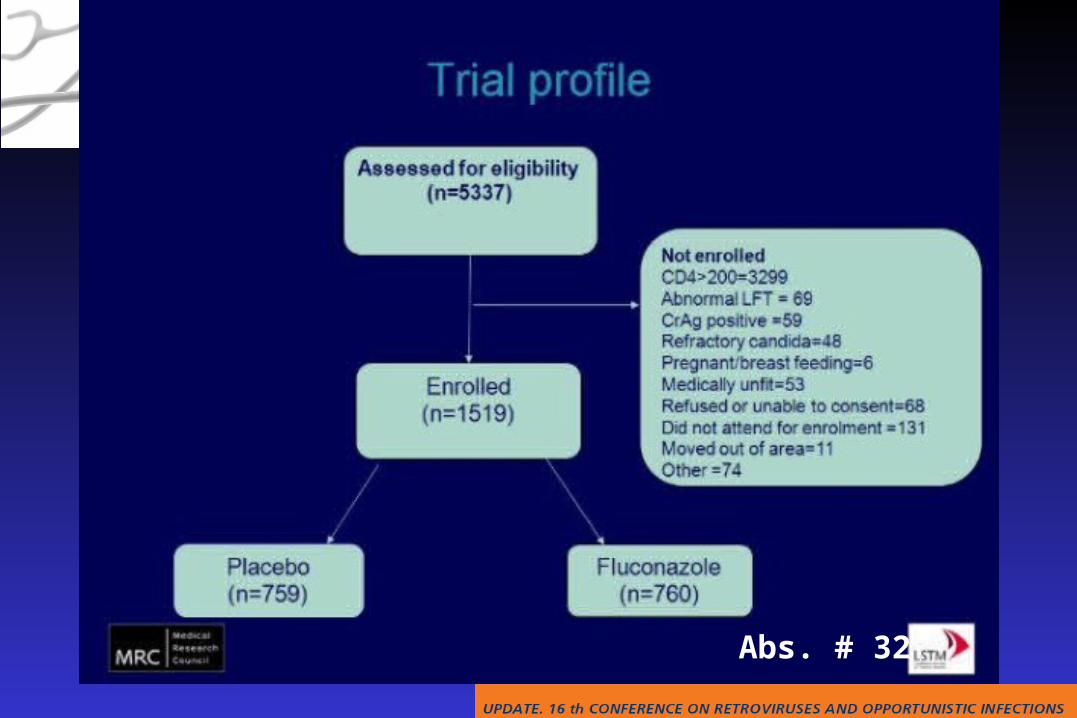
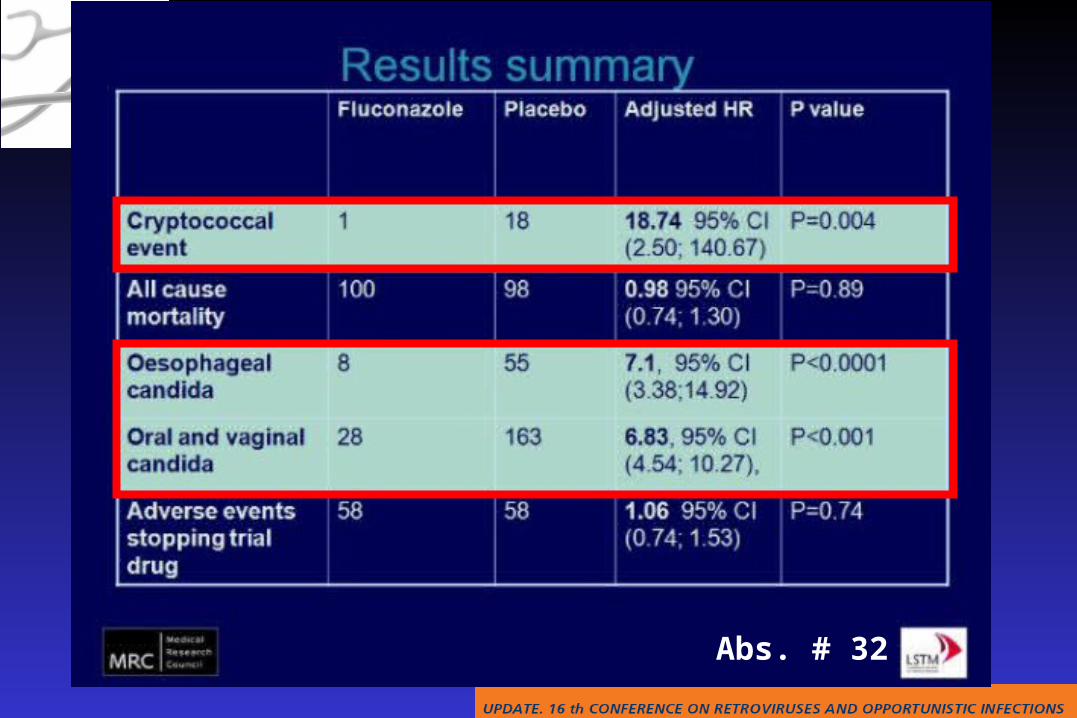
Abs. # 32
Abs. # 32
Abs. # 32
Abs. # 32
Tuberculosis Other opportunistic infections IRIS HBV & HCV co-infections Cirrhosis & liver transplantation Tumors
Tuberculosis Other opportunistic infections IRIS HBV & HCV co-infections Cirrhosis & liver transplantation Tumors
OIs, Hepatitis Coinfections & Tumors
OIs, Hepatitis Coinfections & Tumors
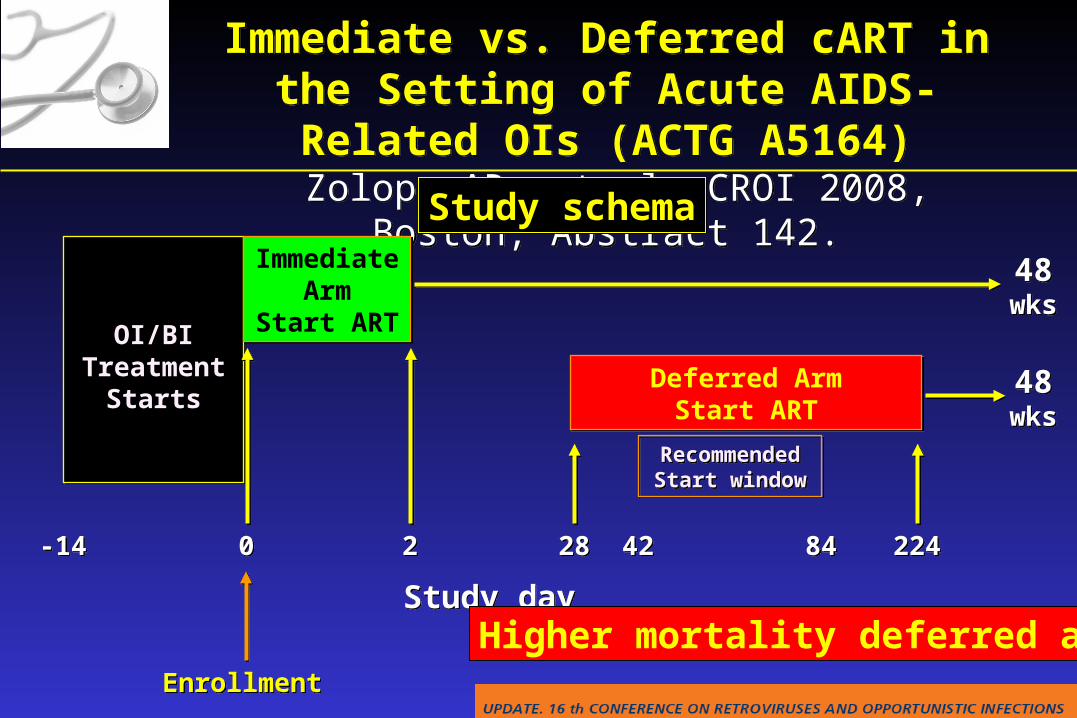
Immediate vs. Deferred cART in the Setting of Acute AIDS-Related OIs (ACTG A5164)
Zolopa AR, et al. CROI 2008, Boston; Abstract 142.
Immediate vs. Deferred cART in the Setting of Acute AIDS-Related OIs (ACTG A5164)
Zolopa AR, et al. CROI 2008, Boston; Abstract 142.
Study day Study day
EnrollmentEnrollment
OI/BI Treatment
Starts
OI/BI Treatment
Starts
Immediate Arm
Start ART
Immediate Arm
Start ART
Deferred ArmStart ART
Deferred ArmStart ART
RecommendedStart window
RecommendedStart window
48wks48
wks
48wks48
wks
-14-14 00 22 2828 4242 8484 224224
Study schemaStudy schema
Higher mortality deferred arm !

Immediate vs. Deferred cART in the Setting of Acute AIDS-Related OIs (ACTG A5164)
Zolopa AR, et al. CROI 2008, Boston; Abstract 142.
Immediate vs. Deferred cART in the Setting of Acute AIDS-Related OIs (ACTG A5164)
Zolopa AR, et al. CROI 2008, Boston; Abstract 142.
Outcome Immediate Deferred p-value
IRIS reported 10 13IRIS confirmed 8 (5.7%) 12 (8.5%)Lab AEsGrades 2-3-4 31 - 39 - 20 36 - 45 - 21 0.77Clinical AEsGrades 2-3-4 14 - 40 - 7 34 - 29 - 6 0.87Hospitalizations (>30 d.)
Subjects 39% 36% 0.63Hospital days (median) 5 6 0.79
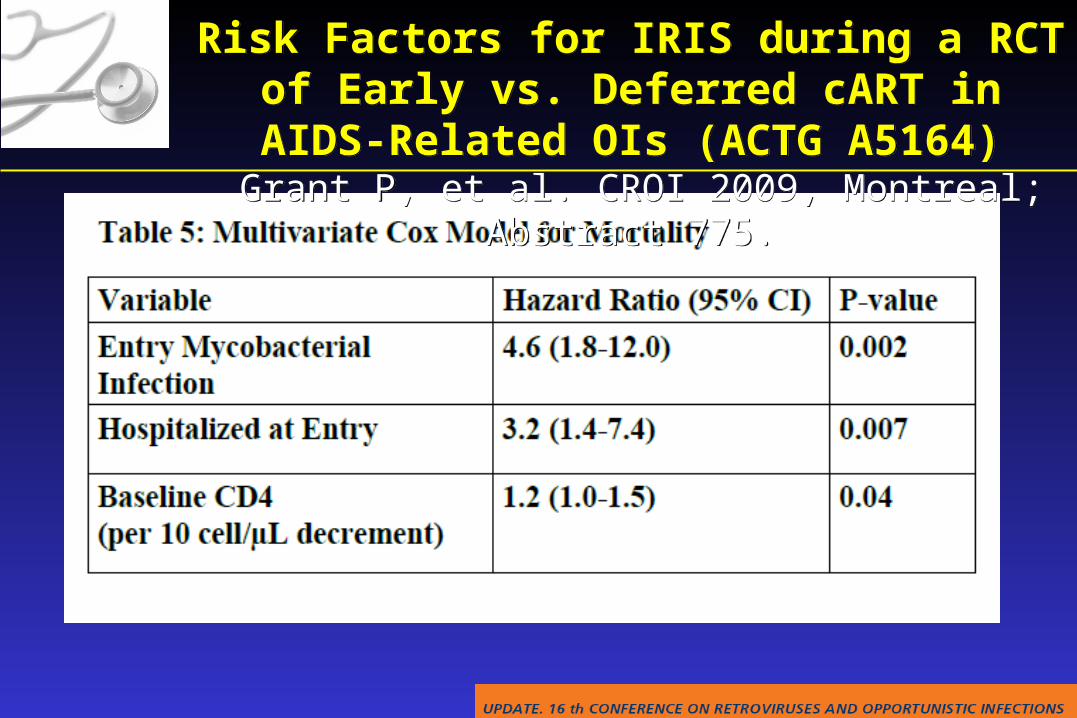
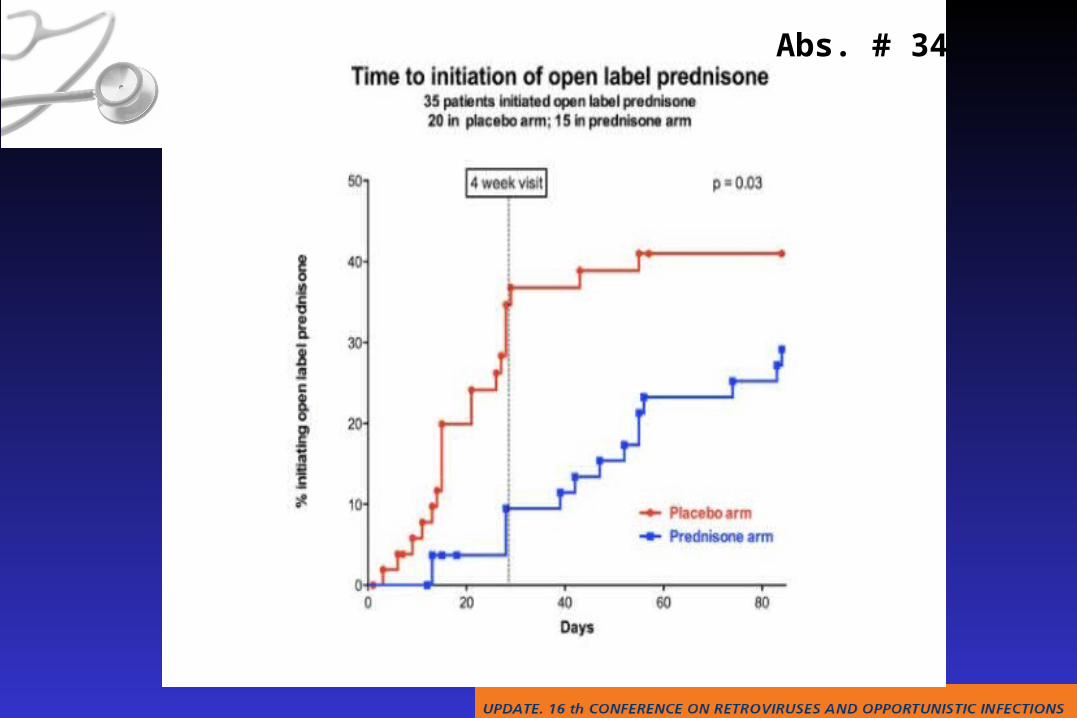
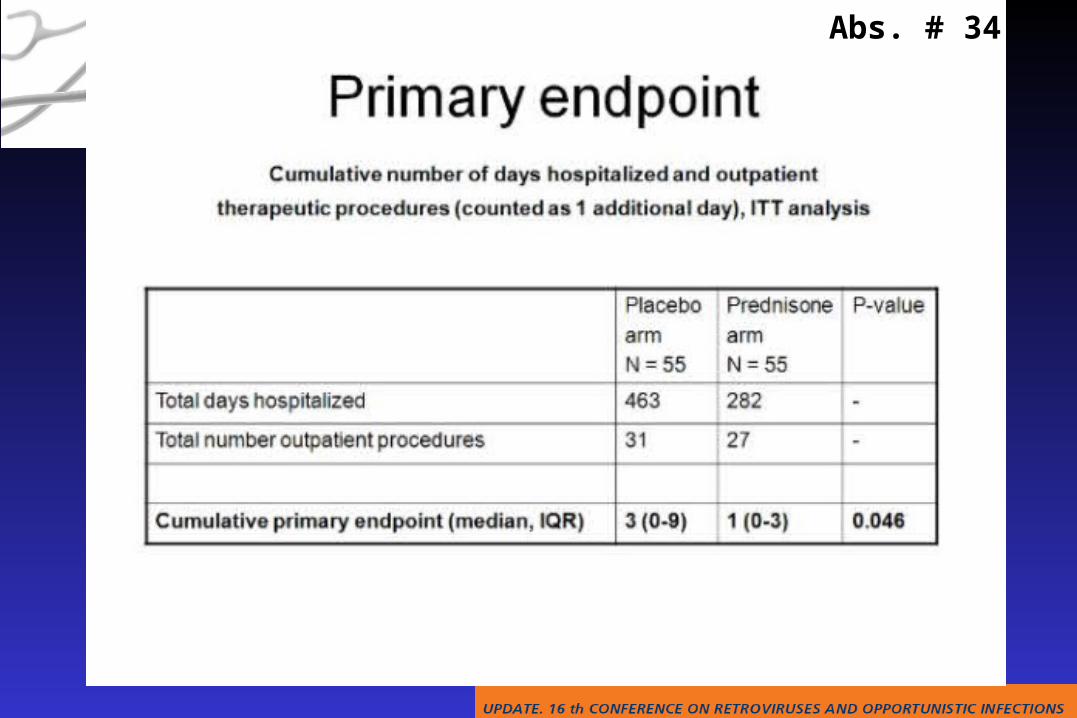
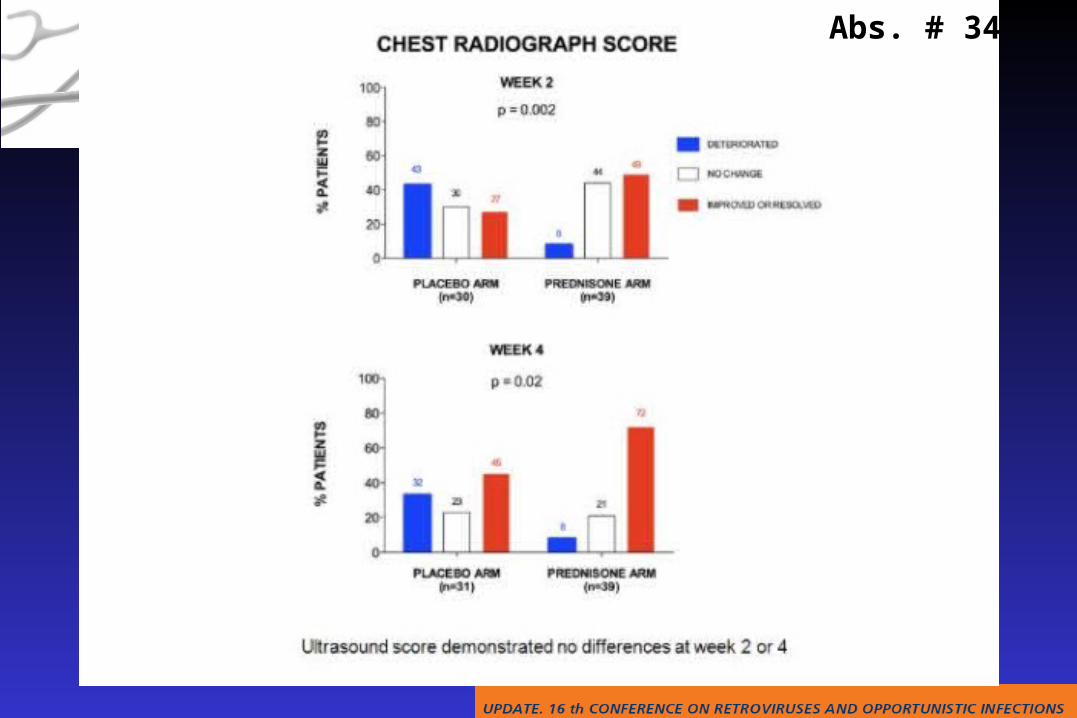
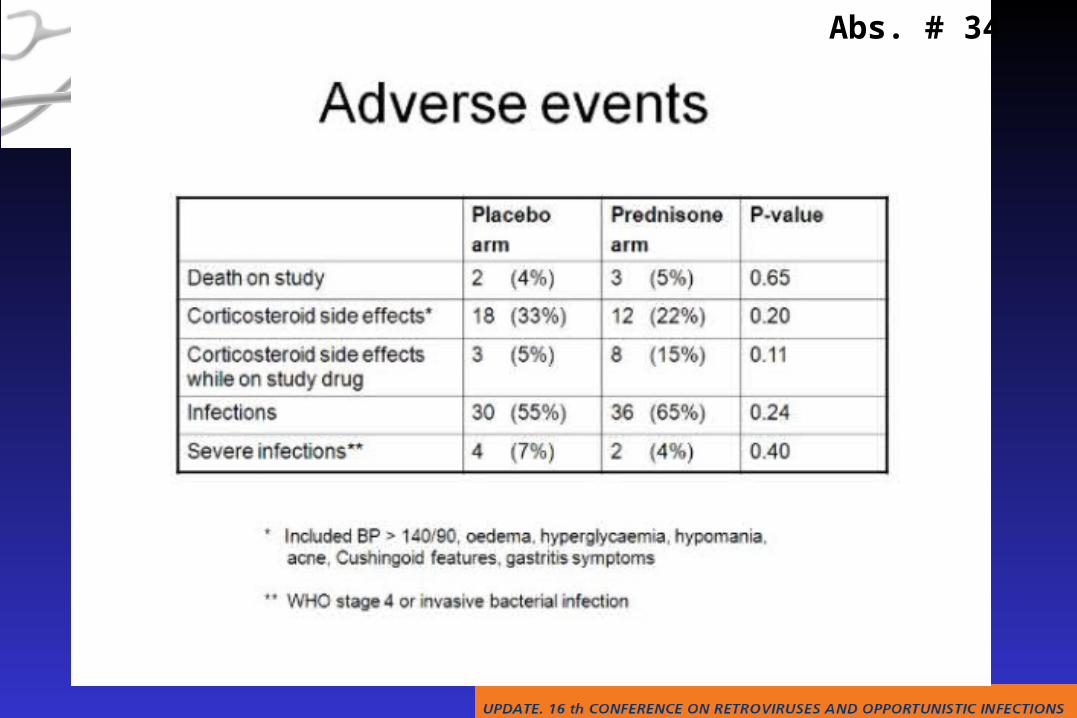
Risk Factors for IRIS during a RCT of Early vs. Deferred cART in AIDS-Related OIs (ACTG A5164)
Grant P, et al. CROI 2009, Montreal; Abstract 775.
Risk Factors for IRIS during a RCT of Early vs. Deferred cART in AIDS-Related OIs (ACTG A5164)
Grant P, et al. CROI 2009, Montreal; Abstract 775.
Abs. # 34
Abs. # 34
Abs. # 34
Abs. # 34
Abs. # 34
Abs. # 34
Abs. # 34
Tuberculosis Other opportunistic infections IRIS HBV & HCV co-infections Cirrhosis & Liver transplantation Tumors
Tuberculosis Other opportunistic infections IRIS HBV & HCV co-infections Cirrhosis & Liver transplantation Tumors
OIs, Hepatitis Coinfections & Tumors
OIs, Hepatitis Coinfections & Tumors
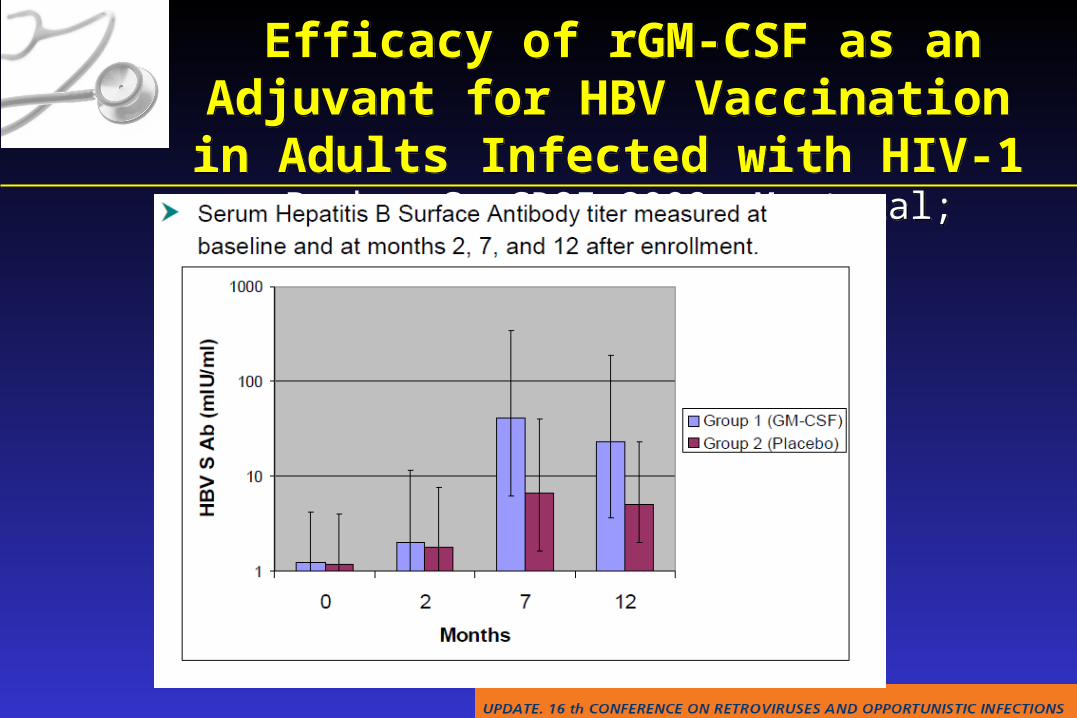
Efficacy of rGM-CSF as an Adjuvant for HBV Vaccination in Adults Infected with HIV-1
Parker S. CROI 2009, Montreal; Abstract 808.
Efficacy of rGM-CSF as an Adjuvant for HBV Vaccination in Adults Infected with HIV-1
Parker S. CROI 2009, Montreal; Abstract 808.
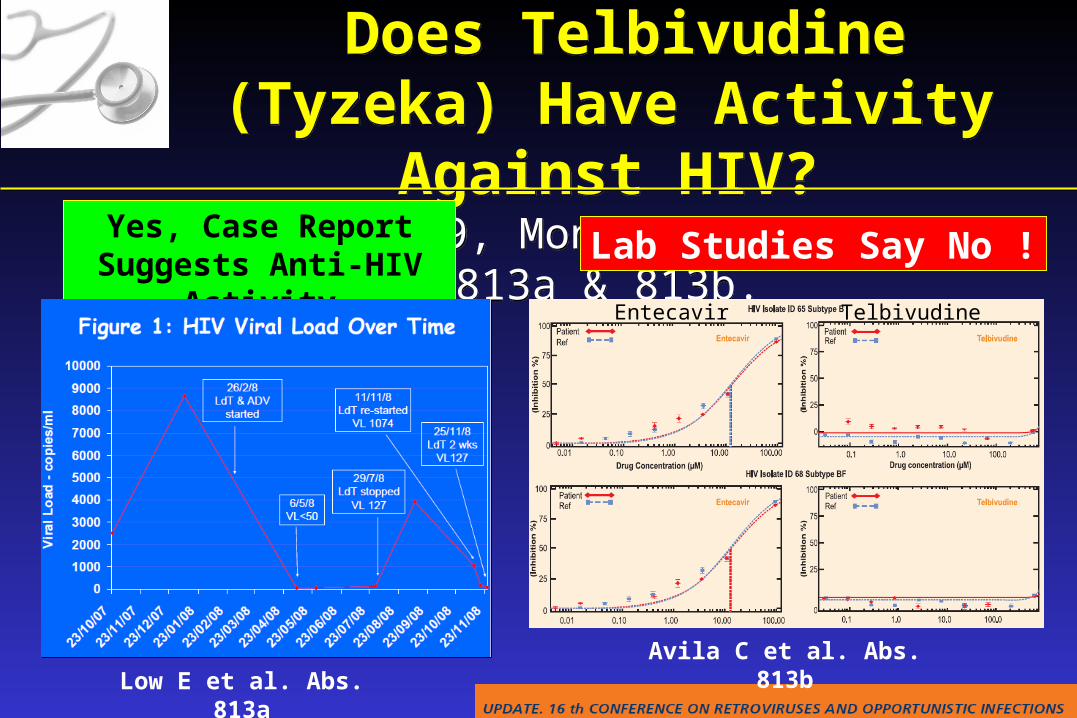
Does Telbivudine (Tyzeka) Have Activity Against HIV?
CROI 2009, Montreal; Abstracts 813a & 813b.
Does Telbivudine (Tyzeka) Have Activity Against HIV?
CROI 2009, Montreal; Abstracts 813a & 813b.Yes, Case Report Suggests
Anti-HIV Activity Lab Studies Say No !
Low E et al. Abs. 813aAvila C et al. Abs. 813b
Entecavir Telbivudine
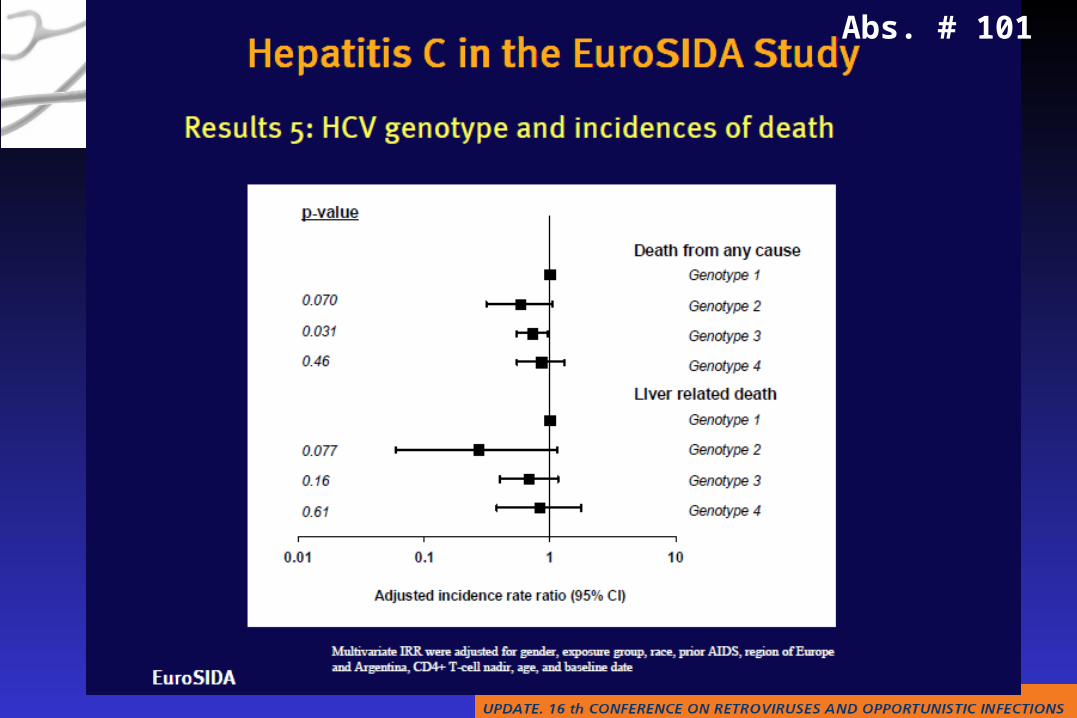
Abs. # 101
Abs. # 101
Abs. # 101
Abs. # 101
Abs. # 101
Abs. # 101

Abs. # 101
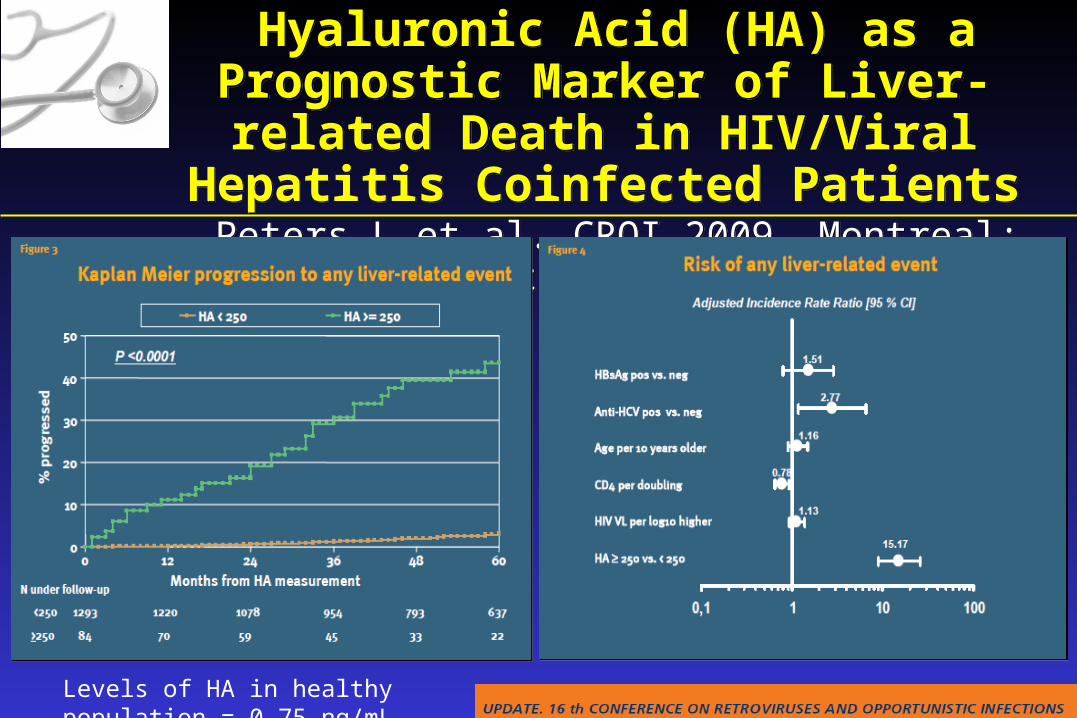
Hyaluronic Acid (HA) as a Prognostic Marker of Liver-related Death in HIV/Viral Hepatitis
Coinfected Patients Peters L et al. CROI 2009, Montreal; Abstracts 821.
Hyaluronic Acid (HA) as a Prognostic Marker of Liver-related Death in HIV/Viral Hepatitis
Coinfected Patients Peters L et al. CROI 2009, Montreal; Abstracts 821.
Levels of HA in healthy population = 0-75 ng/mL
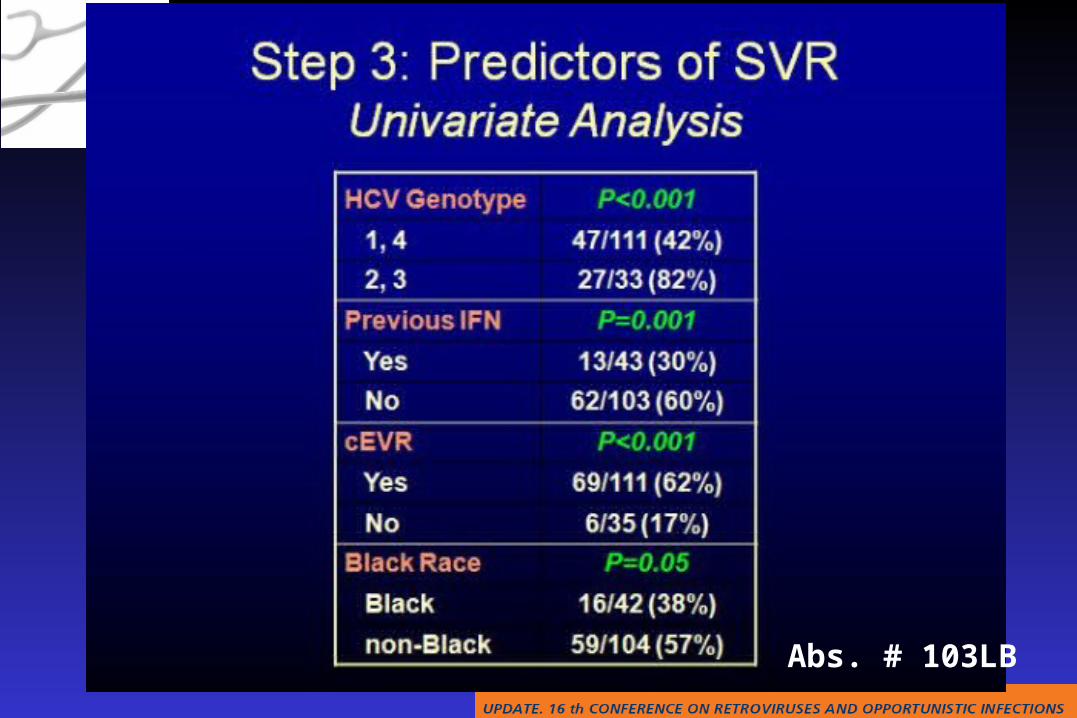
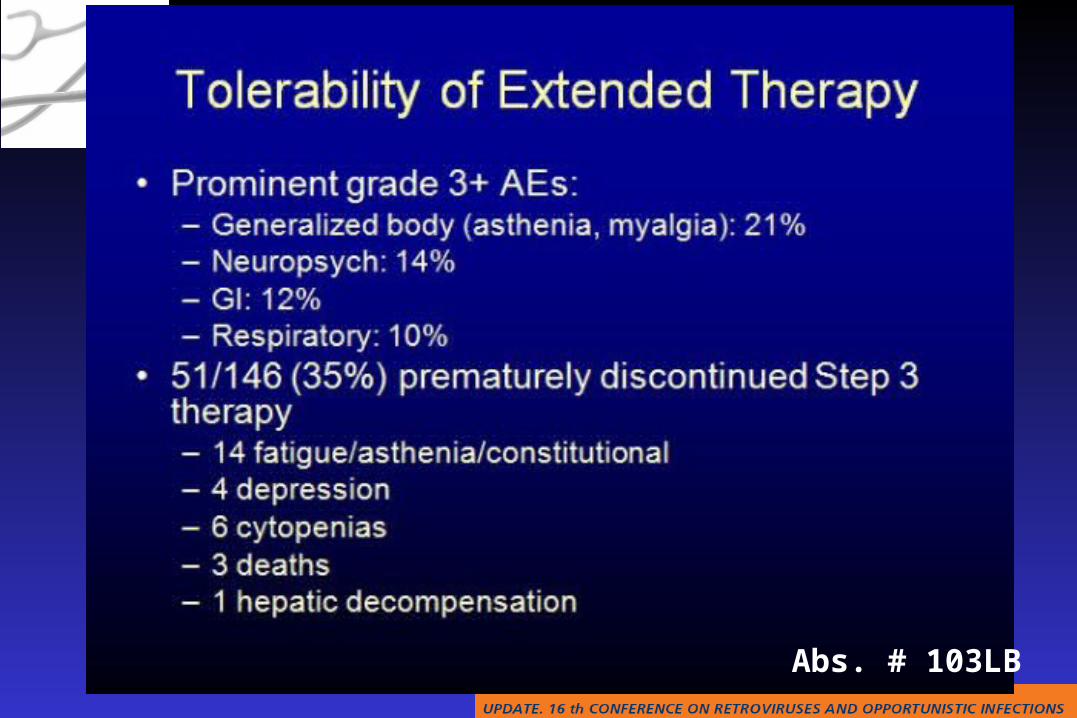
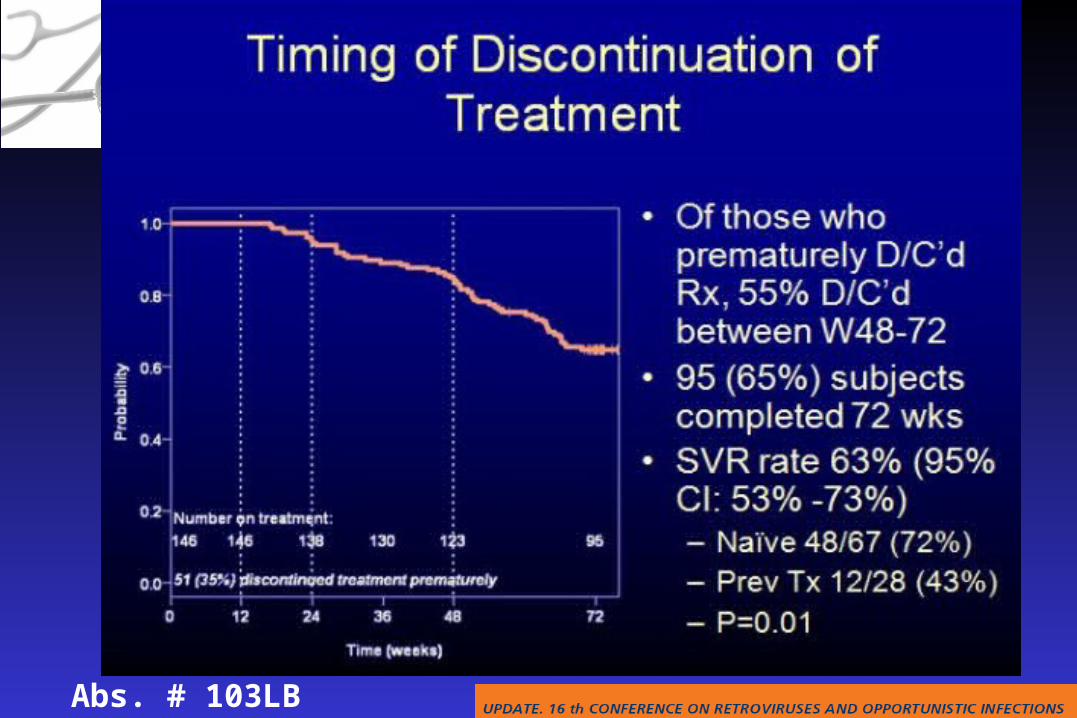
Sustained Long-term Antiviral Maintenance with Pegylated Interferon in HCV/HIV Coinfected
Patients (SLAM-C): Role of Early Virologic Response in Extended Therapy with PEG-
Interferon (PEG) and Weight-Based Ribavirin (WBR) in HCV-HIV Coinfection
RT Chung, T Umbleja, AA Butt, ZD Goodman, JW Andersen, M Koziel, B Alston, M Peters, M Sulkowski, KE Sherman for the
ACTG A5178 Team
Abs. # 103LB
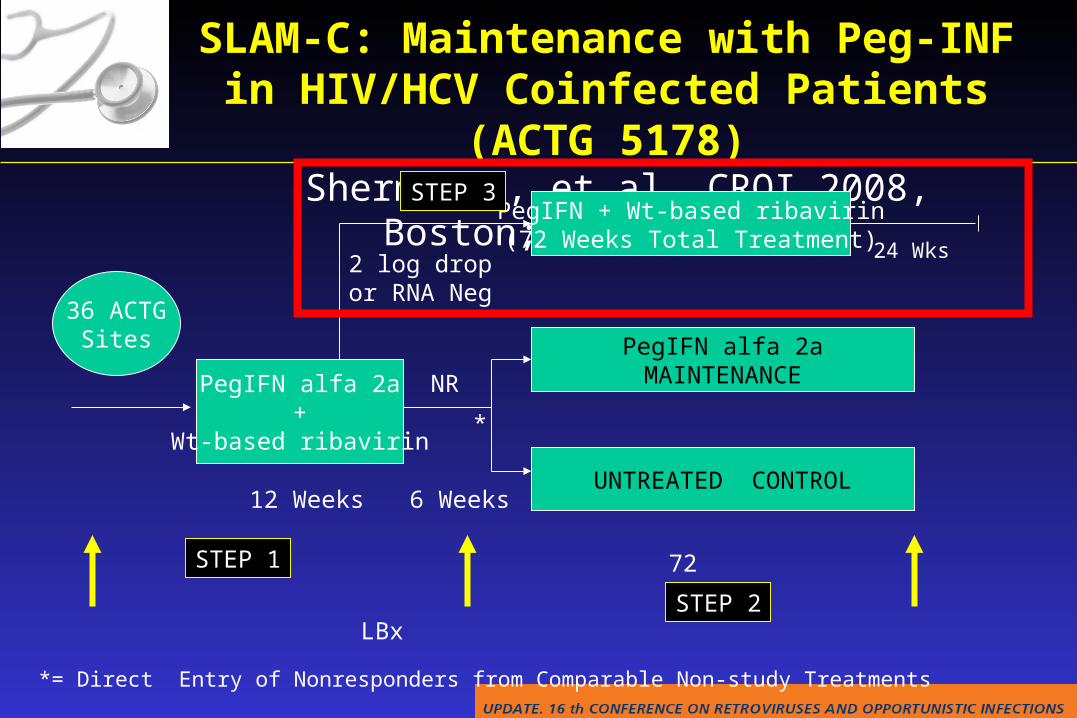
SLAM-C: Maintenance with Peg-INF in HIV/HCV Coinfected Patients (ACTG 5178)
Sherman K, et al. CROI 2008, Boston; Abstract 59.
PegIFN alfa 2a+
Wt-based ribavirin
12 Weeks 6 WeeksUNTREATED CONTROL
PegIFN alfa 2aMAINTENANCE
PegIFN + Wt-based ribavirin(72 Weeks Total Treatment)
72 Weeks
NR
2 log dropor RNA Neg
LBx LBx LBx
24 Wks
36 ACTGSites
*
*= Direct Entry of Nonresponders from Comparable Non-study Treatments
STEP 1
STEP 2
STEP 3
Abs. # 103LB
Abs. # 103LB
Abs. # 103LB
Abs. # 103LB
Abs. # 103LB
Abs. # 103LB
Abs. # 103LB
Tuberculosis Other opportunistic infections IRIS HBV & HCV co-infections Cirrhosis & Liver transplantation Tumors
Tuberculosis Other opportunistic infections IRIS HBV & HCV co-infections Cirrhosis & Liver transplantation Tumors
OIs, Hepatitis Coinfections & Tumors
OIs, Hepatitis Coinfections & Tumors

Survival Of HIV-HCV Co-infected Patients With Compensated Liver Cirrhosis: Impact Of Hepatitis C
TherapyM Montes, J Pascual,, M Lopez-Dieguez, C Tural, C Quereda, E Ortega, A Arranz, M Von Wichmann, E Barquilla, J Arribas, and GESIDA 37/03-FIPSE 36680/07 Study Group.
Abs. # 106
OBJECTIVE
To evaluate the effect of therapy for chronic hepatitis C in HIV-HCV coinfected patients with compensated liver cirrhosis on: Survival The incidence of first hepatic decompensation
Abs. # 106
All HCV
Treated
HCV
Non Treated
P
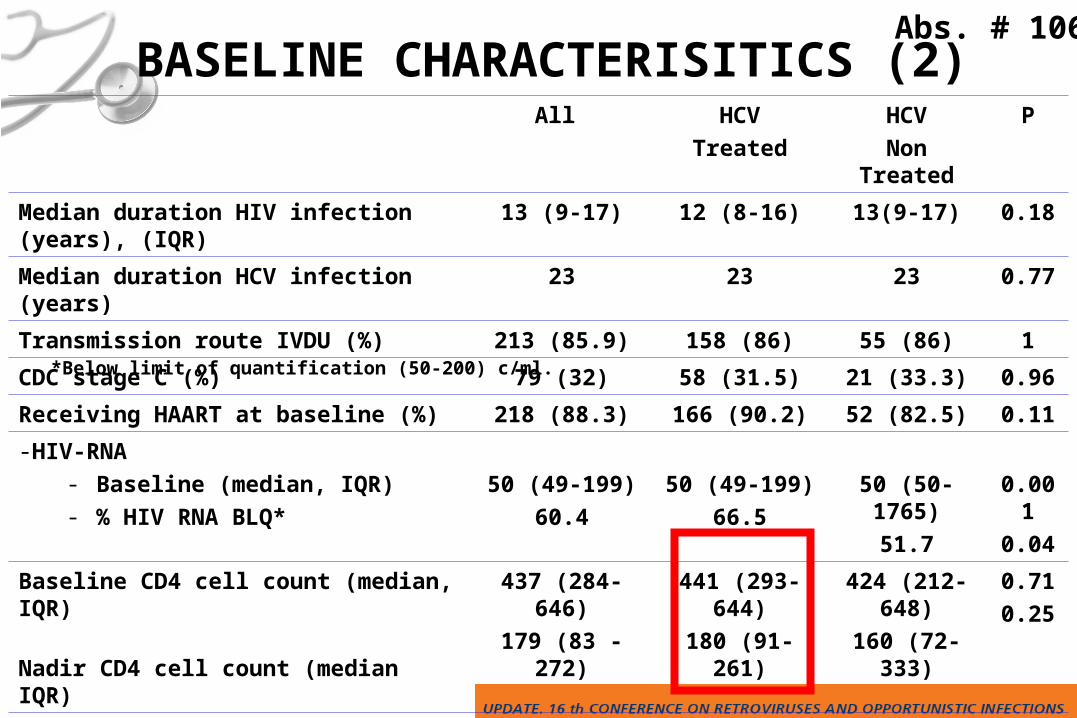
Median duration HIV infection (years), (IQR) 13 (9-17) 12 (8-16) 13(9-17) 0.18
Median duration HCV infection (years) 23 23 23 0.77
Transmission route IVDU (%) 213 (85.9) 158 (86) 55 (86) 1
CDC stage C (%) 79 (32) 58 (31.5) 21 (33.3) 0.96
Receiving HAART at baseline (%) 218 (88.3) 166 (90.2) 52 (82.5) 0.11
-HIV-RNA- Baseline (median, IQR)- % HIV RNA BLQ*
50 (49-199)
60.4
50 (49-199)
66.5
50 (50-1765)
51.7
0.001
0.04
Baseline CD4 cell count (median, IQR)
Nadir CD4 cell count (median IQR)
437 (284-646)
179 (83 - 272)
441 (293-644)
180 (91-261)
424 (212-648)
160 (72-333)
0.71
0.25
HCV treatment received (%)–Sustained virological response (%)–Still receiving HCV treatment (%)–Non responders or relapsers (%)
184 (74,2) 184
44 (24)
3 (1.6%)
137 (74.4)
-
-
-
-
-
-
-
-
BASELINE CHARACTERISITICS (2)
*Below limit of quantification (50-200) c/ml.
Abs. # 106
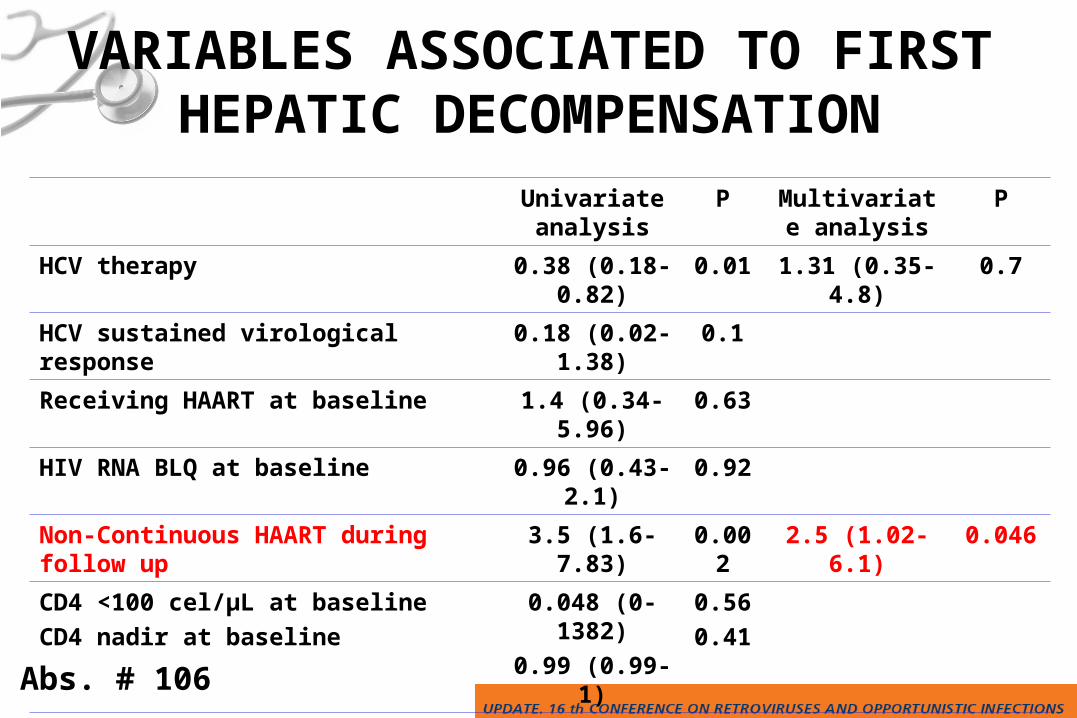
VARIABLES ASSOCIATED TO FIRST HEPATIC DECOMPENSATION
Univariate analysis
P Multivariate analysis
P
HCV therapy 0.38 (0.18-0.82) 0.01 1.31 (0.35-4.8) 0.7
HCV sustained virological response 0.18 (0.02-1.38) 0.1
Receiving HAART at baseline 1.4 (0.34-5.96) 0.63
HIV RNA BLQ at baseline 0.96 (0.43-2.1) 0.92
Non-Continuous HAART during follow up 3.5 (1.6-7.83) 0.002 2.5 (1.02-6.1) 0.046
CD4 <100 cel/µL at baseline
CD4 nadir at baseline
0.048 (0-1382)
0.99 (0.99-1)
0.56
0.41
-Child Pugh score B at baseline-Child Pugh score C at baseline
8.2 (3.66-18.68)
60.5 (7.1-516.5)
0.000
0.0005.8 (2.41-13.8)
62.2 (6.2-618)
0.001
0.001
Abs. # 106
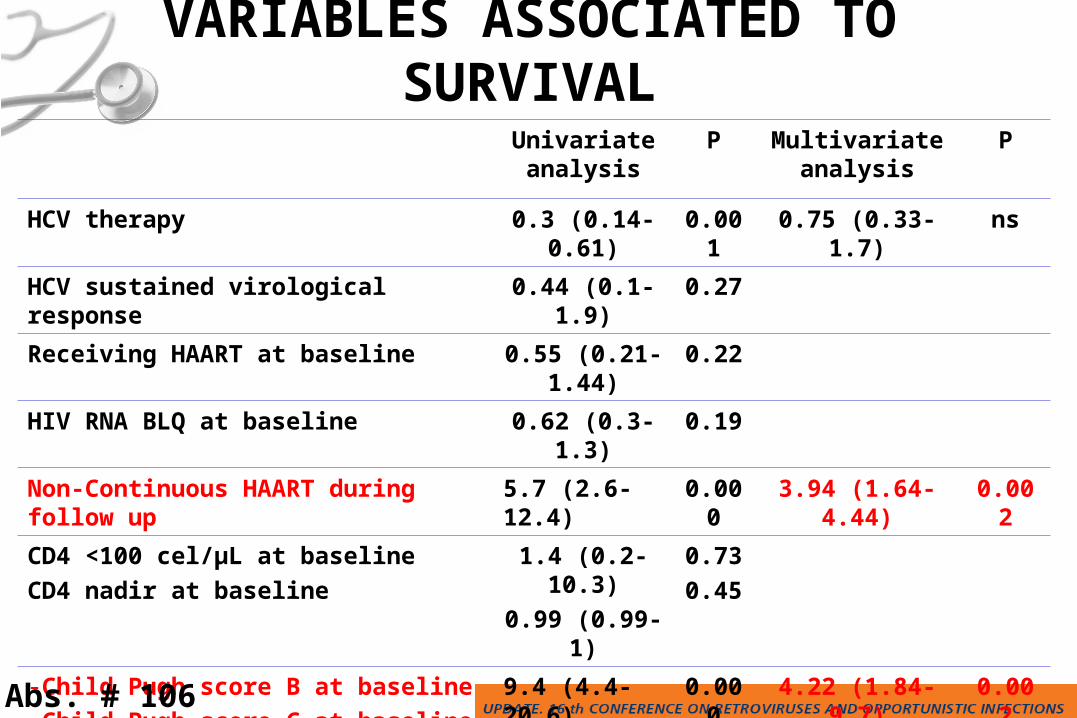
VARIABLES ASSOCIATED TO SURVIVAL
Univariate analysis
P Multivariate analysis
P
HCV therapy 0.3 (0.14-0.61) 0.001 0.75 (0.33-1.7) ns
HCV sustained virological response 0.44 (0.1-1.9) 0.27
Receiving HAART at baseline 0.55 (0.21-1.44) 0.22
HIV RNA BLQ at baseline 0.62 (0.3-1.3) 0.19
Non-Continuous HAART during follow up 5.7 (2.6-12.4) 0.000 3.94 (1.64-4.44) 0.002
CD4 <100 cel/µL at baseline
CD4 nadir at baseline
1.4 (0.2-10.3)
0.99 (0.99-1)
0.73
0.45
-Child Pugh score B at baseline-Child Pugh score C at baseline
9.4 (4.4-20.6)
44 (9.7-201)
0.000
0.000
4.22 (1.84-9.7)
17.2 (2.83-104)
0.002
0.001
-Decompensation during follow up 10.71 (5.21-22) 0.000 5.1 (2.35-11.3) 0.001
Abs. # 106
José M. Miró,1 Miguel Montejo,2 Lluis Castells,3 Juan C. Meneu,4 Antonio Rafecas,5 Marino Blanes,6 Jesús Fortún,7 Gloria de la Rosa,8 Iñaki Pérez,1 Antonio Rimola,1 and the Spanish OLT in HIV-Infected Patients Working
Group.
1Hosp. Clínic-IDIBAPS. Univ. of Barcelona, Barcelona; 2Hosp. Cruces, Bilbao; 3Hosp. Univ. Vall d’Hebrón, Barcelona; 4Hosp. Univ. 12 de Octubre, Madrid; 5Hosp Bellvitge-IDIBELL, Barcelona; 6Hosp. La Fe, Valencia; 7Hosp. Ramón y
Cajal, Madrid; 8Organización Nacional de Trasplante (ONT), Madrid, Spain.
José M. Miró,1 Miguel Montejo,2 Lluis Castells,3 Juan C. Meneu,4 Antonio Rafecas,5 Marino Blanes,6 Jesús Fortún,7 Gloria de la Rosa,8 Iñaki Pérez,1 Antonio Rimola,1 and the Spanish OLT in HIV-Infected Patients Working
Group.
1Hosp. Clínic-IDIBAPS. Univ. of Barcelona, Barcelona; 2Hosp. Cruces, Bilbao; 3Hosp. Univ. Vall d’Hebrón, Barcelona; 4Hosp. Univ. 12 de Octubre, Madrid; 5Hosp Bellvitge-IDIBELL, Barcelona; 6Hosp. La Fe, Valencia; 7Hosp. Ramón y
Cajal, Madrid; 8Organización Nacional de Trasplante (ONT), Madrid, Spain.
5-Year Survival of HCV/HIV- Coinfected Liver Transplant Recipients (OLT): A Case-
Control Study
16th CROI 2009, Montreal (Canada) - 200916th CROI 2009, Montreal (Canada) - 2009
Abs. # 833
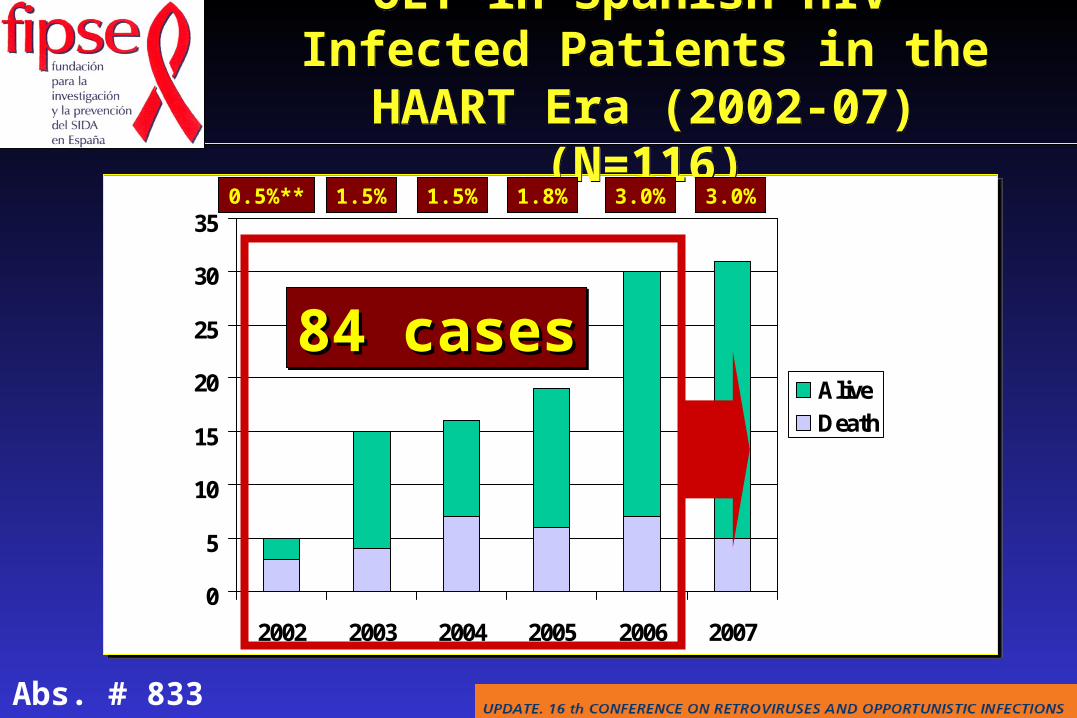
OLT in Spanish HIV-Infected Patients in the HAART Era (2002-07) (N=116)
OLT in Spanish HIV-Infected Patients in the HAART Era (2002-07) (N=116)
0
5
10
15
20
25
30
35
2002 2003 2004 2005 2006 2007
AliveDeath
0.5%** 1.5% 1.8% 3.0% 3.0%1.5%
84 cases84 cases84 cases84 cases
Abs. # 833
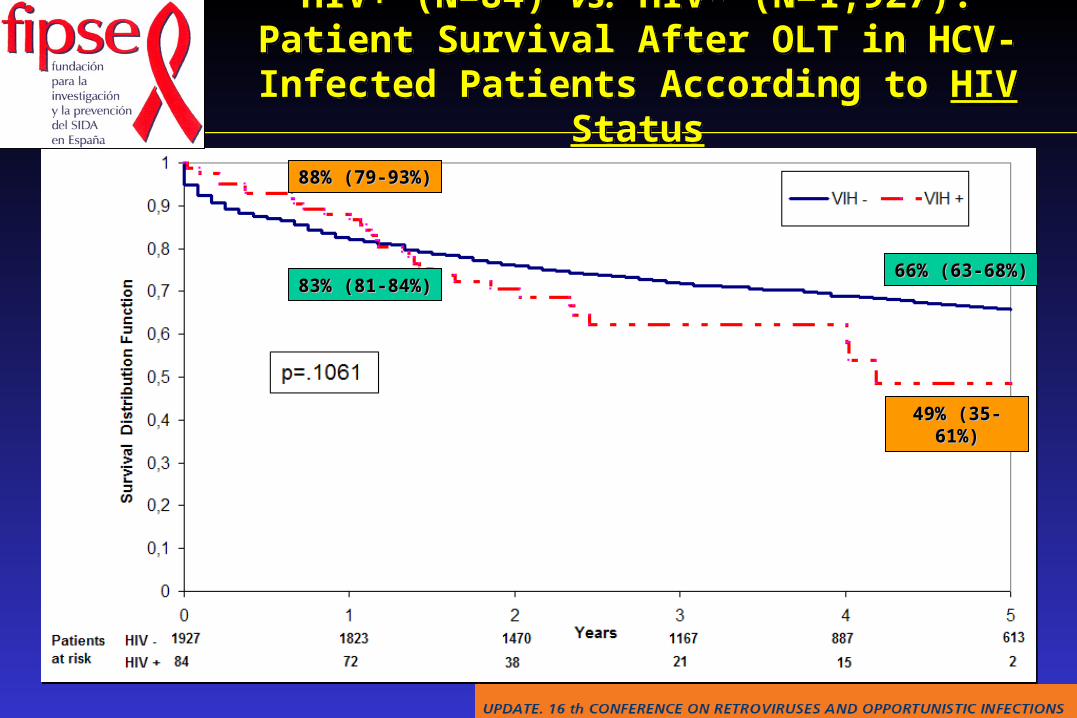
HIV+ (N=84) vs. HIV- (N=1,927): Patient Survival After OLT in HCV-Infected Patients According to HIV StatusHIV+ (N=84) vs. HIV- (N=1,927): Patient Survival After
OLT in HCV-Infected Patients According to HIV Status
49% (35-61%)49% (35-61%)
88% (79-93%)88% (79-93%)
66% (63-68%)66% (63-68%)83% (81-84%)83% (81-84%)
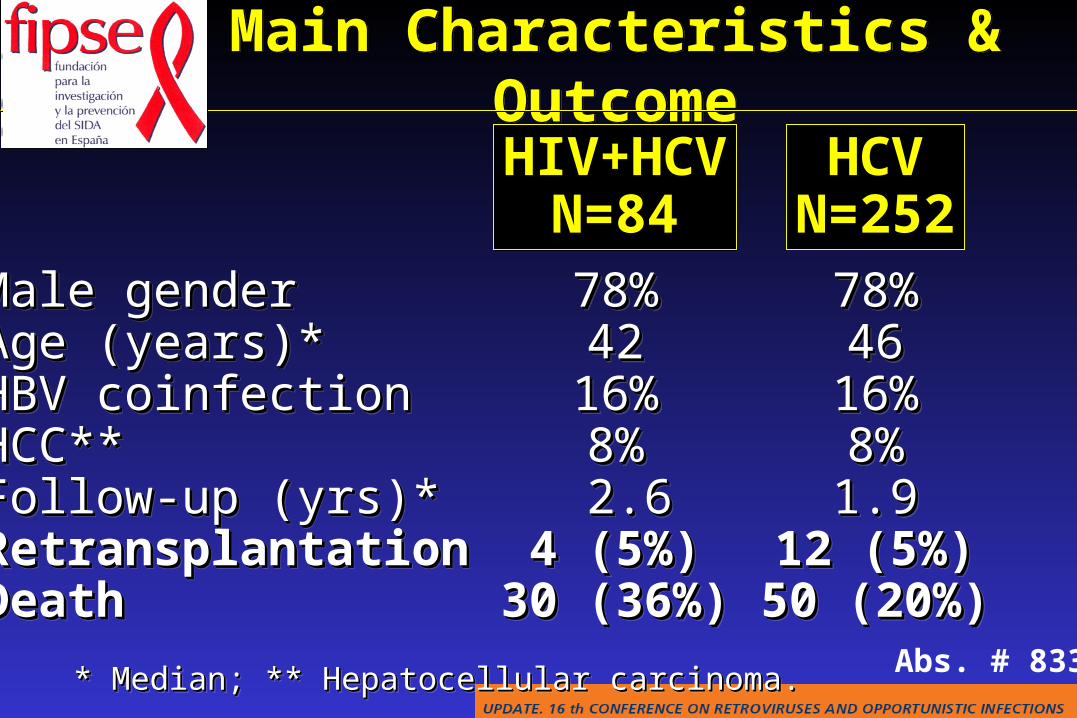
Main Characteristics & OutcomeMain Characteristics & Outcome
Male genderMale genderAgeAge ( (yearsyears)*)*HBV coinfectionHBV coinfectionHCC**HCC**Follow-up (yrs)*Follow-up (yrs)*RetransplantationRetransplantationDeathDeath
Male genderMale genderAgeAge ( (yearsyears)*)*HBV coinfectionHBV coinfectionHCC**HCC**Follow-up (yrs)*Follow-up (yrs)*RetransplantationRetransplantationDeathDeath
78%78%4242
16%16%8%8% 2.62.6
4 (4 (55%)%)30 (36%)30 (36%)
78%78%4242
16%16%8%8% 2.62.6
4 (4 (55%)%)30 (36%)30 (36%)
* * MeMediandian; ** Hepatocellular carcinoma. ; ** Hepatocellular carcinoma. * * MeMediandian; ** Hepatocellular carcinoma. ; ** Hepatocellular carcinoma.
78%78%4646
16%16%8%8%1.91.9
12 (12 (55%)%)50 (20%)50 (20%)
78%78%4646
16%16%8%8%1.91.9
12 (12 (55%)%)50 (20%)50 (20%)
HIV+HCVN=84
HIV+HCVN=84
HCVN=252
Abs. # 833
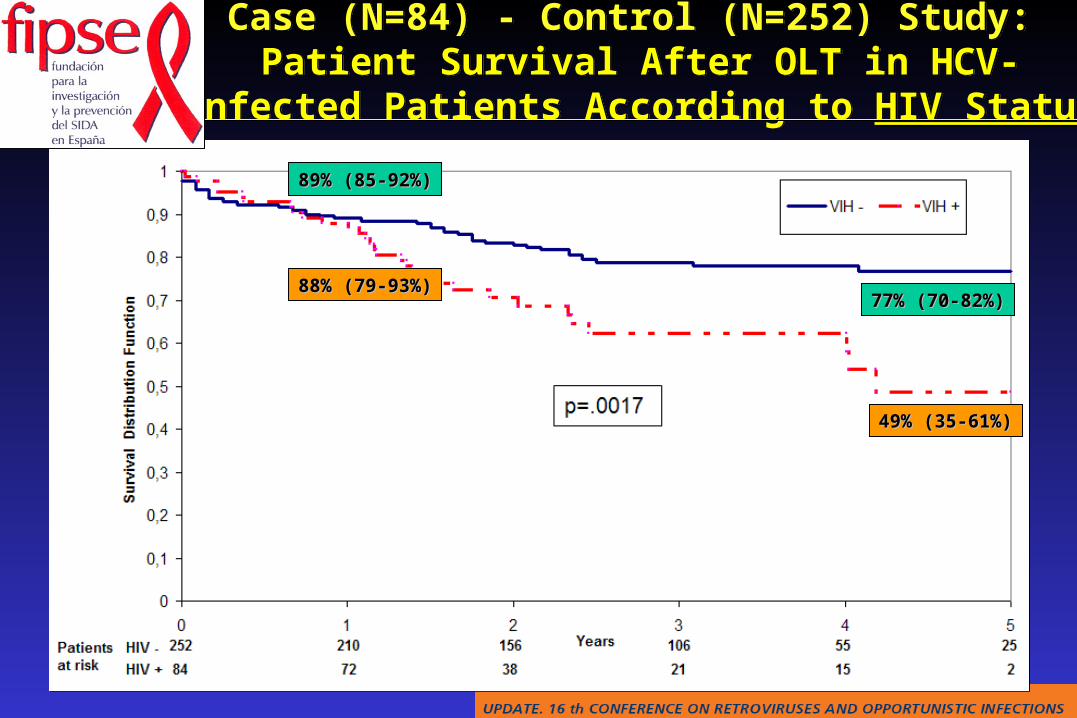
Case (N=84) - Control (N=252) Study: Patient Survival After OLT in HCV-Infected Patients According to HIV Status
Case (N=84) - Control (N=252) Study: Patient Survival After OLT in HCV-Infected Patients According to HIV Status
49% (35-61%)49% (35-61%)
77% (70-82%)77% (70-82%)
89% (85-92%)89% (85-92%)
88% (79-93%)88% (79-93%)
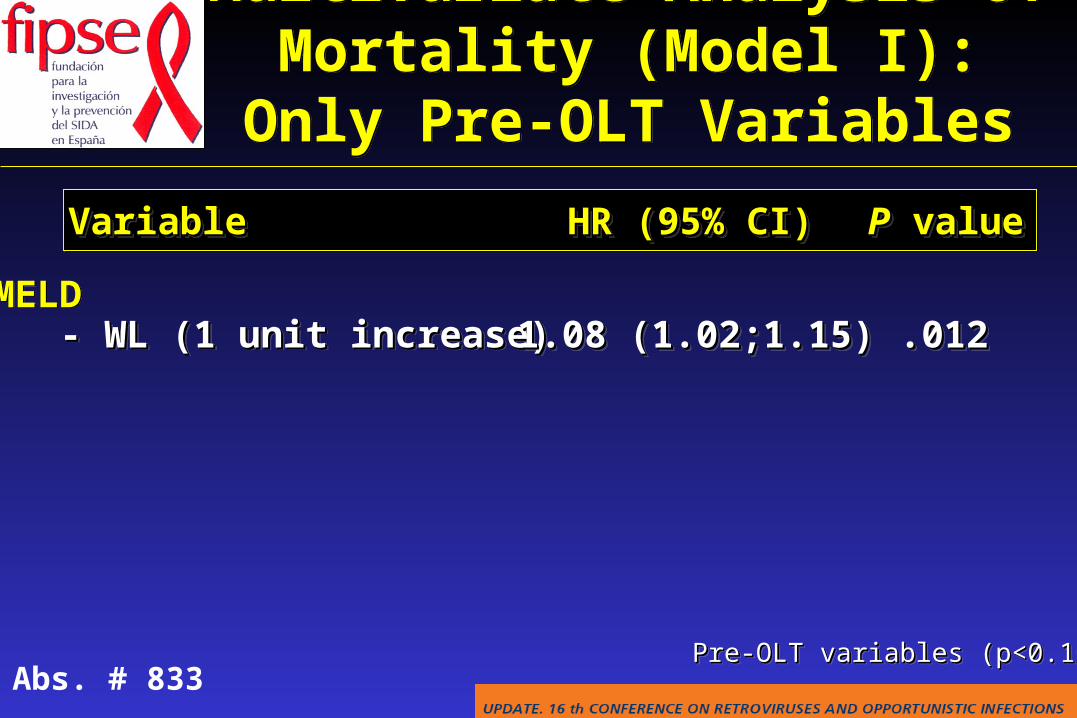
MELD - WL (1 unit increase)- WL (1 unit increase)MELD - WL (1 unit increase)- WL (1 unit increase)
VariableVariableVariableVariable HR (95%HR (95% CI)CI)HR (95%HR (95% CI)CI)
1.08 (1.02;1.15)1.08 (1.02;1.15)1.08 (1.02;1.15)1.08 (1.02;1.15)
PP value valuePP value value
.012.012.012.012
Multivariate Analysis of Mortality (Model I): Only Pre-OLT VariablesMultivariate Analysis of Mortality (Model I): Only Pre-OLT Variables
Pre-OLT variables (p<0.10)Pre-OLT variables (p<0.10)Pre-OLT variables (p<0.10)Pre-OLT variables (p<0.10)Abs. # 833
VariableVariableVariableVariable HR (95%HR (95% CI)CI)HR (95%HR (95% CI)CI) PP value valuePP value value
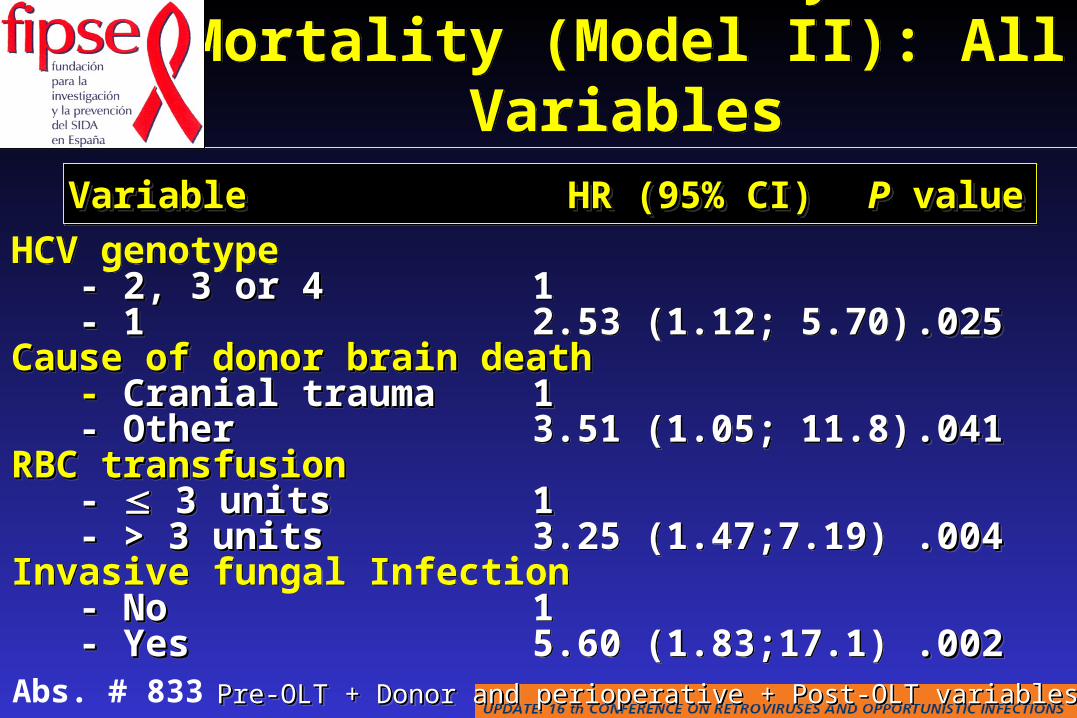
Pre-OLT + Donor and perioperative + Post-OLT variables (p<0.10)Pre-OLT + Donor and perioperative + Post-OLT variables (p<0.10)Pre-OLT + Donor and perioperative + Post-OLT variables (p<0.10)Pre-OLT + Donor and perioperative + Post-OLT variables (p<0.10)
Multivariate Analysis of Mortality (Model II): All Variables
Multivariate Analysis of Mortality (Model II): All Variables
HCV genotype - 2, 3 or 4- 2, 3 or 4 - - 11Cause of donor brain deathCause of donor brain death - - Cranial traumaCranial trauma - Other- OtherRBC RBC ttransfusionransfusion - - 3 units 3 units - > 3 units- > 3 unitsInvasive fungal Infection - No- No - Yes- Yes
HCV genotype - 2, 3 or 4- 2, 3 or 4 - - 11Cause of donor brain deathCause of donor brain death - - Cranial traumaCranial trauma - Other- OtherRBC RBC ttransfusionransfusion - - 3 units 3 units - > 3 units- > 3 unitsInvasive fungal Infection - No- No - Yes- Yes
12.53 (1.12; 5.70)
1 1 3.51 (1.05; 11.8)
1 1 3.25 (1.47;7.19)
15.60 (1.83;17.1)
12.53 (1.12; 5.70)
1 1 3.51 (1.05; 11.8)
1 1 3.25 (1.47;7.19)
15.60 (1.83;17.1)
.025.025
.041.041
.004.004
.002.002
.025.025
.041.041
.004.004
.002.002
Abs. # 833
Tuberculosis Other opportunistic infections IRIS HBV & HCV co-infections SOT in HIV-infected patients Tumors
Tuberculosis Other opportunistic infections IRIS HBV & HCV co-infections SOT in HIV-infected patients Tumors
OIs, Hepatitis Coinfections & Tumors
OIs, Hepatitis Coinfections & Tumors
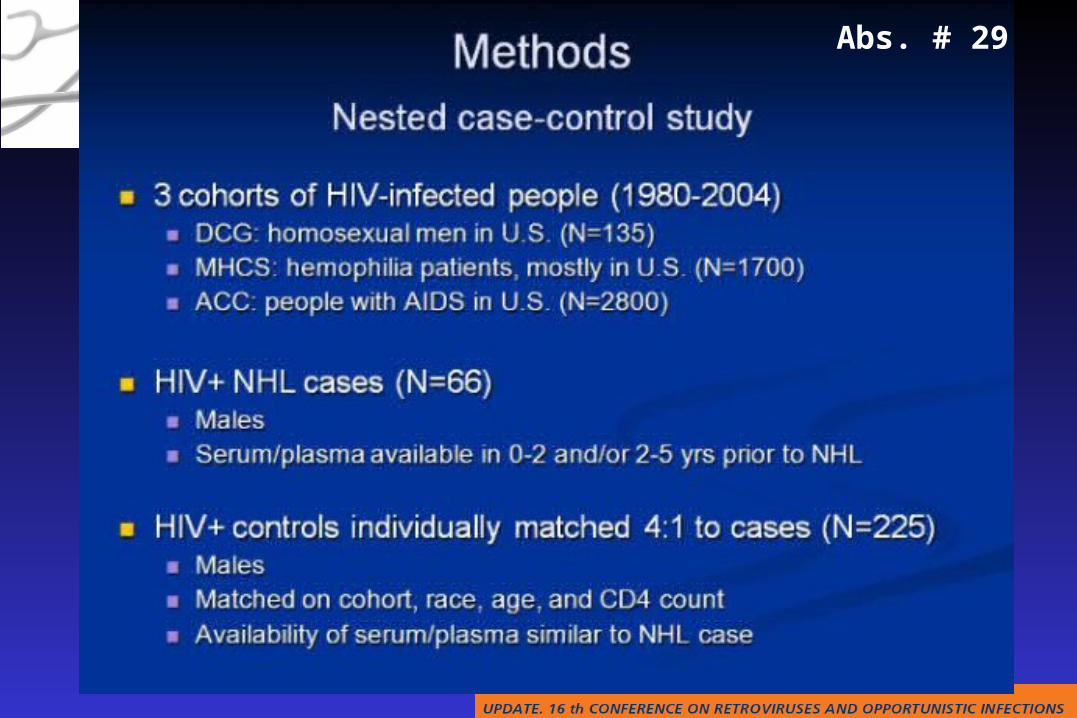
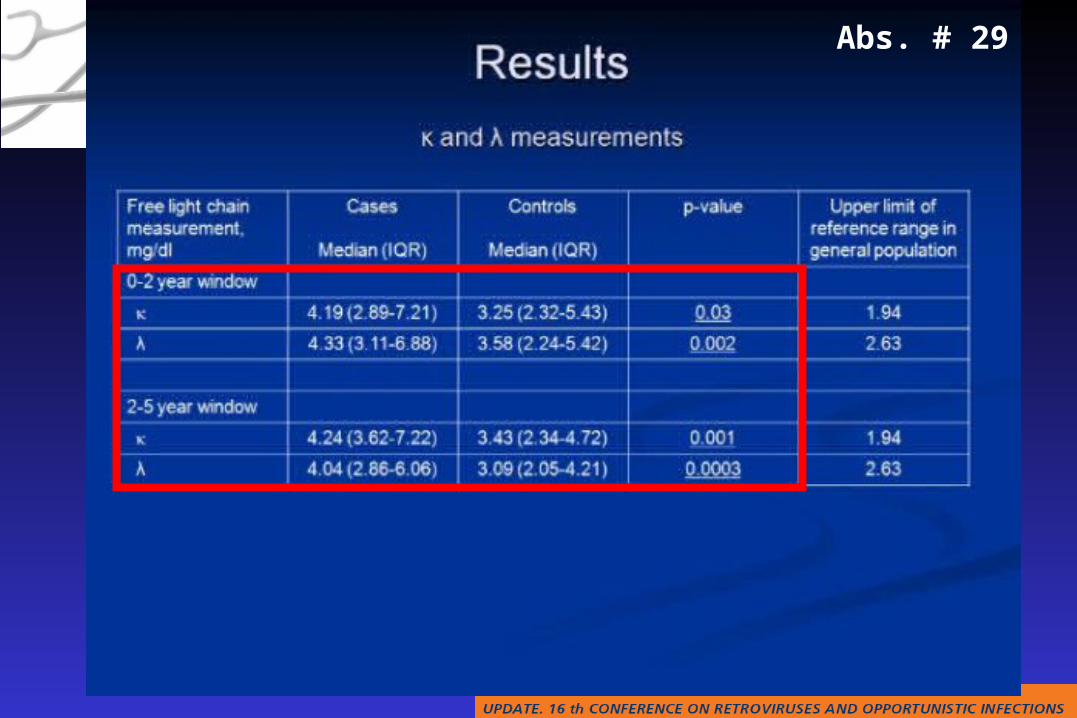
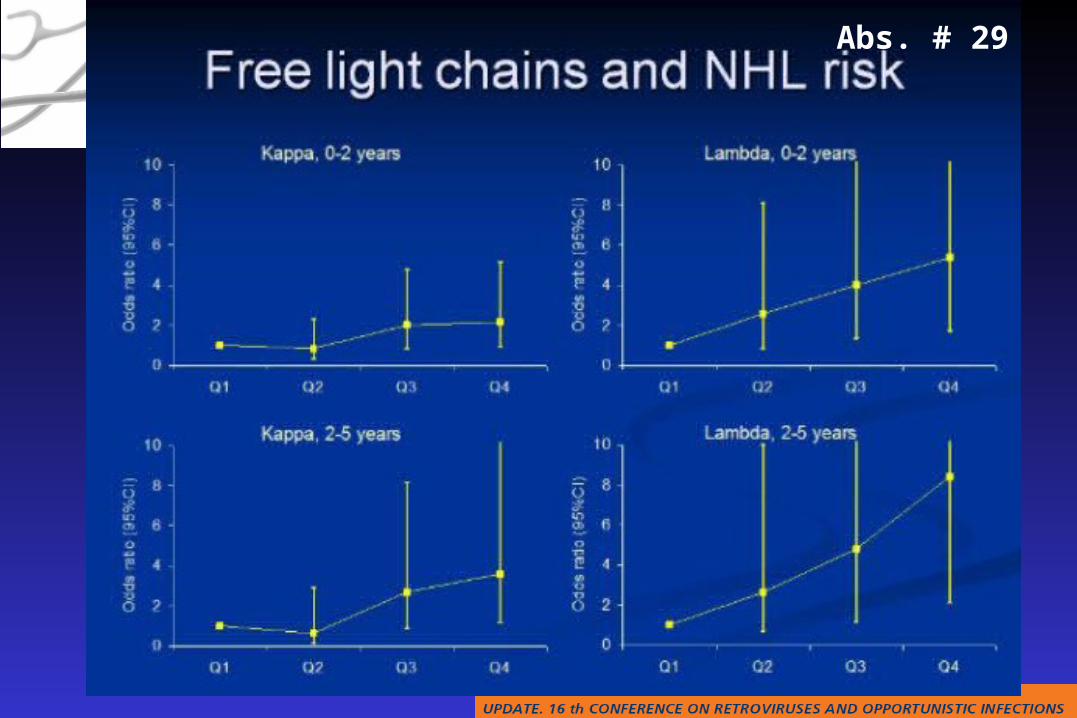
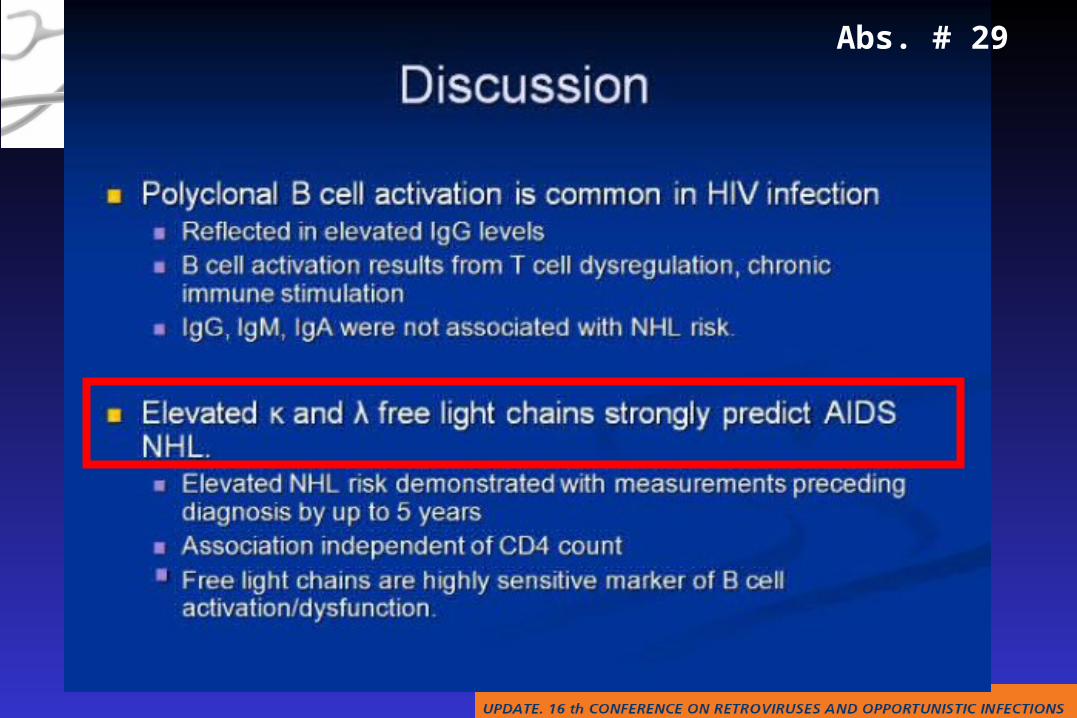
Abs. # 29
Abs. # 29
Abs. # 29
Abs. # 29
Abs. # 29
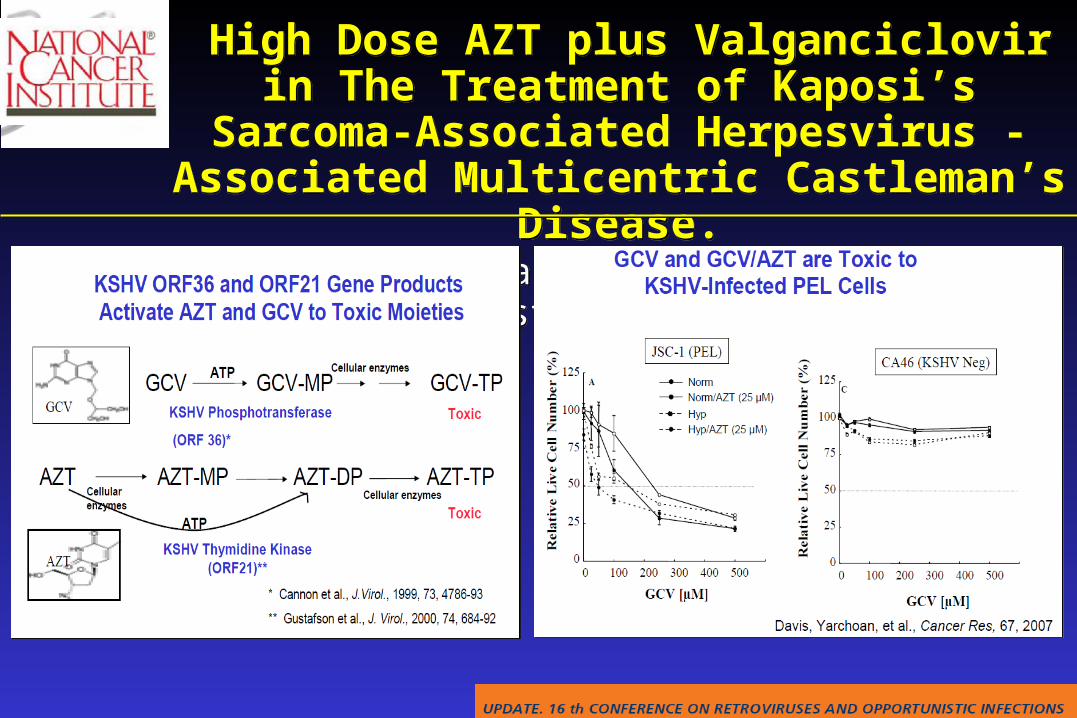
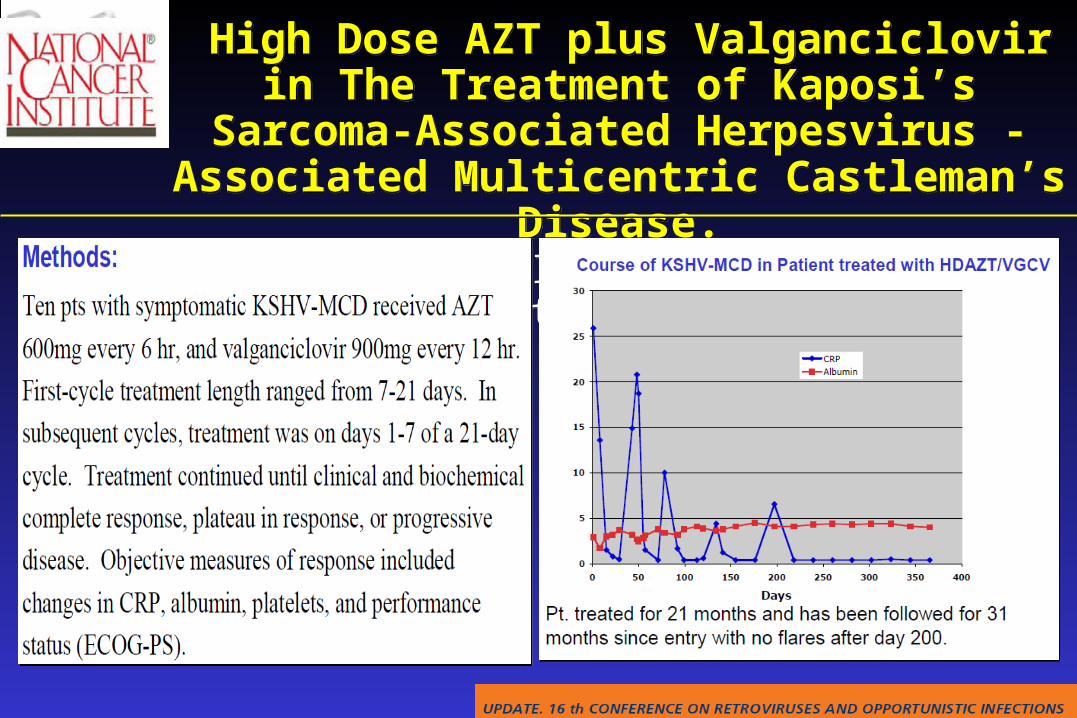
High Dose AZT plus Valganciclovir in The Treatment of Kaposi’s Sarcoma-Associated Herpesvirus -Associated Multicentric Castleman’s Disease.
Uldirch T et al. CROI 2009, Montreal; Abstracts 864.
High Dose AZT plus Valganciclovir in The Treatment of Kaposi’s Sarcoma-Associated Herpesvirus -Associated Multicentric Castleman’s Disease.
Uldirch T et al. CROI 2009, Montreal; Abstracts 864.
High Dose AZT plus Valganciclovir in The Treatment of Kaposi’s Sarcoma-Associated Herpesvirus -Associated Multicentric Castleman’s Disease.
Uldirch T et al. CROI 2009, Montreal; Abstracts 864.
High Dose AZT plus Valganciclovir in The Treatment of Kaposi’s Sarcoma-Associated Herpesvirus -Associated Multicentric Castleman’s Disease.
Uldirch T et al. CROI 2009, Montreal; Abstracts 864.
Abs. # 30
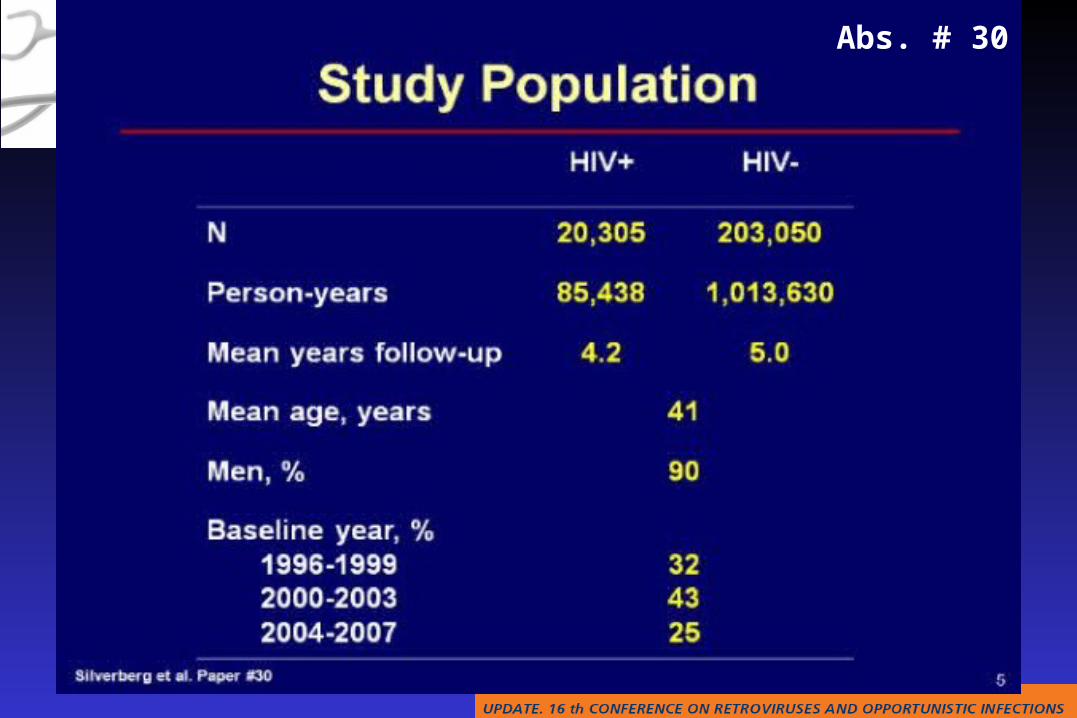
Abs. # 30
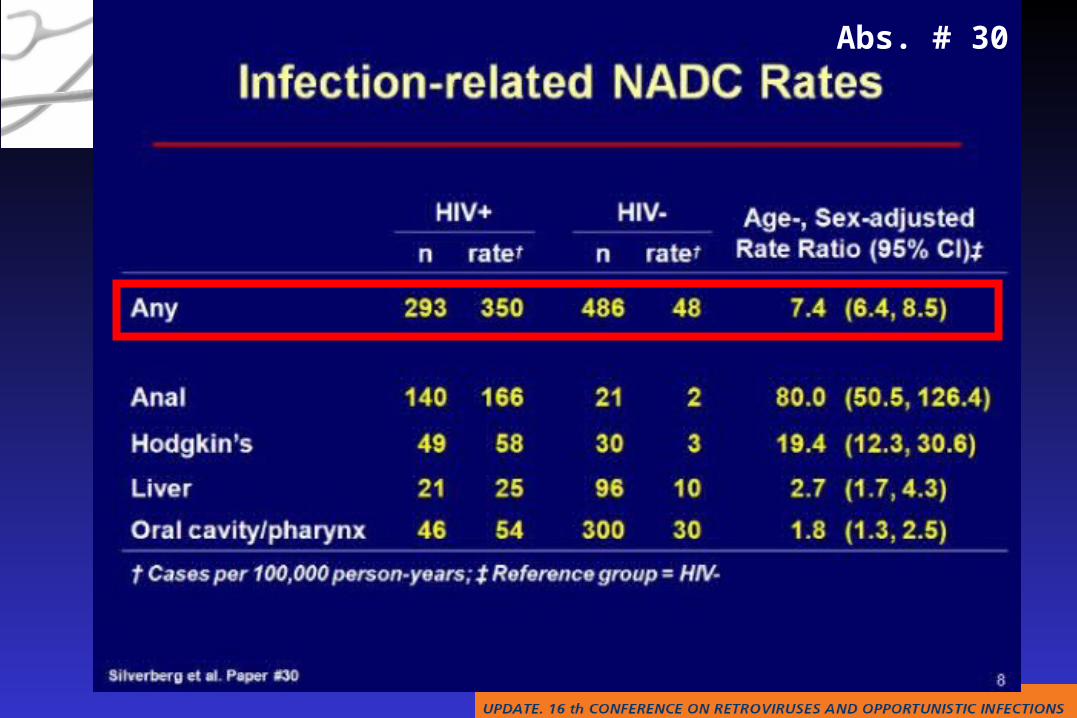
Abs. # 30
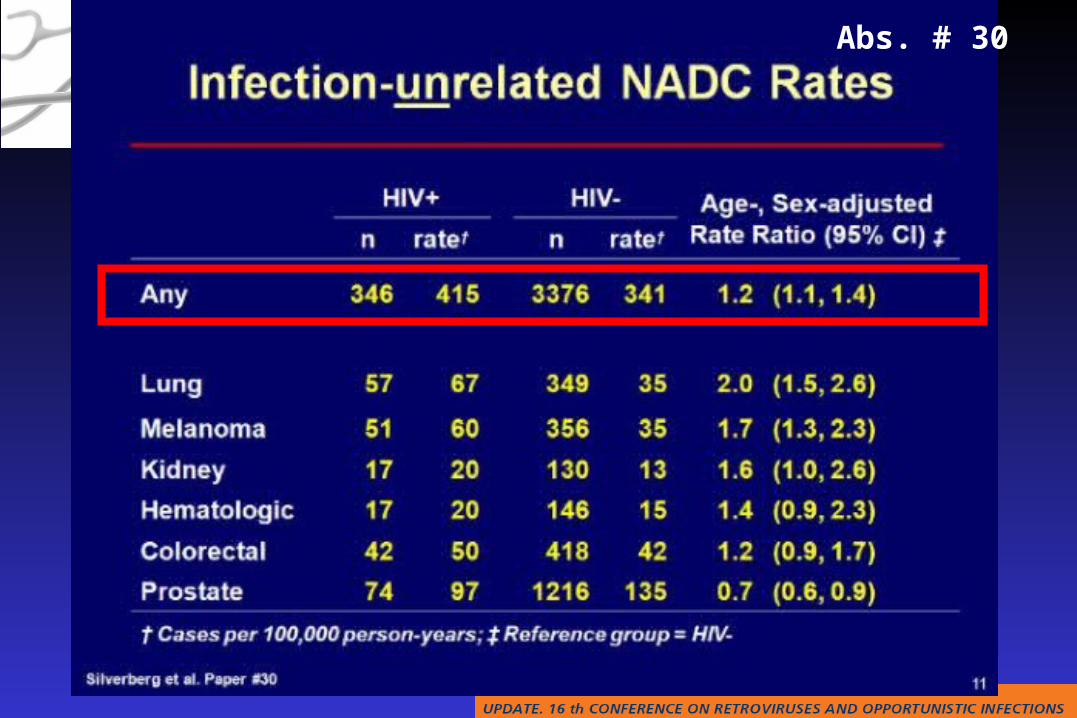
Abs. # 30
Q&A from the audience
Q&A from the audience
OIs, Hepatitis Coinfections & Tumors
OIs, Hepatitis Coinfections & Tumors