163576682 health care delivery system
TRANSCRIPT

HEALTH CARE DELIVERY SYSTEMIN INDIA AND ABROAD
Introduction
Health is the birth right of every individual. Today health is considered more than a basic
human right; it has become a matter of public concern, national priority and political action. Our
health system has traditionally been a disease-oriented system but the current trend is to emphasize
health and its promotion. The nursing profession exists to meet the health need of the people.
Unprecedented changes have occurred in the structure of our society, in lifestyles, in specific and
technological advances.
Health is a multi dimensional with physical, biological, economical, social, cultural and
vocational. Health is not static. A person who is healthy now may not be healthy the next moment.
Public has become more aware and emphasizing on health, health promotion, wellness and self care.
Emphasis has shifted from a focus on cure to a focus on prevention and health maintenance. This has
led to a evolution of a wide range of health promotion techniques, and programmes including
multiphasic screening, life time health monitoring programs.
Special efforts being made by the health care professionals to reach and motive members of
various cultural and social economic groups concerning life style and health practices. All efforts are
to design a health care system that makes comprehensive health care available to all the people at an
affordable cost.
Selected health care definitions:
• Health: According to WHO, health is defined as “a dynamic state of complete physical,
mental and social well-being not merely an absence of disease or infirmity.”
• Health care services: It is defined as “multitude of services rendered to individuals, families or
communities by the agents of the health services or professions for the purpose of promoting,
maintaining, monitoring or restoring health.”
Definitions of health care delivery:
1. Health care delivery system refers to the totality of resources that a population or society
distributes in the organisation and delivery of health population services. It also includes
all personal and public services performed by individuals or institutions for the purpose of
maintaining or restoring health.
-Stanhope(2001)

2. It implies the organisation, delivery staffing regulation and quality control.
J.C.Pak(2001)
3. Health care delivery system is the organisation by which health care is provided.
Wikipedia(2005)
4. A collection of fragmented services provided on free for service basis by numerous
organisations and providers.
Laddy Susan
Components of Health System:
• Concepts e.g. health and disease
• Ideas e.g. equity coverage, effectiveness, efficiency, impact.
• Objects e.g. hospitals, health centres, health programms
• Persons e.g. providers and consumers
Philosophy of Health Care Delivery System:
• Every one from birth to death is part of the market potential for health care services.
• The consumer of health care services is a client and not customer.
• Consumers are less informed about health services than anything else they purchase.
• Health care system is unique because it is not a competitive market.
• Restricted entry in to the health care system.
Goals/Objectives of Health Care Delivery System:
1) To improve the health status of population and the clinical outcomes of care.
2) To improve the experience of care of patients families and communities.
3) To reduce the total economic burden of care and illness.
4) To improve social justice equity in the health status of the population.
Principles of Health Care Delivery System:
1. Supports a coordinated, cohesive health-care delivery system.
2. Opposes the concept that fee-for-practice.
3. Supports the concept of prepaid group practice.
4. Supports the establishment of community based, community controlled health-care system.
5. Urges an emphasis be placed on development of primary care
6. Emphasizes on quality assurance of the care
7. Supports health care as basic human right for all people.
8. Opposes the accrual of profits by health-care-related industries.
9. Supports individuals unrestricted access to the provider, clinic or hospital.
10. Urges that in the establishment of priorities for health-care funding, resource be allocated to
maintain services for the economically deprived.
11. Supports efforts to eliminate unnecessary health care expenditures and voluntary efforts to
limit increase in health care costs.
12. Endorses to provide age old with special health maintenance.
13. Supports public and private funding.
14. Condemns health care fraud.
15. Supports the establishment of a national health care budget.
16. Supports universal health insurance.
Functions of Health Care Delivery System:
1) To provide health services.
2) To raise and pool the resources accessible to pay for health care.
3) To generate human and physical sources that makes the delivery service possible.
4) To set and enforce rules of the game and provide strategic direction for all the different
players involved.
Characters of Health Care Delivery System:
1) Orientation toward health.
2) Population perspective.
3) Intensive use of information.
4) Focus on consumer.
5) Knowledge of treatment outcome.
6) Constrained resources.
7) Coordination of resources.
8) Reconsideration of human values.
9) Expectations of accountability.
10) Growing interdependence.

1. Providers and Consumers.
A health care provider or health professional is an organization or person who delivers
proper health care in a systematic way professionally to any individual in need of health care services.
A health care provider could be a government, institution such as a hospital or laboratory physicians,
support staff, nurses, therapists, psychologists, veterinarians, dentists, pharmacists, or even a health
insurance company.Consumers are the people of the whole world.
Financing
There are generally five primary methods of funding health care systems
1. Direct or Out-of-Pocket payment.
2. General Taxation,
3. Social Health Insurance,
4. Voluntary or private health insurance, and
Health care systems models
• Purely private enterprise health care systems are comparatively rare. Where they exist, it is
usually for a comparatively well-off subpopulation in a poorer country with a poorer standard
of health care–for instance, private clinics for a small, wealthy expatriate population in an
otherwise poor country. But there are countries with a majority-private health care system
with residual public service eg medicare, medicaid.
• The other major models are public insurance systems:
o Social security health care model, where workers and their families are insured by
the State.
o Publicly funded health care model, where the residents of the country are insured by
the State.
o Social health insurance, where the whole population or most of the population is a
member of a sickness insurance company.
HEALTH CARE DELIVERY SYSTEM IN INDIA
In India it is represented by five major sectors or agencies which differ from each other by
health technology applied and by the source of fund available. These are:
I. PUBLIC HEALTH SECTOR
A. Primary Health Care
Primary health centres.
Sub- centres.
B. Hospital/Health Centres
Community health centres.
Rural health centres.
District hospitals/health centre.
Specialist hospitals.
Teaching hospitals.
C. Health Insurance Schemes
Employees State Insurance.
Central Govt. Healh Scheme.
D. Other Agencies
Defence services.
Railways.
II. PRIVATE SECTOR
A. Private hospitals, polyclinics, nursing homes and dispensaries.
B. General practitioners and clinics.
III. INDIGENOUS SYSTEMS OF MEDICINE
• Ayurveda • Sidda• Unani• Homeopathy• Naturopathy• Yoga• Unregistered practioners.•
IV. VOLUNTARY HEALTH AGENCIES
V. NATIONAL HEALTH PROGRAMMES
Model of Health Care System In India
The “inputs” are the health status or health problems of the community, they represent the
health needs and health demands of the community. Since resources are always limited to meet the
many health needs, priorities have to be set.

The “health care services” are designed to meet the health needs of the community through
the use of available knowledge and resources. The services provided should be comprehensive and
community based.
The “health care system” is intended to deliver the health care services, it constitutes the
management sector and involves organizational matters.
The “output” is the changed health status or improved health status of the community which is
expressed in terms of lives saved, deaths averted, diseases prevented etc.
ORGANISATION AND ADMINISTRAION OF HEALTH SERVICES IN INDIA AT
DIFFERENT LEVELS.
India is a union of 28 states and 7 Union territories. Under the constitution states are largely
independent in matters relating to the delivery of health care to the people. Each State, therefore , as
developed its own system of health care delivery, independent of the Central Government. Central
responsibility consists mainly of policy making, planning, guiding, assisting, evaluating and
coordinating the work of the State Health Ministries, so that no state State lags behind in health
services.
Health system in India has 3 links
1. Central level.
2. State level
3. District level
1. CENTRAL LEVEL:
Health is a State subject under the constitution of India. The health Centres are mainly with
international, national and interstate health matters. The centre is also responsible for execution of
health programmes in the centrally administered areas. It advises and helps the States on all health
matters.
Official organs of the health system at the National level consists of:
A. The ministry of Health and Family Welfare.
B. The Directorate General of Health Services.
C. The Central Council of Health and Family Welfare.
A. THE MINISTRY OF HEALTH AND FAMILY WELFARE
Functions:
The responsibilities of the central and state governments in the area of health are defined under
Article 246 of the constitution as follows.
a. Union list
1. International obligations such as International Sanitary Regulations regarding port
quarantine.
2. Administration of central institutes such as All India Institute of Hygiene and Public
Health, Kolkota, National Institute of Communicable Diseases, Delhi, National
Institute of Health and Family Welfare, Delhi.
3. Promotion of research through bodies such as the Indian Council of Medical Research.
4. Regulation and development of medical, dental, pharmaceutical and nursing education
and professionals through their respective councils.
5. Regulation of manufacture and sale of biological products and drugs, including drug
standards.
6. Undertaking census, collecting and publishing health and vital statistics data.
7. Coordination with State in their Health Programs, giving them technical and financial
assistance and procuring for them facilities from international agencies.
8. Coordination with other ministries in matters related to health.
9. Health regulations regarding labour in general and mines and oil fields in particular.
b. Concurrent List:
Both centre and States have simultaneous power of legislationin relation to subjects in
concurrent list.
1. Interstate spread of disease
2. Prevention of adulteration of foods
3. Control of drugs and poisons
4. Vital statistics
5. Labour welfare
6. Minor ports
7. Population control and family planning
8. Social and economic planning
B. THE DIRECTORATE GENERAL OF HEALTH SERVICES
The main functions of the DGHS

1. Conducting various national health programs.
2. Organising health services in the form of central government health scheme
3. Providing Medical Education through the colleges and institutions under its control e.g
Raj Kumari Amrit Kaur College of Nursing, Delhi, All India Institute of Hygiene and
Public Health, Kolkota, JPMER, Pondicheri etc.
4. Medical research through Indian Council of Medical Research and the institutes under it,
as also other institutions, such as the Central Research Institute, Kasauli.
5. International health and quarantile at major ports and international airports.
6. Drug control
7. Medical stores and supplies
8. Health education through Central Health Education Bureau.
9. Health intelligence, through Central Health Intelligence Bureau.
C. THE CENTRAL COUNCIL OF HEALTH AND FAMILY WELFARE
Functions of Central Council of Health and Family Welfare
1. To consider and recommend broad outlines of policy in regard to matters concerning
health in all its aspects such as the provision of remedial and preventive care,
environmental hygiene, nutrition, health education and the promotion of facilities for
training and research.
2. To make proposals for legislation in fields of activity relating to medical and public health
matters and to lay down patterns of development for the country as a whole.
3. To make recommendations to the Central Government regarding distribution of available
grants-in-aid for health purposes to the states and to review periodically the work
accomplished in different areas through the utilization of these grants-in-aid.
4. To establish any organisation or organisations invested with appropriate functions for
promoting and maintaining cooperation between the Central and State Health
administrations.
2. STATE LEVEL
There are 28 states in the country. Health, as states earlier is a State subject. Therefore,
the pattern of organisation, state of integration, level of health services, public health laws and
scales of pay differ from state to state. The aim, however of all states and their Public Health
Administration is the same- health, happiness and longevity for all the people.
A. State Ministry of Health

The ministry has a minister and deputy minister of health. The secretary and Joint secretary,
etc. held by the IAS cadre.
B. State Health Directorate
The process of integration has now been completed in most States. The usual pattern now is
that the State Health Directorate is headed by a Director, usually known as Director of health
services, He is assisted by a suitable number of deputies to look after various health and
medical health services. Some states also have a separate Director Medical Education.
C. District Level:
Each state in Indian union is divided into districts. Total population in each district, urban as
well as rural, varies from one to three million. Just as in case of states, some autonomy has been
given to urban and rural areas in the district as well. The autonomous bodies or local self government
are called Corporation and Muncipal Committees in the cities, Zilla panchayats or Zilla Parishads in
rural districts, Taluka Panchayat or Taluka Parishats in taluka level and Grama panchayat and Nagara
Panchayats in villages and small towns.
Health organisations in Urban Areas:
There are three types of self-gevernment in urban areas of district, depending upon the size of
population:
1. Town areas committees (5000-100000)
2. Muncipal board or Muncipality (10- 2000000)
3. Corporation (Above 200000)
Town areas committees: Its functions primarily limited to provision of sanitary services.
Muncipal board or Muncipality: Its functions are more diverse. These include regulation regarding
construction of houses, latrines and urinals, hotels, and markets; provision of water supply, drainage
and disposal of refuse and excreta, disposal of the dead, registration of births and deaths, keeping of
dogs and control of communicable diseases.
Corporation: Corporation provides essentially the same services as the muncilapity, but on a larger
scale. It also maintains hospitals and dispensaries.
Health organisation in Rural areas:

Under panchayat act 1961, the district administration was reorganised in to 3 levels, self
governing autonomous bodies were formed at different levels as follows:
1. For each villages or group of villages with population from 1000 to 10000 there is a Gram
panchayat. If the population os over 10,000 to 30,000 there is a Nagar Panchayat. The gram
panchayat in constituted by 15-30 elected members, who in turn elect a Sarpanch or president,
Vice president, and panchayat secretary is recruited by government.
2. For each block: There is a Panchayat samiti or taluka panchayat which is a elected body.
3. For each district: there is a zilla panchayat or parishat which is an autonomous body for
district as well as a whole, responsible to the state assembly. It is constituted by elected
members, MLAs, MPs.
In all above provision has been made for reservation for schedule caste schedule tribes and
women to ensure their active participation in all round development of the village.
Primary Health Care In India
• In 1977 government of India launched a rural health scheme, based on the principles of
“Placing people’s health in people’s hands’
• As a signatory to Alma-Ata Declaration, the government of India is committed to
achieving the goal of Health care approach which seeks to provide universal health care at
a cost which is affordable.
• Keeping in view the WHO goal of “Health for All” by 2000 AD, the government of India
evolved a National Health Policy in 1983.
• Keeping in view the Millennium Developmental Goals, the government of India revised
the draft of National Health Policy in 2001.
Principles of primary Health Care
1. Equitable distribution
2. Community participation
3. Intersectoral coordination
4. Appropriate technology
5. Preventive in Nature
6. Man power development.
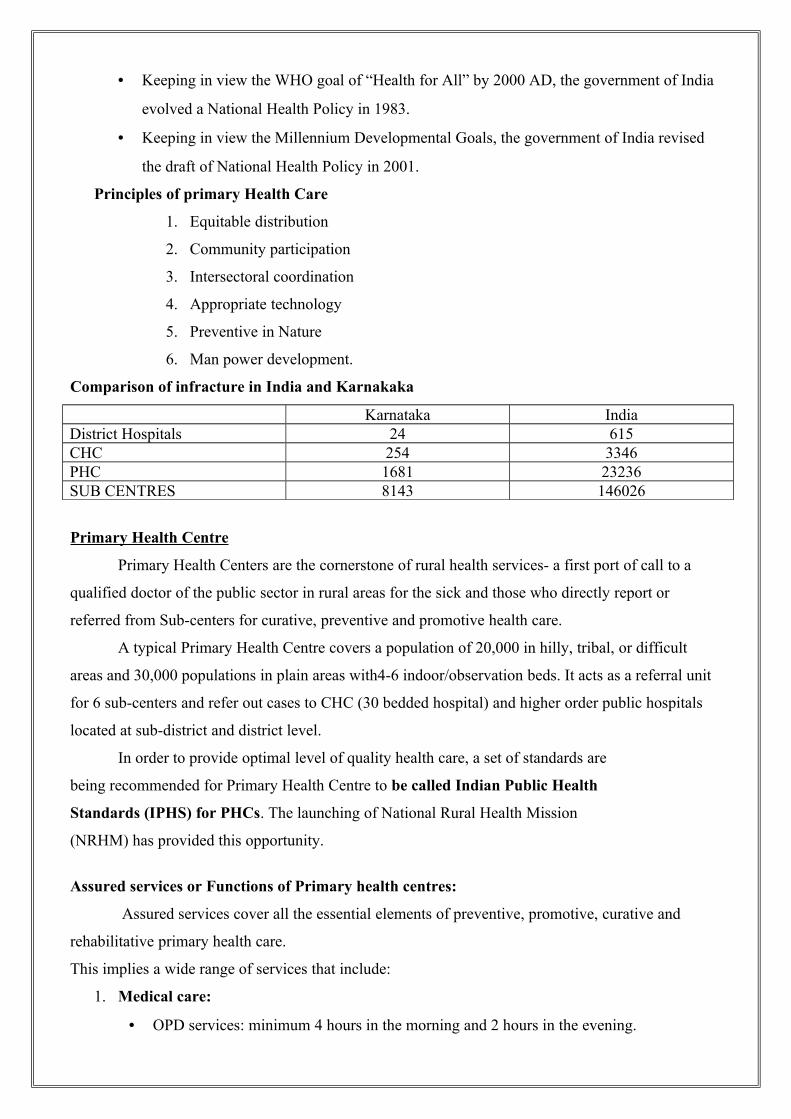
Comparison of infracture in India and Karnakaka
Karnataka IndiaDistrict Hospitals 24 615CHC 254 3346PHC 1681 23236SUB CENTRES 8143 146026
Primary Health Centre
Primary Health Centers are the cornerstone of rural health services- a first port of call to a
qualified doctor of the public sector in rural areas for the sick and those who directly report or
referred from Sub-centers for curative, preventive and promotive health care.
A typical Primary Health Centre covers a population of 20,000 in hilly, tribal, or difficult
areas and 30,000 populations in plain areas with4-6 indoor/observation beds. It acts as a referral unit
for 6 sub-centers and refer out cases to CHC (30 bedded hospital) and higher order public hospitals
located at sub-district and district level.
In order to provide optimal level of quality health care, a set of standards are
being recommended for Primary Health Centre to be called Indian Public Health
Standards (IPHS) for PHCs. The launching of National Rural Health Mission
(NRHM) has provided this opportunity.
Assured services or Functions of Primary health centres:
Assured services cover all the essential elements of preventive, promotive, curative and
rehabilitative primary health care.
This implies a wide range of services that include:
1. Medical care:
• OPD services: minimum 4 hours in the morning and 2 hours in the evening.

• 24 hours emergency services
• Referral services
• In-patient services (6 beds)
2. Maternal and Child Health Care including family planning:
• Antenatal care: Early diagnosis, minimum three antenatal check up, identification and
management of high risk pregnancies, nutrition and health counseling, minimum
laboratory investigation urin albumin, test ofr syphilis, chemoprophylaxis for malaria in
high endemic area as per NVDCP.
• Intra-natal care. (24-hour delivery services both normal and assisted)
• Postnatal Care.( Janani Suraksha Yojana (JSY)) Minimum 2 postpartum visit, initiation of
breast feeding health education on hygiene, contraception etc,
• New Born care.
• Care of The Child.
• Family Planning
3. Medical Termination of Pregnancies using Manual Vacuum Aspiration
(MVA) technique. (Wherever trained personnel and facility exists)
4. Management of Reproductive Tract Infections / Sexually Transmitted
Infections:
5. Nutrition Services (coordinated with ICDS)
6. School Health
7. Adolescent Health Care
8. Promotion of Safe Drinking Water and Basic Sanitation
9. Prevention and control of locally endemic diseases like malaria, Kalaazar,
Japanese Encephalitis, etc
10. Disease Surveillance and Control of Epidemics
11. Collection and reporting of vital events
12. Education about health/Behaviour Change Communication (BCC)
13. National Health Programmes including Reproductive and Child HealthProgramme (RCH),
HIV/AIDS control programme, Non communicable
disease control programme etc
14. Referral Services.
15. Training: ASHA, ANM, LHV
16. Basic Laboratory Services
17. Monitoring and Supervision:

18. AYUSH services as per local people’s preference (Mainstreaming of AYUSH)
19. Rehabilitation
20. Selected Surgical Procedures
Man Power in PHCEXISTING RECOMMENDED
Medical Officer 1 2(one may be from AYUSH or lady medical officer)
Pharmascist 1 1Nurse-midwife (staff nurse) 1 3Health worker(F) 1 1Health Educator 1 1Health assistant(M & F)(LHV and Health Assistant Male)
2 2
Clercks 2 2Laboratory Technician 1 1Driver 1 1Class IV 4 4
SUBCENTRE
In the public sector, a Sub-health Centre is the most peripheral and first contact point between
the primary health care system and the community. As per the population norms, one Sub-centre is
established for every 5000 population in plain areas and for every 3000 population in
hilly/tribal/desert areas. A Sub-centre provides interface with the community at the grass-root level,
providing all the primary health care services. As sub- centres are the first contact point with the
community, the success of any nation wide programme would depend largely on well functioning
sub-centres providing services of acceptable standard to the people. The current level of functioning
of the Subcentres are much below the expectations.
There is a felt need for quality management and quality assurance in health care delivery
system so as to make the same more effective, economical and accountable. No concerted effort has
been made so far to prepare comprehensive standards for the Sub-centres. The launching of NRHM
has provided the opportunity for framing Indian Public Health Standards.
Objectives of Sub-centres:
i. To provide basic Primary health care to the community.
ii. To achieve and maintain an acceptable standard of quality of care.
iii. To make the services more responsive and sensitive to the needs of the community.
Assured services or Functions of Primary health centers:
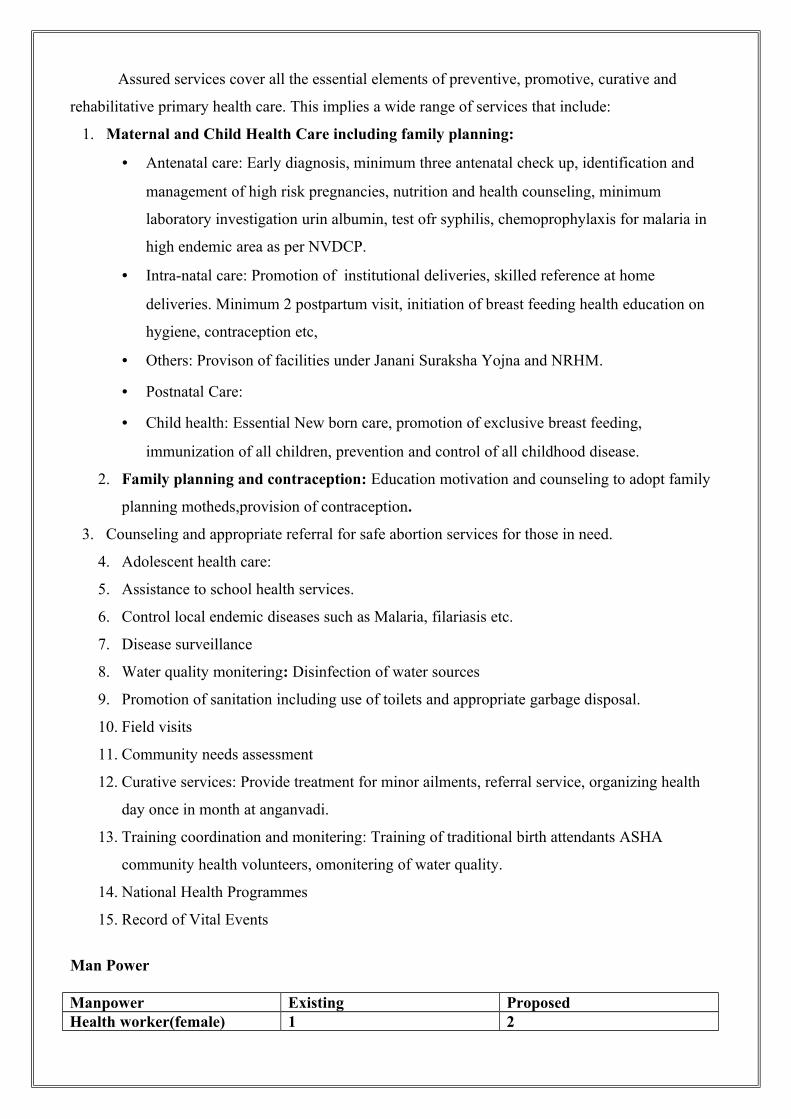
Assured services cover all the essential elements of preventive, promotive, curative and
rehabilitative primary health care. This implies a wide range of services that include:
1. Maternal and Child Health Care including family planning:
• Antenatal care: Early diagnosis, minimum three antenatal check up, identification and
management of high risk pregnancies, nutrition and health counseling, minimum
laboratory investigation urin albumin, test ofr syphilis, chemoprophylaxis for malaria in
high endemic area as per NVDCP.
• Intra-natal care: Promotion of institutional deliveries, skilled reference at home
deliveries. Minimum 2 postpartum visit, initiation of breast feeding health education on
hygiene, contraception etc,
• Others: Provison of facilities under Janani Suraksha Yojna and NRHM.
• Postnatal Care:
• Child health: Essential New born care, promotion of exclusive breast feeding,
immunization of all children, prevention and control of all childhood disease.
2. Family planning and contraception: Education motivation and counseling to adopt family
planning motheds,provision of contraception.
3. Counseling and appropriate referral for safe abortion services for those in need.
4. Adolescent health care:
5. Assistance to school health services.
6. Control local endemic diseases such as Malaria, filariasis etc.
7. Disease surveillance
8. Water quality monitering: Disinfection of water sources
9. Promotion of sanitation including use of toilets and appropriate garbage disposal.
10. Field visits
11. Community needs assessment
12. Curative services: Provide treatment for minor ailments, referral service, organizing health
day once in month at anganvadi.
13. Training coordination and monitering: Training of traditional birth attendants ASHA
community health volunteers, omonitering of water quality.
14. National Health Programmes
15. Record of Vital Events
Man Power
Manpower Existing ProposedHealth worker(female) 1 2
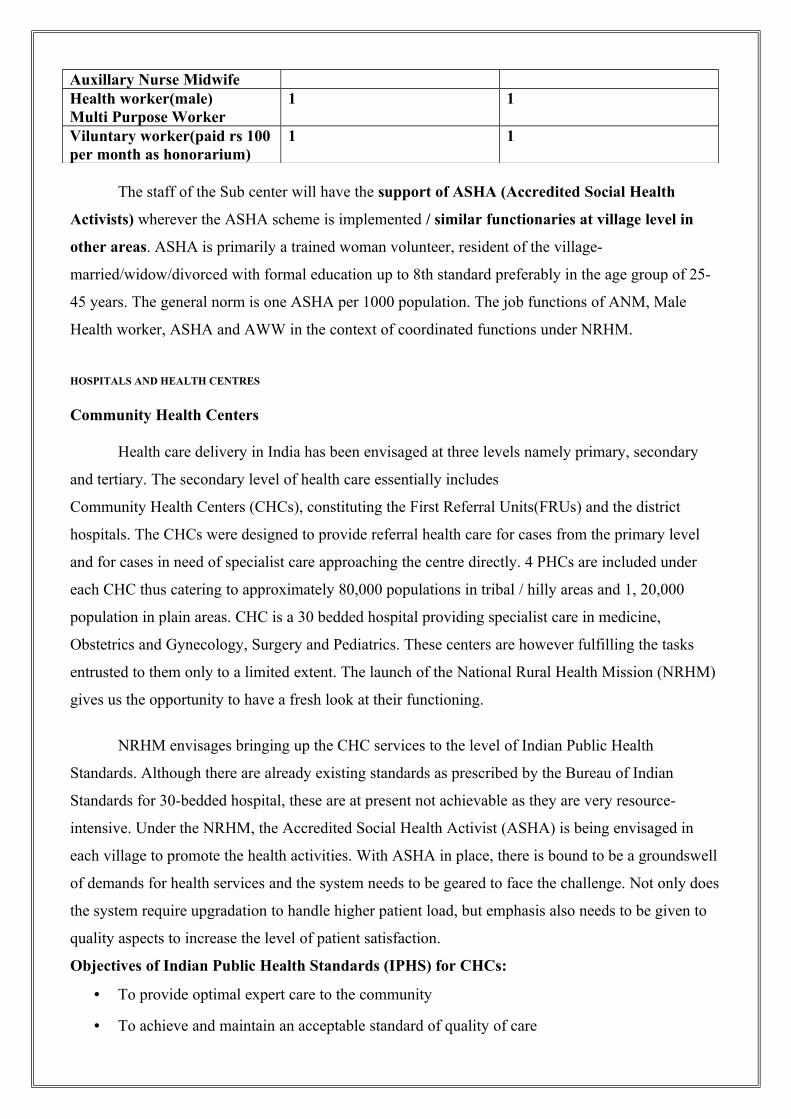
Auxillary Nurse MidwifeHealth worker(male)Multi Purpose Worker
1 1
Viluntary worker(paid rs 100 per month as honorarium)
1 1
The staff of the Sub center will have the support of ASHA (Accredited Social Health
Activists) wherever the ASHA scheme is implemented / similar functionaries at village level in
other areas. ASHA is primarily a trained woman volunteer, resident of the village-
married/widow/divorced with formal education up to 8th standard preferably in the age group of 25-
45 years. The general norm is one ASHA per 1000 population. The job functions of ANM, Male
Health worker, ASHA and AWW in the context of coordinated functions under NRHM.
HOSPITALS AND HEALTH CENTRES
Community Health Centers
Health care delivery in India has been envisaged at three levels namely primary, secondary
and tertiary. The secondary level of health care essentially includes
Community Health Centers (CHCs), constituting the First Referral Units(FRUs) and the district
hospitals. The CHCs were designed to provide referral health care for cases from the primary level
and for cases in need of specialist care approaching the centre directly. 4 PHCs are included under
each CHC thus catering to approximately 80,000 populations in tribal / hilly areas and 1, 20,000
population in plain areas. CHC is a 30 bedded hospital providing specialist care in medicine,
Obstetrics and Gynecology, Surgery and Pediatrics. These centers are however fulfilling the tasks
entrusted to them only to a limited extent. The launch of the National Rural Health Mission (NRHM)
gives us the opportunity to have a fresh look at their functioning.
NRHM envisages bringing up the CHC services to the level of Indian Public Health
Standards. Although there are already existing standards as prescribed by the Bureau of Indian
Standards for 30-bedded hospital, these are at present not achievable as they are very resource-
intensive. Under the NRHM, the Accredited Social Health Activist (ASHA) is being envisaged in
each village to promote the health activities. With ASHA in place, there is bound to be a groundswell
of demands for health services and the system needs to be geared to face the challenge. Not only does
the system require upgradation to handle higher patient load, but emphasis also needs to be given to
quality aspects to increase the level of patient satisfaction.
Objectives of Indian Public Health Standards (IPHS) for CHCs:
• To provide optimal expert care to the community
• To achieve and maintain an acceptable standard of quality of care
• To make the services more responsive and sensitive to the needs of the community.
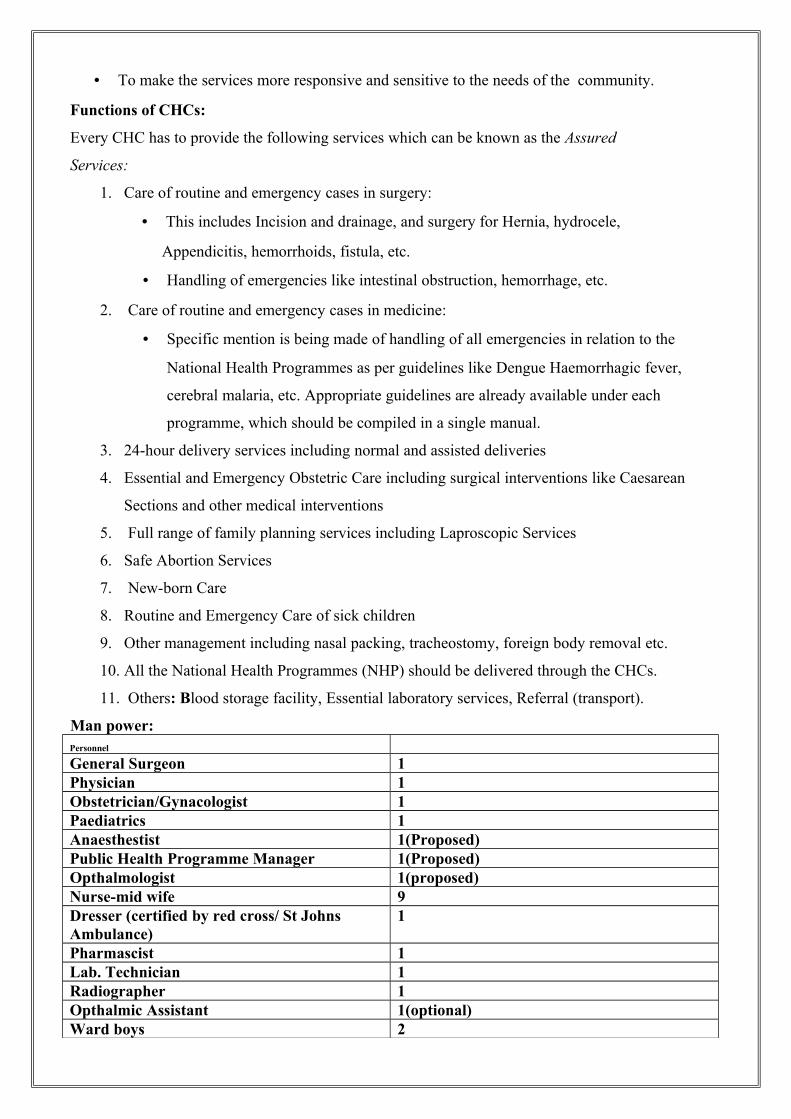
Functions of CHCs:
Every CHC has to provide the following services which can be known as the Assured
Services:
1. Care of routine and emergency cases in surgery:
• This includes Incision and drainage, and surgery for Hernia, hydrocele,
Appendicitis, hemorrhoids, fistula, etc.
• Handling of emergencies like intestinal obstruction, hemorrhage, etc.
2. Care of routine and emergency cases in medicine:
• Specific mention is being made of handling of all emergencies in relation to the
National Health Programmes as per guidelines like Dengue Haemorrhagic fever,
cerebral malaria, etc. Appropriate guidelines are already available under each
programme, which should be compiled in a single manual.
3. 24-hour delivery services including normal and assisted deliveries
4. Essential and Emergency Obstetric Care including surgical interventions like Caesarean
Sections and other medical interventions
5. Full range of family planning services including Laproscopic Services
6. Safe Abortion Services
7. New-born Care
8. Routine and Emergency Care of sick children
9. Other management including nasal packing, tracheostomy, foreign body removal etc.
10. All the National Health Programmes (NHP) should be delivered through the CHCs.
11. Others: Blood storage facility, Essential laboratory services, Referral (transport).
Man power:Personnel
General Surgeon 1Physician 1Obstetrician/Gynacologist 1Paediatrics 1Anaesthestist 1(Proposed)Public Health Programme Manager 1(Proposed)Opthalmologist 1(proposed)Nurse-mid wife 9Dresser (certified by red cross/ St Johns Ambulance)
1
Pharmascist 1Lab. Technician 1Radiographer 1Opthalmic Assistant 1(optional)Ward boys 2

Sweepers 3
Chowkidar 1OPD attendant 1Statical Assistant/Data entry operator 1OT attendant 1Registration Clerk 1
HOSPITALS
India’s Public Health System has been developed over the years as a 3-tier system, namely
primary, secondary and tertiary level of health care. District Health System is the fundamental basis
for implementing various health policies and delivery of healthcare, management of health services
for defined geographic area. District hospital is an essential component of the District health system
and functions as a secondary level of health care, which provides curative, preventive and promotive
healthcare services to the people in the district.
Every district is expected to have a district hospital linked with the public hospital/health
centres down below the district such as Sub-district/Sub-divisional hospitals, Community Health
Centres, Primary Health Centers and Sub-centres. As per the information available, 609 districts in
the country at present are having about 615 District hospitals. However, some of the medical college
hospitals or a sub-divisional hospital is found to serve as a district hospital where a district hospital as
such (particularly the newly created district) has not been established. Few districts have also more
than one district hospital.
Objectives for district hospitals:
The overall objective of IPHS is to provide health care that is quality oriented and sensitive to the
needs of the people of the District. The specific objectives of IPHS for DHs are:
i. To provide comprehensive secondary health care (specialist and referral services) to
the community through the District Hospital.
ii. To achieve and maintain an acceptable standard of quality of care.
iii. To make the services more responsive and sensitive to the needs of the people of the
district and the hospitals/centres from which the cases are referred to the district
hospitals
Definition

The term District Hospital is used here to mean a hospital at the secondary referral level
responsible for a District of a defined geographical area containing a defined population.
Grading of district hospitals:
The size of a district hospital is a function of the hospital bed requirement, which in turn is a
function of the size of the population it serves. In India the population size of a district varies from
35,000 to 30,00,000 (Census 2001). Based on the assumptions of the annual rate of admission as 1
per 50 populations and average length of stay in a hospital as 5 days, the number of beds required for
a district having a population of 10 lakhs will be around 300 beds. However, as the population of the
district varies a lot, it would be prudent to prescribe norms by grading the size of the hospital as per
the number of beds.
Grade I: District hospitals norms for 500 beds
Grade II: District hospitals norms for 300 beds
Grade III: District hospitals norms for 200 beds
Grade IV: District hospitals norms for 100 beds
The disease prevalence in a district varies widely in type and complexities. It is not possible
to treat all of them at district hospitals. Some may require the intervention of highly specialist
services and use of sophisticated expensive medical equipments. Patients with such diseases can be
transferred to tertiary and other specialized hospitals. A district hospital should however be able to
serve 85-95% of the medical needs in the districts. It is expected that the hospital bed occupancy rate
should be at least 80%. Functions
1. It provides effective, affordable healthcare services (curative including specialist services,
preventive and promotive) for a defined population, with their full participation and in co-
operation with agencies in the district that have similar concern. It covers both urban
population (district headquarter town) and the rural population in the district.
2. Function as a secondary level referral centre for the public health institutions below the
district level such as Sub-divisional Hospitals, Community Health Centres, Primary Health
Centres and Sub-centres.
3. To provide wide ranging technical and administrative support and education and training for
primary health care.
Essential Services
Services include OPD, indoor, emergency services.
Secondary level health care services regarding following specialties will be assured at hospital:
Consultation services with following specialists:
General Medicine
General Surgery
Obg & Gyne
Paediatrics including Neonatology
Emergency (Accident & other emergency) (Casualty)
Critical care (ICU)
Anaesthesia
Ophthalmology
ENT
Orthopaedics
Radiology
Dental care
Public Health Management
Para clinical services
• Laboratory Services
• X-Ray Facility
• ECG
• Blood transfusion and storage facilities
• Physiotherapy
• Dental Technology (Dental Hygiene)
• Drugs and Pharmacy
Support Services
Medico-legal/post-mortem
Ambulance services
Dietary services
Security services.
Waste management
Ware housing/central store
Maintenance and repair
Electric Supply (power generation and stabilization)
Water supply (plumbing)
Heating, ventilation and air-conditioning
Transport
Communication
Medical Social Work
Nursing Services
Sterilization and Disinfection
HEALTH INSURANCE:
There is no universal health insurance in India. Health Insurance is at present is limited to
industrial workers and their families.
1. Employees State Insurance Scheme
It was introduced by an act of parliament in 1948. It covers employees
drawing wages not exceeding Rs. 10,000 per month.
The act provides
o Medical benefits
o Sickness benefits
o Disabled benefits
o Maternity benefits
o Dependent benefits
o Funeral benefits
2. Central Government Health Scheme:
This scheme was introduced in New Delhi in 1954 to provide comprehensive medical care to
Central Government employees. The schemes based on the principles of cooperative effort by
the employee and the mutual advantage of both.
Facilities under the scheme include:
o Outpatient care through a network of dispensaries.
o Supply of necessary drugs.
o Laboratory and x-ray investigation.
o Domiciliary visits.
o Hospitalisation facilities at Govt as well as private hospitals recognized for the
purpose.
o Special consultation.
o Paediatric services including immunization.
o Antenatal, natal and postnatal services.
o Emergency treatment.
o Supply of optical and dental aids at reasonable rate.
OTHER AGENCIES:
Defence Medical Services:
Defence services have their own organization for medical care to defence personnel under the
banner “Armed Forces Medical Services”. The services are provided are integrated and
comprehensive.
Health Care of Railway Employees: The Railways provide comprehensive health care services
through the agencies of Railway Hospitals, Health Units and Clinics. Environmental sanitation is
taken care of by Health Inspectors in big stations. Health check-up of employees is provided at the
time of recruitment and thereafter at yearly intervals.
PRIVATE AGENCIES:
In a mixed economy such as India’s, private practice of medicine provides a large share of the
health services available. There has been a rapid expansion in the number of qualified allopathic
physicians to 7.5 lakhs in 2005 and doctor population ration is 1:1428. Most of them they concentrate
in urban areas. They provide mainly curative services. Their services are available to those who can
pay. The private sector of health care services is not organised.
INDEGINOUS SYATEMS OF MEDICINE:
The practioners of indigenous system of medicine provide the bulk of medical care to the rural
people. Ayurvedic physicians alone are estimated to be about 4.5lakhs. Nearly 90% of ayurvedic
physicians serve the rural areas. To promote this these indigenous systems Indian government
established Indian Council For Indian Medicine in 1971. AYUSH is the new approach on this. Which
encompasses Ayurveda, Yoga, Unani, Sidda, Homeopathy.
Objectives of AYUSH:
o To upgrade the educational standards in the Indian Systems of Medicines and Homoeopathy
colleges in the country.
o To strengthen existing research institutions and ensure a time-bound research programme on
identified diseases for which these systems have an effective treatment.
o To draw up schemes for promotion, cultivation and regeneration of medicinal plants used in
these systems.
o To evolve Pharmacopoeial standards for Indian Systems of Medicine and Homoeopathy
drugs.
Voluntary Health Agencies:
A voluntary health agency may be defined as an organization that is administered by an
autonomous board which holds meetings, collects funds for its support, chiefly from private sources
and expands money, whether with or without paid workers, in conducting a programme directed
primarily to furthering the public health by providing health services or health education by
advancing research or legislation for health or by a combination of these activities.
The voluntary health agencies in India are:
o Indian Red Cross Society
o Hind Kusht Nivaran Sangh
o Indian Council for Child Welfare
o Tuberculosis Association of India
o Bharat Sevak Samaj
o Central Social Welfare Board
o The Ksturba Memorial Fund
o Family Planning Association of India
o All India Women’s Conference
o The All- India Blind Relief Society
o Professional Bodies like TNAI, IMA, AIDA etc
o International Agencies like Rockfeller Foundation, CARE, Ford Foundation etc.
NATIONAL HEALTH PROGRAMMES
Since India became free, several measures have been undertaken by National Government to
improve the health of the people. Prominent among these measures are the National Health
Programmes. Which have been launched by the Central Government for control/eradication of the
communicable diseases, improvement of environmental sanitation, raising the standard of nutrition,
control of population and improving rural health. Various international agencies like WHO, UNICEF,
UNFPA etc have been providing technical and material assistance in the implementation of these
programmes.
National Health Programmes are:
• National Vector Borne Disease Control Programme
• National Leprosy Eradication Programme
• Revised National Tuberculosis Control Programme

• National AIDS Control Programme
• National Programme for Control of Blindness
• Iodine Deficiency Disorders Programme
• Universal Immunization Programme
• National Rural Health Mission
• Reproductive and Child Health Programme
• Yaws Eradication Programme
• National Cancer Control Programme
• National Guinea- Worm Eradication Programme
• National Cancer Control Programme
• National Mental Health Programme
• National Diabetes Control Programme
• National Programme for Control and Treatment of Occupational Disease
• Nutritional Programme
• National Surveillance Programme for Communicable Disease
• Integrated Disease Surveillance Programme
• National Family Welfare Programme
• National Water Supply and Sanitation Programme
• Minimum Needs Programme
• 20-Point Programme
Need For an Alternatenative Health Systems of Health Care:
1. The present system is limited to the urban areas.
2. It has greater emphasis on curative aspects rather than preventive and promotive
aspects care.
3. It is expensive.
4. Inadequacy and misdistribution of resources for health services
5. There is lack of clear-cut referral system.
6. There is lack of intersectoral collaboration and community involvement.
7. Over centralization of authority.

8. There is insufficient orientation and training of the primary health care staff and there
is also lack of proper job descriptions resulting in poor implementation of the
projects.
9. The unsuitable working hours of the personnel in the rural areas.
NATIONAL RURAL HEALTH MISSION
The National Rural Health Mission (NRHM) has been launched with a view to bringing about
dramatic improvement in the health system and the health status of the people, especially those who
live in the rural areas of the country. The Mission seeks to provide universal access to equitable,
affordable and quality health care which is accountable at the same time responsive to the needs of
the people, reduction of child and maternal deaths as well as population stabilization, gender and
demographic balance. In this process, the Mission would help achieve goals set under the National
Health Policy and the Millennium Development Goals.
To achieve these goals NRHM will:
• Facilitate increased access and utilization of quality health services by all.
• Forge a partnership between the Central, state and the local governments.
• Set up a platform for involving the Panchayati Raj institutions and community in the
management of primary health programmes and infrastructure.
• Provide an opportunity for promoting equity and social justice.
• Establish a mechanism to provide flexibility to the states and the community to
promote local initiatives.
• Develop a framework for promoting inter-sectoral convergence for promotive and preventive
health care.
The Vision of the Mission
• To provide effective healthcare to rural population throughout the country with
special focus on 18 states, which have weak public health indicators and/or
weak infrastructure.
• 18 special focus states are Arunachal Pradesh, Assam, Bihar, Chattisgarh,
Himachal Pradesh, Jharkhand, Jammu and Kashmir, Manipur , Mizoram,
Meghalaya, Madhya Pradesh, Nagaland, Orissa , Rajasthan, Sikkim, Tripura,
Uttaranchal and Uttar Pradesh.
• To raise public spending on health from 0.9% GDP to 2-3% of GDP, with
improved arrangement for community financing and risk pooling.
• To undertake architectural correction of the health system to enable it to
effectively handle increased allocations and promote policies that strengthen
public health management and service delivery in the country.
• To revitalize local health traditions and mainstream AYUSH into the public health system.
• Effective integration of health concerns through decentralized management at district, with
determinants of health like sanitation and hygiene, nutrition, safe drinking water, gender and
social concerns.
• Address inter State and inter district disparities.
• Time bound goals and report publicly on progress.
• To improve access to rural people, especially poor women and children to equitable,
affordable, accountable and effective primary health care.
The Objectives of the Mission
• Reduction in child and maternal mortality.
• Universal access to public services for food and nutrition, sanitation and hygiene and
universal access to public health care services with emphasis on services addressing women’s
and children’s health and universal immunization.
• Prevention and control of communicable and non-communicable diseases, including locally
endemic diseases.
• Access to integrated comprehensive primary health care.
• Population stabilization, gender and demographic balance.
• Revitalize local health traditions & mainstream AYUSH.
• Promotion of healthy life styles.
The core strategies of the Mission
• Train and enhance capacity of Panchayati Raj Institutions (PRIs) to own, control and manage
public health services.
• Promote access to improved healthcare at household level through the female health activist
(ASHA).
• Health Plan for each village through Village Health Committee of the Panchayat.

• Strengthening sub-centre through better human resource development, clear quality standards,
better community support and an untied fund to enable local planning and action and more
Multi Purpose Workers (MPWs).
• Strengthening existing (PHCs) through better staffing and human resource
development policy, clear quality standards, better community support and an
untied fund to enable the local management committee to achieve these
standards.
• Provision of 30-50 bedded CHC per lakh population for improved curative care to a
normative standard. (IPHS defining personnel, equipment and management standards, its
decentralized administration by a hospital management committee and the provision of
adequate funds and powers to enable these committees to reach desired levels)
• Preparation and implementation of an inter sector District Health Plan prepared by the District
Health Mission, including drinking water, sanitation, hygiene and nutrition.
• Integrating vertical Health and Family Welfare programmes at National, State,
District and Block levels.
• Technical support to National, State and District Health Mission, for public health
management Strengthening capacities for data collection, assessment and review for evidence
based planning, monitoring and supervision.
• Formulation of transparent policies for deployment and career development of
human resource for health.
• Developing capacities for preventive health care at all levels for promoting healthy life style,
reduction in consumption of tobacco and alcohol, etc.
• Promoting non-profit sector particularly in underserved areas.
Programmes
• Reproductive and Child Health Programme – II (RCH-II) and the Janani
Suraksha Yojana (JSY) launched.
• Polio eradication programme intensified – cases reduced from 134 in 2004-05 to 63 (up to
now).
• Sterilization compensation scheme launched.
• Accelerated implementation of the Routine Immunization programme taken up. Catch up
rounds taken up this year in the States of Bihar, Jharkhand and Orisaa.
• Ground work for introduction of JE vaccine completed.
• Ground work for Hepatitis vaccines to all States completed.

• Auto Disabled Syringes introduced throughout the country.
• State Programme Implementation Plans for RCH II appraised by the National
Programme Coordination Committee set up by the Minstry. Funds to the
extent of 26.14% i.e. Rs. 1811.74 crore have been released under NRHM
Outlay.
Mission on nursing education:
The Mission would support strengthening of Nursing Colleges wherever required, as the
demand for ANMs and Staff Nurses and their development is likely to increase significantly.
This would be done on the basis of need assessment, identification of possible partners for
building capacities in the governmental and non governmental sectors in each of the
States/UTs, and ways of financing such support in a sustainable way. Special attention would
be given to setting up ANM training centres in tribal blocks which are currently para-medically
underserved by linking up with higher secondary schools and existing nursing institutions
HEALTH CARE DELIVERY SYSTEM IN ABROAD
UNITED STATES OF AMERICA
In the United States the health care delivery system in constantly changing. Implementation
and changes are brought according to needs of the citizens. There is a great division and
responsibility.
Health care system is divided in to private and public sector. The public section includes
federal state and local divisions and is cincerned with provision of healthy environment. Private
sector usually care for individuals and families.
Health Care Delivery System Models

Elementary Model of the health care delivery system
Consumers engaged in exchange of relationship with providers. It refelts a strange blend of
public and private enterprises. Mostly private patients are charged. More number of specialists
complicate the entry, there is lot of competetion among providers fee for service.

Public and private sector models:
Public system in composed of public health agencies, both voluntary and official at federal,
state and local levels. The private health care delivery system includes clinic, PPO, HMO, Hospital
based etc, here funding agencies are third party.
Health Care Delivery model: public and private sectors
ORGANISATION OF THE HEALTH CARE SYSTEM
PUBLIC SECTOR
Public agencies are financed with tax monies, thus these are accountable to the public. The public
sector includes official(governmental) agencies and voluntary agencies.`
Core Public Health Functions applied to Populations and Peple at Risk
Population- Wide ServicesAssessment
Health status monitering and disease surveillancePublic Policy
Leadership, policy, planning and administrationAssurance
Investigation and control of diseases and injuries
Protection of environment, workplaces, housing, food, and water
Laboratory services to support diseasecontrol and envirnmental proction.
Health education and information
Community mobilization for health-related issues
Targeted outreach and linkage to personal services
Health services quality assurance and assurance and accountability
Training and education of public health professionalsPersonal Services and Home Visits for People at Risk
Primary care for unserved and underserved people
Treating services for targeted conditions
Clinical preventive services
Payments for personal services delivered by others
ORGANISATION OF THE PUBLIC HEALTH SYSTEM
The public health system is organised in to many levels in the
• Federal,
• State,
• Local systems.
THE FEDERAL SYSTEM:

Federal Governmnet has the responsibility for the following aspects of health care.
At the federal level, the primary agencies are concerned with health are organized under the
Department of Health and Human Services(DHHS).
• Providing direct care for certain groups such as Native Americans, military personnel, and
veterans.
• Safeguarding the public health by regulating quarrentines and immigration laws and the
marketing food, drugs and products used in medical care.
• Prevents environmental hazzards, gives grantsin aids to states, local areas and individuals and
supports research.
• Administration of social security, social welfare and related programmes
• Public health service administer health functions such as mental health, health resources, the
National Institutes of health (NIH) Centres for Disease Control and preparation (CDC) and
the food and drug administration (FDA)
• The federal government looks in to the Division of Nursing to provide the competence and
expertise for administering nurse education legislation, interpreting trends and needs of the
nursing component of the nations health care delivery system.
STATE SYSTEM:
• Health financing (such as Medicaid) providing mental health and professional education,
establishing health codes, licensingfacilities and personneland regulating insurance industry.
• Direct assistance to local health departments
• Typical Programs in a State Health Department
o AIDS Services
o Disaster management
o Case management
o Departmental licensing boards
o Division of vital records
o Environmental programmes
o Epidemiology
o Health planning and development
o Health services cost review
o Juveline services
o Legal services
o Media and public relations and educational information
o Medical assistance: policy, compliance operations
o Mental health and addictions
o Mental retardation and developmental disabilities
o Preventive medicine and medical affairs
o Quality assurance
o Referral to resources
o Service to chronically ill and ageing
o STD(screening and treatment
• Nurses serve in many capacities in state health departments as consultants, direct servicce
providers, researchers, teachers and supervisors, as well as participating in programme
development planning, and evaluation of health programs. Many departments have a division
or department of nursing.
LOCAL SYSTEM
• Local health department has direct responsibility to the citizens in its community juridiction.
• Programmes provided by local health departments
o Addiction and alcohol clinics
o Adult health
o Disaster management
o Birth and death records
o Child day care and development
o Child health clinic
o Dental health clinic
o Environmental health
o Epidemiology and disease control
o Family planning
o Health education
o Home health agency
o Hospital discharge planning
o Hypertension clinic
o Immunization clinic
o Information services
o Maternal health
o Medical social work
o Mental health
o Nursing
o Nursing home licences
o Nutrition
o Occupational therapy
o School health
• The local level often provides an opportunity for nurses to take on signifacant leadership
roles, with many nurses serving as directors or managers.
PRIVATE SECTOR
The non governmental and voluntary arm of the health care delivery system includes many
types services.
• Privately owned, non profit agencies which includes most hospitals and wlfare agencies make
up one large group.
• Privately owned for profit agencies
• Private professional health care practice, composed largely of physician in solo practice or
group practice.
Private health services are complementary and supplementary to government healh agencies
FINANCING OF HEALTH CARE
Financing and health care significantly affects community health and community health
nursing practice. It influences the type and quality of services offered as well as the ways in which
those services are used. Sources of payment may be clustered in to three categories
• Third party payments
• Direct consumer payment
• Private or philanthropic support
Third party payments:
These are monetary reimbursements made to providers of health care by some one other that
the consumer who received the care. Organizations that administer these funds are called third party
payers.
Four types of payment sources
• Private insurance companies
• Independent health plans
• Government health programmes
• Claims payment agents
Private insurance companies
Private insurance companies market and underwrite policies aimed at decreasing consumer
risk of economic loss because of a need to use health services.
Three types of private insurers
1) Commercial stock companies: These sell health insurances, usually as a side line. They are
private stock hoders corporations that sell insurance nationally e.g Aetna, Travelers
2) Mutual companies: These insurer that operates in national marketplace are owned by their
policy holders e.g Prudentials,
3) Non profit: These operate under special state enabling laws that give them an exclusive
franchise to whole state and to a specific type of insurance.
E.g Blue cross sells only hospital coverage, Blue Sheild covers only medical insurance, Delta
Dental only dental insurance.
Independent Health Plans
Independent or self health plans underwrite the remaining health insurances in US. Usually
they may only sell health insurances; in some casee they may also provide health services. They focus
on a localized population
Government Health Programs
Government health programs make up the largest source of third party reimbursement in
United States. The governments four major health programme are
• Medicacare,
• Medicaid,
• Federal Health Benefits Plan
• Civilian Health and Medical Program of the Uniformed Services
Medicare:
• Provides mandatory federal health insurance for adults 65 years and older who have paid in to
social securtiy system and for certain disabled persons.
• It is the largest health insurance in US covering about 16% of the population. Among that 2%
are younger than 65 years of age and permanently disabled and chronically ill.
Medicaid

• Provides medical assistance to children, those who are aged, blind or disabled.
Claims payment Agents:
The government contracts with private agents to handle the claims payment process. More
than 80% of the governments third party payments have been handled by these private contractors.
Direct Consumer Reimbursement:
A second major source of health care financing comes from direct fees paid by consumers.
This refers to individual out-of –pocket payments made for several different reasons.
Health Maintainance Organisation:
A HMO is a system in which participants prepay a fixed monthly premium to receive
comprehensive health services delievered by a defined network providers to plan particiapants. HMO
are the oldest model of co ordinated or managed care..
Components of HMO:
• They serve a voluntary population
• There is a fixed annual or monthly payment
• The HMO some finaicial risk or gain.
• In contrast with physician in private practice, physician employed by HMO ecieve a fixed
salary.
There is a little co ordination between health care resources. There is variation in access,
quality of care, availability of health services within the state. It is said the US society in
individualistic, materialistic, aggressively competitive and market oriented.
Helath Care Delivery System in United Kingdom
UK has a tax-supported heath system that is owned by the governmnet, services are available
to all its citizens with out cost or for a small fee.
• In 1948, the United Kingdom passed the Acts which created the three separate but co-
operating National Health Services of Scotland, Northern Ireland and England and Wales that
provided free physician and hospital services to all people resident in the United Kingdom.
• Hospital staff are salaried employees according to nationally agreed contracts,
• whilst primary care is largely provided by independent practices, who are paid, again via a
nationally agreed contract, according to the number of patients registered with them and the
range of additional services offered.
• The National Health Service has been amended from time to time, but is largely intact.
Around 86% of prescriptions are provided free. Prescriptions are provided free to people who

satisfy certain criteria such as low income or permanent disabilities. People that pay for
prescriptions do not pay the full cost.
• Funding comes from a hypothecated health insurance tax and from general taxation.
• Private health services are also available. Private health care continued parallel to the NHS,
paid for largely by private insurance, but it is used only by a small percentage of the
population, and generally as a supplement to NHS services
Health Care Delivery System in Canada
• The Canadian health care delivery system is based on a national health insurance program that
is operated by each provincial governmnet.
• Specialists are concentrated in centres, where as primary health care providers are evenly
distributed through out canadian provinces.
• Canada has a federally sponsored, publicly funded Medicare system. Canada's system is
known as a single payer system, where basic services are provided by private doctors, with the
entire fee paid for by the government at the same rate. These rates are negotiated between the
provincial governments and the province's medical associations, usually on an annual basis. A
physician cannot charge a fee for a service that is higher than the negotiated rate - even to
patients who are not covered by the publicly funded system - unless he opts out of billing the
publicly funded system altogether.
Health Care Delivery System in Australia
• Australia and New Zealand both have publicly funded health care systems, though under the
Conservative government in Australia, there has been new funding and incentives for people
who pay for private health insurance.
• In Australia the current system, known as Medicare, was instituted in 1984. It coexists with a
private health system.
• Medicare is funded partly by a 1.5% income tax levy (with exceptions for low-income
earners), but mostly out of general revenue.
• An additional levy of 1% is imposed on high-income earners without private health insurance.
As well as Medicare, there is a separate Pharmaceutical Benefits Scheme that heavily
subsidises prescription medications

Health Care Delivery System in Cuba
Cuba is an island with an estimated population of 9170000.The climate is subtropical.
Agriculture is the most important economic activity. The world’s biggest producer of sugar.
Principles of health care delivery system in Cuba:
1. Health of a population is government responsibility.
2. Health services should be available to all the population
3. The community should participate actively in health work
4. Preventive and curative health services should be intergraded.
• Cuba has a health service system accessible and available to practically 100% of the
population, with a referral system ensuring the approriate level of care for each patient.
• Preventive curative and rehabilitative services are well planned and integrated and show
excellent result in terms of service indicators and mortality and morbidity data.
• 50% or more of the budget is allotted to to health and education.
• Certain factors have helped to make the Cuban health services efficient, such as extremely
high motivation of health services, complete literacy, high proportion of doctors and other
proffessionals staff, good transport facilities, mass mobilization and full participation of the
people.
Health Care Delivery System in Peru
Peru is a poor country that is considered to be transition. There has never been centrally
controlled or equity in availability of health care. People in countryside are treated by
“curanderos” who are traditional healers. The ministry of health of Peru obtained technical help
from Pan American health organisation and the start of a system of organized care for the poor,
and for the rich began to become a reality. The government has began surveillance of infectious
diseases and has omplememented progras to imoprove sanitation.
WHO works closely with other organizations within the United Nation System. It is a
constitutional requirement that WHO should establish and maintain effective collaboration with
the United Nations and provide health services and facilities. UNICEF has been one of the closest
partners. In 1989 WHO and UNICEF jointly launched an initiatives for mothers and children
called “facts of life”
Health system in Africa
• Health care in Africa is usually non existent or highly limited and under resourced. The
outbreak and spread of HIV/AIDS in Africa has crippled many populations and sent life
expectancies plummeting.

• However some countries have been able to tackle the challenges, for instance health care in
Uganda as well as education has reduced HIV/AIDS infections from 13% to 4.1% from 1990
to 2003.
Health system in Nigeriria Health care provision in Nigeria is a concurrent responsibility of the
three tiers of government in the country. However, because Nigeria operates a mixed economy,
private providers of health care have a visible role to play in health care delivery.
• The federal governments role is mostly limited to coordinating the affairs of the university
teaching hospitals, while the state government manages the various general hospitals and the
local government focus on dispensaries.
• The total expenditure on health care as % of GDP is 4.6, while the percentage of federal
government expenditure on health care is about 1.5%.
• National Health Insurance Scheme, the scheme encompasses government employees, the
organized private sector and the informal sector. Scheme also covers children under five,
permanently disabled persons and prison inmates
Health Care Delivery System in Asia
Israel, South Korea, Seychelles and Taiwan have universal health care. Thailand plans to.In
Sri Lanka, drugs are provided by a government owned drug manufcaturer called the State
Pharmaceuticals Corporation of Sri Lanka. In the Philippines, the Department of Health (Philippines)
organises public health for the country, and was established at the initiative of the American
governers, before independence. Saudi Arabia has a publicly funded health system, although its levels
are lower than the regional average.
Health care delivery system in Singapore
Singapore has a dual system of healthcare delivery, comprising of the public and private
systems. Primary healthcare is provided at outpatient polyclinics and private medical practitioners'
clinics. Secondary and tertiary specialist care are provided in the public and private hospitals.
The private practitioners provide 80% of the primary healthcare services while the public
polyclinics provide the remaining 20%. For hospital care, it is the reverse with 80% of hospital care
being provided by the public sector and the remaining 20% by the private sector.
In 1999, the public healthcare delivery system was re-organized into two vertically
integrated delivery networks, the National Healthcare Group and the Singapore Health Services. This
was to enable the delivery of more integrated and better quality and healthcare services through
greater cooperation and collaboration among the public sector healthcare providers. This system also
minimises the duplication of services and ensures the optimal development of clinical capabilities.
This public healthcare system is supported by the Singapore Civil Defence Force's Ambulance
Service which provides paramedical support and transport for accident and trauma victims as well as
medical emergencies.
Health System in China
Great advances in public health have been hallmark of the People’s Republic of China since it
was founded in 1949. Examples of public health advances that were made in china including
controlling contagious disease such as cholera, typhoid etc. These accomplishments in public health
were credited to a political system that was and is largely socialistic terms as collective.
• The collective health care system was owned and controlled by the state and was
characterised by the use of barefoot doctors who were medical practioners trained at the
community level and who could provide a minimal level of health throughout the country.
• Barefoot doctors combined western medicine with traditional techniques such as acupuncture,
herbal remedies.
• Chinas health care system is modified by the introduction of primary health care system in
community health clinics(CHC) based on the health care system in Canada. With this system,
a family practice physician is assigned 500 or more individuals for whom to provide health
care.
A Comparative Study Of Health Care Delivery System
Comparison of Effectiveness of Different Health Care Delivery System through Available Data
CountryLife
expectancy
Infant mortality
rate
Physicians per 1000 people
Nurses per
1000 people
Per capita expenditure
on health (USD)
Healthcare costs as a percent of
GDP
% of government
revenue spent on health
% of health costs paid
by government
Australia 80.5 5.0 2.47 9.71 2,519 9.5 17.7 67.5
Canada 80.5 5.0 2.14 9.95 2,669 9.9 16.7 69.9
China 31.0 2.0 2.7 24.9
Srilanka 16.00 0.2 1.02 3.0 45.4
Japan 82.5 3.0 1.98 7.79 2,662 7.9 16.8 81.0
Sweden 80.5 3.0 3.28 10.24 3,149 9.4 13.6 85.2
UK 79.5 5.0 2.30 12.12 2,428 8.0 15.8 85.7
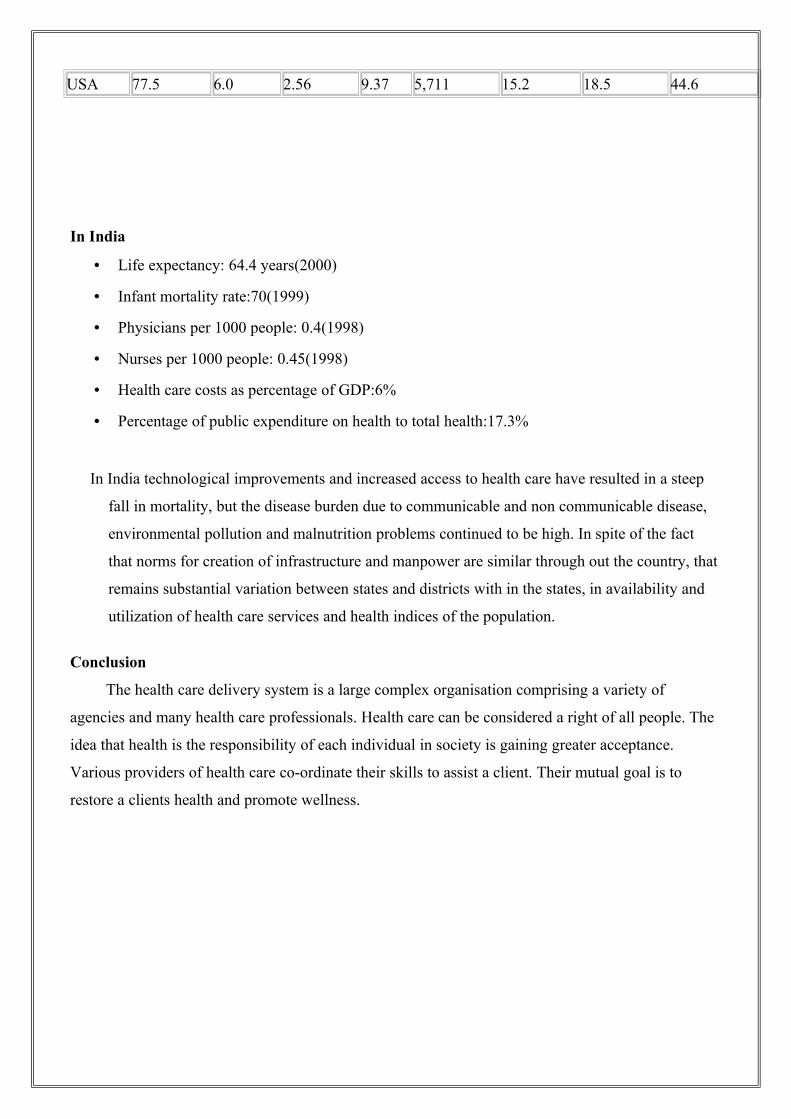
USA 77.5 6.0 2.56 9.37 5,711 15.2 18.5 44.6
In India
• Life expectancy: 64.4 years(2000)
• Infant mortality rate:70(1999)
• Physicians per 1000 people: 0.4(1998)
• Nurses per 1000 people: 0.45(1998)
• Health care costs as percentage of GDP:6%
• Percentage of public expenditure on health to total health:17.3%
In India technological improvements and increased access to health care have resulted in a steep
fall in mortality, but the disease burden due to communicable and non communicable disease,
environmental pollution and malnutrition problems continued to be high. In spite of the fact
that norms for creation of infrastructure and manpower are similar through out the country, that
remains substantial variation between states and districts with in the states, in availability and
utilization of health care services and health indices of the population.
Conclusion
The health care delivery system is a large complex organisation comprising a variety of
agencies and many health care professionals. Health care can be considered a right of all people. The
idea that health is the responsibility of each individual in society is gaining greater acceptance.
Various providers of health care co-ordinate their skills to assist a client. Their mutual goal is to
restore a clients health and promote wellness.

BIBLIOGRAPHY
1. Marcia Stanhope, Jeanette Lancaster. Community and public Health Nursing. 6th ed. United
States of America. Mosby. 200 .P. 72-85
2. Judith Ann Allender, Barbara Walton Spradley. Community Health Nursing. 6th ed. New
York. Lippincott Williams and Wilkins. 200 .P. 108-142
3. Park.J.E, Park.k. Text Book of Preventive and Social Medicine. 19th ed. Jebalpur. Bhansari
Bhanot publishers. 2007.p. 732-745
4. Gupta MC, Mahajan BK. Text Book of Preventive and Social Medicine. 3rd ed. New Delhi.
Jaypee Brothers Publications. 2005. P.450-460.
5. Kasturi Sundar Rao. An Introdction to Community Health nursing. 4th ed. Chennai. BI
Publications. 2005. P. 363-379
6. Patricia A, Potter, Annie Grefin Perry. Fundamnetals of Nursing. 6th e.d. Missouri, Mosby
Publications. 2006. P.26-43
7. Indian Public Health Standards for PHC. Available from URL:http://www.mhfw.org
8. Indian Public Health Standards for Sub Centres. Available from URL:http://www.mhfw.org
9. Indian Public Health Standards for CHC. Available from URL:http://www.mhfw.org
10. http://www.hpp.moh.gov.sg/HPP/1128567828615.html