20 l manganaro rm fetale utilita’ e limiti
TRANSCRIPT

RM
UTILITA’ e LIMITI
Lucia Manganaro
Dipartimento di Scienze Radiologiche
Oncologiche e antamopatologiche
AGGI ORNAMENTI DI
ECOCARDI OGRAFI A
FETALE
I I a edizione
I NFORMAZI ONI GENERALI
COMI TATO SCI ENTI FI CO
Prof.ssa Flavia Ventriglia: U.O.C. di Cardiologia Pediatrica - Azienda Policlinico Umberto I Roma- Sapienza Università di Roma; email: [email protected] Prof. Bruno Marino: U.O.C. di Cardiologia Pediatrica Azienda Policlinico Umberto I Roma- Sapienza Università di Roma; email: [email protected] ECM Il corso è in fase di accreditamento per 15 ECM Discipline principali di riferimento: Cardiologia, Ginecologia, Pediatria, Neonatologia, Genetica medica
SEDE DEL CORSO: Aula Magna della Clinica Pediatrica Policlinico Umberto I, Viale Regina Elena n°324— 00161 Roma Il corso è aperto ad un massimo di 70 partecipanti + 30 riservati a studenti, specializzandi, masterizzandi delle aree interessate
ISCRIZIONE: La quota di iscrizione al co rso è di € 80
.
00 Comprende: Materiale congressuale + coffee breaks + work lunches—Attestato di partecipazione, crediti ECM. Gratuito per tutti i professionisti dipendenti dell’Azienda Sanitaria Policlinico Umberto I e per gli studenti, specializzandi e masterizzandi delle aree di interesse con documentazione allegata
I PARTECIPANTI POTRANNO PRESENTARE DEI CASI CLINICI DA DISCUTERE IN SEDE CONGRESSUALE IL 19/4 ORE 16
S
Dipart iment o di Pediat ria
Policlinico Umbert o I
Università “Sapienza”
Roma
18/ 19 Aprile 2015
Con la collaborazione:
SEGRETERI A ORGANI ZZATI VA Ufficio Formazione – Azienda Policlinico Umberto I mail: [email protected] tel. 06/49974962 Fax 06/49974961 Sito web: policlinicoinformazione.blogspot.it
Con il Pat rocinio
MODALITA’ DI PA GAMENTO: Il pagamento potrà essere effettuato tramite Bonifico bancario: Causale: Iscrizione Corso di Aggiornamento di Ecocardiografia Fetale Aprile 2015 C/C bancario n. 12144/38 – Monte dei Paschi di Siena – Agenzia n°10 Roma, piazza Vescovio, 18 Coordinate bancarie CIN Z, ABI 01030, CAB 03210 IBAN: IT 58C 01030 03210 00000 1214438 MODALITA’ DI IS CRIZIONE: Sul sito: policlinicoinformazione.blogspot.it e/o all'indirizzo http://www.policlinicoumberto1.it/il-policlinico/formazione/calendario-corsi/elenco-corsi-attivi-2015.aspx si troveranno tutte le modalità di iscrizione al corso
BACKGROUND
Congenital heart disease is one of the most frequent prenatal malformations (incidence of 5/1000 live births),it represents the primary cause of death in the first year of life
Considering the wide range of severity, a good prenatal examination acquires a great importance in order to formulate an early diagnosis and improve the pregnancy management
Nowadays investigation of CHD is performed with echocardiography considered the standard reference for diagnosis

TRANSVERSAL VIEWS: - Four chambers
- Five chambers
- Three vessels
SAGITTAL VIEWS: - Short axis left ventricle
- Tricuspid-aortic cut
- Long axis of the ductus arteriosus
- Long axis of the aortic arch
ANGULATED VIEWS: - Long axis of the left ventricle
- Aortic arch and ductus arteriosus
Projection

To simplify the understanding of CHD we identify
7 categories:
1. cardial situs anomalies
2. right and left ventricular hypoplasia
3. cardiac masses
4. great vessel abnormalities
5. abnormalities of transposition and connection
6. defects of inflow and outflow
7. septal defects
Characterization of CHD

a
c
d
Situs inversus is easy to recognize after a first valuation of the position of the fetus compared to the mother in order to define the left and right sides. Moreover fetal MRI allows assessment of the visceroatrial situs in relation to the bronchi. The fluid-filled bronchial tree appears as high-signal-intensity structures on SSFP images *.
*Brugger PC, Stuhr F, Linder C, Prayer D. Methods of fetal MR: beyond T2-weighted imaging. Eur J Radiol2006
1.Cardial situs anomalies
b27-week gestation fetus with complete situs inversus. Fetus position is transversal with head on the right side of
the mother as indicated by the position of the liver( white arrow) and stomach (red arrow)
Figure a) represent the posterior plan of the coronal view acquired on the mother, it shows the liver (arrow)
instead of the stomach, which is endeed shown on an anterior plane of the coronal view ( figure b).
c)Liver is located on the left side of the fetus. d) heart is located on the right side.
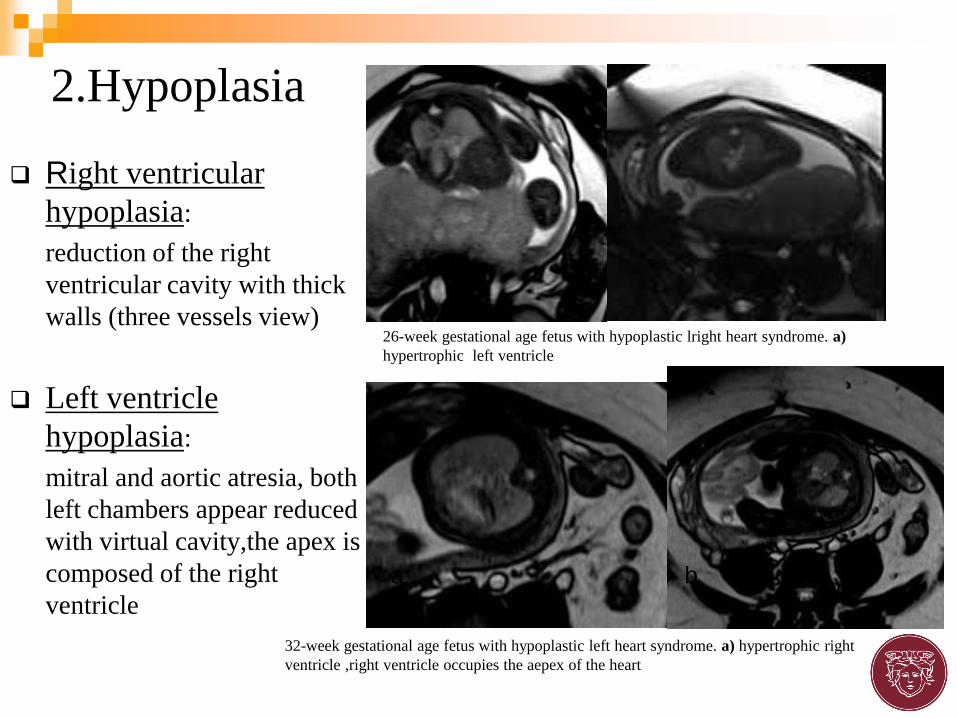
Right ventricular
hypoplasia:
reduction of the right
ventricular cavity with thick
walls (three vessels view)
Left ventricle
hypoplasia:
mitral and aortic atresia, both
left chambers appear reduced
with virtual cavity,the apex is
composed of the right
ventricle
2.Hypoplasia
32-week gestational age fetus with hypoplastic left heart syndrome. a) hypertrophic right
ventricle ,right ventricle occupies the aepex of the heart
a b
26-week gestational age fetus with hypoplastic lright heart syndrome. a)
hypertrophic left ventricle

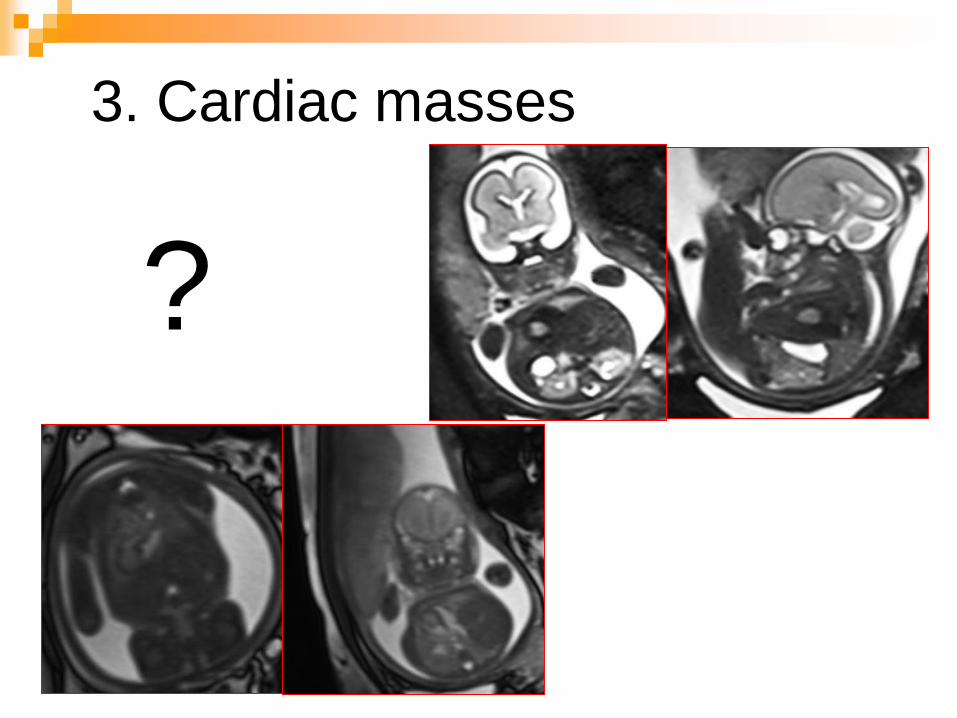
3. Cardiac masses
?

Teratomas:
• inhomogeneous in T2 weighted
sequences for the combination of
solid and fluid components
• differential diagnosis with thorax
pathologies (ex: CCAM , BPS)
3.Cardiac masses 2
25 week gestation fetus affected by perycardial teratoma.
Multilobulated lesion with inhomogeneous signal in T2w
sequences (arrow), located in the perycardium.

Aortic coartaction (CoA): reduction of the left ventricle; There is considerable overlap in the relative size of
the aortic arch, therefore a diagnosis of coartaction is generally a provisional diagnosis even in
echocardioghraphy. preliminary experiences demonstrated how measurement, on the three vessel view, of
the main mediastinal pulmonary artery to ascending Ao diameter ratio can be a helpful tool in distinguishing
true CoA[-]
Slodki M, Rychik J, Moszura et Al.Measurement of the great vessels in the mediastinum could help distinguish true from false-positive
coarctation of the aorta in the third trimester.J Ultrasound Med. 2009 Oct;28(10):1313-7.
.
4.Great vessels abnormalities
32 week gestation fetus affected by aortic coartaction (arrows). a-b) Gradient Echo T1 weighted 3D sequences
a b c

4.Great vessels abnormalities2
Aortic corctation 2:
28-week gestation
fetus.
a)vessel view (arrow)
b)hypoplastic left
ventricle (arrow)
c)aortic coartaction
(arrowhead)
Aortic corctation 3:
27-week gestation fetus
with DiGeorge
syndrome. Both axial
scans illustrate the
aortic coartaction (long
arrow) and the thymus
absence (short arrow) .
a b c

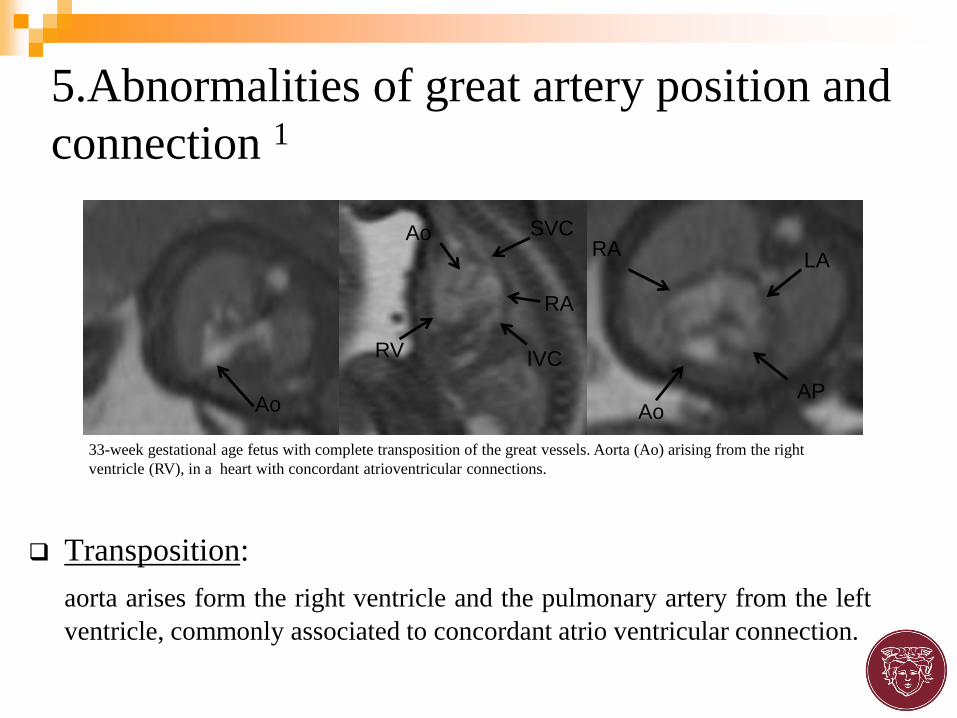
Transposition:
aorta arises form the right ventricle and the pulmonary artery from the left
ventricle, commonly associated to concordant atrio ventricular connection.
5.Abnormalities of great artery position and
connection 1
Ao Ao
RA
AP
LA
Ao
RV
RA
IVC
SVC
33-week gestational age fetus with complete transposition of the great vessels. Aorta (Ao) arising from the right
ventricle (RV), in a heart with concordant atrioventricular connections.
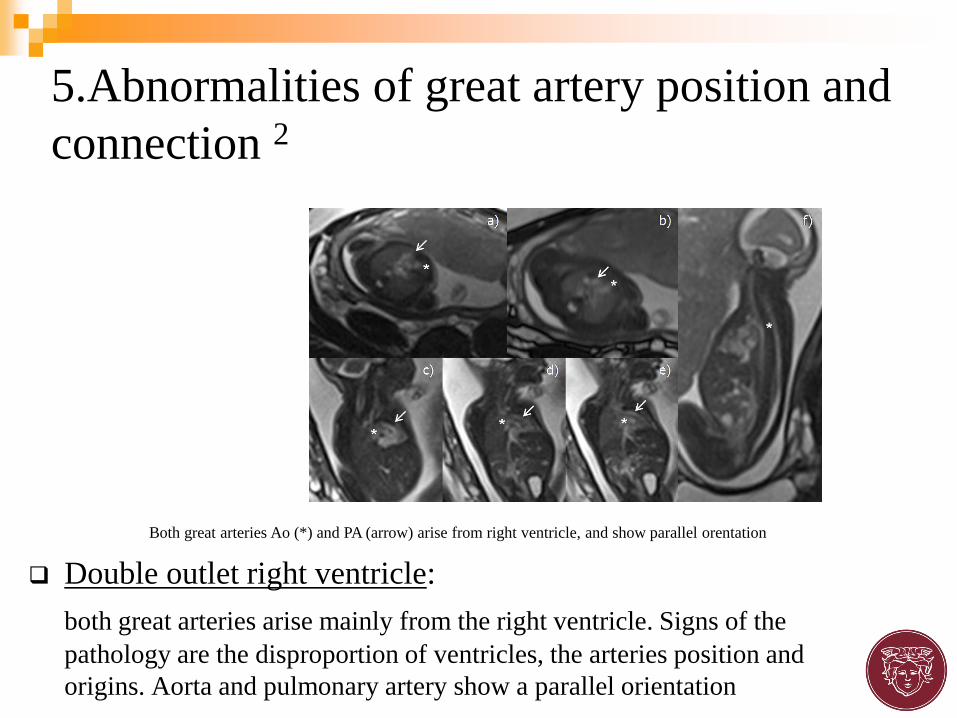
Double outlet right ventricle:
both great arteries arise mainly from the right ventricle. Signs of the
pathology are the disproportion of ventricles, the arteries position and
origins. Aorta and pulmonary artery show a parallel orientation
5.Abnormalities of great artery position and
connection 2
Both great arteries Ao (*) and PA (arrow) arise from right ventricle, and show parallel orentation
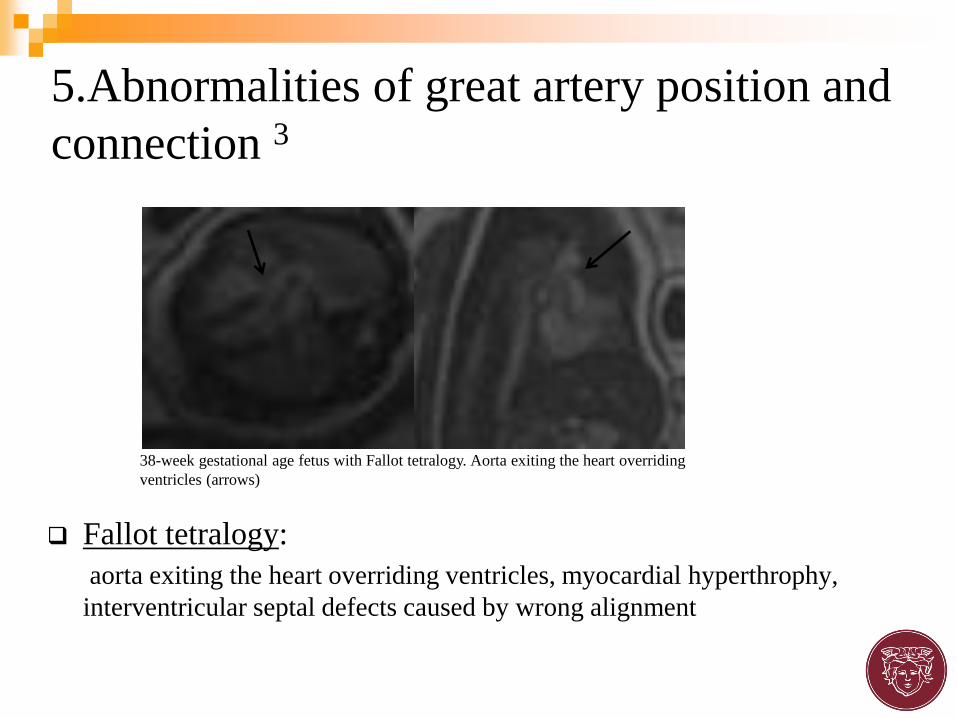
Fallot tetralogy:
aorta exiting the heart overriding ventricles, myocardial hyperthrophy,
interventricular septal defects caused by wrong alignment
5.Abnormalities of great artery position and
connection 3
38-week gestational age fetus with Fallot tetralogy. Aorta exiting the heart overriding
ventricles (arrows)
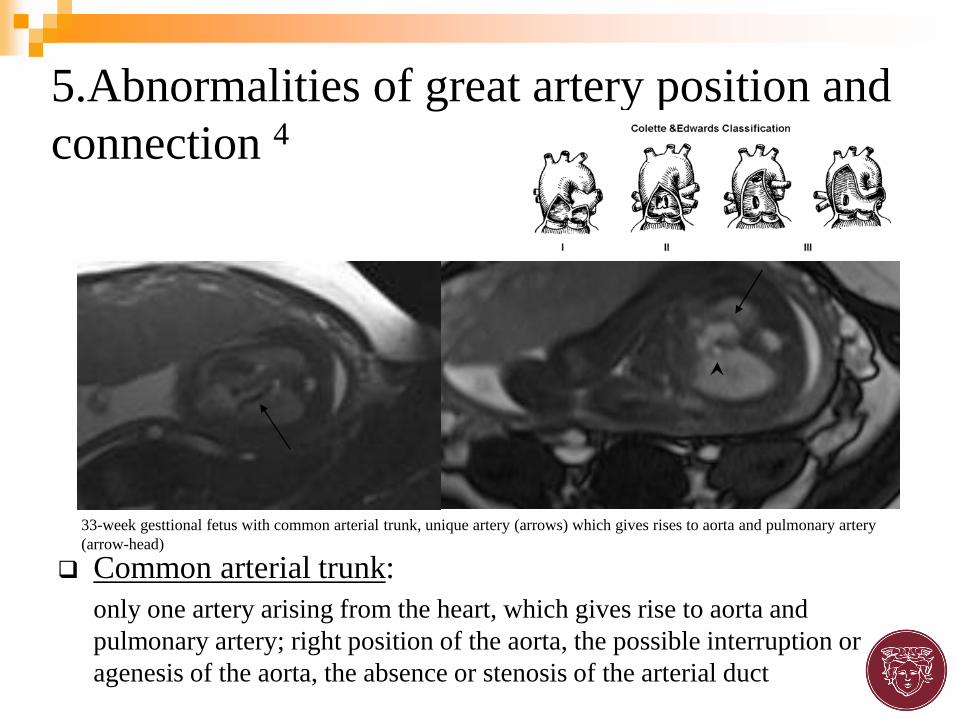
Common arterial trunk:
only one artery arising from the heart, which gives rise to aorta and
pulmonary artery; right position of the aorta, the possible interruption or
agenesis of the aorta, the absence or stenosis of the arterial duct
5.Abnormalities of great artery position and
connection 4
33-week gesttional fetus with common arterial trunk, unique artery (arrows) which gives rises to aorta and pulmonary artery
(arrow-head)

5.Abnormalities of great artery
position and connection 5
Azygos
continuation

Double aortic arch
5.Abnormalities of great artery position and
connection 6

Outflow defects:
obstructive left outflow:
disproportion of the left and right
chambers with the possibility of a
wider right ventricle
obstructive right outflow:
enlargement of the right ventricle,
associated to a right atrial
enlargement and myocardial
thickness.
Inflow defects:
mitral stenosis or valves
deficiency
6. Outflow and Inflow defects
30° week gestation fetus affected by obstructive right outflow (tricuspidal
atresia). Severe reduction of the right ventricle with virtual lumen (arrow) and
right atrium dilatation (*). B) absente visualization of pulmonary outflow

DIV
PULMONARYATRESIA
DIV27 Week
AP?
SVC
AO
AO
SVC
AO

PULMONARY ATRESIA
32° WEEK

Septal atrial defects:
secundum atrial septal defect,
difficult to diagnose because of
the physiological persistence of
the foramen ovale. In wide defects
indirect signs such as an
enlargement of the right atrium
can be associated.
Septal ventricular defects:
well studied in the four chamber
views, often associated with other
pathologies such as a Fallot
syndrome.
7.Septal defects 1
32-week gestational age fetus with septal ventricle defect. Lack of
continuity in the lower septal part (arrow)
27-weekgestational fetu swith wide septal artial defect, absence of the atrial
sepum (arrow) in a four chamber view.

Common atrioventricular
septal defect:
associated with a deficiency in
the central septal , a unique
central valve and a defect of the
ventricular septum which
appear to unevenly divide the
heart (unbalanced ventricles)
More difficult is the diagnosis
of partial atrioventricular septal
defect characterized by only the
atrial defect.
7.Septal defects 2
a) Wide septal atrial and ventricular defect . b) malrotation of the
cardiac axis

29-weeks fetus - VENTRICULAR SEPTAL DEFECT
(VSD) with possible association of coartaction of the aorta excluded by angio-MR sequences
T1 3D SPOILED
GE angio-MR
sequences to
assess the aorta
(MIP)

Various studies demonstrated the potential role of fetal magnetic resonance imaging as an adjunctive imaging technique in the prenatal evaluation of CHD.
MRI may add other clinical information regarding associated extracardiacpathologies *
MRI could be advisable from the second trimester of pregnancy, when a preliminary ultrasound examination proves inadequate or diagnostically inconclusive *
MRI could offer a better imaging compared to US in an advanced gestational stage because of the progressive reduction of amniotic fluid and the ribs ossification
ROLE OF FETAL MRI

Various studies demonstrated the potential role of fetal magnetic resonance imaging as an adjunctive imaging technique in the prenatal evaluation of CHD.
MRI may add other clinical information regarding associated extracardiacpathologies *
MRI could be advisable from the second trimester of pregnancy, when a preliminary ultrasound examination proves inadequate or diagnostically inconclusive *
MRI could offer a better imaging compared to US in an advanced gestational stage because of the progressive reduction of amniotic fluid and the ribs ossification
ROLE OF FETAL MRI

Lungs
Thymus
Other malformations (BRAIN)

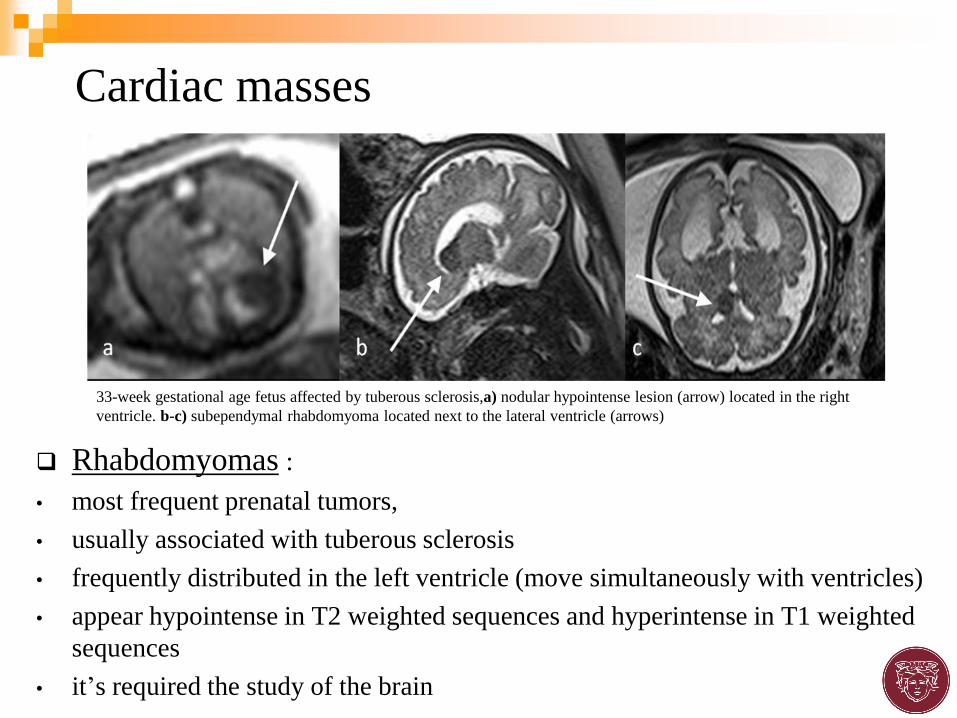
Rhabdomyomas :
• most frequent prenatal tumors,
• usually associated with tuberous sclerosis
• frequently distributed in the left ventricle (move simultaneously with ventricles)
• appear hypointense in T2 weighted sequences and hyperintense in T1 weighted
sequences
• it’s required the study of the brain
Cardiac masses
33-week gestational age fetus affected by tuberous sclerosis,a) nodular hypointense lesion (arrow) located in the right
ventricle. b-c) subependymal rhabdomyoma located next to the lateral ventricle (arrows)

ROLE OF FETAL MRI
Postmortem cardiac imaging in fetuses
3-D cardiac postmortem MRI
MARIAS (magnetic resonance imaging autopsy study) compared the
diagnostic accuracy of 3-D cardiac postmortem MRI with conventional
autopsy and histopathology assessment in fetuses and children
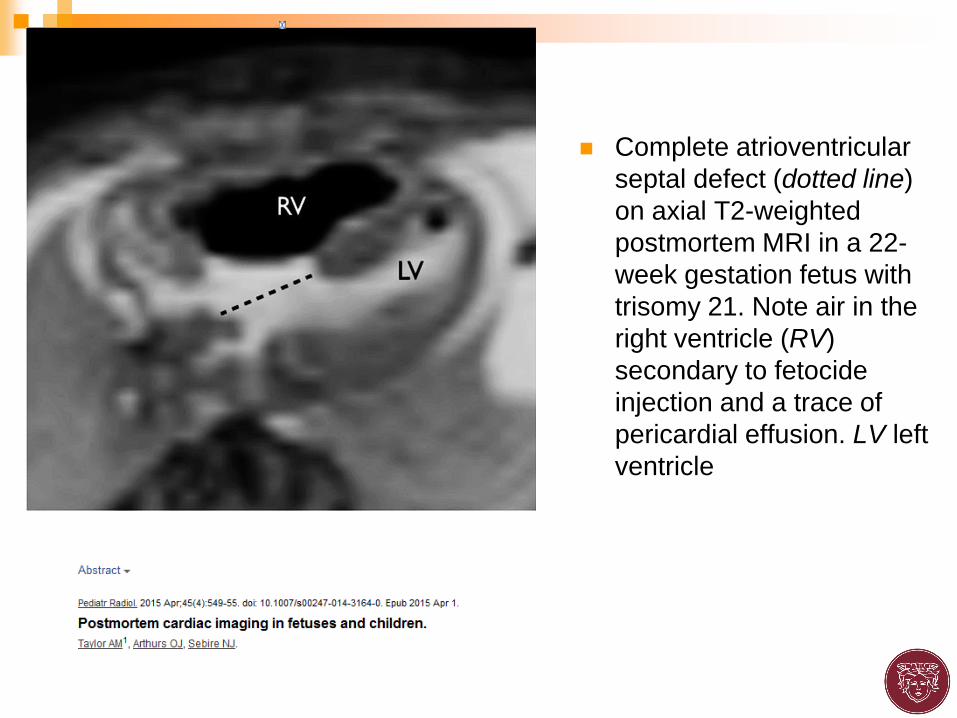
Complete atrioventricular
septal defect (dotted line)
on axial T2-weighted
postmortem MRI in a 22-
week gestation fetus with
trisomy 21. Note air in the
right ventricle (RV)
secondary to fetocide
injection and a trace of
pericardial effusion. LV left
ventricle

Fetal cardiac postmortem
MRI in a 29-week gestation fetus
shows a large cardiac teratoma (T)
following unsuccessful in utero
laser ablation. The large teratoma
displaces the heart posteriorly and
laterally on (a) axial and (b)
oblique coronal T2-weighted
images. LV left ventricle, Rvrig
ventricle

Fetal cardiac postmortem MRI shows
hypoplastic left heart syndrome
on sagittal T2-weighted image in a 22-
week gestation fetus. LV left
ventricle, RV right ventricle.

Three-dimensional cardiac postmortem MRI can provide
equivalent structural information to that of conventional autopsy
in the majority of larger fetuses, newborns and children.
This technique may have a major role in developing lessinvasive
autopsy methods. Moreover, routine use of cardiac
postmortem MRI as an adjuvant to conventional autopsy may
increase the yield from conventional autopsy. Further study of
high-field postmortem MRI, postmortem CT and micro-CT
will continue to optimize the best methods for this form of
less-invasive postmortem assessment.

Studies with heterogenus and small population
Absence of standardized measurement and protocols
Technical and Anatomical Limitations :
Severe heart malrotation
Small heart size
Low evaluation of motion fluid
Absence of real time resolution due to:
- Fast fetal heart rate
- Low time resolution
- cardiac triggering
LIMITS OF CARDIOVASCULAR MRI
Inability to study : - valvular disease (indirect signs)
- rhythm disorders


FETAL CARDIAC MRI
FETAL CARDIAC MRI
3D MRI SEQUENCES
Higher SNR
Ability to reformat images in muliple planes
Fast free –breathing in vivo fetal imaging using time-resolved 3D-MRI
technique: preliminary results
Liu J et al . Quant Imaging Med Surg 2014

FETAL CARDIAC MRI
More sensitive to fetal motion

FETAL MRI
Although advances in magnetic resonance technology have expanded the clinical role of MRI
for pediatric patients with CHD, the application of MRI to the fetal heart has been limited
because of the small size of fetal cardiac structures, random fetal motion, and the challenge
of gating the rapidly beating fetal heart in the absence of a fetal electrocardiogram.
Furthermore, in contrast to conventional ultrasound technology, MRI requires expensive,
large, less portable equipment, as well as specialized expertise to perform and interpret.
Nevertheless, MRI offers several advantages over obstetric ultrasound. Fetal position, rib
calcification, maternal obesity, and oligohydramnios, particularly during the third trimester,
interfere more with ultrasound imaging than with MRI. If the challenges relating to motion and
cardiac gating can be overcome, MRI has the potential to provide high-resolution imaging of
the fetal heart in multiple planes and to generate volume data sets with greater resolution
than those obtained with ultrasound, offering the potential to provide robust quantitative
evaluation of cardiac function and chamber volumes and to provide unique perspectives on
venous and arterial anatomy, visceroatrial situs, and thoracic extracardiac malformations
affecting fetal cardiovascular structure/function.


Lucia Manganaro
Department of Radiological Sciences
Policlinico Umberto I Hospital, “Sapienza” University of Rome