obstetrical & neonatal respiratory issues mike clark, m.d., m.b.a., m.s. obstetrics &...
TRANSCRIPT

Obstetrical & Neonatal Respiratory Issues
Mike Clark, M.D., M.B.A., M.S.Obstetrics & Gynecology
Visit me at Williammclarkmd.com

Maternal TopicsI. Normal Anatomical and Physiologic Respiratory Changes in Pregnancy
II. Maternal Respiratory Disorders in Pregnancy A. Pulmonary Edema associated with Preeclampsia B. Pulmonary Embolism in Pregnancy C. Amniotic Fluid Embolism D. Asthma in Pregnancy E. Pneumonia in Pregnancy F. Tuberculosis in Pregnancy G. Idiopathic Pulmonary Fibrosis H. Kyphoscoliosis I. Sarcoidosis J. Lung Cancer

Fetal and Neonatal TopicsIII. Fetal and Neonatal Respiratory Problems A. Fetal Distress diagnosed by Fetal Monitoring B. Viability C. Amniotic Fluid Testing for Lung Maturation D. Respiratory Distress Syndrome of the Newborn E. Meconium Aspiration F. Hypoplastic Lungs G. Asphyxiating Thoracic Dystrophy H. Patent Ductus Arteriosus I. Patent Foramen Ovale (Atrial Septal Defect) J. Tetralogy of Fallot K. Anomalous Venous Return L. Transposition of the Great Vessels

MATERNAL ISSUES

Normal physiologic changes during pregnancy
Major hemodynamic alterations occur during pregnancy, labor, delivery and the postpartum period. These changes begin to take place during the first 5 to 8 weeks of pregnancy and reach their peak late in the second trimester. In patients with preexisting cardiac disease, cardiac decompensation often coincides with this peak.

Figure 28.15
Uterine Changes in Pregnancy
Enlarging uterus decreases chest wall compliance

Diaphragm pushedup
36 week fetus
Ribs and sternumpushed out. Subcostalangle widened.

Anatomical Respiratory Changes in Pregnancy (1)
• Capillary engorgement of the nasal and oropharyngeal mucosae and larynx begins early in the first trimester and increase progressively throughout pregnancy.
• Nasal breathing commonly becomes difficult, and epistaxis may occur because of nasal mucosal engorgement.

Anatomical Respiratory Changes in Pregnancy (2)
• Airway conductance increases, indicating dilation of the large airways below the larynx, mainly due to direct effects of progesterone, cortisone, and relaxin and possibly enhanced beta-adrenergic activity induced by progesterone. However, FEV1 and FEV1/FVC does not change.
Flow = ΔP/R R (Resistance) = 8ηL/πr4
r is the radius raised to the fourth power– thus dilation increases flow
Anatomical Respiratory Changes in Pregnancy (3)
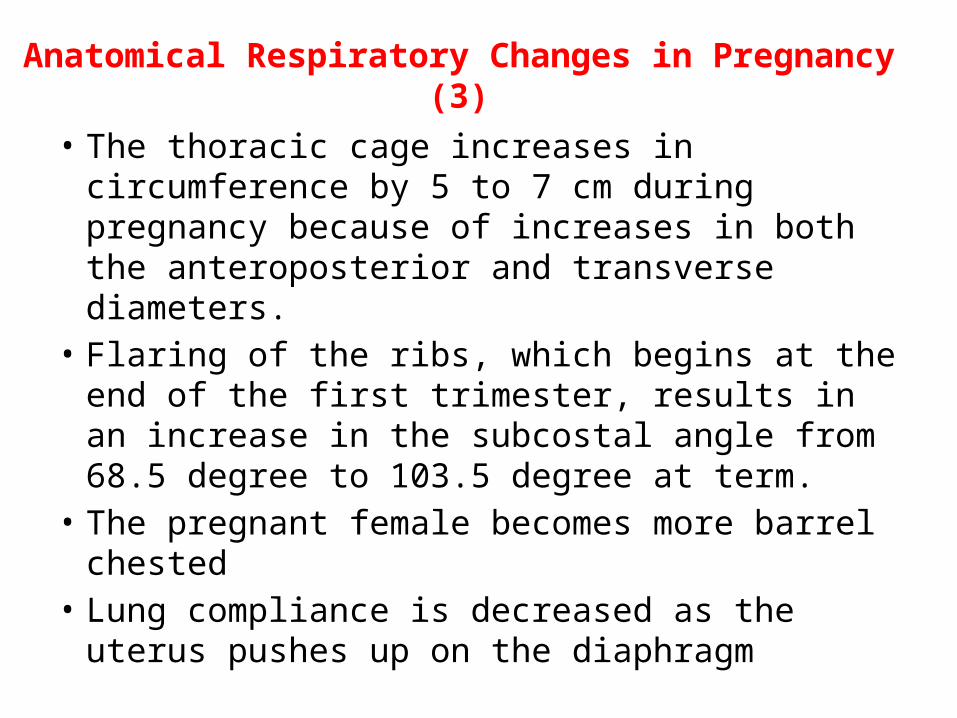
• The thoracic cage increases in circumference by 5 to 7 cm during pregnancy because of increases in both the anteroposterior and transverse diameters.
• Flaring of the ribs, which begins at the end of the first trimester, results in an increase in the subcostal angle from 68.5 degree to 103.5 degree at term.
• The pregnant female becomes more barrel chested• Lung compliance is decreased as the uterus pushes
up on the diaphragm

Copyright © 2010 Pearson Education, Inc.
Intercostal spaces
Trueribs(1–7)
Falseribs(8–12)
Jugular notchClavicular notch
ManubriumSternal angle
BodyXiphisternaljointXiphoidprocess
L1
Vertebra Floating ribs (11, 12)
Sternum
Costal cartilageCostal margin

• Pregnancy places a great demand on the physiology of the maternal body – many organ-systems are changed and stressed.
• Many preexisting medical conditions in the female are exacerbated during pregnancy.

• Major hemodynamic alterations occur during pregnancy, labor, and delivery and the postpartum period. These changes begin to take place during the first 5 to 8 weeks of pregnancy and reach their peak late in the second trimester. In patients with preexisting respiratory disease, cardiac disease, decompensation often coincides with this peak.
Physiological Changes

Note that blood pressure generally goes down in pregnancy due to decreased vascular Resistance.

Physiological Respiratory Changes in Pregnancy
Oxygen consumption: • Several authors have reported that oxygen
consumption increases by 30% to 40% during pregnancy, the progressive rise is due primary to the metabolic needs of the fetus, uterus, and placenta and secondarily to increased cardiac and respiratory work. Carbon dioxide production shows changes similar to those of oxygen consumption

Ventilation • Minute ventilation increases by 45% during pregnancy, with increase
evident early in the first trimester, as a *result of increase in tidal volume. Although respiratory rate declines slightly during mid gestation, it is essentially unaltered during pregnancy. Some females complain of *dyspnea as a result of no change in the respiratory rate.
• The increased ventilation during pregnancy results from hormonal changes (particularly progesterone elevation) and increased carbon dioxide production. Though there is increased CO2 production – the increased minute ventilation actually drops the PaCO2 from 40 Hg in the non-pregnant state to 32 – 34 Hg in the pregnant state.
• The central chemoreceptors become more sensitive to carbon dioxide levels due to progesterone level increases.
• * Discussed on next slide

Physiologic Dyspnea• The increased minute ventilation in pregnancy is often
perceived as a shortness in breath.• Shortness of breath at rest or with mild exertion is so
common that it is often referred to a “physiologic dyspnea.”
• About 75% of pregnant women have exertional dyspnea by 30 weeks of gestation
• The proposed causes of dyspnea are increased drive to breath and the load imposed by the enlarging uterus
• Other factors are increased pulmonary blood volume, anemia, and nasal congestion

The tidal volume expansion is a result of a decrease in Expiratory Reserve Volume
Progesterone and Breathing• Progesterone is a smooth muscle relaxant – thus it can dilate the
tracheal-bronchial tree – providing increased airway conductance.
• Progesterone is a known stimulant of respiration and respiratory drive, and its levels rise gradually rise from approximately 25 ng/mL at six weeks to 150 ng/mL at term
• The respiratory centers in the brain appear to change their homeostatic set points during pregnancy; this is probably a function of the increasing levels of progesterone .
• The mechanism is thought to involve an increasing sensitivity of the medulla (central chemoreceptor) to carbon dioxide such that increases in PaCO2 elicit an exaggerated respiratory effort , although a direct effect of progesterone on the respiratory center (DRG) cannot be excluded.


Maternal Respiratory Complications of Pregnancy
A. Pulmonary Edema associated with Preeclampsia B. Pulmonary Embolism in Pregnancy C. Amniotic Fluid Embolism D. Asthma in Pregnancy E. Pneumonia in Pregnancy F. Tuberculosis in Pregnancy G. Idiopathic Pulmonary Fibrosis H. Kyphoscoliosis I. Sarcoidosis J. Lung Cancer
Preeclampsia
• A pregnancy-specific syndrome characterized by new-onset hypertension and proteinuria, occurring usually after 20 weeks' gestation – most commonly after 34 weeks
• Diagnosis - – BP of 140/90 mm Hg or greater after 20 weeks' gestation
in a women with previously normal blood pressure and with proteinuria (>0.3 g protein in 24-h urine specimen).
– Eclampsia is defined as seizures that cannot be attributable to other causes in a woman with preeclampsia

PreeclampsiaPreeclampsia can be mild, moderate or severe
Severe preeclampsia is defined as the presence of one of the following symptoms or signs in the presence of preeclampsia:
1. Systolic BP of 160 mm Hg or higher or diastolic BP of 110 mm Hg or higher on 2 occasions at least 6 hours apart
2. Proteinuria of more than 5 g in 24-hour period 3. Pulmonary edema 4. Oliguria (<400 mL in 24 h) 5. Persistent headaches 6. Epigastric pain and/or impaired liver function 7. Thrombocytopenia 8. Intrauterine growth restriction

Pulmonary Embolism in Pregnancy• Pregnancy 5X increases the risk for Deep Venous
Thrombosis (DVT) and a subsequent PE• Occurs in 1-5/1,000 deliveries • Leading cause of maternal death• DVT most common in left leg • Clotting factor V seems to be most involved• Difficult to diagnose since many pregnant patients have
lower extremity edema and dyspnea• Perfusion scans generally used for diagnosis• Primary Treatment is Heparin (Coumadin cannot be used in
pregnancy) Coumadin can cross the placenta• Thrombolytic agents can be used but cautiously due to
increased bleeding

The Food and Drug Administration (FDA) created the following rating system in 1979 to categorize the
potential risk to the fetus for a given drug. Category A: Controlled human studies have demonstrated
no fetal risk Category B: Animal studies indicate no fetal risk, but no
human studies OR adverse effects in animals , but not in well- controlled human studies
Category C: No adequate human or animal studies, OR adverse fetal effects in animal studies, but no available human data.
Category D: Evidence of fetal risk, but benefits outweigh risks.
Category X: Evidence of fetal risk. Risks outweigh any benefits.

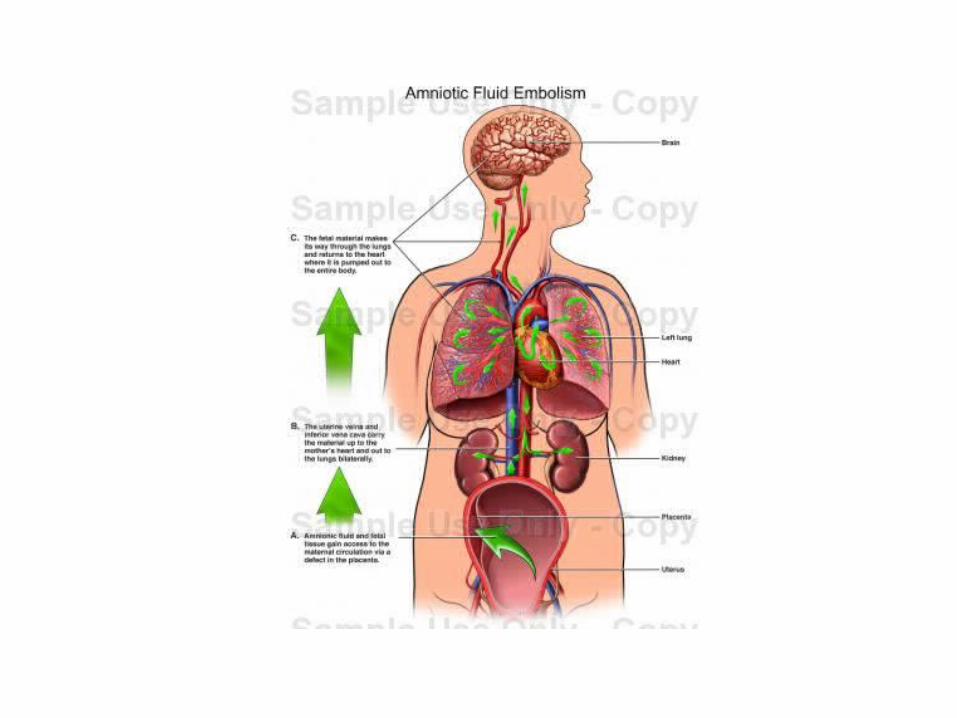
Amniotic Fluid Embolus (1)• Occurs in 1/ 8,000 – 1/ 80,000 Pregnancies• Accounts for 10% of maternal deaths• Major risk factors are maternal age and
multiparity• Lesser risk factors are amniotomy, cesarean
section, intrauterine fetal monitoring, induction of labor, term pregnancy with an IUD in place
• Most occur during labor – but can happen during any trimester, usually in the setting of uterine manipulation or trauma

Amniotic Fluid Embolus (2)Classic presenting signs and symptoms are;
1. Severe dyspnea and tachypnea2. Pulmonary Edema3. Tachycardia with cardiovascular collapse4. Cyanosis5. Disseminated Intravascular Coagulation (DIC)The diagnosis is made clinically- may aspirate from right atrium• Respiratory treatment is supportive – maximize oxygenation
through mechanical ventilation with high oxygen concentrations using low tidal volumes
• Cardiovascular treatment is to stabilize circulation using inotropic agents and vasoactive agents. The goal is to maximize cardiac output with the lowest possible left ventricular end diastolic pressures

Asthma in Pregnancy (1)• The prevalence of asthma in pregnancy is on the rise• In the world the asthma incidence in pregnancy ranges from
3.7 % - 13% (lower rate in U.S. and higher rate in the UK)• It is well known and widely reported that one third of
women experience worsening of asthma during pregnancy, one third improve, and one third remain the same.
• Between 25 and 32 weeks gestation, there was a significant increase in asthma symptoms for women that reported asthma worsening – whereas those reporting asthma improving – there was a decrease in wheezing
• In all women there was a significant improvement in symptoms between 37 and 40 weeks
Asthma in Pregnancy (2)• The improvement of some pregnant patients with asthma
is most likely due to increased levels of cortisol and progesterone during pregnancy
• An interesting finding is that pregnant females carrying boys have less asthma symptoms than those with girls
• Another interesting finding is smoking is more common among pregnant females with asthma those without the condition
• Women having an exacerbation of their asthma during pregnancy had a higher incidence of Low Birth Weight babies– but not of premature babies
• Inhaled corticosteroids have proven to be the most effective management of asthma in pregnancy

Sarcoidosis in Pregnancy Sarcoidosis is a systemic
granulomatous inflammatory disease characterized by caseating granulomas (small inflammatory nodules). Its cause is unknown. Granulomas most often appear in the lungs or the lymph nodes, but virtually any organ can be affected. Normally the onset is gradual. Sarcoidosis may be asymptomatic or chronic and may cause death.

Pneumonia in Pregnancy
• The most common cause of fatal non-obstetric infection• Can have adverse consequences for both the mother and her fetus,
with certain infections (particularly viral and fungal) assuming greater virulence and mortality than in non-pregnant women of similar age
• The pathogens for Community-Acquired Pneumonia are similar in pregnant and non-pregnant patients, with Streptococcus pneumoniae, Haemophilus influenza, Mycoplasma pneumoniae, Legionella spp., Chlamydophila pneumoniae, and influenza A accounting for the majority of cases
• However, reduction in cell mediated immunity particularly in the third trimester increases the risk for more severe pneumonia infections with organisms such as herpes, varicella and coccidiomycosis

Pneumonia in Pregnancy• The incidence of pneumonia in pregnancy is widely varied among studies in
different regions of the world – Finland has one of the higher rates and the U.S. one of the lower rates
• The incidence of pneumonia in the U. S. has declined with the highest rate being found in the large urban hospitals
• The onset of pneumonia can be at any time during gestation – with the mean gestational age being 24 – 31 weeks.
• Major risk factors for pneumonia in pregnancy are anemia and history of asthma, use of tocolytic (labor stopping) agents, cigarette smoking and drug abuse
• Viral and fungal pneumonia bear more significance in pregnancy than the bacterial pneumonias
• Pregnancies having a pneumonia complication have an increased chance of preterm delivery and small for gestational age babies

Pregnancy changes predisposing to an increased incidence and Mortality from Pneumonia
Immunologic changes• Reduced lymphocyte proliferative response• Delayed cell-mediated cytotoxicity• Reduced number of T-helper cells• Reduced lymphokine response to alloantigensPhysiologic changes• Increase in Oxygen Consumption• Increase in lung water• Elevation of the diaphragm• Aspiration more likely in labor and deliveryCoexisting illnesses• Smoking• Anemia• Asthma• Cystic Fibrosis• Illicit Drug Use• Immunosuppressive illness and therapy• Placental Abruption

Pneumonia in Pregnancy• The clinical presentation in pregnancy is not substantially different from
the non-pregnant presentation – fever, cough, pleuritic chest pain, rigors, chills, and dyspnea
• Most women with pneumonia do not have multilobar involvement – but when present does complicate the course of illness
• The Pneumonia Severity Index (PSI) is the most widely used tool in the U.S. to determine if the patient needs inpatient care and the need for the ICU.
• The PSI uses demographics (whether someone is older, and is male or female), the coexistence of co-morbid illnesses, findings on physical examination and vital signs, and essential laboratory findings. This study demonstrated that patients could be stratified into five risk categories, Risk Classes I-V, and that these classes could be used to predict 30-day survival.

Pneumonia in Pregnancy
• Initial treatment is towards Streptococcus pneumoniae, Haemophilus influenza, Mycoplasma pneumoniae, Legionella spp., Chlamydophila pneumoniae – in that these are the most common organisms
• Antibiotics that are safe in pregnancy against Community-Acquired Pneumonia are the penicillins, cephalosporins and erythromycin. Clindamycin may also be safe – but not adequately tested.
• The fluoroquinolones should not be used in pregnancy

Antibiotics not to use in Pregnancy“unless absolutely necessary‘’
• Fluoroquinolones – due to risk of arthropathy, malformations, and carcinogenic (Baloxin, Raxar)
• Chloramphenicol – can cause bone marrow suppression in fetus and if given near term can cause “gray baby syndrome” with gray facies, flaccidity and cardiovascular collapse
• Tetracyclines – mother at risk for fulminant hepatitis and staining of teeth in newborn along with other dental abnormalities
• Sulfa drugs can cause fetal kernicterus• Aminoglycosides – can cause fetal ototoxicity• Vancomycin poses a risk to the fetus in terms of
nephrotoxicity and ototoxicity

The Food and Drug Administration (FDA) created the following rating system in 1979 to categorize the
potential risk to the fetus for a given drug. Category A: Controlled human studies have demonstrated
no fetal risk Category B: Animal studies indicate no fetal risk, but no
human studies OR adverse effects in animals , but not in well- controlled human studies
Category C: No adequate human or animal studies, OR adverse fetal effects in animal studies, but no available human data.
Category D: Evidence of fetal risk, but benefits outweigh risks.
Category X: Evidence of fetal risk. Risks outweigh any benefits.

Viral Pneumonia in Pregnancy
• The most common viral organism causing pneumonia is influenza A although other viral infections can also occur
• Pregnant women are at increased risk for both acquiring influenza, and developing complications of the infection
• Historically, influenza in pregnancy has been associated with a higher rate of morbidity and mortality (with the mortality highest in the last 3 months of pregnancy)
• The clinical presentation is not altered by pregnancy• Antibiotics should be given to prevent secondary bacterial
infections• Some antiviral medications can be given in pregnancy – such
as Amantadine

Fungal Pneumonia in Pregnancy• Fungal pneumonia in pregnancy is rare – and if the
women is healthy normally resolves without treatment.
• If the fungal infection becomes widely disseminated – it carries a more serious prognosis
• Cryptococcus neoformans, Histoplasma capsulatum, Sporothrix Schenckii, Blastomyces dermatitis, and Coccidioides immitis are the most common fungal organisms
• For disseminated disease or severe pneumonia treatment with intravenous amphotericin B (pregnancy category B) is recommended followed by oral fluconazole post-partum.

Tuberculosis in Pregnancy
Caused by infection with Mycobacterium tuberculosis• Attacks mostly the lungs – but can attack other
organs• 1/3 of the world’s population now carries the TB
bacterium• Not all that are infected with TB show signs (active
TB) -many have a latent infection (asymptomatic)

Tuberculosis in Pregnancy
• Two millennia ago – the Greeks believed that pregnancy made TB get better – thus women with TB were encouraged to get pregnant
• This idea persisted until the 19th and 20th centuries when the concept completely changed – pregnancy is bad for TB
• Currently – the concept is pregnancy does not alter the course of TB
• Testing for TB in pregnancy is the same as in the non-pregnant patient – PPD, Chest X-ray and sputum cultures
• Treatment for TB is virtually the same as in the non-pregnant state – Isoniazid (INH) and Rifampin

Tuberculosis in Pregnancy• INH does cross the placenta – but causes no problems in the
fetus – however it does have some degree of hepatoxicity in the mother during pregnancy – thus if therapy can be delayed till after pregnancy – that it preferable
• Treatment can generally be delayed if the patient has latent TB
• Breast feeding while taking TB medication is OK if the mother does not have active TB – if the mother has active TB – it could be transferred to the newborn in cough droplets while breast feeding
• Congenital transplacental transmission of TB is rare and occurs most commonly through hematogenous infection via the umbilical vein in mothers who have active TB of the placenta or genital tract

C= ∆V ⁄∆P Idiopathic Pulmonary Fibrosis in Pregnancy
• Not common in pregnancy due to a higher incidence in males and usually occurs in women past childbearing age
• The pregnancy outcome depends on the severity of the disease at the time of conception
• In all restrictive lung diseases in pregnancy – patients experience breathing difficulties as pregnancy progresses since the expected increase in tidal volume is limited by the restrictive physiology and the much needed increase in minute ventilation is then achieved by an increase in respiratory rate.
• Patients with severe IPF should avoid pregnancy• Epidural anesthesia is advised to minimize the stress of labor

Kyphoscoliosis in Pregnancy
When the angle is greater than 100°, the vital capacity is reduced by50%.
Historically, patients with this condition were cautioned against pregnancy. However, studies of patients with a Cobb angle greater than 60° - show successful vaginal deliveries in most cases.
Anesthetic considerations in pregnant patients during labor and delivery follow the same principles as other patients with restrictive lung disease.
The severity of spinal curvature is measured by the Cobb angle, which is the angle formed by the intersection of perpendicular lines drawn superior to the highest vertebrae and the inferior angle to The lower vertebrae involved in the curvature.

Sarcoidosis in Pregnancy• Account for approximately 0.02 – 0.06% of
normal deliveries• Has not been associated with an increased risk
of fetal or maternal complications• The effect of pregnancy on the course of the
disease is variable• Treatment during pregnancy is the same as in
the non-pregnant state

Lung Cancer in Pregnancy (1)• Lung cancer has surpassed colon cancer as the leading cause
of death in women• There is an increased incidence of smoking among adolescent
girls• Evaluation for lung malignancy is generally delayed in
pregnancy due to signs and symptoms being misinterpreted as respiratory changes of pregnancy and apprehension by doctors to do radiographic studies during pregnancy
• Unfortunately many cases of lung cancer in pregnancy are diagnosed once the disease is locally advanced or metastatic.
• Of 19 reported cases of lung cancer in pregnancy, placental metastasis were found in 8.
• While the infant outcome is usually healthy – two reports describe metastasis to the infant- found months after delivery

Lung Cancer in Pregnancy (2)• Treatment depends on histologic cell type, gestational age at the time
of diagnosis, clinical stage, possibility of surgery, and desires of the patient.
• Generally surgery is delayed till the second trimester after organogenesis has been completed unless the patient opts for a therapeutic abortion
• Low dose radiation with the abdomen shielded has not produced deleterious outcomes for the fetus
• Overall chemotherapy is best reserved for the second or third trimester ,if necessary
• If amniocentesis shows fetal lung maturity, early delivery may be an option – particularly for women that do not want to risk fetal exposure to radiation and/or chemotherapy

FETAL ISSUES
Trimester One Trimester Two Trimester Three
LMP
LMP till end of 12th week Start of 13th week till 28th week 28th week till delivery
Date of Delivery ?
ORGANOGENESIS ORGAN GROWTH AND INITIAL FUNCTIONING ORGAN MATURATION

Fetal CardiorespiratoryDevelopment and Anatomy

Human Developmental Terms• Normal length of pregnancy from the date of fertilization till the time of
delivery is 266 days (38 weeks)
• Since most women do not know when they actually got pregnant – the term gestation period was introduced.
• Normal Gestation Period – starts with the Last Menstrual Period (approximately two weeks before the women got pregnant) – thus two weeks is added so approximately 40 weeks
• Normal Range for date of delivery using date of fertilization is 36 to 40 weeks
• Normal Range for date of delivery using LMP is 37 – 42 weeks.
• Before 37 weeks – preterm or premature• • After 42 weeks – postterm or post dates.

Human Developmental Terms• Human embryonic period includes the first 8 weeks
since date of fertilization – known as date of conception
• Human fetal period – which is week 9 after date of fertilization till birth
• The perinatal period is from week 20 of gestation (some suggest week 28) till 1- 4 weeks after the baby is born
• The neonatal period is the first 28 days after birth• Antepartum – before birth• Postpartum (postnatal) – after birth • Parturition - birth

Figure 18.23
(a) Day 20: Endothelial tubes begin to fuse.
(b) Day 22: Heart starts pumping.
(c) Day 24: Heart continues to elongate and starts to bend.
(d) Day 28: Bending continues as ventricle moves caudally and atrium moves cranially.
(e) Day 35: Bending is complete.
Tubularheart Ventricle
Ventricle
Atrium
Venous end Venous end
Arterial end Arterial end4a4
321
AortaSuperiorvenacava
Inferiorvena cava
Ductusarteriosus
Pulmonarytrunk
Foramenovale
Ventricle
The heart begins to beat on approximately the 22nd day since fertilization (5th week of gestation). However, it only beats 3.3 beats per day. By week 9 it beats at 155 – 195 beats Per minute – then by week 12 it goes into the normal recognizable rate of 120 – 160 BPM.
Human Heart Development
Bulbus Cordis
Sinus Venosus
Fetal heart sounds can be generally initially heard with the Doppler at 9 – 10 weeks of gestation - definitely heard with Doppler at 12 weeks – with fetoscope at 20 weeks.


Human Lung DevelopmentLung Development is subsumed into stages(1) Embryonic stage ( 3 – 6 weeks)(2) Fetal Pseudoglandular stage (7 – 17 weeks)(3) Fetal Canalicular stage (18 – 24 weeks)(4) Fetal Saccular stage ( 24 weeks till birth)(5) Postnatal Alveolar Stage

Embryonic Stage ( 3 – 6 weeks) Day 26 Tracheoesophageal septum developsDay 28 Buds of mainstem bronchi appearDay 33 Buds of lung lobes appearDay 41 Bronchopulmonary segments develop and
lungs become lobulated
Main Fact – Lung develops to the levelof the Bronchopulmonary Segments.

Fetal Pseudoglandular stage (7 – 17 weeks)
The pseudoglandular stage takes place during the first three to four months of gestation. During this time, the conducting airways are being formed inside what looks like a gland-like structure. Tall columnar epithelium cells grow inside these airways and form a lining. Tubular branching continues to develop throughout this stage. As early as two months into the pseudoglandular stage, all of the bronchi segments are present.
Main Fact: All of the bronchi segments are present

Fetal Canalicular stage (18 – 24 weeks)
• The canalicular stage of fetal lung development starts at the 16th week of gestation and lasts until the 24th week.
• Further branchings of the lungs occur – with the start of the formation of bronchioles.
• The capillaries that will later on allow for future gas exchange form
• Surrounding lung muscles begin to take shape.
Main Fact: Bronchioles start to develop as well as lung vasculature

Fetal Saccular stage (24 weeks till birth)
• The saccular stage starts at the 24th week and lasts until the fetus comes to term. Airway development begins to spread out and form airspaces, or saccules, within the chambers. The airspace expands as saccules continue to form.
• Terminal bronchioles divide into three or four respiratory bronchioles
• Type II pneumocytes, important in surfactant synthesis, begin to proliferate during this phase
Main Fact: Respiratory bronchioles form and surfactant production begins

Postnatal Alveolar Stage
• Begins approximately 1 – 2 months after birth. • Alveoli are developed
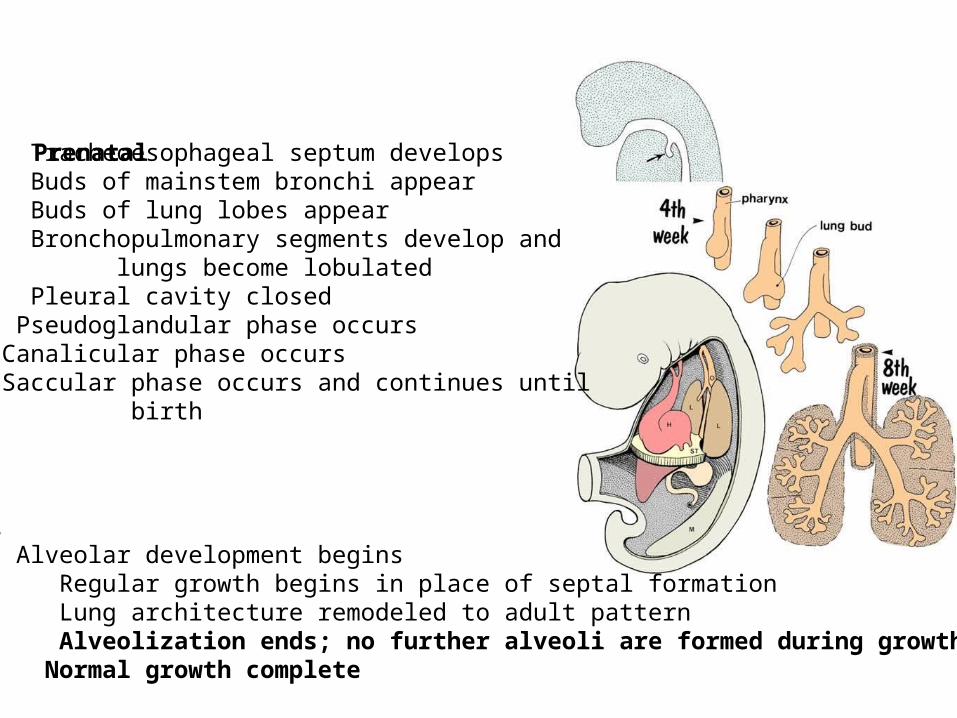
Day 26 Tracheoesophageal septum developsDay 28 Buds of mainstem bronchi appearDay 33 Buds of lung lobes appearDay 41 Bronchopulmonary segments develop and lungs become lobulatedDay 52 Pleural cavity closedWeek 8 Pseudoglandular phase occursWeek 16 Canalicular phase occursWeek 24 Saccular phase occurs and continues until birth
BIRTH
Postnatal2 months Alveolar development begins2 years Regular growth begins in place of septal formation7 years Lung architecture remodeled to adult pattern8 years Alveolization ends; no further alveoli are formed during growth15 years Normal growth complete
Prenatal

Figure 22.28
Stomodeum(future mouth)
Future mouth
Eye
Trachea
Bronchial buds
Pharynx
Foregut
OlfactoryplacodeEsophagusLiver
Laryngotrachealbud
(a) 4 weeks: anterior superficial view of the embryo’s head
(b) 5 weeks: left lateral view of the developing lower respiratory passageway mucosae
Frontonasalelevation Olfactoryplacode


Respiratory Bronchiole

Normal ValuesRespiratory Rates
• Average respiratory rates, by age:• Newborns: Average 44 breaths per minute • Infants: 40-60 breaths per minute • Preschool children: 20–30 breaths per minute • Older children: 16–25 breaths per minute
Volumes• Tidal Volume 6 – 8 ml/Kg (Adult 7 ml/kg)• Dead Space 2 – 2.5 ml/Kg (Adult 2.0)• Average newborn weight – 2.5 – 4 kg

SURFACTANT Surfactant is secreted by the type II pneumocytesSurfactant is composed of Lipids and ProteinsLipid Composition Over 90% of the surfactant is lipids; around half (50%) of
which is dipalmitoylphosphatidylcholine (DPPC) also known as lecithin. Phosphatidylcholine molecules form ~85% of the lipid in surfactant. Phosphatidylglycerol (PG) forms about 11% of the lipids in surfactant, it has unsaturated fatty acid chains that fluidize the lipid monolayer at the interface. Neutral lipids and cholesterol are also present. The components for these lipids diffuse from the blood into type II alveolar cells where they are assembled and packaged for secretion into secretory organelles called lamellar bodies.

Protein composition of Surfactant (1)
• Proteins make up the remaining 10% of surfactant. Half of this 10% is plasma proteins but the rest is formed by the apoproteins SP-A (SFTPA1), B (SFTPB), C (SFTPC) and D (SFTPD). (SP standing for "surfactant protein".)
• SP-A and SP-D confer innate immunity as they have carbohydrate recognition domains that allow them to coat bacteria and viruses promoting phagocytosis by macrophages. SP-A is also thought to be involved in a negative feedback mechanism to control the production of surfactant.

Protein composition of Surfactant (2)
SP-B and SP-C are hydrophobic membrane proteins that increase the rate that surfactant spreads over the surface. SP-B and SP-C are required for proper biophysical function of the lung. Humans and animals born with a congenital absence of SP-B suffer from intractable respiratory failure whereas those born lacking SP-C tend to develop progressive interstitial pneumonitis.

Respiratory Membrane
Figure 22.9c ,d

Chemical Stimulants of Surfactant Production
• Numerous agents such as Beta adrenergic agonists, corticosteroids, activators of protein Kinase C, leukotrienes and purinergic agonists stimulate secretion of surfactant.
• Respiratory Distress of the Newborn is due to lack of surfactant particularly the PG.

Surfactant Production Timeline
Lecithin and Phosphatidyl Glycerol (PG) increase aspregnancy proceeds while PI (other phosphatidyl choline molecules)decrease.

Fetal Lung Fluid
During fetal life the lungs are filled with fluid produced by the lungs themselves. Additionally some fluid in the fetal lungs is amniotic fluid. Amniotic fluid is produced initially by the placenta then after the kidneys start to function – they take over the job.

Fetal Lung Fluid• The degree to which lungs are expanded by liquid is
vital for normal lung development. Reductions in the degree of lung distension cause lung growth and development to cease, whereas increases in lung distension accelerate the normal growth and development of the lung. At the time of birth, however, this liquid must be cleared to enable the newborn infant to initiate air breathing.
• Removal of lung fluid before birth is due to (1) decrease production of lung fluid (2) resorption of fluid and (3) vaginal squeeze

Oligohydramnios
Oligohydramnios due to urinary track obstruction. Note the poorlung development.

FETAL CIRCULATION

Figure 28.13a
1. Oxygenated blood comesfrom the placenta travelingto the fetus in the umbilicalVein2. The umbilical vein dumps50% of blood into the inferior Vena Cava – through the DuctusVenosus and the other 50%Of the blood enters the inferiorMargin of the liver3. The blood from the inferiorVena Cava enters into the rightAtrium4. Since the placenta is supplyingOxygen to the fetus – much blood is Shunted away from the lungs throughThe Foramen Ovale and the DuctusArteriosus.
5. Blood travelsfrom the left ventricleto the Aorta – whichgives blood to perfusethe organs.6. Blood then entersthe very low resistanceumbilical arteries on itsway back to the placenta.

In the fetal period- pulmonary vascular resistance is high causing right sided heart pressure to be higher than left sided heart pressure. Thus bloodIs shunted from theright side to the leftthrough the ForamenOvale and DuctusArteriosus.
The Foramen Ovale is an opening between the right atrium and left.
The Ductus Arteriosus is an opening between thepulmonary artery and aorta.

Respiratory Transition at Birth• With birth the following sequence occurs: • The placental circulation is removed and systemic vascular resistance
increases. This in turn, increases pressures in the left ventricle and left atrium. – The foramen will tend to close when pulmonary blood flow increases as
increased pulmonary flow will increase the blood volume entering the left atrium and in so doing, increase left atrial pressure
– Increased left atrial pressure (more than right atrial pressure) results in functional closure of the foramen ovale
• With the onset of ventilation, the oxygen tension in the alveolus and in arterial blood increases. – as alveolar PaO2 increases, pulmonary vasoconstriction relaxes and
pulmonary vascular resistance becomes less than systemic vascular resistance – increased oxygenation also results in constriction of the ductus arteriosus
• The onset of ventilation also represents the onset of lung expansion resulting in the straightening out of mechanically compressed vessels
• The end result of these changes is a closure of the fetal conduits that carried blood by the lungs, but not into them

Figure 28.13b
The Ductus Arteriosusafter closure becomesthe Ligamentum Arteriosum
The Foramen Ovale afterclosure becomes the FossaOvalis
Closure of the Ductus Venosusbecomes the LigamentumVenosum

Fetal and Neonatal Respiratory Complications
A. Fetal Distress diagnosed by Fetal Monitoring B. Viability C. Amniotic Fluid Testing for Lung Maturation D. Respiratory Distress Syndrome of the Newborn E. Meconium Aspiration F. Hypoplastic Lungs G. Asphyxiating Thoracic Dystrophy H. Patent Ductus Arteriosus I. Patent Foramen Ovale (Atrial Septal Defect) J. Tetralogy of Fallot K. Anomalous Venous Return L. Transposition of the Great Vessels

Fetal Monitoring• Electronic fetal monitoring is used to evaluate
fetal well being and to assess labor progress.• The main goal is to rule out fetal distress• Fetal heart rate in association with uterine
contractions are measured• Fetal heart rate and uterine contractions are
monitored using an external electronic device until the amniotic fluid bag breaks – then internal electronic monitoring can be performed.

Normal Fetal Heart Rate –120 – 160 BPM
Look For1. Variability2. Early Deceleration(Head compression)3. Variable Deceleration(Cord Compression)4. Late Deceleration**(uteroplacental
insufficiency )

APGAR (Postpartum analysis) • The Apgar score was devised in 1952 by Dr.
Virginia Apgar as a simple and repeatable method to quickly and summarily assess the health of newborn children immediately after birth
• The Apgar score is determined by evaluating the newborn baby on five simple criteria on a scale from zero to two, then summing up the five values thus obtained. The resulting Apgar score ranges from zero to 10. The five criteria (Appearance, Pulse, Grimace, Activity, Respiration) are used as a mnemonic learning aid.

The test is generally done at one and five minutes after birth, and may be repeated later if the score is and remains low. Scores 3 and below are generally regarded as critically low, 4 to 6 fairly low, and 7 to 10 generally normal.

Viability• Viability is the ability of a fetus to survive outside the uterus
• There is no sharp limit of development, age, or weight at which a fetus automatically becomes viable.
• According to data years 2003-2005, 20 to 35 percent of babies born at 23 weeks of gestation survive,
• while 50 to 70 percent of babies born at 24 to 25 weeks,
• and more than 90 percent born at 26 to 27 weeks, survive.
• It is rare for a baby weighing less than 500 gm to survive.

Legal Issues of Viability• The Supreme Court stated in Roe v. Wade (1973) that viability (i.e.,
the "interim point at which the fetus becomes ... potentially able to live outside the mother's womb, albeit with artificial aid") "is usually placed at about seven months (28 weeks) but may occur earlier, even at 24 weeks."The 28-week definition became part of the "trimester framework" marking the point at which the "compelling state interest" (under the doctrine of strict scrutiny) in preserving potential life became possibly controlling, permitting states to freely regulate and even ban abortion after the 28th week. The subsequent Planned Parenthood v. Casey (1992) modified the "trimester framework," permitting the states to regulate abortion in ways not posing an "undue burden" on the right of the mother to an abortion at any point before and after viability; on account of technological developments between 1973 and 1992, viability itself was legally dissociated from the hard line of 28 weeks, leaving the point at which "undue burdens" were permissible variable depending on the technology of the time and the judgment of the state legislatures.
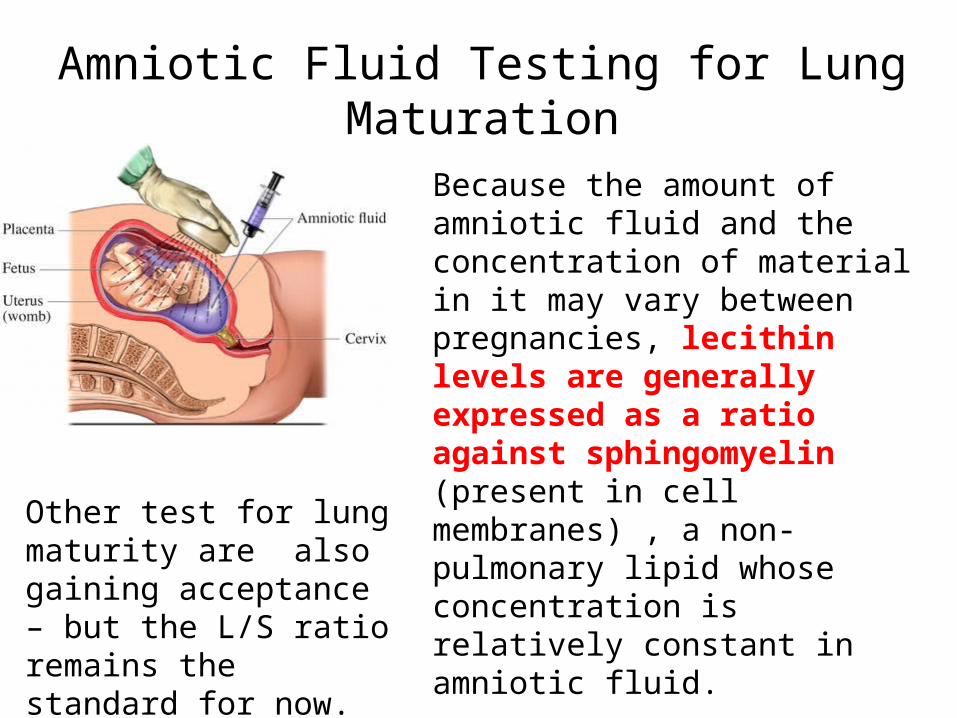
Amniotic Fluid Testing for Lung Maturation
Because the amount of amniotic fluid and the concentration of material in it may vary between pregnancies, lecithin levels are generally expressed as a ratio against sphingomyelin (present in cell membranes) , a non-pulmonary lipid whose concentration is relatively constant in amniotic fluid.
Phosphatidylglycerol (PG) is a second lipid that shows a similar time course: it is undetectable in amniotic fluid until lung maturity just prior to birth. The RDS risk is about 2% if PG is present.
Other test for lung maturity are also gaining acceptance – but the L/S ratio remains the standard for now.

Surfactant Production Timeline
Lecithin and Phosphatidyl Glycerol (PG) increase aspregnancy proceeds while PI (other phosphatidyl choline molecules)decrease.

Respiratory Distress Syndrome of the Newborn
• A syndrome caused in premature infants by developmental insufficiency of surfactant production and structural immaturity in the lungs. It can also result from a genetic problem with the production of surfactant associated proteins – in particular surfactant protein B (SP-B).
• The characteristic pathology seen in babies who die from RDS was the source of the name "hyaline membrane disease". These waxy-appearing layers line the collapsed tiny air sacs of the lung.


Normal Neonatal Lung
RDS Lung
Note the opacities in the lung fields indicating atelectasis
Air Bronchograms

Respiratory Distress Syndrome
• RDS affects about 1% of newborn infants and is the leading cause of death in preterm infants. The incidence decreases with advancing gestational age, from about 50% in babies born at 26–28 weeks, to about 25% at 30–31 weeks. The syndrome is more frequent in infants of diabetic mothers and in the second born of premature twins.

Surfactant Production Timeline
Lecithin and Phosphatidyl Glycerol (PG) increase aspregnancy proceeds while PI (other phosphatidyl choline molecules)decrease.

Respiratory Distress SyndromeClinical course• Respiratory distress syndrome begins shortly after birth and is manifest
by tachypnea, tachycardia, chest wall retractions , expiratory grunting, flaring of the nostrils and cyanosis during breathing efforts.
• As the disease progresses, the baby may develop ventilatory failure and prolonged cessations of breathing.
• Whether treated or not, the clinical course for the acute disease lasts about 2 to 3 days. During the first, the patient worsens and requires more support. During the second the baby may be remarkably stable on adequate support and resolution is noted during the third day, heralded by a prompt diuresis.
• Despite huge advances in care, RDS remains the most common single cause of death in the first month of life of the developed world.
• Complications include metabolic disorders (acidosis, low blood sugar), patent ductus arteriosus, low blood pressure, chronic lung changes, and intracranial hemorrhage.

Respiratory Distress SyndromePrevention• The main preventive measure is to deliver a baby at
term• If, for some reason, the baby must be delivered
early an amniocentesis to determine lung maturity (L/S ratio and PG) is ideally performed if greater than 30 weeks of gestation
• Another preventive technique is to inject the mother with glucocorticoids if less than 34 weeks of gestation. Glucocorticoids accelerate surfactant production.
Treatment for RDSTreatment depends on the severity of the condition.• Mild Condition – O2, CPAP, Intravenous fluids to
stabilize blood sugar, electrolytes and blood pressure
• Moderate to Severe– Endotracheal tube, PEEP, exogenous surfactant through the endotracheal tube
• ECMO – not generally used even in severe cases in that a neonate under 4.5 pounds (2 Kg) – does not have blood vessels large enough to adequately cannulate

Over Oxygenation
• Bronchopulmonary Dysplasia• Retrolental Fibroplasia

Hyperoxia conditions• Bronchopulmonary dysplasia (BPD; formerly Chronic Lung
Disease of Infancy) is a chronic lung disorder that is most common among children who were born prematurely, with low birth weights and who received prolonged mechanical ventilation to treat respiratory distress syndrome. BPD is clinically defined as oxygen dependence at 36 weeks' postmenstrual age.
• BPD is characterized by inflammation and scarring in the lungs. More specifically, the high pressures of oxygen delivery result in necrotizing bronchiolitis and alveolar septal injury, further compromising oxygenation of blood.
Hyperoxia conditions• Retinopathy of prematurity (ROP), previously known
as retrolental fibroplasia (RLF), is an eye disease that affects prematurely born babies. It is thought to be caused by disorganized growth of retinal blood vessels which may result in scarring and retinal detachment. ROP can be mild and may resolve spontaneously, but may lead to blindness in serious cases. As such, all preterm babies are at risk for ROP, and very low birth weight is an additional risk factor. Both oxygen toxicity and relative hypoxia can contribute to the development of ROP.

Retinopathy• Normally, maturation of the retina proceeds in-utero and at
term, the mature infant has fully vascularized retina. However, in preterm infants, the retina is often not fully vascularized. ROP occurs when the development of the retinal vasculature is arrested and then proceeds abnormally. The key disease element is fibrovascular proliferation. Associated with the growth of these new vessels is fibrous tissue (scar tissue) that may contract to cause retinal detachment. Supplemental oxygen exposure, while a risk factor, is not the main risk factor for development of this disease. Restricting supplemental oxygen use does not necessarily reduce the rate of ROP, and may raise the risk of other hypoxia-related systemic complications.

Meconium Aspiration• It occurs when meconium is present in their lungs
during or before delivery. Meconium is the first stool of an infant, composed of materials ingested during the time the infant spends in the uterus – which mainly are substances in the amniotic fluid.
• Meconium is normally stored in the infant's intestines until after birth, but sometimes (often in response to fetal distress) it is expelled into the amniotic fluid prior to birth, or during labor. If the baby then inhales the contaminated fluid, respiratory problems may occur.


Meconium Signs and Symptoms• The most obvious sign that meconium has been passed during or before
labor is the greenish or yellowish appearance of the amniotic fluid. The infant's skin, umbilical cord, or nail beds may be stained green if the meconium was passed a considerable amount of time before birth. These symptoms alone do not necessarily indicate that the baby has inhaled in the fluid by gasping in utero or after birth.
• After birth, rapid or labored breathing, cyanosis, slow heartbeat, a barrel-shaped chest or low Apgar score are all signs of the syndrome. Inhalation can be confirmed by one or more tests such as using a stethoscope to listen for abnormal lung sounds (diffuse crackles and rhonchi), performing blood gas tests to confirm a severe loss of lung function, and using chest X-rays to look for patchy or streaked areas on the lungs.
• Infants who have inhaled meconium may develop respiratory distress
syndrome often requiring ventilatory support. Complications of MAS include pneumothorax and persistent pulmonary hypertension.
Cause of Meconium Staining• Fetal Distress (not necessarily RDS) during labor
causes intestinal contractions, as well relaxation of the anal sphincter, which allows meconium to pass into the amniotic fluid and contaminate the amniotic fluid.
• Meconium passage into the amniotic fluid occurs in about 5-20 percent of all births and more common in overdue births.
• Of the cases where meconium is found in the amniotic fluid, meconium aspiration syndrome develops less than 5 percent of the time.
• Amniotic fluid is normally clear, but becomes greenish if it is tinted with meconium.

Treatment of Meconium Aspiration• Amnioinfusion has not shown a benefit in treating MAS .
• Until recently it had been recommended that the throat and nose of the baby be suctioned by the delivery attendant as soon as the head is delivered. However, new studies have shown that this is not useful and the revised Neonatal Resuscitation Guidelines published by the American Academy of Pediatrics no longer recommend it.
• When meconium staining of the amniotic fluid is present and the baby is born depressed, it is recommended by the guidelines that an individual trained in neonatal intubation use a laryngoscope and endotracheal tube to suction meconium from below the vocal cords.
• If the condition worsens to a point where treatments are not affecting the newborn as they should, ECMO can be necessary to keep the infant alive.
• Surfaxin (Lucinactant) is used as a treatment of MAS.

Hypoplastic Lungs Pulmonary hypoplasia is part of the
spectrum of malformations characterized by incomplete development of lung tissue.
Chest radiograph of a newborn with primary pulmonary hypoplasia of the right lung showing shift of the mediastinum to the right hemithorax.Chest radiograph of a newborn with primary pulmonary hypoplasia of the right lung showing shift of the mediastinum to the right hemithorax.

Hypoplastic Lungs • The severity of the lesion depends on the timing
of the insult in relation to the stage of lung development and the presence of other anatomic anomalies.
• The hypoplastic lung consists of a carina, a malformed bronchial stump, and absent or poorly differentiated distal lung tissue.
• In more than 50% of these cases, coexisting cardiac, GI, genitourinary, and skeletal malformations are present, as well as variations in the bronchopulmonary vasculature.

Normal Tracheobronchial tree
Carina and Bronchial Stump

Hypoplastic Lung• In order for adequate development of the lung
physical space in the fetal thoracic cavity must be adequate, proper fluid levels in the lung from lung secretions and amniotic fluid must be present, proper genetics and proper kidney development.
• The kidney provides amniotic fluid and provides proline which is important in lung development

Hypoplastic Lung• Hypoplastic Lung may be primary, but generally it is secondary,
manifested by a small fetal thoracic volume due to some compression in the hemithorax.
• Some compression conditions are congenital diaphragmatic hernia, pleural effusion with fetal hydrops, abdominal mass lesions, malformation lesions (e.g.. Asphyxiating thoracic dystrophy)
• Other causes are prolonged oligohydramnios (low amniotic fluid), early rupture of membranes, longer latent period before delivery, decreased fetal breathing
• Congenital heart disease with poor pulmonary flow is also a cause – conditions such a Tetralogy of Fallot, Hypoplastic Right Heart, Pulmonary Artery Hypoplasia , Trisomies 18, 13 and 21

Asphyxiating Thoracic Dystrophy Asphyxiating thoracic dystrophy, also known as Jeune
syndrome, is an inherited disorder of bone growth characterized by a small chest, short ribs, and shortened bones in the arms and legs. Additional skeletal abnormalities can include unusually shaped pelvic bones and extra fingers and/or toes (polydactyly).
Infants with this condition are born with an extremely narrow, bell-shaped chest that can restrict the growth and expansion of the lungs. Life-threatening problems with breathing often result, and most people with asphyxiating thoracic dystrophy live only into infancy or early childhood.

Incidence of 1 in 100,000 to 130,000 people
Extremely narrow – bell shaped chest

Patent Ductus Arteriosus• A congenital disorder of the heart wherein a neonate's
ductus arteriosus fails to close after birth. • Early symptoms are uncommon, but in the first year of life
include increased work of breathing and poor weight gain. With age, the PDA may lead to congestive heart failure if left uncorrected.
• A patent ductus arteriosus can be idiopathic, or secondary to another condition. Some common contributing factors in humans include:
• Preterm birth• Congenital Rubella Syndrome• Chromosomal abnormalities such as Down’s Syndrome


Patent Ductus Arteriosus• At birth pulmonary vascular resistance decreases such that the
right heart and pulmonary vasculature becomes less pressured than the left heart and aorta.
• Shortly after birth, the lungs release bradykinin to constrict the smooth muscle wall of the DA and reduce blood flow through the DA as it narrows and completely closes, usually within the first few weeks of life. The main stimulus to cause the release of bradykinin is an increased oxygen content of the neonate’s blood.
• In normal newborns, the DA is substantially closed within 12-24 hours after birth, and is completely sealed after three weeks.
• Withdrawal from maternal circulating prostaglandins also contributes to ductal closure.
Patent Ductus ArteriosusSome mild PDAs are asymptomatic but common
symptoms include:
• tachycardia • respiratory problems • Shortness of breath• continuous machine-like murmur• Enlarged heart• Left subclavicular thrill • Bounding pulse• Widened pulse pressure
Patent Ductus Arteriosus (Diagnosis)
• PDA is usually diagnosed using non-invasive techniques. Echocardiography and associated Doppler studies are the primary methods of detecting PDA.
• Electrocardiography (EKG )is not particularly helpful as there are no specific rhythms or ECG patterns which can be used to detect PDA.
• A chest X-ray may be taken. A small PDA most often shows a normal sized heart and normal blood flow to the lungs. A large PDA generally shows an enlarged cardiac silhouette and increased blood flow to the lungs.

Patent Ductus Arteriosus (Treatment)• Neonates without adverse symptoms may simply be
monitored as outpatients, while symptomatic PDA can be treated with both surgical and non-surgical methods.
• Surgically, the DA may be closed by ligation, wherein the DA is manually tied shut, or with intravascular coils or plugs that leads to formation of a thrombus in the DA.
• Because Prostaglandin E2 is responsible for keeping the ductus patent, NSAIDS (inhibitors of prostaglandin synthesis) such as indomethacin or a special form of ibuprofen have been used to help close a PDA. This is an especially viable alternative for premature infants.

Patent Foramen Ovale A condition in which the fetal opening (Foramen Ovale)
between the right and left atria does properly close – thus creating an Atrial Septal Defect (ASD).

Patent Foramen Ovale• After birth when the pulmonary vascular resistance drops –
giving the left atrium more pressure than the right – a left to right shunt of blood forms
• This extra blood from the left atrium may cause a volume overload of both the right atrium and the right ventricle, which if left untreated, can result in enlargement of the right side of the heart and ultimately heart failure.
• The right ventricle will have to push out more blood than the left ventricle due to the left-to-right shunt. This constant overload of the right side of the heart will cause an overload of the entire pulmonary vasculature. Eventually the pulmonary vasculature will develop pulmonary hypertension to try to divert the extra blood volume away from the lungs.

Patent Foramen Ovale (ASD)• There are different types of Atrial Septal Defects-
Patent Foramen Ovale is the common type• As a group, atrial septal defects are detected in 1
child per 1500 live births. PFO are quite common (appearing in 10 - 20% of adults) but asymptomatic and therefore undiagnosed.
• ASDs make up 30 to 40% of all congenital heart disease that is seen in adults.
• The ostium secundum atrial septal defect accounts for 7% of all congenital heart lesions. This lesion shows a female preponderance, with a male : female ratio of 1:2.

Patent Foramen Ovale (ASD)• Most individuals with a significant ASD are diagnosed
in utero or in early childhood with the use of ultrasonography or auscultation of the heart sounds during physical examination
• Once someone is found to have an atrial septal defect, a determination of whether it should be corrected has to be made.
• Surgical mortality due to closure of an ASD is lowest when the procedure is performed prior to the development of significant pulmonary hypertension. The lowest mortality rates are achieved in individuals with a pulmonary artery systolic pressure of less than *40 mmHg.

RAP2-6mmHg PAP 15-25 mmHg/5-15 mmHg
RVP 15 – 25 mm Hg/0 -8 mmHg
LAP 6 – 12 mmHg
LVP 120/0- 8 mm Hg
Pulmonary Artery Wedge Pressure4 -12 mm Hg (indirect measurementOf Left Atrial Pressure
Aortic Pressure120/80
Adult

Tetralogy of Fallot A congenital heart defect which is classically
understood to involve four anatomical abnormalities (although only three of them are always present). It is the most common cyanotic heart defect, and the most common cause of blue baby syndrome.

A. Pulmonary Stenosis – the major cause of the malformation, with the other associated malformations acting as a compensatory mechanism to the pulmonic stenosis. The degree of stenosis varies between individuals with TOF, and is the primary determinant of symptoms and severity.
B. Overriding Aorta - An aortic valve with biventricular connection, that is, it is situated above the ventricular septal defect and connected to both the right and the left ventricle. The degree to which the aorta is attached to the right ventricle is referred to as its degree of "override“ – range from 5 – 95%
C. Ventricular Septal Defect - A hole between the two bottom chambers (ventricles) of the heart. The defect is centered around the most superior aspect of the ventricular septum (the outlet septum), and in the majority of cases is single and large. In some cases thickening of the septum (septal hypertrophy) can narrow the margins of the defect .
D. Right Ventricular Hypertrophy - The right ventricle is more muscular than normal. The right ventricular wall increases in size to deal with the increased obstruction to the right outflow tract (Pulmonic Stenosis) . This feature is now generally agreed to be a secondary anomaly, as the level of hypertrophy generally increases with age
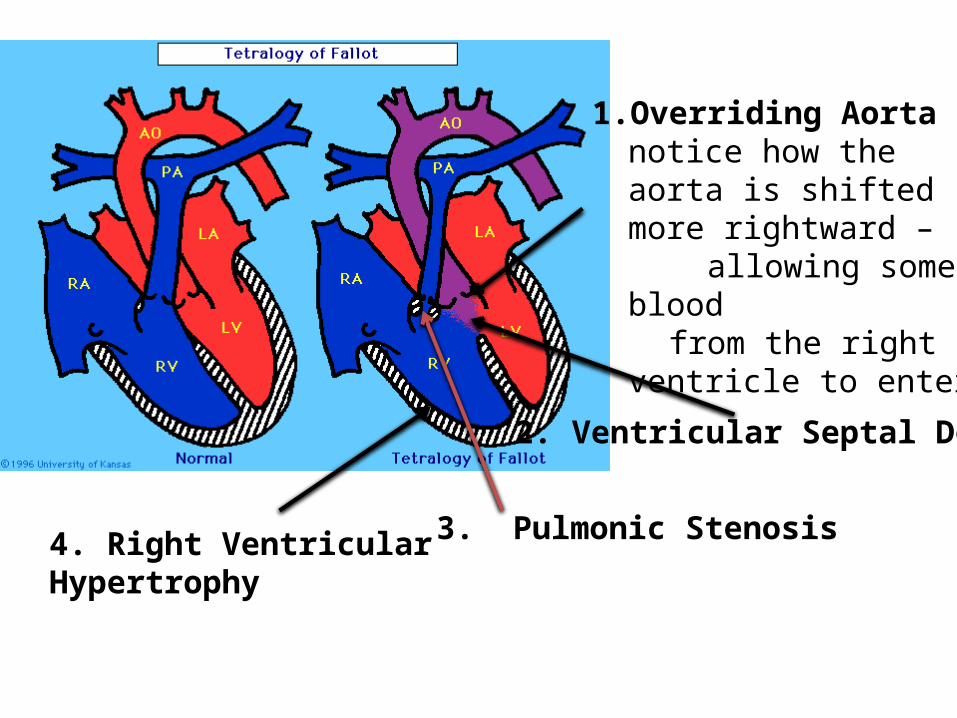
1. Overriding Aorta – notice how the aorta is shifted more rightward –
allowing some blood from the right ventricle to
enter
2. Ventricular Septal Defect
3. Pulmonic Stenosis4. Right Ventricular Hypertrophy

Additional Anomalies can sometimes occur in Tetralogy of Fallot
• stenosis of the left pulmonary artery , in 40% of patients • a bicuspid pulmonary valve, in 40% of patients • Right sided aortic arch, in 25% of patients • Coronary artery anomalies, in 10% of patients • a patent foramen ovale or atrial septal defect, in which
case the syndrome is sometimes called a pentalogy of Fallot
• partially or totally anomalous pulmonary venous return (discussed in later PowerPoint Slide)
• forked ribs and scoliosis

Tetralogy of Fallot results in low oxygenation of blood due to the mixing of oxygenated and deoxygenated blood in the left ventricle via the VSD and preferential flow of the mixed blood from both ventricles through the aorta because of the obstruction to flow through the pulmonary valve. This is known as a right- to- left shunt. The primary symptom is low blood oxygen saturation with or without cyanosis from birth or developing in the first year of life.
Main Treatment - Surgery Total repair of Tetralogy of Fallot initially carried a
high mortality risk. This risk has gone down steadily over the years. Surgery is now often carried out in infants one year of age or younger with less than 5% perioperative mortality. The open-heart surgery is designed (1) to relieve the right ventricular outflow tract stenosis by careful resection of muscle and (2) to repair the VSD.

Prognosis• Untreated, tetralogy of Fallot rapidly results in
progressive right ventricular hypertrophy. This progresses to heart failure (dilated cardiomyopathy) which begins in the right heart and often leads to left heart failure.
• Actuarial survival for untreated tetralogy of Fallot is approximately 75% after the first year of life, 60% by four years, 30% by ten years, and 5% by forty years.
• Patients who have undergone total surgical repair of tetralogy of Fallot have improved hemodynamics and often have good to excellent cardiac function.
Anomalous Pulmonary Venous Return• A Partial anomalous pulmonary venous
connection is a congenital defect where right atrium is the point of return for the blood from some (but not all) of the pulmonary veins.
• A Total anomalous pulmonary venous connection is a rare cyanotic congenital heart defect in which all four pulmonary veins are malpositioned and make anomalous connections to the systemic venous circulation.

Partial Anomalous Pulmonary Venous Return
Only Right upper pulmonary veinEntering the superior Vena Cava
NOTE
NOTE

Transposition of the Great Vessels• Transposition of the great vessels is a group of
congenital heart defects involving an abnormal spatial arrangement of any of the primary blood vessels: superior and/or inferior vena cava, pulmonary artery, pulmonary veins, and aorta.
• Transposition of the great arteries is a sub-category of Transposition of the Great Vessels in which the right ventricle empties into the aorta and the left ventricle empties into the pulmonary artery.

Transposition of the Great Vessels(Transposition of the Great Arteries)

Transposition of the Great Vessels Factors in the mother that may increase the risk of this
condition include:• Age over 40 • Alcoholism • Diabetes • Poor nutrition during pregnancy (prenatal nutrition) • Rubella or other viral illness during pregnancy
• In many cases, TGV is accompanied by other heart defects, the most common type being intracardiac shunts such as atrial septal defect, ventricular septal defect , and patent ductus arteriosus. Stenosis, or other defects, of valves and/or vessels may also be present.

Treatment for Transposition of the Great Vessels
• Immediate IV prostaglandin infusion to keep the ductus arteriosus open which allows some mixing of the two blood circulations.
• A balloon atrial septostomy may be needed to create a large hole in the atrial septum to allow blood to mix.
• A surgery called an arterial switch procedure is used to permanently correct the problem within the baby's first week of life. This surgery switches the great arteries back to the normal position and keeps the coronary arteries attached to the aorta

For a copy of the PowerPoint visit
Williammclarkmd.com
Look under special topics