2016 trenhaile mdi oset final.key
TRANSCRIPT

The Inferior Capsular Shift For MDI: Is it a thing of the past, do I ever do it
open?
Scott W. Trenhaile, MDAssistant Professor - Rush University Medical Center - Chicago
Assistant Clinical Professor - University of Illinois College of Medicine - Rockford Rockford, Illinois USA
www.scotttrenhailemd.com

Disclosures
• Smith & Nephew, Inc.
• Consultant Income
• Royalty Agreement
• Exactech, Inc: Consultant
• Research Support
• AAOS disclosures up to date on website

What is MDI?
• Laxity
• Normal Looseness
• Measured on EUA
• Equal side to side
• Instability
• Pathologic movement GH jt: Symptoms
• Change from normal
• injury, overuse, fatigue, posture, scapular dyskinesia

MDI: Neer
• “uncontrollable involuntary inferior subluxation or dislocation” along with both “anterior and posterior directions”
• Symptomatic subluxation in 2 or more directions
• True inferior instability
• Rotator interval laxity

MDI: Etiology• Congenital:
• Usually no surgery needed unless to facilitate Rehab
• Repetitive Stress (swimming/gymnastics)
• Surgery is possibly needed
• Traumatic: specific injury
• Surgery usually needed

Why is MDI Symptomatic?
• Pain from RC tendonitis
• Scapular protraction leads to:
• Trapezius pain/spasm/weakness
• Weakness= subluxation

MDI: What does it look like

Treatment: Rehabilitation
• Decrease inflammation
• Correct scapular position
• Pain-free cuff exercises
• Functional Rehabilitation
• Improve Core and hip strength
• Occasionally bracing for feedback

Surgical Indications
• Pain
• Functional Impairment
• Failed PT
• Usually a traumatic event
• Options:
• Open shift or arthroscopic plication

Open Capsular Shift in 2016
• Relative Contraindications to Scope Shift
• HAGL lesions
• Capsular Ruptures
• Revision of previous shift, esp cap deficiency
• Failed Thermal Capsulorraphy
• Failed Open stabilization with failed subscapularis tendon
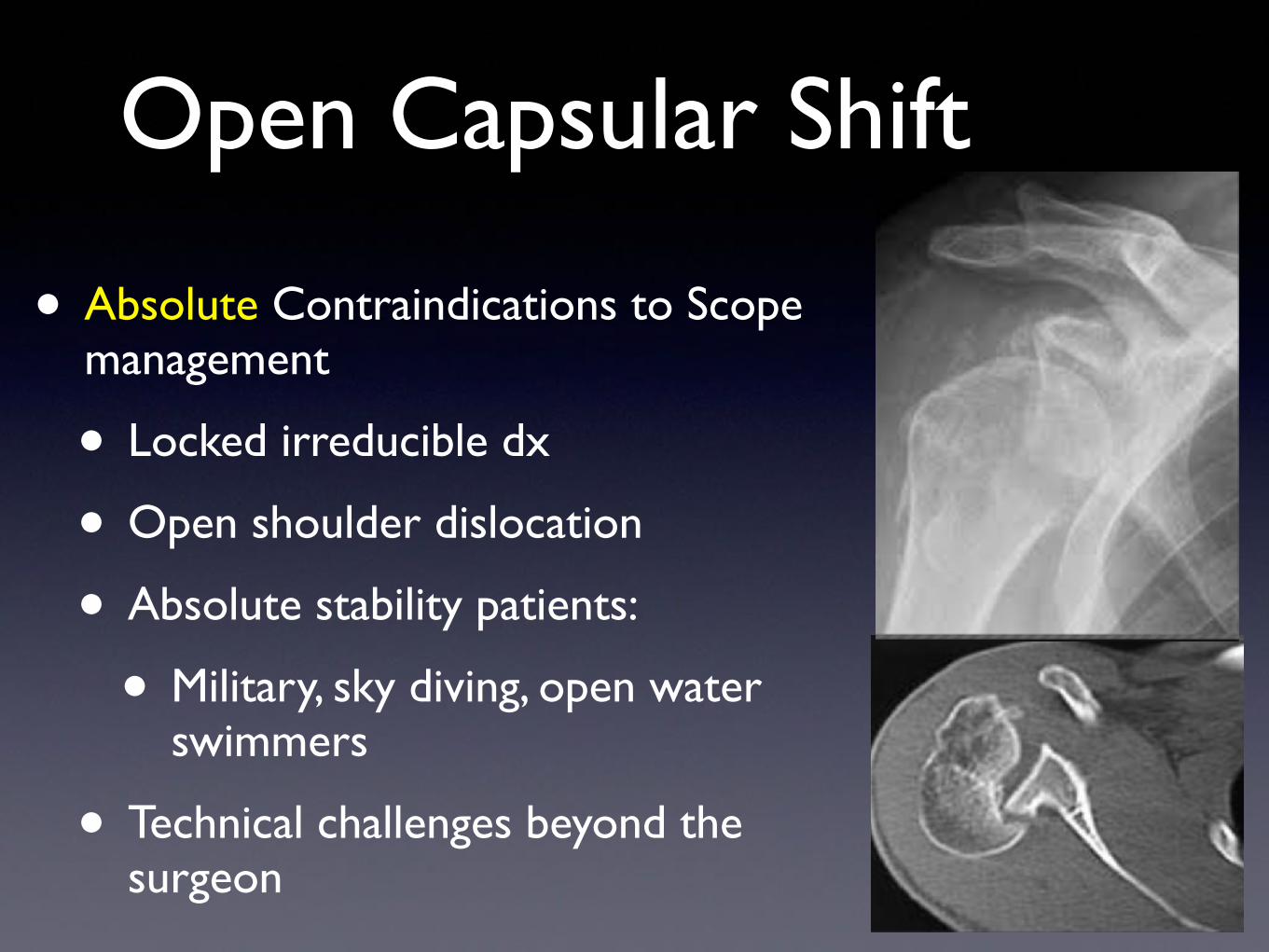
Open Capsular Shift
• Absolute Contraindications to Scope management
• Locked irreducible dx
• Open shoulder dislocation
• Absolute stability patients:
• Military, sky diving, open water swimmers
• Technical challenges beyond the surgeon

MDI: Pathology
• Address:
• “Patulous” Capsule
• Widened rotator interval
• Address associated labral tears (trauma?)

• T-Capsular humeral incision overlapping to reduce redundancy
• 40 shoulders
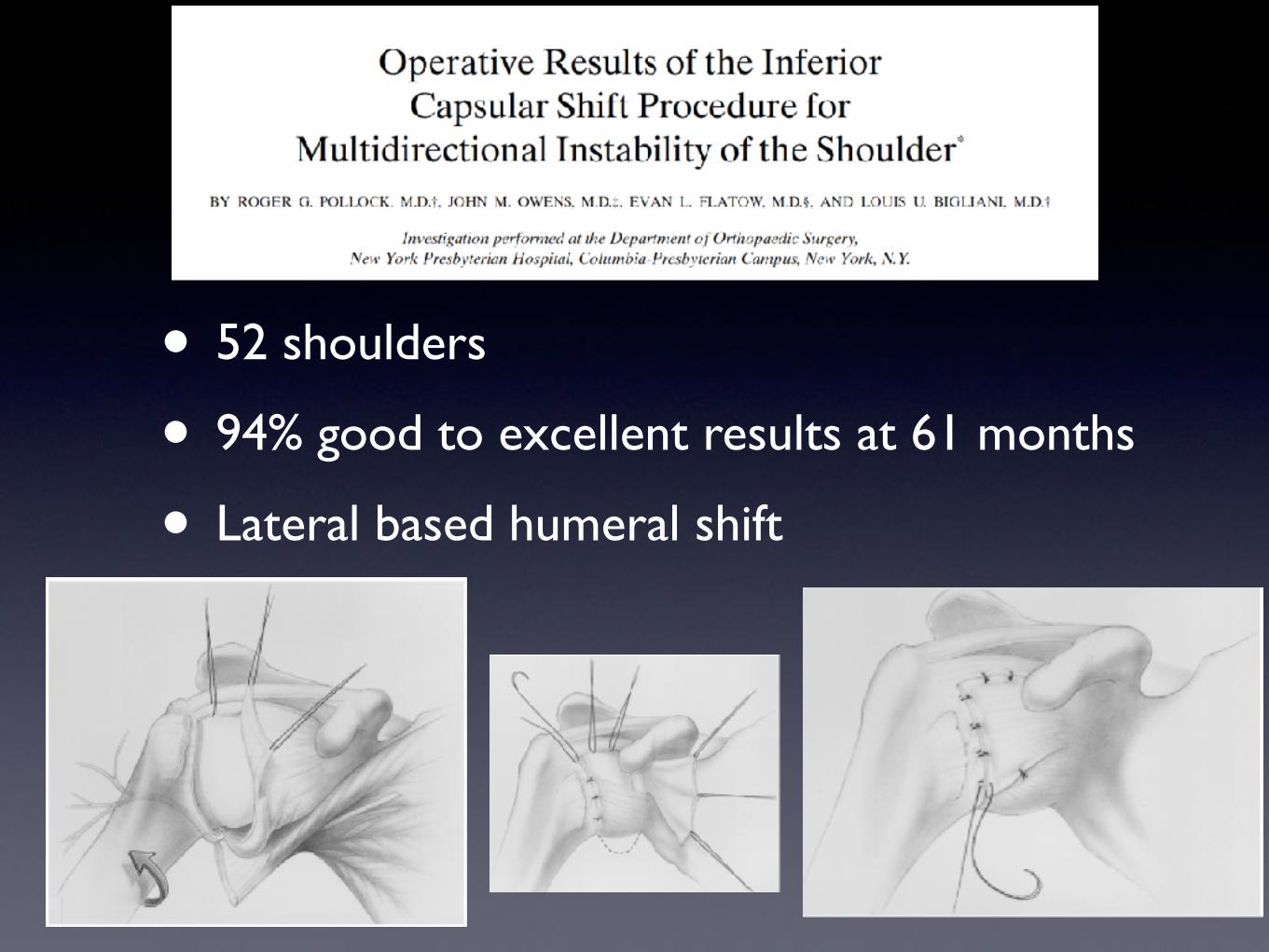
• 52 shoulders
• 94% good to excellent results at 61 months
• Lateral based humeral shift

Arthroscopic Results
• Gartsman: 47 patients, ATS shift
• 94% G/E results at 5 years
• ASES: 94 with RTS 85% Arthroscopy 2001
• Baker: 43 athletes, ATS Shift
• ASES: 91, WOSI: 91, 86% RTS AJSM 2009
• Snyder: 83% G/E ortho Clin North Am 2003

Cadaver Studies: Arthroscopic Shift
• Multiple pleats progressively decrease volume of the capsule
• Flanigan. Arthroscopy 2006
• Anterior, posterior, inferior pleats decrease capsular volume more than open shift
• Sekiya. Arthroscopy 2007
Cadaver Studies: Arthroscopic Shift
• Suture fixation of capsular pleats directly to labrum similar load to failure as anchors
• Anchor provides more rigid fixation
• Anchors recommended when labrum hypo plastic
• Provencher. Arthroscopy 2008

Lateral Decubitus Position
• Provides hands free lateral traction
• Facilitates access to inferior and posterior quadrant
• Positions the surgeon at the head of the table with access to both anterior/posterior shoulder (360 degree access)

Portal Placement

7 O’clock Portal

Diagnostic Arthroscopy
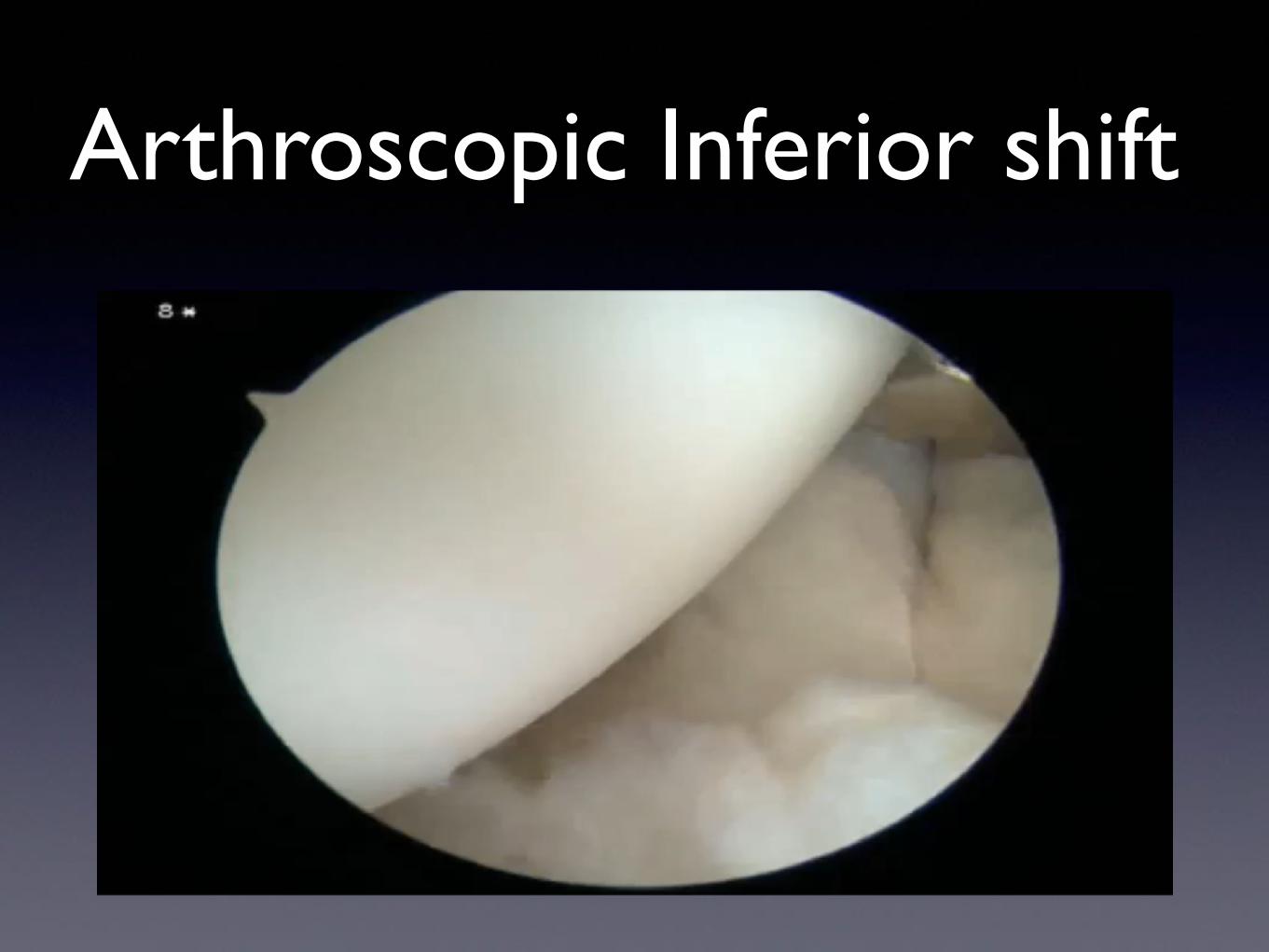
Arthroscopic Inferior shift
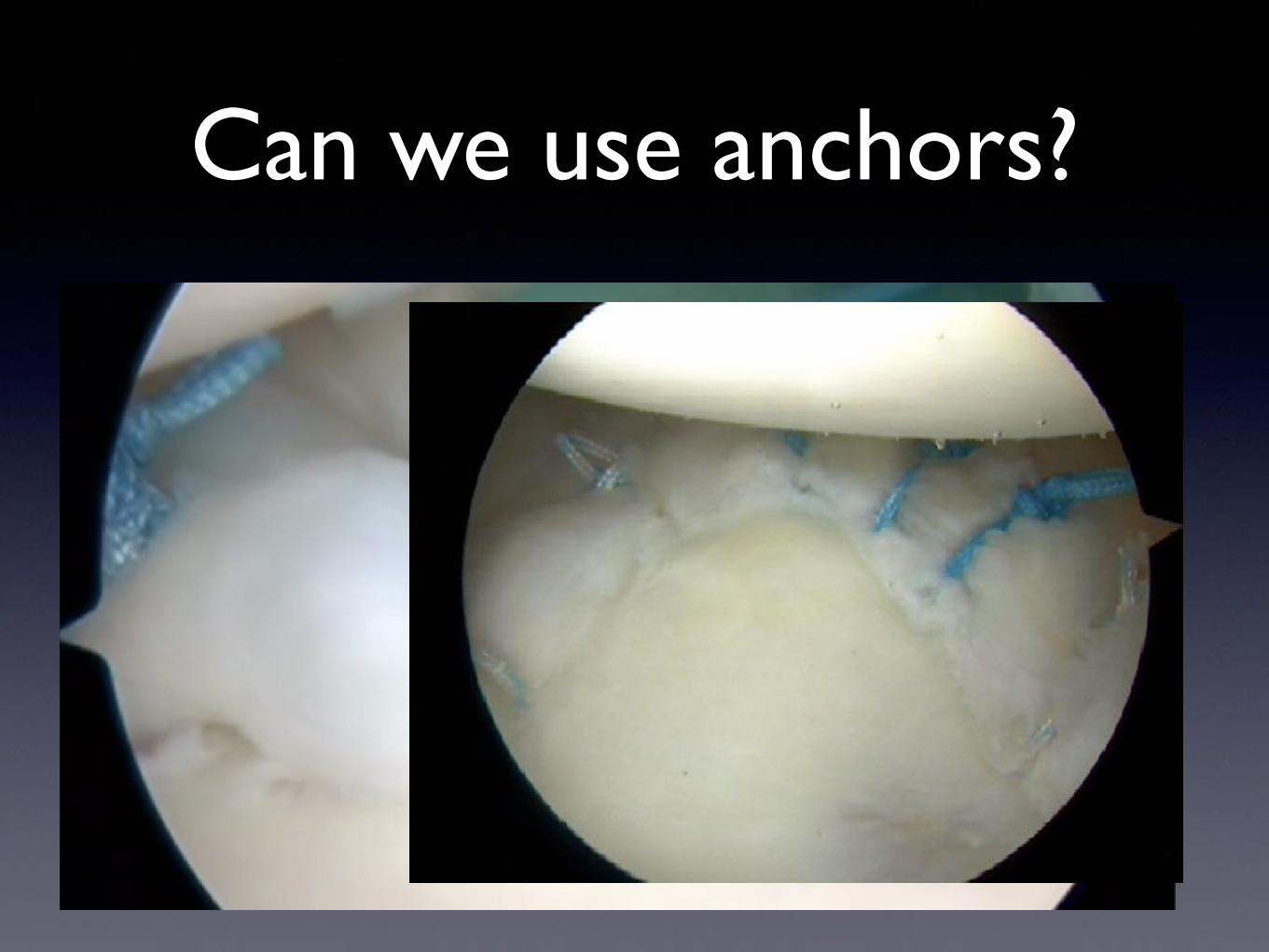
Can we use anchors?

Post-Op Rehabilitation
• Immobilize 6 weeks
• Scapular rehab week #1
• Consider Scapular brace/tape
• Avoid stretching in therapy
• Don’t shoot for Full Flexion until 12 weeks
• Nervous?….pool work with loosen up if stiff
Conclusion
• Arthroscopic Capsular shift is my preference
• Allows for “dialing” in your surgery
• Absorbable suture to labrum works in younger patients
• Suture anchors works:
• Deficient labrum
• ? revisions

Thank You
• www.scotttrenhailemd.com