2012 step 1 review: the respiratory system mike keller
TRANSCRIPT

2012 Step 1 Review: The Respiratory System
Mike Keller
Respiratory
• General Comments• Anatomy• Chest Wall Mechanics• Hemoglobin Physiology• Hypoxemia• Obstructive vs Restrictive Lung Disease• Lung Cancer

Anatomy
• Conducting vs. Respiratory Zone– Goblet cells are last present in the regular bronchioles– Cilia are last present in respiratory bronchioles
• Type I Pneumocytes (Squamous) vs. Type II Pneumocytes (cuboidal) – Type II cells may serve as precursors to Type I (proliferate with lung damage)– Type II – Lamellar Bodies store DPPC, released by Ca mediated endocytosis
• Pleura– Parietal Pleura – Pain! - Phrenic and Intercostal Nerves – Parietal Pleura Surface Anatomy – 8,10,12 (Lung 6,8,10)


CO2Fetal Hb
CO2

Hemoglobin PhysiologyHemoglobin modifications:(1) Methemoglobin – Oxidixed form (ferrous Fe2+ ferric Fe3+) – Impaired
oxygen carrying capacity!- Multiple causes (including G6PDH deficiency!)- Induced in order to treat cyanide poisoning (methemoglobin has higher CN- affinity).- Methemoglobinemia treated with methylene blue
(2) Carboxyhemoglobin – Hb bound to CO rather than O2 – Reduced oxygen carrying and unloading capacity!** CO has much greater (200X) affinity for Hb compared to O2
CO2 transport:(1) Bicarbonate (90%) – converted from CO2 within peripheral tissues by carbonic
anhydrase, reverse reaction occurs at lungs
(2) Carbaminohemoglobin (5%) – bound at Hb N-terminus, not heme!
(3) Dissolved CO2 (5%)
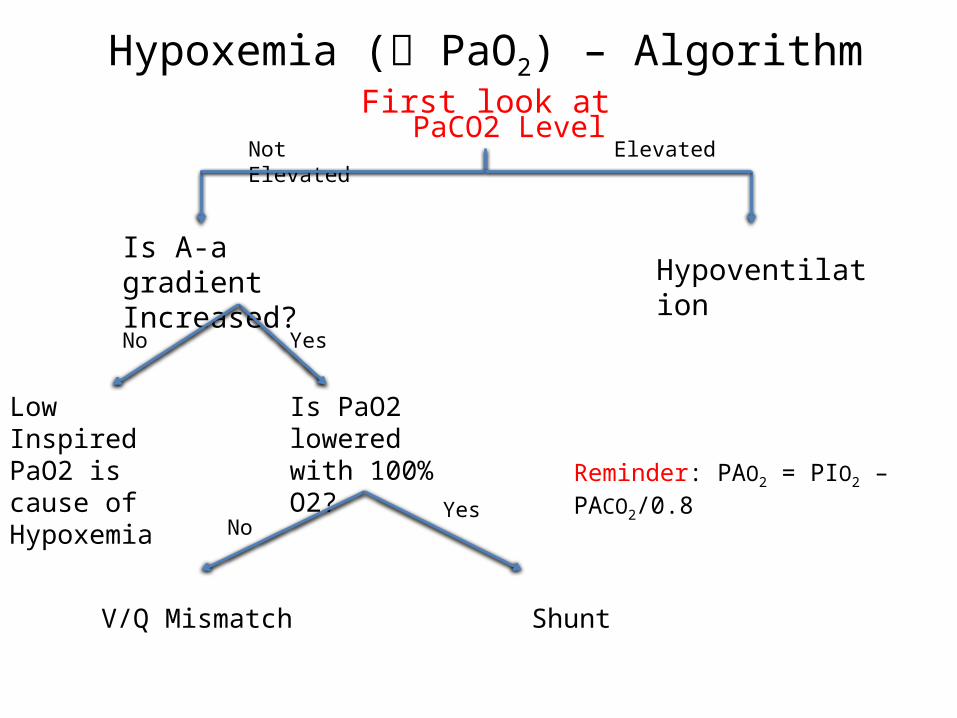
Hypoxemia ( PaO2) – AlgorithmFirst look atPaCO2 Level
Is A-a gradient Increased? Hypoventilation
Low Inspired PaO2 is cause of Hypoxemia
Is PaO2 lowered with 100% O2?
V/Q Mismatch Shunt
No Yes
NoYes
ElevatedNot Elevated
Reminder: PAO2 = PIO2 – PACO2/0.8

Obstructive vs. Restrictive Lung DiseaseLu
ng V
olum
e (L
)
Time (s)
7
3
5
1
Lung
Vol
ume
(L)
Time (s)
7
3
5
1
Lung
Vol
ume
(L)
Time (s)
7
3
5
1
FEV1 FVC
FEV1
FVCFEV1
FVC
FEV1/FVC = 80% FEV1/FVC < 80% FEV1/FVC > 80%
Normal Obstructive Restrictive
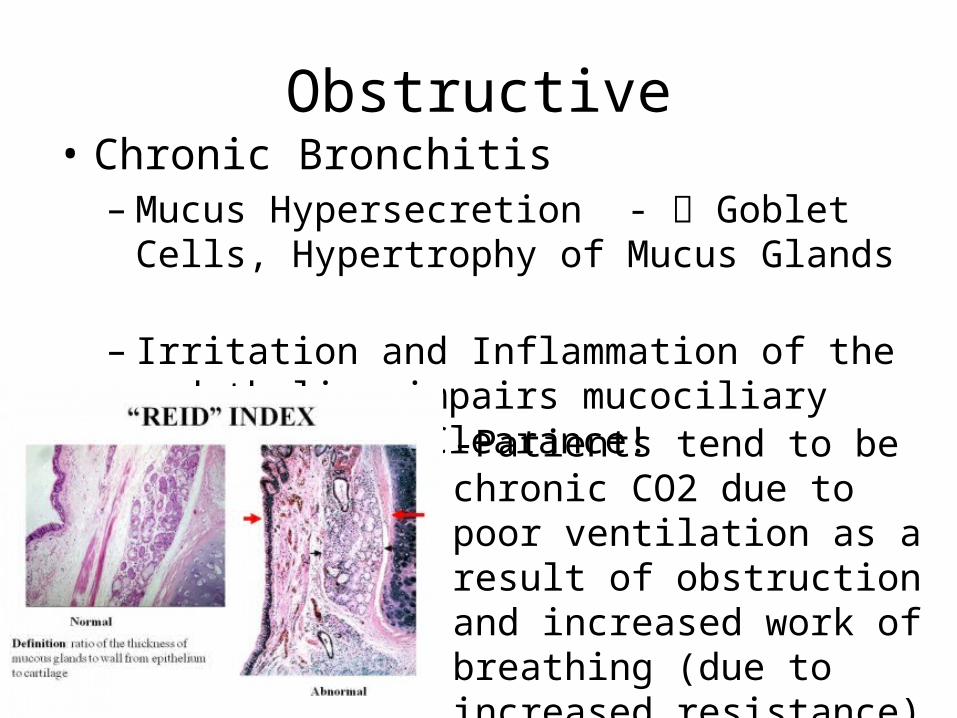
Obstructive• Chronic Bronchitis– Mucus Hypersecretion - Goblet Cells,
Hypertrophy of Mucus Glands – Irritation and Inflammation of the endothelium
impairs mucociliary response = Clearance!
-Patients tend to be chronic CO2 due to poor ventilation as a result of obstruction and increased work of breathing (due to increased resistance)

Obstructive
• Emphysema– Destruction of alveolar walls = enlargement of air
spaces distal to terminal bronchioles– Elastase activity
• Smoking is chemotactic to Neutrophils and Macrophages which release elastase. Smoking inactivates alpha 1-anitrypsin (which inactivates elastase) = Centriacinar
• Alpha 1 – antitrypsin deficiency = elastase activity = panacinar
• Hyperinflated Lungs – Due to air trapping (dynamic hyperinflation) and increased pulmonary compliance
Obstructive• Asthma
– Largely reversible airflow obstruction due to chronic airway inflammation and hyperresponsiveness.• Initial sensitizing event TH2 mediated increase in IgE Mast cells armed
with IgE Environmental trigger activates sensitized mast cells
– Chronic Inflammation leads to airway remodeling.• Smooth muscle hyperplasia/hypertrophy• Goblet Cell Hyperplasia w/ mucus hypersecretion• Basement membrane thickening w/ airway edema
– Triad of Wheezing, Dyspnea, Cough
Restrictive
• Extrapulmonary – impaired muscular effort (eg. polio, mysthenia gravis) or abnormal structural apparatus (eg. scoliosis, morbid obesity).
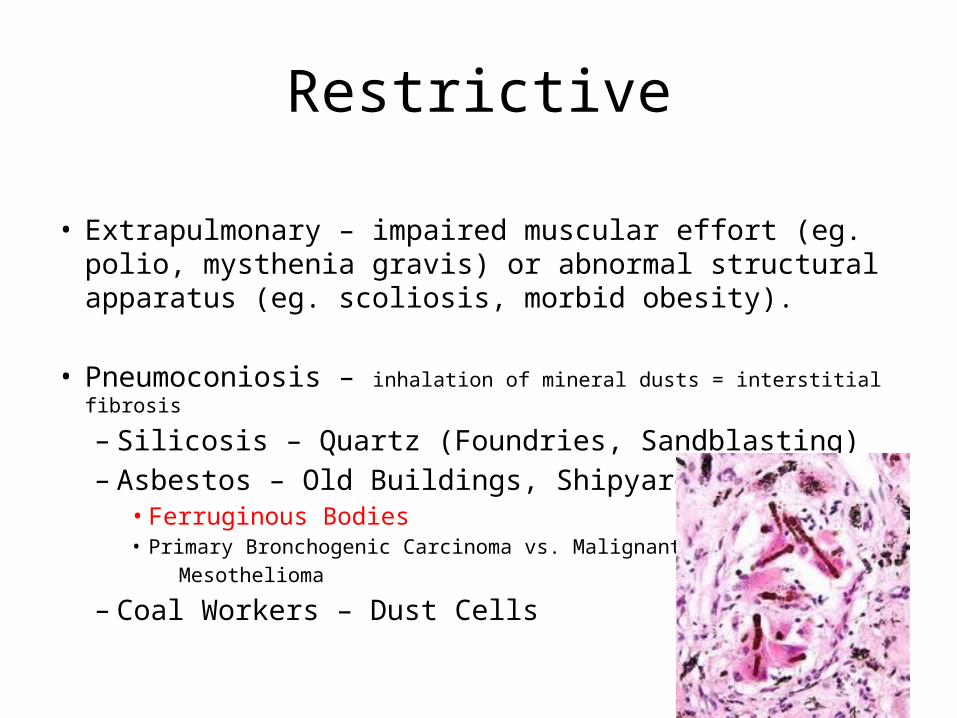
• Pneumoconiosis – inhalation of mineral dusts = interstitial fibrosis
– Silicosis – Quartz (Foundries, Sandblasting)– Asbestos – Old Buildings, Shipyard
• Ferruginous Bodies• Primary Bronchogenic Carcinoma vs. Malignant Mesothelioma
– Coal Workers – Dust Cells

Restrictive
• Sarcoidosis – multisystem granulomatous disease– Interstitial Granulomas + Mediastinal and Hilar
lymphadenopathy. – Schaumann Bodies and Asteroid Bodies
• Idiopathic Pulmonary Fibrosis– Excessive interstitial fibrosis (especially in alveoli)
• Others – Goodpasture’s Syndrome, Wegener’s granulomatosis, Collagen Vascular Disease etc..
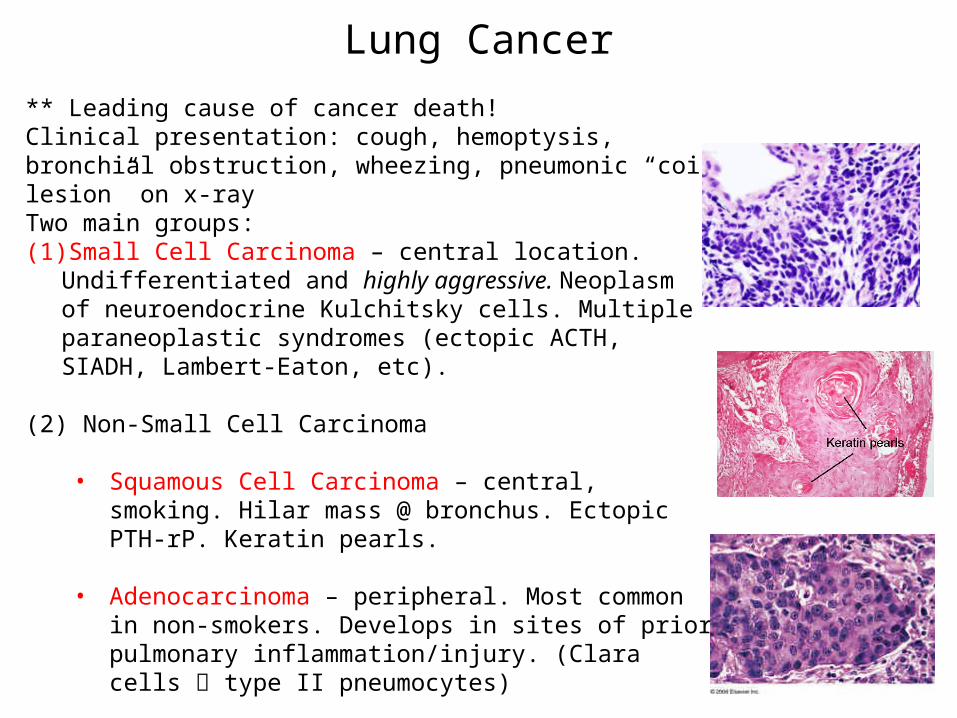
Lung Cancer** Leading cause of cancer death!Clinical presentation: cough, hemoptysis, bronchial obstruction, wheezing, pneumonic “coin lesion” on x-rayTwo main groups:(1) Small Cell Carcinoma – central location. Undifferentiated and highly
aggressive. Neoplasm of neuroendocrine Kulchitsky cells. Multiple paraneoplastic syndromes (ectopic ACTH, SIADH, Lambert-Eaton, etc).
(2) Non-Small Cell Carcinoma
• Squamous Cell Carcinoma – central, smoking. Hilar mass @ bronchus. Ectopic PTH-rP. Keratin pearls.
• Adenocarcinoma – peripheral. Most common in non-smokers. Develops in sites of prior pulmonary inflammation/injury. (Clara cells type II pneumocytes)
• Large Cell Carcinoma – peripheral. Highly anaplastic and undifferentiated, poor prognosis. Pleomorphic giant cells.
Question # 1
An unconscious patient in the supine position aspirates oral fluid into the lungs. Which of the following is the most likely anatomical location of the foreign material?
• A) Left lower lobe
• B) Right upper lobe
• C) Right lower lobe
• D) Left upper lobe

Question #2
A 45-year-old man with cirrhosis due to alpha1-antitrypsin deficiency receives a liver transplant. Although currently in good health, he is at increased risk of developing which of the following types of emphysema?
• (A) Centriacinar• (B) Compensatory• (C) Interstitial• (D) Panacinar• (E) Paraseptal

Question #3
A 34 year – old male arrives to the ER unconscious after an overdose of sedative drug. His respiratory rate is per minute, BP 80/40 mmHg. His ABG shows ph= 6.4pco2=80 mm Hgpo2= 40 mm HgHco3 = 12 mEq/LWhich is his acid -base status?A) Metabolic acidodsis with respiratory compensationB) Respiratory acidodsis and metabolic acidodsisC) Respiratory acidosis with metabolic compensationD) Uncompensated Meatbolic AcidosisE) Uncompensated Respiratory Acidosis

Question #4
You are called to perform thoracentesis on 66 year old breast cancer patient with a pleural effusion. If you are to avoid injuring lung or neurovascular elements, where would you insert the aspiration needle?
(A) the top of interspace 8 in the midclavicular line(B) the bottom of interspace 8 in the midclavicular line(C) the top of interspace 9 in the midaxillary line(D) the bottom of interspace 9 in the midaxillary line(D) the top of interspace 11 in the scapular line

Question #5
A 35-year-old man has a vital capacity (VC) of 5 L, a tidal volume (TV) of 0.5 L, an inspiratory capacity of 3.5 L, and a functional residual capacity (FRC) of 2.5 L. What is his expiratory reserve volume (ERV)?
(A) 4.5 L(B) 3.9 L(C) 3.6 L(D) 3.0 L(E) 2.5 L(F) 2.0 L(G) 1.5 L

Question #6• A 39 year old female with a history of Asthma and OCP use
presents to the ED with a compound fracture of her left leg following a motor vehicle accident requiring surgical repair. On postoperative day 4, she develops chest pain and acute SOB. Her temperature is 100o F, RR: 36, HR: 110, BP: 90/60. Which of the following is most likely characteristic of this patients disease:
• (A) Acute Bronchospasm• (B) Increased ventilation to perfusion ratio in affected areas of the
lung• (C) Complete Collapse of one Lung• (D) Decrease in pulmonary vasculature resistance• (E) Left Lower Lobe Consolidation
Question #7 A patient presents with respiratory distress. Following arterial blood gas analysis, the difference between the patient’s alveolar and arterial partial pressure of oxygen is calculated to be greater than 25mmHg. Following application of 100% oxygen, the patient’s status does not improve. Which best approximates this patient’s V/Q ratio?
A) 100
B) 1
C) 0.4
D) 3

Question #8
A 22-year-old gang member arrives in the E.R. with multiple gun shot wounds to the chest and abdomen. He has labored breathing is cyanotic, diaphoretic, cold and shivering. His blood pressure is 60 over 40. His pulse rate is 150, barely perceptible. He is in respiratory distress, has big distended veins in his neck and forehead, his trachea is deviated to the left, and the right side of his chest is tympantic, with no breath sounds. What is the most likely diagnosis?
(A) Myocardial Infarction(B) Hemothorax(C) Tension Pneumothorax(D) Pericardial Tamponade(E) Aortic Dissection
Question #9
A 58-year-old male with a 50-pack-year smoking history complains of fevers, fatigue, and weight loss. He has a chronic cough. A chest x-ray shows a left hilar mass. A CT guided biopsy shows sheets of small, round, blue cells with little cytoplasm. Which of the following is associated with this condition?
A. HypercalcemiaB. SIADHC. HypoparathyroidismD. HypothyroidismE. Pseudohypoparathyroidism

Question #10• A 19-year-old college student presents to the student health clinic
complaining of weakness, malaise, and a chronic cough. He has a fever of 100 degrees F and a dry cough; no sputum can be obtained for laboratory analysis, so a bronchial lavage is performed and the washings are submitted to the laboratory. The laboratory reports that the organism is "slow-growing." Serodiagnosis reveals cold agglutinins in the patient's serum. Which of the following organisms is the most likely cause of this student's illness? A. Klebsiella pneumoniae B. Mycoplasma pneumoniae C. Parainfluenza virus D. Respiratory syncytial virus E. Streptococcus pneumoniae

Question #11
Which of the following metabolic changes would be expected to facilitate oxygen unloading in peripheral tissues?
• A) ↑ pH
• B) Reduced glycolysis
• C) ↓ H+
• D) ↑ PCO2
Additional Items
• Make sure you understand what physical exam findings correlate to specific disease processes.
• Memorize formulas for Dead Space, Oxygen concentration etc…
• Review Dr. Preston’s Acid Base Lectures• Constantly review in order to keep the
material fresh!