2014 ias-usa treatment guidelines
TRANSCRIPT

NORTHWEST AIDS EDUCATION AND TRAINING CENTER
2014 IAS-USA Treatment Guidelines Brian R. Wood, MD Medical Director, NW AETC ECHO Assistant Professor of Medicine, University of Washington
Presentation prepared by: Presenter Last Updated: 10/16/14

International Antiviral Society-USA Guidelines Updated July 2014
§ Prevention Guidelines – Dr. Marrazzo will discuss 11/6/14 § Treatment Guidelines

Rating Scale
• Strength of Recommendations: - A: Strong support - B: Moderate support - C: Limited support
• Quality of Evidence: - Ia: >1 RCTs published in peer-reviewed literature - Ib: >1 RCTs presented at peer-reviewed scientific meetings - IIa: non-RCT’s, cohort, or case-control studies published - IIb: non-RCT’s, cohort, or case-control studies presented - III: panel’s analysis of accumulated available evidence

When to Start
ART is recommended regardless of CD4 count
CD4 count <500: AIa
CD4 count >500: BIII
Pregnancy: AIa Chronic hepatitis B: AIIa
HIV-associated nephropathy: AIIa

What to Start: Recommended Initial Regimens
Anchor Backbone Comments Dolutegravir Tenofovir-emtricitabine May increase serum creatinine
Dolutegravir^ Abacavir-lamivudine Abacavir not inferior to tenofovir at high HIV RNA levels if given with dolutegravir
Elvitegravir/cobicistat^
Tenofovir-emtricitabine May increase serum creatinine; similar drug interactions as ritonavir
Raltegravir Tenofovir-emtricitabine Raltegravir twice daily
Efavirenz^ Tenofovir-emtricitabine CNS/psych SE’s; no longer contraindicated in pregnancy but avoid in woman of child-bearing potential
Efavirenz Abacavir-lamivudine Same as above
Rilpivirine^ Tenofovir-emtricitabine Avoid if HIV RNA >100,000 copies or on PPI; taken with full meal
Atazanavir/ritonavir Tenofovir-emtricitabine May cause cholelithiasis/nephrolithiasis; consider H2 blocker/PPI interactions
Darunavir/ritonavir Tenofovir-emtricitabine Once-daily dosing for initial therapy ^Single tablet regimen (STR) option!

Additional Considerations
• Tenofovir: - Potential for renal and bone toxicity
• Abacavir: - Associated with cardiovascular events, though data conflicting - HLA-B*5701 must be negative
• Abacavir/lamivudine: - Less efficacious than tenofovir/emtricitabine when given with
efavirenz or boosted atazanavir if baseline HIV RNA >100,000
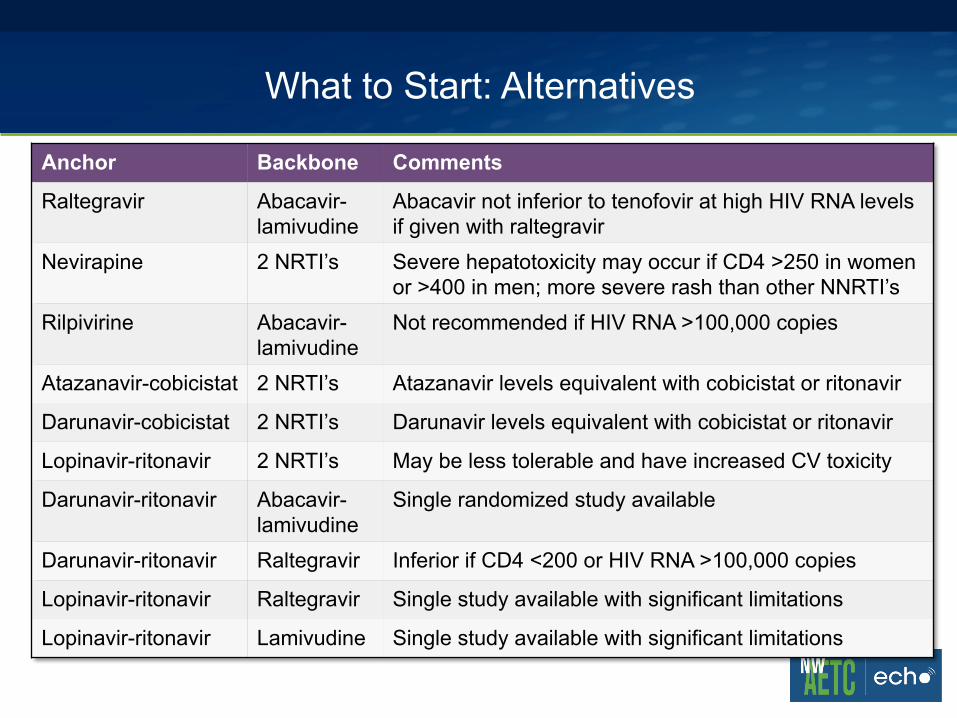
What to Start: Alternatives
Anchor Backbone Comments
Raltegravir Abacavir-lamivudine
Abacavir not inferior to tenofovir at high HIV RNA levels if given with raltegravir
Nevirapine 2 NRTI’s Severe hepatotoxicity may occur if CD4 >250 in women or >400 in men; more severe rash than other NNRTI’s
Rilpivirine Abacavir-lamivudine
Not recommended if HIV RNA >100,000 copies
Atazanavir-cobicistat 2 NRTI’s Atazanavir levels equivalent with cobicistat or ritonavir
Darunavir-cobicistat 2 NRTI’s Darunavir levels equivalent with cobicistat or ritonavir
Lopinavir-ritonavir 2 NRTI’s May be less tolerable and have increased CV toxicity
Darunavir-ritonavir Abacavir-lamivudine
Single randomized study available
Darunavir-ritonavir Raltegravir Inferior if CD4 <200 or HIV RNA >100,000 copies
Lopinavir-ritonavir Raltegravir Single study available with significant limitations
Lopinavir-ritonavir Lamivudine Single study available with significant limitations

Estimated Patent Expiration Dates for Branded Antiretrovirals
Year Antiretrovirals
2012 Zidovudine, lamivudine, stavudine, didanosine, saquinavir, nevirapine
2013 Ritonavir, efavirenz, zidovudine/lamivudine
2016 Abacavir, lopinavir/ritonavir (softgel)
2017 Tenofovir, atazanavir, darunavir
2019 Etravirine, abacavir/lamivudine
2024 Tenofovir/emtricitabine
2025 Raltegravir
2026 Tenofovir/emtricitabine/efavirenz, tenofovir/emtricitabine/rilpivirine, dolutegravir

Initiating ART in Special Circumstances
• “ART should be offered to all individuals with acute infection and should be started as early as possible to maximize benefit” (BIII)
• Benefits: reduction of proviral DNA and plasma viral load, lower viral set point, robust immune reconstitution
Acute HIV:
• “The data for initiating ART in elite controllers is stronger than before but still insufficient to recommend routine therapy”
Elite Controllers:
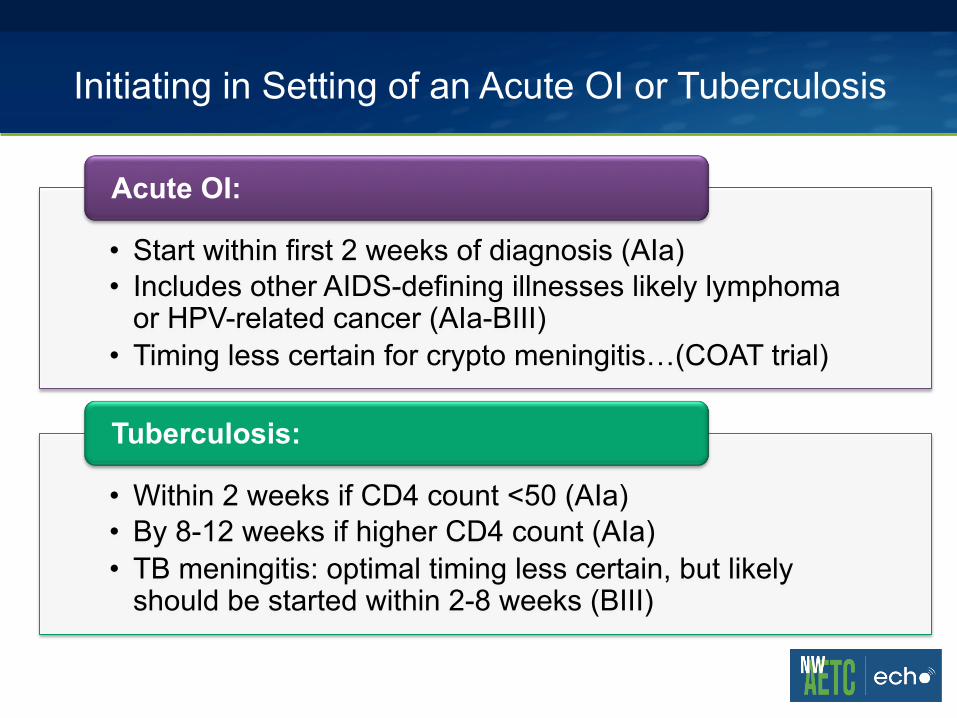
Initiating in Setting of an Acute OI or Tuberculosis
• Start within first 2 weeks of diagnosis (AIa) • Includes other AIDS-defining illnesses likely lymphoma
or HPV-related cancer (AIa-BIII) • Timing less certain for crypto meningitis…(COAT trial)
Acute OI:
• Within 2 weeks if CD4 count <50 (AIa) • By 8-12 weeks if higher CD4 count (AIa) • TB meningitis: optimal timing less certain, but likely
should be started within 2-8 weeks (BIII)
Tuberculosis:
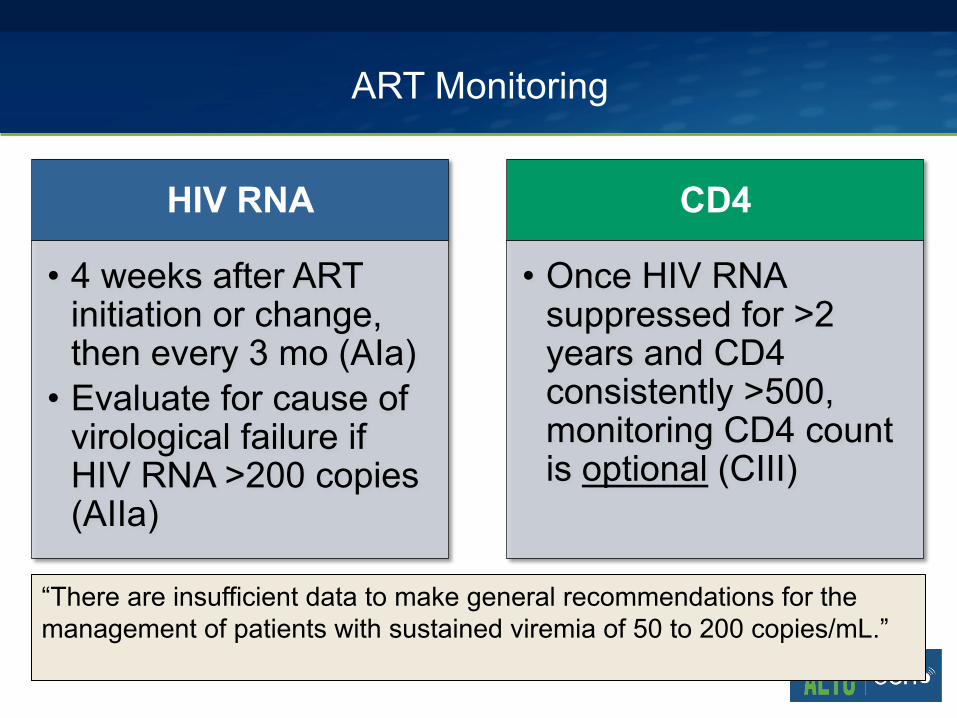
ART Monitoring
HIV RNA
• 4 weeks after ART initiation or change, then every 3 mo (AIa)
• Evaluate for cause of virological failure if HIV RNA >200 copies (AIIa)
CD4
• Once HIV RNA suppressed for >2 years and CD4 consistently >500, monitoring CD4 count is optional (CIII)
“There are insufficient data to make general recommendations for the management of patients with sustained viremia of 50 to 200 copies/mL.” !