2004 gen med
DESCRIPTION
2004 Gen MedTRANSCRIPT

2004 gen med
48.
Ans: A: epinephrine 1: 1000
Ref: harrison 17/ e – pg 117, KDT,6/E- Pg 130
Exp: adrenaline is a life saving drug in anaphylaxis and given 0. 2 – 0.5 mg SC/ IM . It not only increases BP but also counteracts bronchospasm or laryngeal edema and hence the choice of drug in anaphylaxis( Type I hypersensitivity reaction).
Additional info: a detailed description is given in 2005 gen med paper- Q-41.
49.
Ans:C: excessive sweating
Ref: harrison 17/ e- pg 5
Exp:Although all options are correct but minmal losses is likely to occur in sweating compared to the other options given.hence the chopice of answer.
Additional info:
Hyponatremia:
Hyponatremia This is defined as a serum [Na+] <135 mmol/L and is among themost common electrolyte abnormalities encountered in hospitalized pts.
Causes: Hyponatremia is almost always the result of an increase in circulating AVP and/or increased renal sensitivity to AVP;
hyponatremia is primarily a disorder of H2Ohomeostasis.
Pts with hyponatremia are thus categorized diagnostically into three groups, depending on their clinical volume status: hypovolemic, euvolemic, and hypervolemic hyponatremia All three forms of hyponatremia share an exaggerated, “nonosmotic” increase in circulating AVP, in the setting of reduced serum osmolality.
Notably, hyponatremia is often multifactoria land include drugs, pain, nausea, and strenuous exercise.
Table 2-1 describes the diagnostic approach for the types of hyponatremia.( harrison 17/ e pg 5)
Symptomsinclude nausea, vomiting, confusion, lethargy, and disorientation; if severe (<120mmol/L) and/or abrupt, seizures, central herniation, coma, or death may result .
Hypovolemic Hyponatremia .Hypovolemia causes profound neurohumoral activation, inducing systems that preserve effective circulating volume, such as the renin-angiotensin-aldosterone axis (RAA), the sympathetic nervous system, and AVP.
The increase in circulating AVP serves to increase the retention of ingested free H2O, leading to hyponatremia.
The optimal treatment of hypovolemic hyponatremia is volume administration, generally as isotonic crystalloid, i.e., 0.9% NaCl (“normal ”). If the history suggests that hyponatremia has been “chronic,” i.e., present for 48 hours, care should be taken to avoid overcorrectionHypervolemic Hyponatremia:
The edematous disorders, are often associated with mild to moderate degrees of hyponatremia .
The pathophysiology is similar to that in hypovolemic hyponatremia, except that “effective circulating volume” is decreased due to the specific etiologic factors, i.e., cardiac dysfunction, peripheral vasodilation in cirrhosis, and hypoalbuminemia in nephroticsyndrome. The degree of hyponatremia is an indirect index of the associatedneurohumoral activation and an important prognostic indicator in hypervolemic hyponatremia.
Management consists of treatment of the underlying disorder (e.g., afterloadreduction inulatory therapy in some forms of nephrotic syndrome), Na+ restriction, diuretic therapy, and, in some pts, H2O restriction. Vasopressin antagonists (e.g., tolvaptan and conivaptan) are also effective in normalizing hyponatremia associatedwith both cirrhosis and CHF.
Euvolemic Hyponatremia The syndrome of inappropriate ADH secretion (SIADH) characterizes most cases of euvolemic hyponatremia. notably,
repletion of the glucocorticoid levels may cause a rapid drop in circulating AVP levels and overcorrection of serum [Na+] .
Optimal treatment of euvolemic hyponatremia includes treatment of theunderlying disorder. H2O restriction to <1 L/d is a cornerstone of therapy but maybe ineffective or poorly tolerated. However, vasopressin antagonists are predictablyeffective in normalizing serum [Na+] in SIADH. Alternatives include thecoadministration of loop diuretics to inhibit the countercurrent mechanism and reduceurinary concentration, combined with oral salt tablets to abrogate diuretic-inducedsalt loss and attendant hypovolemia.
Acute Symptomatic Hyponatremia
Acute symptomatic hyponatremia is a medical emergency; a sudden drop in serum [Na+] can overwhelm the capacity of the brain to regulate cell volume, leading to cerebral edema, seizures, and death.
Women, particularly premenopausal women, are particularly prone to such sequelae;neurologic consequences are comparatively rare in male pts.
Many of these pts develop hyponatremia from iatrogenic causes, including hypotonic fluids in the postoperative period.
Severe symptoms may occur. Nausea and vomiting are common premonitory symptoms of more severe sequelae. An important concomitant is respiratory failure, whichmay be hypercapnic due to CNS depression or normocapnic due to neurogenic,noncardiogenic pulmonary edema.
Diagnosis:Laboratory investigation of a pt with hyponatremia should include a measurement of serum osmolality.Serum glucose also should be measured; Serum Na+ falls by 1.4 mM for every 100-mg/dL increase in glucose, due to glucoseinduced H2O efflux from cells.
Hyperkalemia may suggest adrenal insufficiency or hypoaldosteronism;
increased blood urea nitrogen (BUN) and creatinine may suggest a renal cause.
Urine electrolytes and osmolality are also critical tests in the initial evaluation of hyponatremia Urine osmolality <100 mosmol/kg is suggestive of polydipsia or, inrare cases, of decreased solute intake; urine osmolality >400 mosmol/kg suggeststhat AVP excess is playing a more dominant role, whereas intermediatevalues are more consistent with multifactorial pathophysiology (e.g., AVP excesswith a component of polydipsia).
Finally, in the right clinical setting, thyroid, adrenal, and pituitary function should also be tested
Treatment: Three considerations are critical in the therapy of hyponatremia. First, the presence, absence, and/or severity of symptoms determine the urgency oftherapy (see above for acute symptomatic hyponatremia).
Second, pts withhyponatremia that has been present for >48 h (“chronic hyponatremia”) are at risk for osmotic demyelination syndrome, typically central pontine myelinolysis,if serum Na+ is corrected by >10–12 mM within the first 24 h and/or by >18 mM within the first 48 h.
Third, the response to interventions, such as hypertonic saline or vasopressin antagonists, can be highly unpredictable, such that frequent monitoring of serum Na+ (every 2–4 h) is imperative.
Treatment of acute symptomatic hyponatremia should include hypertonicsaline to acutely increase serum Na+ by 1–2 mM/h to a total increase of 4–6mM; this increase is typically sufficient to alleviate acute symptoms, after serum [Na+] should be monitored every 2–4 h during and after treatment with hypertonic saline.
The administration of supplemental O2 and ventilatory support can also be critical in acute hyponatremia. Vasopressin antagonists are highly effective in SIADH and in hypervolemic hyponatremia due to heart failure or cirrhosis.close monitoring of the response of serum [Na+] is essential to adjust therapy.
Also note:Bailey and love surgery- 25/ e- pg 226

The following are the approximate daily requirements of some electrolytes in adults:• sodium: 50–90mMday–1;• potassium: 50mMday–1;• calcium: 5mMday–1;• magnesium: 1mMday
50.Ans: B: acidic urine excretionRef: Harrison 17 / e- pg 20Exp:persistent vomiting causes hypocholeremia , hypokalemia, hypoventilation metabolic alkalosis with paradoxical acidic urine excretion. Thus both B and C are alternatives. Hypocholeremia is found in both initial as well as compensatory phase but paradoxiacal aciduria exists only when there is severe hypokalemia. Since the question specifically asks about the likely event B is the choice of answer.
Additional info:
Metabolic alkalosis:
Metabolic alkalosis is due to a primary increase in serum [HCO3 –], distinguished from chronic respiratory acidosis—with a compensatory increase in renal HCO3 –reabsorption—by the associated increase in arterial pH (normal or decreased in chronic respiratory acidosis).
Causes and patho phsiology:
Administered, exogenous alkali (HCO3–, acetate, citrate, or lactate) may cause alkalosis if the normal capacity to excrete HCO3 – is reduced or if renal HCO3– reabsorption is enhanced.
Metabolic alkalosis is primarily caused by renal retention of HCO3 – and isdue to a variety of underlying mechanisms. Pts are typically separated into twomajor subtypes: Cl–-responsive and Cl–-resistant. Measurement of urine Cl– affordsthis separation in the clinical setting .
persistent vomiting produces loss of fluid with high chloride and hydrogen ion concentration, hypochlorermia in blood and excess bicarbonate accumulation ( metabolic alkalosis.

This contraction of ECF volume stimulates maximal reabsorption of sodium to maintain volume. Since there is less of chloride in glomerular filtrate for reabsorptiuon of sodium in the PCT ,more sodium must be absorbed in the distal tubule, where sodium reabsorption occurs in exchange of potassium and hydrogen ( if potassium is depleted).
Hypokalemia from continued vomiting and above exchange mechanism encourages exchange of hydrogen for sodium .since less potassium is available. If this continues, alkaline urine becomes acidic with excretion of hydrogen ions in it.
causes and the diagnostic approach is given in table 2-6 ( Harrison 17/ e – pg 19)most of these pts are hypokalemic, volume-expanded, and/or hypertensive.
Diagnosis:
Common forms of metabolic alkalosis are generally diagnosed from the history,physical examination, and/or basic laboratory tests.
ABGs will help determine whether an elevated [HCO3 –] is reflective of metabolic alkalosis or chronic respiratory acidosis; ABGs are required for the diagnosis of mixed acid-base disorders.
Measurement of urinary electrolytes will aid in separating Cl–-responsiveand Cl–-resistant forms. Urinary [Na+] may thus be >20 meq/L in Cl–-responsivealkalosis despite the presence of hypovolemia; however, urinary [Cl–] will bevery low.
Notably, urinary [Cl–] may be variable in pts with diuretic-associated alkalosis, depending on the temporal relationship to diuretic administration.
Other diagnostic tests—e.g., plasma renin, aldosterone, cortisol—may be appropriatein Cl–-resistant forms with high urinary [Cl–].
treatment:
The acid-base disorder in Cl–-responsive alkalosis will typically respond to saline infusion; however, the associated hypokalemia should also be corrected.
Pts with true or apparent mineralocorticoid excess require specific treatment to blockade of the mineralocorticoid receptor with spironolactone or eplerenone.
Finally, severe alkalosis in the critical care setting may require treatment with acidifying agents such as acetazolamide or HCl.
51.
Ans: C: idiopathic ipsilateral paralysis of the facial nerve.Ref: Harrison 17/ e- pg 1021Exp: bell s paralysis is an idiopathic lower motor neuron type of lesion of facial nerve of acute onset. pathogenesis is not known . Associated with herpes simplex lesion.
Additional info:
Bells palsy:
Most common form of idiopathic facial paralysis; affects 1 in 60 persons over a lifetime.
The facial nerve can be damaged at the cerebellopontine angle, within the internal auditory meatus, within the middle ear, at the skull base and within the parotid gland.
Association with herpes simplex virus type seen.
Clinical features and Symptoms:.
Onset is acute. Mild pain at stylomastoid foramen for a few days may precede the palsy.
Weakness evolves over 12–48 h, sometimes preceded by retroaural pain.
Hyperacusis may be present.
Paralysis of all the facial muscles of expression on the side of palsy.
Drooping of the corner of the mouth, creases and skin fold on the affected side.
Weakness of frowning and eye closure since the upper facial muscles are weak.
Deviation of the angle of mouth away from the side and drooping of saliva from the angle of the mouth.
On attempted closure of the eyelid , the eye on the paralysed side rolled upwards( bell phenomenon)
Diagnosis:Diagnosis can be made clinically in pts with (1) a typical presentation, (2) no risk factors or preexisting symptoms for other causes of facial paralysis, (3) no lesions of herpes zoster in the external ear canal, and (4) a normal neurologic examination with the exception of the facial nerve.
In uncertain cases, an ESR, testing for diabetes mellitus, a Lyme titer, angiotensin-converting enzyme level, and chest x-ray for possible sarcoidosis, a lumbar puncture for possible Guillain- Barre syndrome, or MRI scanning may be indicated.
Treatment:
Protect the eye with paper tape to depress the upper eyelid during sleep.
Prednisone (60–80 mg/d over 5 days, tapered off over the next 5 days) when startedearly appears to shorten the recovery period and modestly improve functional outcome. A recently published trial found no added benefit of acyclovir compared to prednisolone alone; the value of valacyclovir (usual dose 1000 mg/d for 5–7 days) is not known
prognosis:
Full recovery within several weeks or months in 80%; incomplete paralysis in first week is the most favorable prognostic sign. Older patients may show poor prognosis.
Also note:( harrisson 17/ e- pg 1021)
Ramsay Hunt syndrome is caused by herpes zoster infection of geniculate ganglion; distinguished from Bell’s palsy by a vesicular eruption in pharynx and external auditory canal, and by frequent involvement of eighth cranial nerveBilateral facial weakness may occur in Guillain-Barre syndrome, sarcoidosis, Lyme disease, and leprosy. Hemifacial spasm may occur with Bell’s palsy, irritative lesions (e.g., acoustic neuroma, basilar artery aneurysm, an aberrant vessel compressing the nerve), or as an idiopathic disorder.

Melkerrson Rosenthal syndrome has a triad of recurrent facial paralysis, facial edema and scrotal tongue.
52.Ans: A : loss of diurnal variationRef: cyclic cushings syndrome- a clinical challenge by-J R Meinardi,B H Wolffenbuttel and R P F DullaartExp: patients with cushings syndrome classically lack the normal circadian rhythm . In normal individuals the serum levels of cortisol reach their lowest levels at midnight. In patients with cushings disease , this diurnal variation is lost and serum levels of cortisol remain same throughout 24 hrs. levels of cortisol changes in urine and hence loss of diurnal variation is the earliest manifestation of cushings syndrome. This is used as a diagnostic protocol in cushings syndrome.
Additional info:
Cushings syndrome:
This disorder is caused by any condition that produces an elevation in glucocorticoid levels
Causes:
The most common cause of Cushing’s syndrome is iatrogenic, due to administration of glucocorticoids for therapeutic reasons.
Endogenous Cushing’s syndrome results from production of excess cortisol (and other steroid hormones) by the adrenal cortex.
The major cause is bilateral adrenal hyperplasia secondary to hypersecretion of adrenocorticotropic hormone (ACTH) by the pituitary (Cushing’s disease) or from ectopic sources such as small cell carcinoma of the lung; medullary carcinoma of the thyroid; or tumors of the thymus, pancreas, or ovary.
Adenomas or carcinoma of the adrenal gland account for about 25% of Cushing’s syndrome cases.
Clinical Features
Some common manifestations (central obesity, hypertension, osteoporosis psychological disturbances, acne, amenorrhea, and diabetes mellitus)are relatively nonspecific.
More specific findings include easy bruising, purple striae, proximal myopathy, fat deposition in the face and interscapular areas (moon facies and buffalo hump), and virilization.
Glucocorticoids induce gluconeogenesis and inhibit the uptake of glucose by cells, with resultant hyperglycemia, glucosuria, and polydipsia, mimicking diabetes mellitus.
The catabolic effects on proteins cause loss of collagen and resorption of bone. Thus, the skin is thin, fragile, and easily bruised; cutaneous striae are particularly common in the abdominal area. Bone resorption results in the development of osteoporosis, with consequent increased susceptibility to fractures.
Because glucocorticoids suppress the immune response, patients with Cushing syndrome are also at increased risk for a variety of infections.
Additional manifestations include hirsutism and menstrual abnormalities, as well as a number of mental disturbances, including mood swings, depression, and frank psychosis.
Extra-adrenal Cushing syndrome caused by pituitary or ectopic ACTH secretion is usually associated with increased skin pigmentation, because of melanocyte-stimulating activity in the ACTH precursor molecule.
Hypokalemia and metabolic alkalosis are prominent, particularly with ectopic production of ACTH.
Microscopical feature: The morphologic features in the adrenal include bilateral cortical atrophy (in exogenous steroid-induced disease), bilateral diffuse or nodular hyperplasia (most common finding in endogenous Cushing syndrome), or an adrenocortical neoplasm.
Diagnosis
The diagnosis of Cushing’s syndrome requires demonstration of increasedcortisol production and abnormal cortisol suppression in response to dexamethasone.

For initial screening, measurement of 24-h urinary free cortisol, the 1-mg overnight dexamethasone test [8 A.M. plasma cortisol < 1.8 g/dL (50 nmol/L)] or late night salivary cortisol measurement is appropriate.
Repeat testing or performance of more than one screening test may be required.
Definitive diagnosis is established in equivocal cases by inadequate suppression ofurinary [<10 g/d (25 nmol/d)] or plasma cortisol [<5 g/dL (140 nmol/L)] after0.5 mg dexamethasone every 6 h for 48 h.
This test may also be combined with corticotropin-releasing hormone (CRH) testing to rule out pseudo-Cushing’s states.
Once the diagnosis of Cushing’s syndrome is established, further biochemical testing is required to localize the source.
Low levels of plasma ACTH levels suggest an adrenal adenoma or carcinoma; inappropriately normal or high plasma ACTH levels suggest a pituitary or ectopic source. In 95% of ACTH-producing pituitary microadenomas, cortisol production is suppressed by high-dose dexamethasone (2 mg every 6 h for 48 h), and MRI of thepituitary should be obtained.
However, because up to 10% of ectopic sources of ACTH may also suppress after high-dose dexamethasone testing, inferior petrosal sinus sampling may be required to distinguish pituitary from peripheral sources of ACTH. Imaging of the chest and abdomen is required to localize the source of ectopic ACTH production.
Pts with chronic alcoholism and depression may have false-positive results in testing for Cushing’s syndrome.
Similarly, pts with acute illness may have abnormal laboratory test results, since major stress disrupts the normal regulation of ACTH secretion.
Treatment:
Therapy of adrenal adenoma or carcinoma requires surgical excision;
stress doses of glucocorticoids must be given pre- and postoperatively.
Metastatic and unresectable adrenal carcinomas are treated with mitotane in doses gradually increased to 6 g/d in three or four divided doses.
Transsphenoidal surgery can be curative for pituitary microadenomas that secrete ACTH, though radiation may be used when cure is not achieved .,debulking of lung carcinoma or resection of carcinoid tumors can result in remission of ectopic Cushing’s syndrome.
If the source of ACTH cannot be resected, bilateral total adrenalectomy or medical management with ketoconazole (600–1200 mg/d), metyrapone (2–3 g/d), or mitotane (2–3 mg/d) may relieve manifestations of cortisol excess. Patients with unresectable pituitary adenomas who have bilateral adrenalectomy are at risk for Nelson’s syndrome(pituitary adenoma enlargement).
53.Ans: D: congenital adrenal hyperplasia.Ref: harrison 17/ e- pg 926, robins path 8/ e- pg – 760, WHO – 2002 articleexp: hypothyroidism, protein energy malnutrition all are associated with retardation and maturation of skeletal maturity.congenital adrenal hyperplasia is aassociated with obesity and increased glucocorticoids in the blood and therefore increases maturation of the skeleton. Hence D is the choice of answer.
Additional info:
Lets have a review of the choicesHypothyroidism:
Hypothyroidism is caused by any structural or functional derangement that interferes with the production of adequate levels of thyroid hormone.
Causes: table- robins path- 8/e – pg 760
The clinical manifestations of hypothyroidism include cretinism and myxedema.
Cretinism refers to hypothyroidism developing in infancy or early childhood.
This disorder was formerly fairly common in areas of the world where dietary iodine deficiency is endemic,
It has now become much less frequent because of the widespread supplementation of foods with iodine.
On rare occasions cretinism may also result from inborn errors in metabolism (e.g., enzyme deficiencies) that interfere with the biosynthesis of normal levels of thyroid hormone (sporadic cretinism).
Clinical features of cretinism include impaired development of the skeletal system and central nervous system, with severe mental retardation, short stature, coarse facial features, a protruding tongue, and umbilical hernia.
The severity of the mental impairment in cretinism seems to be directly influenced by the time at which thyroid deficiency occurs in utero.
Normally, maternal hormones that are critical to fetal brain development, including T3 and T4, cross the placenta. If there is maternal thyroid deficiency before the development of the fetal thyroid gland, mental retardation is severe.
In contrast, reduction in maternal thyroid hormones later in pregnancy, after the fetal thyroid has developed, allows normal brain development.
Hypothyroidism developing in older children and adults results in a condition known as myxedema.
Myxedema, or Gull disease, was first linked with thyroid dysfunction in 1873 by Sir William Gull in a paper addressing the development of a "cretinoid state" in adults.
Manifestations of myxedema include generalized apathy and mental sluggishness that in the early stages of disease may mimic depression.
Individuals with myxedema are resttless, cold intolerant, and often obese.
Mucopolysaccharide-rich edema accumulates in skin, subcutaneous tissue, and a number of visceral sites, with resultant broadening and coarsening of facial features, enlargement of the tongue, and deepening of the voice.
Bowel motility is decreased, resulting in constipation.
Pericardial effusions are common; in later stages the heart is enlarged, and heart failure may supervene. Diagnosis:
Table in Harrison 17/ e- pg 927
Laboratory evaluation has a vital role in the diagnosis of suspected hypothyroidism because of the nonspecific nature of symptoms.
Measurement of the serum TSH is the most sensitive screening test for this disorder.
The serum TSH is increased in primary hypothyroidism because of a loss of feedback inhibition of thyrotropin-releasing hormone (TRH) and TSH production by the hypothalamus and pituitary, respectively.
The TSH concentration is not increased in persons with hypothyroidism caused by primary hypothalamic or pituitary disease. Serum T4 is decreased in individuals with hypothyroidism of any origin.
Treatment:
Adult pts <60 years without evidence of heart disease may be started on 50–100g of levothyroxine (T4) daily. In the elderly or in pts with known coronary arterydisease, the starting dose of levothyroxine is 12.5–25 g/d.
The dose should be adjusted in 12.5- to 25-g increments every 6–8 weeks on the basis of TSH levels, until a normal TSH level is achieved.
The usual daily replacement 13 dose is 1.6 (g/kg)/d. Women on levothyroxine replacement should have a TSH level checked as soon as pregnancy is diagnosed, as the replacement dose typically increases by 30–50% during pregnancy.
Failure to recognize and treat maternal hypothyroidism may adversely affect fetal neural development.
Therapy for myxedema coma should include levothyroxine (500 g) as a single IV bolus followed by daily treatment with levothyroxine (50–100 g/d), along with hydrocortisone (50 mg every 6 h) for impaired adrenal reserve, ventilatory support,space blankets, and therapy of precipitating factors.
Protein energy malnutrition(PEN) Protein–energy malnutrition (or protein–calorie malnutrition) refers to a form of malnutrition where there is inadequate protein intake.
Types include:
Kwashiorkor (protein malnutrition predominant) Marasmus (deficiency in calorie intake) Marasmic Kwashiorkor (marked protein deficiency and marked calorie
insufficiency signs present, sometimes referred to as the most severe form of malnutrition)
Note that this may also be secondary to other conditions such as chronic renal disease or cancer cachexia in which protein energy wasting may occur.
Protein–energy malnutrition affects CH Protein malnutrition is detrimental at any point in life, but protein malnutrition prenatally has been shown to have significant lifelong effects. During pregnancy, diet that consists at least 20% protein for the health of the fetus. The following are some studies in which prenatal protein deficiency has been shown to have unfavorable consequences.
Decreased brain size: Protein deficiency has been shown to affect the size and composition of brains
Impaired neocortical long-term potentiation: Mild protein deficiency (in which 7.2% of the diet consists of protein) impair entorhinal cortex plasticity (visuospatial memory), noradrenergic function in the neocortex, and neocortical long-term potentiation
Altered fat distribution:
Increased obesity: the prenatally undernourished mice were shown to have increased body weight and adiposity (body fat), while those who were adequately nourished prenatally did not show an increase in body weight or adiposity when fed the same high-fat diet after birth.

Decreased birth weight, and gestation duration: Supplementation of protein and energy can lead to increased duration of gestation and higher birth weight. When fed a supplement containing protein, energy, and micronutrients, pregnant women showed more successful results during birth, including high birth weights, longer gestations, and fewer pre-term births, than women who had consumed a supplement with micronutrients and low energy but no protein (although this finding may be due to the increase of energy in the supplements, not the increase of protein).
Increased stress sensitivity: Male offspring of pregnant rats fed low-protein diets have been shown to exhibit blood pressure that is hyperresponsive to stress and salt.
Decreased sperm quality: A low-protein diet during gestation in rats has been shown to affect the sperm quality of the male offspring in adulthood. The protein deficiency appeared to reduce sertoli cell number, sperm motility, and sperm count.
Altered cardiac energy metabolism: Prenatal nutrition, specifically protein nutrition, may affect the regulation of cardiac energy metabolism through changes in specific genes.
Increased passive stiffness: Intrauterine undernutrition was shown to increase passive stiffness in skeletal muscles in rats.]
it is possible to conclude that prenatal protein nutrition is vital to the development of the fetus, especially the brain, the susceptibility to diseases in adulthood, and even gene expression.. These findings highlight the great significance of adequate protein in the prenatal diet.
54Ans: A: jod basedow effect:Ref: bailey and love surgery 8 / e- pg 788Exp:Jod basedow effect is iodine induced hyper thyroidism and occurs in patients with multinodular goiter after intake of large amount of iodine in the diet, radiographic contrast material or drug amiodarone and is seen as endemic in European countries. In European countries diffuse toxic goitre is often called Basedow’s disease or Jod–Basedow
thyrotoxicosis (Jod = German for iodine + Basedow). Large doses of iodide given to a hyperplastic endemic goitre that is iodine avid may produce temporary hyperthyroidism and, very occasionally, persistent hyperthyroidismWolff chaikoff effect – excess iodine inhibits ithyroid iodide organification. This phenomenon of iodine dependent transient suppression of thyroid is called wolff chaikoff effect Thyrotoxicosis factitia: Hyperthyroidism may be induced by taking thyroxine, but only ifthe dosage exceeds the normal requirements of 0.15–0.25 mg /day.epidemics have been caused by consumption of ground beef contaminated with bovine thyroid gland.
De Quervain s thyroiditis: form of autoimmune thyroiditis . mild hyperthyroidism may occur in the early stages because of the liberation of thyroid hormones from damaged tissue.
additional info:
thyrotoxicosis/ hyperthyroidism: Its a hypermetabolic state which shows increased circulating thyroid harmones.
Etiology
Causes of thyroid hormone excess include primary hyperthyroidism(Graves’ disease, toxic multinodular goiter, toxic adenoma, iodine excess); thyroiddestruction (subacute thyroiditis, silent thyroiditis, amiodarone, radiation);extrathyroidal sources of thyroid hormone (thyrotoxicosis factitia, struma ovarii,functioning follicular carcinoma); and secondary hyperthyroidism [TSH-secreting pituitary adenoma, thyroid hormone resistance syndrome, human chorionic gonadotropin (hCG)-secreting tumors, gestational thyrotoxicosis].
Clinical Features: Symptoms include nervousness, irritability, heat intolerance, excessive sweating, palpitations, fatigue and weakness, weight loss with increased appetite, frequent bowel movements, and oligomenorrhea.
Pts are anxious, restless, and fidgety. Skin is warm and moist, and fingernails may separate from the nail bed (Plummer’s nails). Eyelid retraction and lid lag may be present.

Cardiovascular findings include tachycardia, systolic hypertension, systolic murmur, and atrial fibrillation
A fine tremor, hyperreflexia, and proximal muscle weakness may also be present.
Long-standing thyrotoxicosis may lead to osteopenia.
In Graves’ disease, the thyroid is usually diffusely enlarged to two to three times its normal size, and a bruit or thrill may be present.
Infiltrative ophthalmopathy (with variable degrees of proptosis, periorbital swelling, and ophthalmoplegia) and dermopathy (pretibial myxedema) may also be found.
In subacute thyroiditis, the thyroid is exquisitely tender and enlarged with referred pain to the jaw or ear, and sometimes accompanied by fever and preceded by an upper respiratory tract infection. Solitary or multiple nodules may be present in toxic adenoma or toxic multinodular goiter.
Thyrotoxic crisis, or thyroid storm, is rare, presents as a life-threatening exacerbationof hyperthyroidism, and can be accompanied by fever, delirium, seizures,arrhythmias, coma, vomiting, diarrhea, and jaundice.
Diagnosis
Table 19-2( Harrison 17/ e – pg 929 Serum TSH is a sensitive marker of thyrotoxicosis caused by Graves’ disease, autonomous thyroid nodules, thyroiditis, and exogenous levothyroxine treatment.
Associated laboratory abnormalities include elevation of bilirubin, liver enzymes, and ferritin. Radionuclide uptake may be required to distinguish the various etiologies:
high uptake in Graves’ disease and nodular disease vs. low uptake in thyroid destruction, iodine excess, and extrathyroidal sources of thyroid hormone. The ESR is elevated in subacute thyroiditis.
Treatment:
Graves’ disease may be treated with antithyroid drugs or radioiodine;
Subtotal thyroidectomy is rarely indicated.

The main antithyroid drugs are methima zole or carbimazole (10–20 mg two to three times a day initially, titrated to 2.5–10 mg/d) and propylthiouracil (100–200 mg every 8 h initially, titrated to 50 mg once or twice a day).
Thyroid function tests should be checked 3–4 weeks after initiation of treatment, with adjustments to maintain a normal free T4 level. The common side effects are rash, urticaria, fever, and arthralgia (1– 5% of pts). Rare but major side effects include hepatitis, an SLE-like syndrome, and agranulocytosis (<1%). All pts should be given written instructions regarding the symptoms of possible agranulocytosis (sore throat, fever, mouth ulcers) and the need to stop treatment pending a complete blood countto confirm that agranulocytosis is not present.
Propranolol (20–40 mg every 6 h) or longer acting beta blockers such as atenolol (50 mg/d) may be useful to control adrenergic symptoms. Anticoagulation with warfarin should be considered in all pts with atrial fibrillation.
Radioiodine can also be used as initial treatment or in pts who do not undergo remission after a 1- to 2-year trial of antithyroid drugs. Antecedent treatment with antithyroid drugs should be considered in elderly pts and those with cardiac problems, with cessation of antithyroid drugs 3–5 days prior to radioiodine administration.
Radioiodine treatment is contraindicated in pregnancy; instead, symptoms should be controlled with the lowest effective dose of propylthiouracil (PTU).
Corneal drying may be relieved with artificial tears and taping the eyelids shut duringsleep. Progressive exophthalmos with chemosis, ophthalmoplegia, or visionloss is treated with large doses of prednisone (40–80 mg/d) and ophthalmologicreferral; orbital decompression may be required.
In thyroid storm, large doses of PTU (600-mg loading dose) should be administeredorally, per nasogastric tube, or per rectum, followed 1 h later by 5 drops saturated solution of KI (SSKI) q6h. PTU (200–300 mg every 6 h) should be continued, along with propranolol (40–60 mg PO q4h or 2 mg IV every 4 h) and dexamethasone (2 mg every 6 h).
Any underlying precipitating cause should be identified and treated.
Radioiodine is the treatment of choice for toxic nodules.

Subacute thyroiditis should be treated with NSAIDs and beta blockade to control symptoms, with monitoring of the TSH and free T4 levels every 4 weeks.
Transient levothyroxine replacement (50–100 g/d) may be required if the hypothyroidphase is prolonged. Silent thyroiditis (or postpartum thyroiditis if within 3–6 months of delivery) should be treated with beta blockade during the thyrotoxic phase and levothyroxine in the hypothyroid phase, with withdrawal after 6– 9 months to assess recovery.Also note:
Thyrotoxicosis : other causes:
Thyrotoxicosis factitia.Jod–Basedow thyrotoxicosis.Subacute/acute forms of autoimmune thyroiditis or ofde Quervain’s thyroiditis. described above
Secondary carcinomaA large mass of secondary carcinoma will rarely produce sufficient hormone to induce mild hyperthyroidism.
Neonatal thyrotoxicosisNeonatal thyrotoxicosis occurs in babies born to hyperthyroid mothers or to euthyroid mothers who have had thyrotoxicosis. High TSH-RAb titres are present in both mother and child because TSH-RAbs can cross the placental barrier.
55.Ans: B: lebers hereditary optic neuropathy Ref: net sourcesExp:
Retinopathy of prematurity (ROP) or Terry syndrome, previously known as retrolental fibroplasia (RLF), is a disease of the eye affecting prematurely-born babies is thought to be caused by disorganized growth of retinal blood vessels which may result in scarring and retinal detachment. ROP can be mild and may resolve spontaneously, but it may lead to blindness in serious cases

Retinitis pigmentosa (RP) is an inherited, degenerative eye disease that causes severe vision impairment and often blindness
Retinal detachment is a disorder of the eye in which the retina peels away from its underlying layer of support tissue. Initial detachment may be localized, but without rapid treatment the entire retina may detach, leading to vision loss and blindness. It is a medical emergency.
Leber’s hereditary optic neuropathy (LHON) or Leber optic atrophy is a mitochondrially inherited (transmitted from mother to offspring) degeneration of retinal ganglion cells (RGCs) and their axons that leads to an acute or subacute loss of central vision and hence the choice of answer.
Additional info:
Leber’s hereditary optic neuropathy (LHON) or Leber optic atrophy is a mitochondrially inherited (transmitted from mother to offspring) degeneration of retinal ganglion cells (RGCs) and their axons that leads to an acute or subacute loss of central vision
It affects predominantly young adult males.
However, LHON is only transmitted through the mother as it is primarily due to mutations in the mitochondrial (not nuclear) genome and only the egg contributes mitochondria to the embryo.
LHON is usually due to one of three pathogenic mitochondrial DNA (mtDNA) point mutations. These mutations are at nucleotide position of complex I of the oxidative phosphorylation chain in mitochondria.
Clinical features:
Clinically, there is an acute onset of visual loss, first in one eye, and then a few weeks to months later in the other.
Onset is usually young adulthood, and age range at onset from 7-75.
The age of onset is slightly higher in females (range 19–55 years: mean 31.3 years) than males (range 15–53 years: mean 24.3).

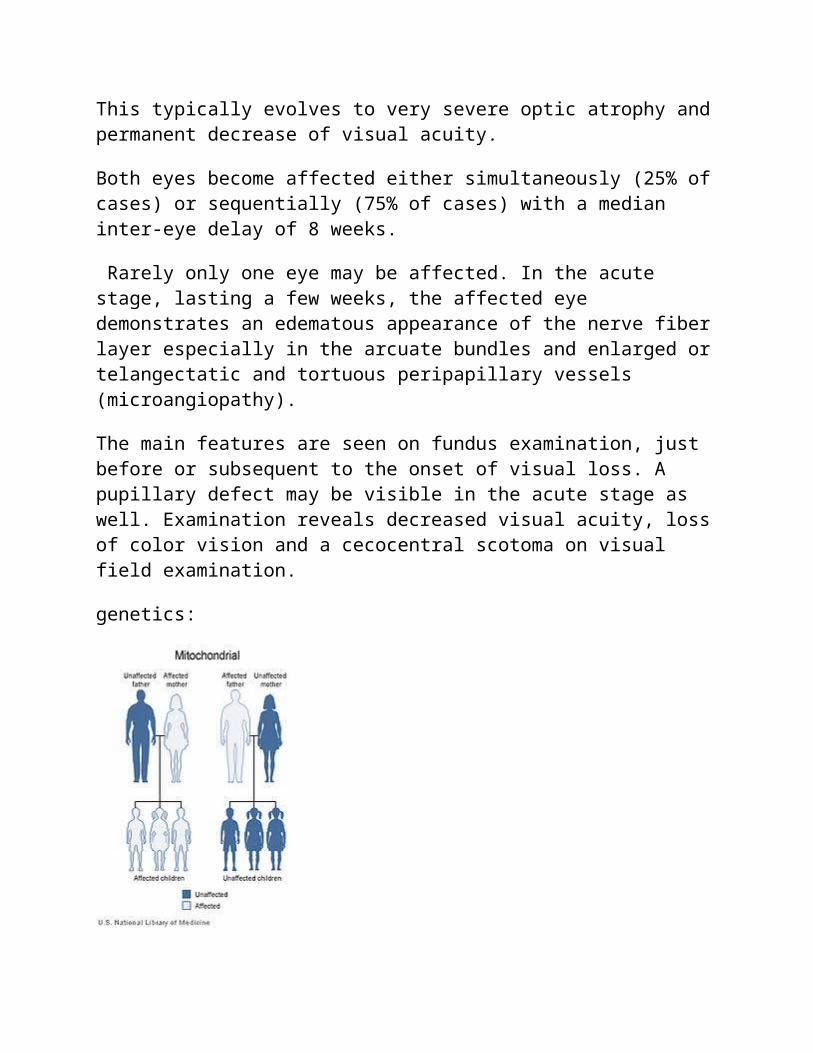
This typically evolves to very severe optic atrophy and permanent decrease of visual acuity.
Both eyes become affected either simultaneously (25% of cases) or sequentially (75% of cases) with a median inter-eye delay of 8 weeks.
Rarely only one eye may be affected. In the acute stage, lasting a few weeks, the affected eye demonstrates an edematous appearance of the nerve fiber layer especially in the arcuate bundles and enlarged or telangectatic and tortuous peripapillary vessels (microangiopathy).
The main features are seen on fundus examination, just before or subsequent to the onset of visual loss. A pupillary defect may be visible in the acute stage as well. Examination reveals decreased visual acuity, loss of color vision and a cecocentral scotoma on visual field examination.
genetics:
Leber’s hereditary optic neuropathy has a mitochondrial inheritance pattern.
Leber hereditary optic neuropathy is a condition related to changes in mitochondrial DNA. Although most DNA is packaged in chromosomes within the nucleus, mitochondria have a distinct mitochondrial genome composed of mtDNA.
Mutations in the MT-ND1, MT-ND4, MT-ND4L, and MT-ND6 genes cause Leber hereditary optic neuropathy. These genes code for the NADH dehydrogenase protein involved in the normal mitochondrial function of oxidative phosphorylation.
Oxidative phosphorylation uses a series of four large multienzyme complexes, which are all embedded in the inner mitochondrial membrane to convert oxygen and simple sugars to energy.
Mutations in any of the genes disrupt this process to cause a variety of syndromes depending on the type of mutation and other factors. It s unclear how these genetic changes cause the death of cells in the optic nerve and lead to the specific features of Leber hereditary optic neuropathy.
Pathophysiology
The eye pathology is limited to the retinal ganglion cell layer especially the maculopapillary bundle.
Degeneration is evident from the retinal ganglion cell bodies to the axonal pathways leading to the lateral geniculate nucleii.
Experimental evidence reveals impaired glutamate transport and increased reactive oxygen species (ROS) causing apoptosis of retinal ganglion cells.
The normal non LHON affected retinal ganglion cells produce less of the potent superoxide radical than other normal central nervous system neurons. Viral vector experiments which augment superoxide dismutase 2 in LHON cybrids or LHON animal models or use of exogenous glutathione in LHON cybrids have been shown to rescue LHON affected retinal ganglion cells from apoptotic death. .
Diagnosis
known family history of LHON.
the diagnosis usually requires a neuro-ophthalmological evaluation and blood testing for mitochondrial DNA assessment.
It is important to exclude other possible causes of vision loss and important associated syndromes such as heart electrical conduction system abnormalities.
Management:
Regular corrected visual acuity and perimetry checks are advised for follow up of affected individuals. There is beneficial treatment available for some cases of this disease especially for early onset disease.
Also, experimental treatment protocols are in progress.
Genetic counselling should be offered. Health and lifestyle choices should be reassessed particularly in light of toxic and nutritional theories of gene expression. Vision aides assistance and work rehabilitation should be used to assist in maintaining employment.
For those who are carriers of a LHON mutation, preclinical markers may be used to monitor progress.
For example fundus photography can monitor nerve fiber layer swelling.
Optical coherence tomography can be used for more detailed study of retinal nerve fiber layer thickness. Red green color vision testing may detect losses.
Contrast sensitivity may be diminished. There could be an abnormal electroretinogram or visual evoked potentials. Neuron-specific enolase and axonal heavy chain neurofilament blood markers may predict conversion to affected status.
Cyanocobalamin (a form of B12) should be avoided as it may lead to blindness in Leber's disease patients.
Avoiding optic nerve toxins is generally advised, especially tobacco and alcohol.
Certain prescription drugs are known to be a potential risk, so all drugs should be treated with suspicion and checked before use by those at risk. Ethambutol, in particular, has been implicated as triggering visual loss in carriers of LHON.
In fact, toxic and nutritional optic neuropathies may have overlaps with LHON in symptoms, mitochondrial mechanisms of disease and management.
Of note, when a patient carrying or suffering from LHON or toxic/nutritional optic neuropathy suffers a hypertensive crisis as a possible complication of the disease
process, nitroprusside (trade name: Nipride) should not be used due to increased risk of optic nerve ischemia in response to this anti-hypertensive in particular.[26]
Idebenone has been shown in a small placebo controlled trial to have modest benefit in about half of patients. People most likely to respond best were those treated early in onset.
α-Tocotrienol-quinone, a vitamin E metabolite, has had some success in small open label trials in reversing early onset vision loss.
There are various treatment approaches which have had early trials or are proposed, none yet with convincing evidence of usefulness or safety for treatment or prevention including brimonidine, minocycline curcumin, glutathione, near infrared light treatment, and viral vector techniques.
56.
Ans: D: MEN II B
Ref: shafers oral pathology-5/e – pg 278
Exp:The association of medullary carcinoma , thyroid and pheochromocytoma , with mucosal neuromas and marinoid habitus is MEN II B. MEN I syndrome is associated with parathyroid , pituitary , pancreatic cell tumour . MEN II is associated with medullary carcinoma, pheochromocytoma, whereas parathyroid hyperplasia is specific for MEN II A, mucosal neuromas and marfinoid habitus are the most distinguishing feature in MEN II B. hence the choice of answer.
Additional info:
MEN stands for "Multiple Endocrine Neoplasia". The term multiple endocrine neoplasia (MEN) encompasses several distinct syndromes featuring tumors of endocrine glands, each with its own characteristic pattern. In some cases, the tumors are malignant, in others, benign. Benign or malignant tumors of nonendocrine tissues occur as components of some of these tumor syndromes.
MEN syndromes are inherited as autosomal dominant disorders. When they are inherited, they are passed from one generation to the next.
There are three main types of multiple endocrine neoplasia (MEN) - MEN 1, MEN 2a and MEN 2b. Each type of MEN is associated with a specific cluster of illnesses. Physicians use the term "syndrome" when clinical diseases

come in groups of three. Each of the three types of MEN syndromes, therefore, have three diseases. The main health problems in each of the MEN syndromes are:
MEN 1 = Parathyroid tumors, pancreatic tumors, and pituitary tumors. MEN 2a = Medullary thyroid cancers (MTC), pheochromocytoma, and parathyroid tumors. MEN 2b = Medullary thyroid cancers, pheochromocytoma and neuromas and marfinus habitus.
MEN II B / MEN III.
The MEN syndromes are xharacterised by tumours of neuro- endocrine origin. The type MEN III syndrome also called MEN II B was initially described by wagemann in 1922.
The disease is associated with adrenal pheochromocytoma, medullary carcinoma of thyroid, diffuse alimentary tract ganglioneuromatosis and multiple small submucosal neuroma nodules of the upper digestive tract .
Clinical features:
The affected individual has atall, lanky, marfinoid body type with a narrow face and muscle wasting.
The adrenal and thyroid tumours typically donot present until after puberty while the mucosal neuromas usually develop during the first decade of life. Mucosal neuromas are extremely rare
Genetics:
MEN syndromes are caused by mutations of the RET proto-oncogene an important regulator of neural crest deveelopment and the receptor of gliaderiaved neurotrophic factor( GDNF)
Oral manifestations:
The oral mucosal neuroma of this disease presents as a 2-7mm yellowish sessile , painless nodule of the lips, anterior tongue and buccal commissures.
The neuromas in the body of the lips produce enlargement and a bumpy lip appearance
Facial skin around the nose is involved.
Histological features:
The mucosal neuroma is compromised of a partially encapsulated aggregation or proliferation of nerves , often with thickened perineurium, intertwined with one another in a plexiform pattern. No inflammatory cells seen.
Lab findings:
Serum and urinary calcitonin levels are elevated ( medullary carcinoma of thyroid)
Serum levels of vanillyl mandelic acid is increased and altered epinephrine / noerepinephrine ratios( pheochromocytoma)
Treatment :
The mucosal neuromas are asymptomatic and self limiting and present no problem requiring treatment. They may be surgically removed for esthetic purposes , if traumatised
57.
Ans: D: hemochromatosis
Ref: Harrison 17. E pg 975
Exp: hemachromatosis is a disorder due to iron overload and the treatment modalities aim to reduce the iron content in the body and supportive therapy for the damaged organs. Bone marrow transplantation is not a treatment modality for hemochromatosis. Its indicated in osteopetrosis, hurlers syndrome and adrenoluekodystrophy. Hence D the choice of answer.
Additional info: Lets have a review of the other choices: Hemochromatosis:
Hemochromatosis is a disorder of iron storage that results in increased intestinaliron absorption with Fe deposition and damage to many tissues.
The classic clinical constellation of hemochromatosis is a patient presenting withbronze skin, diabetes, cardiac conduction abnormalities, and liver disease.
Two major causes of hemochromatosis exist: hereditary (due to inheritance of mutantHFE genes) and secondary iron overload (usually the result of disordered erythropoiesis). Alcoholic liver disease and chronic excessive Fe ingestion may also be associated with a moderate increase in hepatic Fe and elevated body Fe stores.
Clinical Features
Early symptoms include weakness, lassitude, weight loss, a bronze pigmentation or darkening of skin, abdominal pain, and loss of libido. Hepatomegaly occurs in 95% of pts, sometimes in the presence of normal LFTs. Other signs include spider angiomas, splenomegaly, arthropathy, ascites, cardiac arrhythmias, CHF, loss of body hair, palmar erythema, gynecomastia, and testicular atrophy. Diabetes mellitus occurs in about 65%, usually in pts with family history of diabetes. Adrenal insufficiency, hypothyroidism, and hypoparathyroidism rarely occur.Diagnosis Serum Fe, percent transferrin saturation, and serum ferritin levels are increased.
In an otherwise-healthy person, a fasting serum transferrin saturation > 50% is abnormal and suggests homozygosity for hemochromatosis.
In most untreated pts with hemochromatosis, the serum ferritin level is alsogreatly increased.\ If either the percent transferrin saturation or the serum ferritin level is abnormal, genetic testing for hemochromatosis should be performed.
All first-degree relatives of pts with hemochromatosis should be tested for the C282Y and H63D mutations. Liver biopsy may be required in affected
individuals to evaluate possible cirrhosis or to quantify tissue iron.
An algorithmfor evaluating pts with possible hemochromatosis is shown in Fig. 188-1.
Death in untreated pts results from cardiac failure (30%), cirrhosis (25%), andhepatocellular carcinoma (30%); the latter may develop despite adequate Fe removal.
Treatment:
Therapy involves removal of excess body Fe, usually by intermittent phlebotomy,and supportive treatment of damaged organs. Since 1 unit of blood contains~250 mg Fe, and since ≥25 g of Fe must be removed, phlebotomy isperformed weekly for 1–2 years.
Less frequent phlebotomy is then used to maintain serum Fe at <27 mol/L (<150 g/dL).
Chelating agents such as deferoxamine (infused SC using a portable pump) remove 10–20 mg iron per day, a fraction of that mobilized by weekly phlebotomy. Chelation therapy is indicated, however, when phlebotomy is inappropriate, such as with anemiaor hypoproteinemia.
Osteopetrosis/ albers – Schonberg disease / marble bone disease / osteosclerosis fragilis generalisata is characterized by inability of the osteoclasts to resorb bone .
2 forms: benign dominant form and malignant recessive form
Clinical features:
Benign Dominant form:
occur later in life Half are asymptomatic
Multiple pathologic fractures seen. Bone pain, cranial nerve palsy, osteomyelitis occur.
Malignant recessive form:
Optic atrophy, hepato-splenomeagaly seen

Poor growth, frontal bossing, pathologic fractures seen
Anemia- myelophthisthic : displacement of the bone marrow into the peripheral blood
Oral manifestation:
Osteomyelitis or fracture during extraction.
Enamel hypoplasia, teeth prone to caries
Eruption retardation due to dense bone.
Radiological features: reduced medullary spaces
Sclerosis opf bones , clubbing and transverse striations of bone,
Lab findings:Elevated serum acid phosphate levels.
Anemia
H/F: less osteoclast Deficient collagen matrix fibrils.
Treatment:
Bone marrow transplantation.
Adrenoleukodystrophy
Adrenoleukodystrophy (also known as X-linked adrenoleukodystrophy, ALD, X-ALD, adrenomyeloneuropathy, AMN, Siemerling–Creutzfeldt disease or bronze Schilder disease) is a disorder of peroxisomal fatty acid beta oxidation which results in the accumulation of very-long chain fatty acids in tissues throughout the body.
The most severely affected tissues are the myelin in the central nervous system, the adrenal cortex and the Leydig cells in the testes.
Clinically, ALD is a heterogenous disorder, presenting with several distinct phenotypes, and no clear pattern of genotype-phenotype correlation.
As an X-linked disorder, ALD presents most commonly in males, however approximately 50% of heterozygote females show some symptoms later in life.
Approximately one-third of ALD patients will present with the childhood cerebral form of the disease, which is the most severe form. It is characterized by normal development in early childhood, followed by rapid degeneration to a vegetative state. The other forms of ALD vary in terms of onset and clinical severity, ranging from adrenal insufficiency to progressive paraparesis in early adulthood (this form of the disease is typically known as adrenomyeloneuropathy).
ALD is caused by mutations in ABCD1, a peroxisomal membrane transporter protein, located on the X chromosome. The exact mechanism of the pathogenesis of the various forms of ALD is not known. Biochemically, individuals with ALD show very high levels of unbranched, saturated, very long chain fatty acids, particularly cerotic acid (26:0). The level of cerotic acid in plasma does not correlate with clinical presentation.
Clinical features:
ALD is a clinically heterogeneous disease.
The different clinical presentations are complicated by the pattern of X-linked recessive inheritance.
There have been seven phenotypes described in male patients with ABCD1 mutations and five in females. Initial symptoms in boys affected with the childhood cerebral form of ALD include emotional instability, hyperactivity and disruptive behavior at school.
Older patients affected with the cerebral form will present with similar symptoms. Untreated, cerebral ALD is characterized by progressive demyelination leading to a vegetative state and death.

Adult males with an adrenomyeloneuropathy presentation typically present initially with muscle stiffness, paraparesis and sexual dysfunction. All patients with clinically recognized ALD phenotypes are at risk for adrenal insufficiency.
There is no reliable way to predict which form of the disease an affected individual will develop, with multiple phenotypes being demonstrated within families
therapy
Initial attempts at dietary therapy in ALD involved restricting the intake of very-long chain fatty acids (VLCFA). Dietary intake is not the only source for VLCFA in the body, as they are also synthesized endogenously. This dietary restriction did not impact the levels of VLCFA in plasma and other body tissues.
After the realization that endogenous synthesis was an important contribution to VLCFA in the body, efforts at dietary therapy shifted to inhibiting these synthetic pathways in the body. A dietary treatment to slow the progression of the disease was developed. a mixture of unsaturated fatty acids (glycerol trioleate and glyceryl trierucate in a 4:1 ratio), known as Lorenzo's oil that inhibits elongation of saturated fatty acids in the body.
Supplementation with Lorenzo's oil has been found to normalize the VLCFA concentrations in the body, although its effectiveness at treating the cerebral manifestations of the disease are still controversial and unproven. Trials with Lorenzo's oil have shown that it does not stop the neurological degradation in symptomatic patients, nor does it improve adrenal function.
Transplant
While dietary therapy has been shown to be effective to normalize the very-long chain fatty acid concentrations in the plasma of individuals with ALD, allogeneic hematopoietic stem cell transplants are the only treatment that can stop the demyelination that is the hallmark of the cerebral forms of the disease.
In order to be effective, the transplant must be done at an early stage of the disease; if the demyelination has progressed, transplant can worsen the outcome, and increase the rate of decline. While transplants have been shown to be effective at halting the demyelination process in those presenting with the childhood
cerebral form of ALD, follow-up of these patients has shown that it does not improve adrenal function.
Gene therapy
For patients where an appropriate match for a transplant cannot be found, there have been investigations into the use of gene therapy. Appropriate vectors are selected and modified to express wild type ABCD1, which is then transplanted into the patients using a similar procedure as for a bone marrow or stem cell transplant Gene therapy has only been tried on a small number of patients, mainly in France. These patients were only considered for gene therapy after there was no HLA match for a traditional transplant. In two reported cases, the gene therapy was successful, with a resolution of the demyelination process up to two years after the procedure. Although the gene therapy was successful in resolving the neurological symptoms, plasma VLCFA levels remained elevated.
Hurler syndrome:
Excessive intracellular accumulation of chondroiin sulphate B and heparin sulphate in the tissues.
Autosomal recessive disorder.
Clinical features:
Large head, prominent forehead, saddle nose, wide nasal bridge, hypertelorism, bushy eyebrows, puffy eyelids, thick lips large tongue .
Progressive corneal clouding.
Oral manifestations:
Short broad mandible,Teeth widely spaced ,Gingival hyperplasia.
Histological features:
Intracellular mucopolysaccharide accumulation. Involve fibroblast have an appearance of clear cells or gorgoyl cells.
Hurler cells or gorgoyle cells in gingiva are demonstrated by alcian blue or toludiene blue staining.

Lab finding:
railey bodies or metachromatic granules in the cyoplasm of the circulating lymphocytes.
Treatment.
Bone transplantation is indicated.