2016 cobra guide
DESCRIPTION
ÂTRANSCRIPT

303-776-6200 • 395 S. PRATT PKWY.• LONGMONT, CO 80501 • SVVSD.ORG
OPEN ENROLLMENT
ST. VRAIN VALLEY SCHOOLS’
COBRA

CNIC PPO PLANThe self-insured CNIC Plan is a Preferred Provider Organization (PPO) plan that offers a large network of contracted doctors and hospitals to choose from whenever care is needed. In Colorado, the Plan utilizes the Rocky Mountain Health Network and if you are outside of Colorado, you will want to access the Aetna Signature Network to maximize your savings. After you meet your annual deductible, you are responsible for paying a portion of remaining eligible expenses (your coinsurance).
When you enroll in the CNIC HRA plan, you automatically receive prescription drug coverage through NPS (National Pharmaceutical Services). You must use an in-network pharmacy to receive a benefit under the NPS pharmacy plan.
Most national pharmacy chains and local pharmacies participate in the NPS Network. (Please visit the NPS website at www.pti-nps.com to view the most up-to-date listing of pharmacy providers near you.)
KAISER PERMANENTE (DHMO) PLANThe Kaiser Permanente plan is a non-profit Deductible Health Maintenance Organization (DHMO) plan that provides services through the Kaiser Permanente network of doctors, partner hospitals and other health care facilities.
There is no out-of-network coverage unless you experience a life-threatening injury or illness that requires ambulance and/or emergency room assistance.
Each time you visit a Kaiser Permanente pharmacy or other provider for care, you pay a copay or an amount based on your deductible and coinsurance responsibility. Your out-of-pocket costs for eligible expenses are capped annually at $2,500 for an individual or $5,000 for a family.
• Deductible – the amount of covered expenses you must pay before charges are paid by your medical plan
• Copayment – a fixed-dollar amount you pay for covered services through your medical plan
• Coinsurance – your share of the cost of covered services, calculated as a percentage (for instance, you pay 10% and the Plan pays 90%); typically payable after you have met your deductible
• Out-of-PocketMaximum - the maximum amount you pay in a calendar year for covered expenses under your health plan (once you or your covered dependent reach the OOP Maximum, the plan covers 100% of eligible expenses for the remainder of the year)
KEY DEFINITIONS

CONNECT YOUR CARE • 877-292-4040 • CONNECTYOURCARE.COM
When picking up your prescription at the pharmacy, show your ID card and pay your copay. It’s that simple! Your benefit will be processed onsite (no claim needed).
There are two ways you can receive your prescription drug benefits:
• Retail Pharmacy – You receive up to a 30-day supply.• Mail Order – If you are taking a maintenance medication (for a medical condition
that requires ongoing use of medications such as high blood pressure, diabetes or a thyroid condition), you may want to use the mail-order prescription service through Integrated HMO Pharmacy. When you order prescriptions by mail, you can receive up to a 90-day supply and you’ll typically save money.
Using in-network providers can save you money in several ways:
• You have a lower upfront deductible and the Plan reimburses at a higher level for in-network charges
• In-network providers have agreed to negotiated fees that are typically lower than out-of-network providers
• The Healthcare Bluebook, a service provided at no additional cost to all CNIC plan participants, provides online tools to help you identify the fair market price for thousands of medical procedures, tests, and other services. Check it out at: www.healthcarebluebook.com/cc/stvrain Password: hcbbstvrain
KEEP IN MINDOTHER RESOURCESMedical ContactsCNIC800-426-7453cnichs.com
Healthcare Blue Book800-426-7453healthcarebluebook.com/cc/stvrainpassword: hcbbstvrain
Kaiser Permanente800-632-9700kp.org
PharmacyNPS (Retail)800-546-5677pti-nps.com
Integrated HMO (Mail Order)800-633-7928pti-nps.com
DentalDelta Dental800-610-0201deltadentalco.com
VisionVSP800-877-7195vsp.com
RetirementPERA303-832-9550copera.org
Connect Your CareCOBRA Dept.PO Box 873682Kansas City, MO 64187
(p): 855-687-2021(f): [email protected]

CNIC (PPO) IN-NETWORKHRA Contribution (funded by SVVSD) $750 Individual; $1,500 Employee + Dependent(s) N/A
Deductible (excludes RX/Vision copays) $2,000 Individual/ $4,000 Employee + Dependent(s)
$4,000 Individual/ $8,000 Employee + Dependent(s)
$250 Individual/$500 Employee + Dependent(s)
Out-of-Pocket Maximum$2,500 Individual/ $5,000 Employee + Dependent(s)
(excludes RX/Vision copays; includes deductibles)
$5,000 Individual/ $10,000 Employee + Dependent(s)
$2,500 Individual/ $5,000 Employee + Dependent(s)
(includes copays and deductibles)
Lifetime Maximum Unlimited Unlimited
Preventive Care Covered at 100% 50% coinsurance* Covered at 100%
Women’s Preventive Care (includes contraceptive devices, drugs and services)
Covered at 100% 50% coinsurance* Covered at 100%
Office Visits 10% coinsurance* 50% coinsurance* $25 copay (PCP) / $40 copay (Specialist)
Diagnostic Lab/X-RayDiagnostic CT, PET, MRI
10% coinsurance*50% coinsurance*
Lab covered at 100%;Diagnostic x-ray, 10%* coinsurance;
CT, PET, MRI $100 copay per procedure
Chiropractic Care 10% coinsurance* 50% coinsurance* Not Covered
Outpatient Surgery 10% coinsurance* 50% coinsurance* 10% coinsurance*
Inpatient Hospital Services 10% coinsurance* 50% coinsurance* 10% coinsurance*
Ambulance 10% coinsurance* 10% coinsurance* 10% coinsurance, up to $500
Emergency Room 10% coinsurance* 10% coinsurance* $150 copay
Urgent Care 10% coinsurance* 50% coinsurance* $50 copay at a KP after-hours medical office
Outpatient Mental Health/Substance Abuse 10% coinsurance* 50% coinsurance* $25 copay
Therapies (PT/OT/Speech)• Inpatient• Outpatient• Chiropractic
10% coinsurance*10% coinsurance*10% coinsurance*
50% coinsurance*50% coinsurance*50% coinsurance*
10% coinsurance*$25 copay
Not Covered
Durable Medical Equipment 10% coinsurance* 50% coinsurance* 10% coinsurance*
Routine Vision Exam $10 copay (one exam every 24 months)
Up to $100 allowance (one exam every 24 months)
$25 copay(one exam every 12 months)
Prescription Drugs (Retail Pharmacies)Up to a 30-day supply
$10 Copay Generic$45 Copay Brand Name, Formulary
$60 Copay Brand Name, Non-Formulary Not Covered$15 Copay Generic
$40 Copay Brand Name20% Coinsurance, Specialty
(max. $250 per fill)
Prescription Drugs (Retail Pharmacies)Up to a 90-day supply
$25 Copay Generic$113 Copay Brand Name, Formulary
$150 Copay Brand Name, Non-Formulary Not Covered$30 Copay Generic
$80 Copay Brand Name 20% Coinsurance, Specialty
(max. $250 per fill)
MEDICAL SERVICES
*After plan deductible is met.
CNIC (PPO) OUT-OF-NETWORK

HRA Contribution (funded by SVVSD) $750 Individual; $1,500 Employee + Dependent(s) N/A
Deductible (excludes RX/Vision copays) $2,000 Individual/ $4,000 Employee + Dependent(s)
$4,000 Individual/ $8,000 Employee + Dependent(s)
$250 Individual/$500 Employee + Dependent(s)
Out-of-Pocket Maximum$2,500 Individual/ $5,000 Employee + Dependent(s)
(excludes RX/Vision copays; includes deductibles)
$5,000 Individual/ $10,000 Employee + Dependent(s)
$2,500 Individual/ $5,000 Employee + Dependent(s)
(includes copays and deductibles)
Lifetime Maximum Unlimited Unlimited
Preventive Care Covered at 100% 50% coinsurance* Covered at 100%
Women’s Preventive Care (includes contraceptive devices, drugs and services)
Covered at 100% 50% coinsurance* Covered at 100%
Office Visits 10% coinsurance* 50% coinsurance* $25 copay (PCP) / $40 copay (Specialist)
Diagnostic Lab/X-RayDiagnostic CT, PET, MRI
10% coinsurance*50% coinsurance*
Lab covered at 100%;Diagnostic x-ray, 10%* coinsurance;
CT, PET, MRI $100 copay per procedure
Chiropractic Care 10% coinsurance* 50% coinsurance* Not Covered
Outpatient Surgery 10% coinsurance* 50% coinsurance* 10% coinsurance*
Inpatient Hospital Services 10% coinsurance* 50% coinsurance* 10% coinsurance*
Ambulance 10% coinsurance* 10% coinsurance* 10% coinsurance, up to $500
Emergency Room 10% coinsurance* 10% coinsurance* $150 copay
Urgent Care 10% coinsurance* 50% coinsurance* $50 copay at a KP after-hours medical office
Outpatient Mental Health/Substance Abuse 10% coinsurance* 50% coinsurance* $25 copay
Therapies (PT/OT/Speech)• Inpatient• Outpatient• Chiropractic
10% coinsurance*10% coinsurance*10% coinsurance*
50% coinsurance*50% coinsurance*50% coinsurance*
10% coinsurance*$25 copay
Not Covered
Durable Medical Equipment 10% coinsurance* 50% coinsurance* 10% coinsurance*
Routine Vision Exam $10 copay (one exam every 24 months)
Up to $100 allowance (one exam every 24 months)
$25 copay(one exam every 12 months)
Prescription Drugs (Retail Pharmacies)Up to a 30-day supply
$10 Copay Generic$45 Copay Brand Name, Formulary
$60 Copay Brand Name, Non-Formulary Not Covered$15 Copay Generic
$40 Copay Brand Name20% Coinsurance, Specialty
(max. $250 per fill)
Prescription Drugs (Retail Pharmacies)Up to a 90-day supply
$25 Copay Generic$113 Copay Brand Name, Formulary
$150 Copay Brand Name, Non-Formulary Not Covered$30 Copay Generic
$80 Copay Brand Name 20% Coinsurance, Specialty
(max. $250 per fill)
CNIC (PPO) OUT-OF-NETWORK KAISER (DHMO) IN-NETWORK ONLY

DENTAL INSURANCEThe self-insured dental plan, administered through Delta Dental of Colorado, is designed to help you maintain a healthy smile through regular preventive dental care, and to fix any problems as soon as they occur. Because preventive dental care is so important, the plan covers these services in full with no deductible or copay when you visit a Delta Dental PPO dentist. Although you are free to visit any licensed dentist for your care, you will save money by visiting a Delta Dental PPO or Premier® dentist.
For in-network providers, visit www.deltadentalco.com and use the “Find a Dentist” search tool. See summary of dental benefits below:
Annual Deductible (waived for preventive services)
$50 Individual/$100Employee + Dependent(s)
Preventive Services (oral exams, x-rays, cleanings)
100% 80% after deductible 80% after deductible
Basic & Restorative Services (fillings, endodontics, periodontics)
80% after deductible 80% after deductible 80% after deductible
Major Services (dentures, crowns, bridges)
50% after deductible 50% after deductible 50% after deductible
Orthodontia (children up to 19 years of age)
50% up to $1,000 lifetime maximum. Deductible waived
Annual Benefit Maximum $1,500 per person
PPODENTIST 1
PREMIERDENTIST 2
NON-PARTICIPANTDENTIST 3
1 The PPO percentage of benefits is based on the PPO Schedule of Allowance 2 The Premier percentage of benefits is limited to the Premier Maximum Plan Allowance. 3 The Non-Participating percentage of benefits is limited to the non-participating Maximum Plan Allowance. You are responsible for the difference between the non-participating Maximum Plan Allowance and the fee charged by the dentist.
ID Cards are mailed after enrollment or visit deltadentalco.com to print your own.
DENTALSERVICES

CONNECT YOUR CARE • 877-292-4040 • CONNECTYOURCARE.COM
VISION INSURANCEThe VSP vision plan includes benefits for eye exams, eyeglasses, and contact lenses. When you visit a VSP provider, you must pay a copay to your provider at the time of service.
Your provider will file claims for you and will be reimbursed directly by the insurance carrier for allowable charges. No need to show an insurance card, simply tell your vision provider you have VSP.
To find a VSP provider, go to www.vsp.com. Reference the “choice” network to find an in-network VSP doctor.
When you visit an out-of-network provider for your vision care, you must pay your expenses in full at the time of service and submit a claim to VSP for reimbursement up to plan allowances, which are shown in the table below:
Discounts are available for non-covered services such as additional glasses and sunglasses, contact lenses and laser vision correction surgery.
Vision exam (every 12 months) $10 copay $45
Frames (every 12 months) Up to $140, then receive 20% discount $70
Lenses (every 12 months):Single vision lensesBifocal lensesTrifocal lenses
-$10 copay$10 copay$10copay
-$30$50$65
Elective contact lenses, fitting and evaluation (in lieu of glasses)
Up to $140 $105
IN-NETWORKYOU PAY
OUT-OF-NETWORKREIMBURSEMENT
VISIONSERVICES
ALL PREMIUMS ON BACK PAGE.
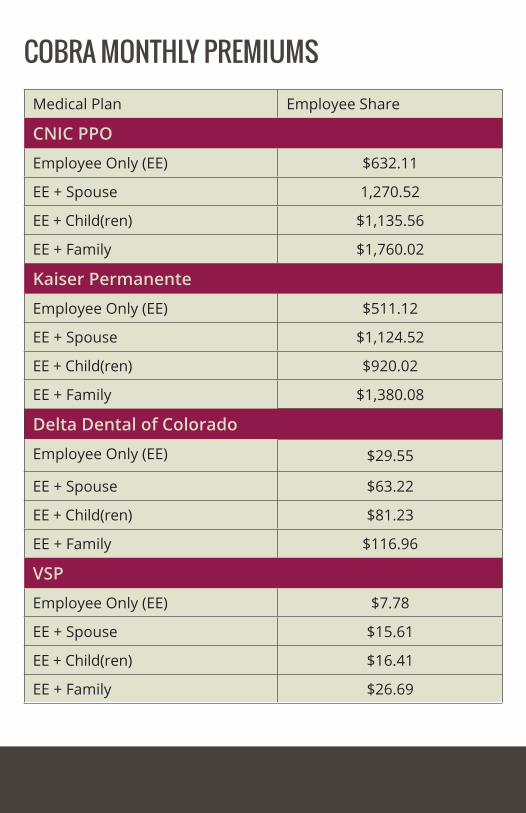
Medical Plan Employee Share
CNIC PPO
Employee Only (EE) $632.11
EE + Spouse 1,270.52
EE + Child(ren) $1,135.56
EE + Family $1,760.02
Kaiser Permanente
Employee Only (EE) $511.12
EE + Spouse $1,124.52
EE + Child(ren) $920.02
EE + Family $1,380.08
Delta Dental of Colorado
Employee Only (EE) $29.55
EE + Spouse $63.22
EE + Child(ren) $81.23
EE + Family $116.96
VSP
Employee Only (EE) $7.78
EE + Spouse $15.61
EE + Child(ren) $16.41
EE + Family $26.69
COBRA MONTHLY PREMIUMS