18th iasgo congress - istanbul, october 8-11, 2008 surgical treatment of large liver hydatidosis –...
TRANSCRIPT

18th IASGO Congress - Istanbul, October 8-11, 2008
SURGICAL TREATMENT OF LARGE LIVER HYDATIDOSIS – A COMPARISON OF DIFFERENT PROCEDURES
Dr. Avdyl Krasniqi – Kosova( Prishtina )Dr. Viktor QERESHNIKU – Albania ( Tirana )
E bp. A.Krasniqi¹, V. Qereshniku², B. Elezi ² , D. Limani ¹, F. Hoxha ¹,, A. Beqiri ², B. Bicaj ¹, A. Gjata ² , R.
Musa ¹, S. Agolli ² , G. Spahija ¹, A. Kerciku ² , S. Krasniqi³, L. Gashi-Luci ³
¹University Clinical Centre of Kosova, Prishtina, Kosovo
² University Hospital Centre “Mother Theresa”, Tirana, Albania
³ University of Prishtina,Faculty of Medicine, Prishtina, Kosovo

18th IASGO Congress - Istanbul, October 8-11, 2008
INTRODUCTION

18th IASGO Congress - Istanbul, October 8-11, 2008
INTRODUCTION
• Liver hydatidosis has been a common pathology for years in the surgical departments of our hospitals;
• Surgery combined with scolicidal therapy is the most often used treatment modality;
– Mainly treated large liver hydatid cysts of:• Different topographic locations (T)¹
• Different levels of complication (C1-C6)» ¹Kjosev KT, Losanoff JE: J Gastroenterol Hepatol. 2005;20:352-9

18th IASGO Congress - Istanbul, October 8-11, 2008
INTRODUCTION
• Although concept of management of liver hydatidosis is changing, surgery is still gold standard for complete cure²
• There is still contraversy regarding the appropriate surgical technique³
• Open surgical procedures: – Tissue sparing techniques; endocystectomies/partial
pericystectomy– Radical procedures; complete pericystectomy/resection
» ²Dervenis et al.:Journal of Gastrointestinal Surgery 2005;9:869-877.
» ³Skroubis et.: World Journal of Surgery 2002;26:704-708.

18th IASGO Congress - Istanbul, October 8-11, 2008
OBJECTIVE
• To analyze the outcome of different surgical procedures that were used for treatment of 545 patients with large liver hydatid cysts.

18th IASGO Congress - Istanbul, October 8-11, 2008
MATERIAL AND METHODS
• A retrospective study• Chart review of patients with large liver hydatid cysts
treated surgically over 15 years period in two university hospitals with almost similar settings in terms of patients, hospital resources and surgical teams:
• University Clinical Centre of Kosova (UCKK) in Prishtina• University Hospital Centre “Mother Theresa” in Tirana
(UHCT), Albania
18th IASGO Congress - Istanbul, October 8-11, 2008
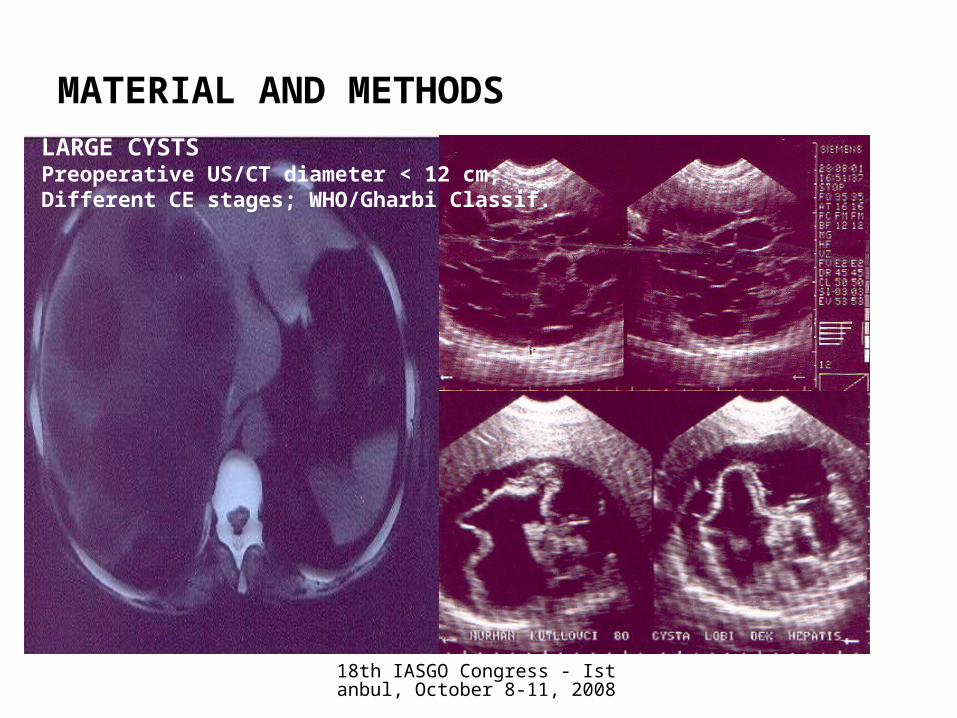
LARGE CYSTSPreoperative US/CT diameter < 12 cm;Different CE stages; WHO/Gharbi Classif.
MATERIAL AND METHODS

18th IASGO Congress - Istanbul, October 8-11, 2008
PATIENTS• Total 545
– Goup I 293 (UCCK - Prishtina• Female 182 (62.08%)• Male 111 (37.92%)
– F:M = 1.63:1
– Group II 252 (UHC – Tirana)
• Age– Median 37 years (Range 17-81)
• 20-40 range most often attacked
MATERIAL AND METHODS

18th IASGO Congress - Istanbul, October 8-11, 2008
TREATMENT – FOLLOWED PRINCIPLES
• Choice of procedure depends from:– Size of the cyst– Localization– Intrabiliary communication– Age– Equipment– Surgical team
18th IASGO Congress - Istanbul, October 8-11, 2008
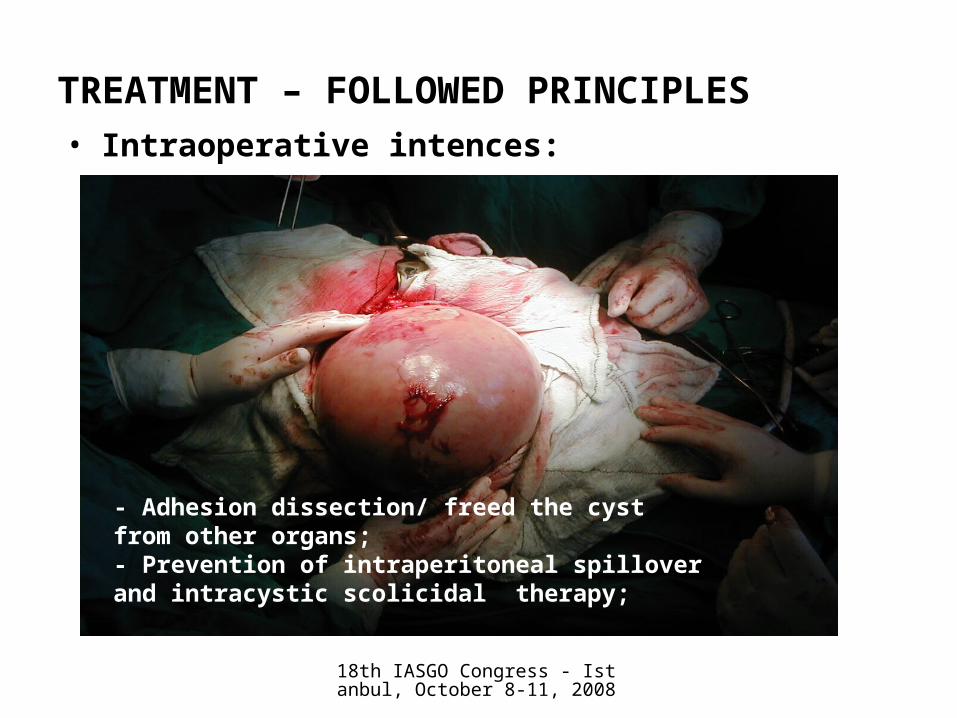
TREATMENT – FOLLOWED PRINCIPLES• Intraoperative intences:
- Adhesion dissection/ freed the cyst from other organs;- Prevention of intraperitoneal spillover and intracystic scolicidal therapy;

18th IASGO Congress - Istanbul, October 8-11, 2008
TREATMENT – FOLLOWED PRINCIPLES• Intraoperative intences:
- Removal/ennucleation of cysts

18th IASGO Congress - Istanbul, October 8-11, 2008
TREATMENT – FOLLOWED PRINCIPLES• Intraoperative intences:
–Total/partial pericystectomy

18th IASGO Congress - Istanbul, October 8-11, 2008
TREATMENT – FOLLOWED PRINCIPLES• Intraoperative intences:
- Careful treatment of the cavity- closure of eroded bile channels-Check main bile channel for daughter cysts (selectively)-Pre/post operative ERCP/removal of daughter cysts (rarely)

18th IASGO Congress - Istanbul, October 8-11, 2008
TREATMENT – FOLLOWED PRINCIPLES• Intraoperative intences:
–Omentoplication, T-tube (selectively)
–Drainage; Cavity and sub hepatic

18th IASGO Congress - Istanbul, October 8-11, 2008
RESULTS
Localisation (%) in the Liver
62.75%27.80%
18.90%
Right Lobe
Left Lobe
Both Lobes

18th IASGO Congress - Istanbul, October 8-11, 2008
Main Clinical Signs
53.6
30.9
19.5 17.8
76.6
50.441.3
20.6
65.1
40.6
30.4
19.2
0
1020
3040
5060
7080
90
Hepatomegaly Abdominalmass
Temperature Joundice
%
Groupe I
Groupe II
Average

18th IASGO Congress - Istanbul, October 8-11, 2008
SURGICAL PROCEDURES
202
2556
10
192
46
5 9
394
71 61
19
0
50
100
150
200
250
300
350
400
450
Endocyst
&part
ial/subto
tpericyste
cto
my
Tota
l peric/liv
er
resec
Endocyst&
capitonnage
Exte
rnal dra
inage
Nu
mb
er
of
pts
.
Groupe I
Groupe II
Total

18th IASGO Congress - Istanbul, October 8-11, 2008
Surgical Procedures in %
Endocyst & partial/subtot pericystect.
69%
Total peric/liver resec12%
Endocyst&capitonnage
11%
External drainage
8%

18th IASGO Congress - Istanbul, October 8-11, 2008
CYST LOCALISATION IN THE LIVER
SURGICAL PROCEDURES
Mean postoperative hospital days
16.6
34
0 10 20 30 40
Group I
Group II
Postop. hospital stay
• Mean postoperative hospital days:– 25.3 (min. 5, max. 93)
• Gr. I: 16.6 (min. 5, max. 71)• Gr. II: 34 (min. 9, max. 93)
• Bile duct exploration: – 95 pts (17.43%)
• Gr. I: 43 pts (14.6%)• Gr. II: 52 pts (20.6%)

18th IASGO Congress - Istanbul, October 8-11, 2008
Postoperative Complications
0
5
10
15
20
25
30%
Group I 4.99 15.07 6 3.87 4.4 0.34
Group I I 4.7 1.15 28.1 1.19 4.36 3.17
Average 4.84 8.11 17.05 2.82 4.38 3.15
Billiary fistula
PleuritisWound
infectionAbscessus
sd.Abscessus
of cavityMortality

18th IASGO Congress - Istanbul, October 8-11, 2008
CONCLUSION
• This study showed that:– Enucleation of endocysts, clean up of detritus and
other materials from cavity, partial pericystectomy, closure of eroded bile channels, introflexion of pericystic edges and omentolplasty, was most often applied.
– Marsupialization, endocystectomy with capitonnage as well as external drainage that were used in the past decades, had a higher postoperative complication rate and longer hospital stay compared to the previous procedure.

18th IASGO Congress - Istanbul, October 8-11, 2008
– Radical surgical approach to a benign pathology such as LH is not an appropriate treatment modality for hospitals with limited resources.
• Therefore:– For large and complicated LH we recommend
endocystectomy, partial pericistectomy with omentoplasty.

18th IASGO Congress - Istanbul, October 8-11, 2008
THANK YOU!