2018 clinical revisions - interqual review manager · american medical association, 515 ... review...
TRANSCRIPT

Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 1
InterQual® Specialty Referral Criteria
2018 Clinical Revisions
Proprietary Notice and Disclaimers
General Terms: Change Healthcare LLC and/or one of its subsidiaries (“Change Healthcare”) is the owner/licensor of InterQual® Clinical
Decision Support Criteria (the “Clinical Content” or the “Work”). Change Healthcare has prepared this Work for exclusive use of its
licensees of software applications embodying the Clinical Content. This Work contains confidential and trade secret information of
Change Healthcare and is provided to licensees who have an existing license agreement in force only under the time-limited license as
provided under that license agreement. Licensee and any recipient shall use the Work in accordance with the terms and conditions of
the license agreement.
Proprietary Notice: The Work is protected under United States and international copyright and other intellectual property laws. If this Work
is delivered pursuant to a federal government contract that requires the conveyance of rights in data to the government, it is
understood that the Work, including commercial software, clinical content, third-party software, documentation and/or other technical
data, was developed exclusively at Change Healthcare's private expense, and that Change Healthcare will convey only limited or
restricted rights in the Work to the government consistent with the guidance set forth in the Federal Acquisition Regulation (“FAR”)
and/or FAR Supplements. Conveyance of any additional rights beyond limited or restricted rights in the Work requires Change
Healthcare’s express consent contained in a separate written agreement.
© 2018 Change Healthcare LLC and/or one of its subsidiaries. All rights reserved.
Produced in Cork, Ireland.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 2
Acknowledgments and Disclaimer: The Clinical Content is developed by Change Healthcare’s clinical research staff which includes
physicians, registered nurses, and other healthcare professionals. Many of Change Healthcare's clinical staff hold advanced degrees
and case management certification. The Clinical Content is reviewed and validated by a national panel of clinicians and medical
experts, including those in community and academic practice settings, as well as within the managed care industry throughout the
United States. The Clinical Content is a synthesis of evidence-based standards of care, current practices, and consensus from licensed
specialists and/or primary care physicians.
The Clinical Content reflects clinical interpretations and analyses and cannot alone either resolve medical ambiguities of particular
situations or provide the sole basis for definitive decisions. The Clinical Content is intended solely for use as screening guidelines with
respect to the medical appropriateness of healthcare services and not for final clinical or payment determinations concerning the type
or level of medical care provided, or proposed to be provided, to a patient.
THE WORK IS PROVIDED “AS IS.” CHANGE HEALTHCARE DISCLAIMS ANY OTHER WARRANTY, EXPRESS OR IMPLIED, INCLUDING AS TO
MERCHANTABILITY AND FITNESS FOR A PARTICULAR PURPOSE OR SERVICE OF THE WORK, OR THE COMPATIBILITY OF OUTPUT USING THE
WORK WITH ANY LAW, REGULATION, OR ORDER. IN NO EVENT SHALL CHANGE HEALTHCARE BE LIABLE FOR SPECIAL, INCIDENTAL,
CONSEQUENTIAL, OR EXEMPLARY DAMAGES IN CONNECTION WITH, OR ARISING OUT OF, ANY USE OF THE WORK.
Trademarks: InterQual® is a trademark of Change Healthcare LLC and/or one of its subsidiaries. All other trademarks are the property of
their respective owners.
Third Party Notices:
AMA CPT® Codes: The Work may incorporate the CPT® terminology developed and copyrighted by the American Medical Association
(“AMA”). The CPT codes and terminology are provided pursuant to a license agreement between Change Healthcare and the AMA.
CPT copyright 2017 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or
related components are not assigned by the AMA, are not part of CPT, and the AMA is not recommending their use. The AMA does not
directly or indirectly practice medicine or dispense medical services. The AMA assumes no liability for data contained or not contained
herein. CPT is a registered trademark of the American Medical Association.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 3
Applicable FARS/DFARS Restrictions Apply to Government Use.
U.S. Government Rights
This product includes CPT which is commercial technical data and/or computer data bases and/or commercial computer software
and/or commercial computer software documentation, as applicable, which was developed exclusively at private expense by the
American Medical Association, 515 North State Street, Chicago, Illinois, 60654. U.S. Government rights to use, modify, reproduce, release,
perform, display, or disclose these technical data and/or computer data bases and/or computer software and/or computer software
documentation are subject to the limited rights restrictions of DFARS 252.227-7015(b)(2) (November 1995) and/or subject to the
restrictions of DFARS 227.7202-1(a) (June 1995) and DFARS 227.7202-3(a) (June 1995), as applicable, for U.S. Department of Defense
procurements and the limited rights restrictions of FAR 52.227-14 (December 2007) and/or subject to the restricted rights provisions of FAR
52.227-14 (December 2007) and FAR 52.227-19 (December 2007), as applicable, and any applicable agency FAR Supplements, for non-
Department of Defense Federal procurements.
Review and Incorporation of Recent Medical Literature
Change Healthcare is committed to keeping the InterQual product suite current and accurate. Criteria are continually reviewed and
updated, with new editions of every product released at least annually. Change Healthcares' staff of physicians, nurses, other licensed
healthcare professionals, and its extensive array of primary care and specialty consultants participate in ongoing criteria revision as new
medical information emerges. Each release of the criteria reflects a thorough review of new medical literature, society guidelines,
current practice standards, and incorporation of expert clinical consultant and user feedback.
Customer Hub
The Customer Hub (https://customerhub.changehealthcare.com) provides interactive support, answers to commonly asked questions,
and links to other resources. Need a user ID and password? Click the link above and then click the "Need a user ID and password?" link.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 4
Organization and features
Although some revisions below apply to all criteria subsets, the revisions will only display in new criteria sets or in those that were updated
this cycle. Criteria subsets that were not updated this cycle will be updated in the next revision cycle.
Criteria-Specific Changes
Category: Cardiovascular Disorders
Subset Indication Revision Rationale
Congenital
Heart Disease
Changed indication "Congenital heart
disease by TTE/Hx with CXR results available"
to "Congenital heart disease by transthoracic
or transesophageal echocardiogram or by
history”
Congenital heart disease can be diagnosed by
transesophageal echocardiogram, in addition to
transthoracic echocardiogram.
Congenital
Heart Disease
Congenital heart
disease by
transthoracic or
transesophageal
Added "New symptoms or findings and CXR
results available"
Cardiology management may be needed when
the patient with congenital heart disease has
new symptoms or findings.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 5
Subset Indication Revision Rationale
echocardiogram
or by history
Congenital
Heart Disease
Congenital heart
disease by
transthoracic or
transesophageal
echocardiogram
or by history
Added "Follow-up" Cardiology management is appropriate for an
adult with congenital heart disease.
Congenital
Heart Disease
Congenital heart
disease by
transthoracic or
transesophageal
echocardiogram
or by history
Added "Pregnancy" Cardiology management and consultation with
a high-risk obstetrician are appropriate for a
woman who is pregnant or contemplating
pregnancy who has congenital heart disease.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 6
Subset Indication Revision Rationale
Hypertension
(HTN)
Hypertensive
emergency
Changed “Systolic BP > 160 mmHg” and
“Diastolic BP > 100 mmHg” to “Systolic BP ≥
160 mmHg” and “Diastolic BP ≥ 100 mmHg”
under “Elevated BP”
Referral to a specialist should include patients
with a systolic BP of 160 mmHg or a diastolic BP of
100 mmHg.
Hypertension
(HTN)
Hypertensive
urgency
Changed “Systolic BP > 160 mmHg” and
“Diastolic BP > 100 mmHg” to “Systolic BP ≥
160 mmHg” and “Diastolic BP ≥ 100 mmHg”
under “Elevated BP”
Referral to a specialist should include patients
with a systolic BP of 160 mmHg or a diastolic BP of
100 mmHg.
Hypertension
(HTN)
Continued
hypertension
(HTN) after
treatment
Changed “Systolic BP > 140 mmHg” to
“Systolic BP ≥ 140 mmHg” under “Findings”
Referral to a specialist should include patients
with a systolic BP of 140 mmHg.
Hypertension
(HTN)
Continued
hypertension
Changed “Diastolic BP > 90 mmHg” to
“Diastolic BP ≥ 90 mmHg” under “Findings”
Referral to a specialist should include patients
with a diastolic BP of 90 mmHg.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 7
Subset Indication Revision Rationale
(HTN) after
treatment
Hypertension
(HTN)
Continued
hypertension
(HTN) after
treatment
Changed “Systolic BP > 130 mmHg with
DM/chronic renal disease by Hx” to “Systolic
BP ≥ 130 mmHg and,” “Predicted 10-year risk
by atherosclerotic cardiovascular disease
(ASCVD) calculator ≥ 10%,” “Coronary artery
disease (CAD) by history,” “Heart failure (HF)
by physical examination or chest x-ray,”
“Stroke or transient ischemic attack (TIA) by
history,” “Diabetes mellitus (DM) by history,”
and “Chronic renal disease by history” under
“Findings”
Joint guidelines from the American Heart
Association and the American College of
Cardiology recommend pharmacological and
nonpharmacological interventions for patients
with a systolic BP of 130 mmHg or more when
there is a history of cardiovascular disease or an
estimated 10-year atherosclerotic cardiovascular
disease risk of 10% or more.
Hypertension
(HTN)
Continued
hypertension
Changed “Diastolic BP > 80 mmHg with
DM/chronic renal disease by Hx” to “Diastolic
BP ≥ 80 mmHg and,” “Predicted 10-year risk
Joint guidelines from the American Heart
Association and the American College of
Cardiology recommend pharmacological and

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 8
Subset Indication Revision Rationale
(HTN) after
treatment
by atherosclerotic cardiovascular disease
(ASCVD) calculator ≥ 10%,” “Coronary artery
disease (CAD) by history,” “Heart failure (HF)
by physical examination or chest x-ray,”
“Stroke or transient ischemic attack (TIA) by
history,” “Diabetes mellitus (DM) by history,”
and “Chronic renal disease by history” under
“Findings”
nonpharmacological interventions for patients
with a diastolic BP of 80 mmHg or more when
there is a history of cardiovascular disease or an
estimated 10-year atherosclerotic cardiovascular
disease risk of 10% or more.
Hypertension
(HTN)
Renovascular
hypertension
(HTN)
Changed “Systolic BP > 140 mmHg” and
“Diastolic BP > 90 mmHg” to “Systolic BP ≥ 140
mmHg” and “Diastolic BP ≥ 90 mmHg” under
“Findings”
Referral to a specialist should include patients
with a systolic BP of 140 mmHg or a diastolic BP of
90 mmHg.
Myocarditis Changed indication "Acute myocarditis" to
"Suspected acute myocarditis"
Without doing an endomyocardial biopsy and
looking at the histology, a diagnosis of
myocarditis can only be suspected based on

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 9
Subset Indication Revision Rationale
history, examination, laboratory studies, and
imaging findings.
Myocarditis Suspected acute
myocarditis
Added "Symptoms," “Chest pain,” “New
onset or worsening heart failure or dyspnea,”
“Palpitations,” “Syncope,” “or Cardiogenic
shock”
Although not all patients with acute myocarditis
are symptomatic, the primary care provider
would not suspect acute myocarditis unless the
patient had the symptoms as listed.
Myocarditis Suspected acute
myocarditis
Changed "Cardiac enzyme/C-reactive
protein/ESR elevation" to "Cardiac enzyme
results available"
C-reactive protein and ESR are nonspecific
markers of inflammation so they may not be
checked in all patients with suspected
myocarditis. Cardiac enzymes should be
checked, however, to exclude myocardial
ischemia as a cause of the patient's symptoms.
Myocarditis Suspected acute
myocarditis
Added "Chest x-ray results available" Chest x-ray should be done in the evaluation of
suspected myocarditis to exclude other causes
of the patient's symptoms.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 10
Category: Dermatologic Disorders
Subset Indication Revision Rationale
Acne, Rosacea,
and Perioral
Dermatitis
Acne Removed "Topical Abx ≥ 8 wks" under
"Continued findings after Rx" and changed
TWO "Medications" to ONE
Although combination therapy is likely more
effective, monotherapy can be tried first line in
the treatment of mild acne. Topical antibiotics
can be tried but should not be used alone.
Atopic Dermatitis
(Eczema)
Changed indication “Atopic dermatitis
(eczema)” to “Atopic dermatitis (eczema)
by physical examination”
This change was made to clarify that the
patient was being referred for current findings
and not a history of eczema.
Atopic Dermatitis
(Eczema)
Added indication "Atopic dermatitis by
history"
A dermatologist may follow a patient with
ongoing symptoms or findings of atopic
dermatitis.
Atopic Dermatitis
(Eczema)
Atopic dermatitis
(eczema) by
physical
examination
Added "Allergist" to the list of specialists
appropriate for referral
An allergist, as well as a dermatologist, may be
involved in the care of a patient with atopic
dermatitis.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 11
Subset Indication Revision Rationale
Drug Eruptions and
Hypersensitivity
Syndromes
Drug eruption Changed "Erythematous macules/papules
by PE" to "Erythematous macules or
papules or bullae by physical examination"
Some drugs can cause a bullous reaction.
Drug Eruptions and
Hypersensitivity
Syndromes
Erythema
multiforme
Added "Oral mucosa" under "Involved
area"
In addition to the trunk or extremities, the oral
mucosa may be involved in erythema
multiforme.
Drug Eruptions and
Hypersensitivity
Syndromes
Stevens−Johnson
syndrome or
toxic epidermal
necrolysis (TEN)
Added "Ophthalmologist,” “Critical Care
Specialist,” and “Infectious Disease
Specialist" to the list of specialists
appropriate for referral
Referral to these specialists, in addition to a
dermatologist, may be appropriate for the
diagnosis or management of a patient with
Stevens-Johnson syndrome or toxic epidermal
necrolysis.
Drug Eruptions and
Hypersensitivity
Syndromes
Changed indications "Stevens-Johnson
syndrome" and "Toxic epidermal necrolysis
(TEN)" to "Stevens-Johnson syndrome or
toxic epidermal necrolysis (TEN)"
Stevens-Johnson syndrome and toxic
epidermal necrolysis are both severe
mucutaneous drug reactions, distinguished

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 12
Subset Indication Revision Rationale
only by severity and percent body surface
area involved.
Drug Eruptions and
Hypersensitivity
Syndromes
Stevens−Johnson
syndrome or
toxic epidermal
necrolysis (TEN)
Change the rule of BOTH "Erythema" and
"Exfoliation" to "Erythema or exfoliation"
under "Skin findings"
The patient may only have erythema if early in
the presentation.
Drug Eruptions and
Hypersensitivity
Syndromes
Stevens-Johnson
syndrome or
toxic epidermal
necrolysis (TEN)
Added "Involved area," "Trunk," "Palms or
soles," or Extremities" under "Skin findings"
These areas represent the usual distribution of
Stevens Johnson syndrome or toxic epidermal
necrolysis.
Drug Eruptions and
Hypersensitivity
Syndromes
Erythema
nodosum
Removed “Distribution” and “Bilateral” The primary distribution of erythema nodosum
is the extensor aspect of the extremities, which
is not always bilateral.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 13
Subset Indication Revision Rationale
Drug Eruptions and
Hypersensitivity
Syndromes
Erythema
nodosum
Added "Tuberculin skin test (TST) or
interferon gamma release assay (IGRA)"
under "Tests nondiagnostic for etiology of
erythema nodosum"
The individual should be tested to exclude
tuberculosis as a cause of erythema nodosum.
Hair Disorders Androgenetic
alopecia in
female patient
Removed "Periodic Assessment" as a
reason for specialty involvement
The primary care provider can follow a woman
with androgenetic alopecia long-term.
Hidradenitis
Suppurativa
Hidradenitis
suppurativa
Added "Severe disease" under "Findings" Referral for evaluation of a patient with severe
disease at initial presentation, not only
recurrent nodules or abscesses, is appropriate.
Infections of the
Skin, Bacterial
Folliculitis Changed "Continued findings after
systemic Abx ≥ 10 days" to "Continued
findings after systemic antibiotics"
A full course of systemic antibiotics, not
necessarily 10 days or longer, should have
been tried.
Infections of the
Skin, Bacterial
Impetigo Added "Oral antibiotics ≥ 7 days" under
"Continued findings after treatment"
Oral antibiotics should be tried if there is no
resolution of findings after topical treatment.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 14
Subset Indication Revision Rationale
Infections of the
Skin, Bacterial
Suspected
erythema
migrans
(cutaneous
Lyme disease)
Added "Oral antibiotics ≥ 10 days" The primary care provider should treat
erythema migrans with oral antibiotics, as
these have been shown to be effective in
eradicating Borrelia bacteria.
Infections of the
Skin, Fungal
Changed indication "Tinea versicolor" to
"Tinea (pityriasis) versicolor"
This change was made to reflect current
medical terminology.
Infections of the
Skin, Fungal
Tinea capitis Changed "Continued findings after oral
antifungal Rx ≥ 6 wks" to "Continued
findings after oral antifungal treatment ≥ 4
weeks"
Treatment for 4, not 6, weeks is sufficient to see
improvement in tinea capitis.
Infections of the
Skin, Fungal
Tinea barbae Changed "Oral antifungal Rx ≥ 6 wks" to
"Oral antifungal treatment ≥ 4 weeks"
Treatment for 4, not 6, weeks is sufficient to see
improvement in tinea barbae.
Infections of the
Skin, Viral
Removed indication "Molluscum
contagiosum"
Molluscum contagiosum can be managed by
the primary care provider.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 15
Subset Indication Revision Rationale
Infections of the
Skin, Viral
Herpes simplex Changed "≥ 5 episodes in 1 year, with
continued findings despite prophylactic
treatment" to "≥ 5 episodes in 1 year, with
continued findings despite suppressive
treatment"
This change was made to reflect current
medical terminology.
Infections of the
Skin, Viral
Herpes simplex Changed "< 5 episodes in 1 year, with
continued findings after abortive
treatment" to "< 5 episodes in 1 year, with
continued findings after episodic
treatment"
This change was made to reflect current
medical terminology.
Insect Infestations Scabies Changed "Continued findings after topical
permethrin x2 applications" to "Continued
findings after topical permethrin x2
applications, ≥ 1 week apart"
This change was made to clarify the time
between permethrin applications.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 16
Subset Indication Revision Rationale
Insect Infestations Scabies Added "Crusted (Norwegian) scabies"
under "Findings"
Crusted scabies is treated differently than
classic scabies.
Insect Infestations Scabies Changed "Household contacts treated" to
"Close contacts treated"
All close contacts, not only household
members, should be treated, as they can
transmit scabies even if asymptomatic.
Neoplasms and
Hyperplasias of the
Skin, Benign
Skin tag
(acrochordon)
Removed "Diagnosis" as a reason for
specialty involvement
Skin tags can be diagnosed by the primary
care provider and referral to the specialist is
not needed.
Neoplasms and
Hyperplasias of the
Skin, Benign
Keloid or
hypertrophic
scar
Added "Symptomatic," "Pain or pruritus," or
"Sensitive to touch or hyperesthesia," or
"Interferes with activities of daily living
(ADLs)"
In addition to growth or the need for
counseling, specialist involvement may be
appropriate for keloids or scars that are
symptomatic or interfere with functioning.
Neoplasms of the
Skin, Malignant and
Premalignant
Melanoma Changed "Change in shape/size/ color" to
"Evolution or change in shape or size or
color"
This change was made to complete the
ABCDE's of skin changes that make one
suspect melanoma.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 17
Subset Indication Revision Rationale
Neoplasms of the
Skin, Malignant and
Premalignant
Dysplastic nevus Changed "Change in shape/size/ color" to
"Evolution or change in shape or size or
color"
This change was made to complete the
ABCDE's of skin changes that make one
suspect dysplastic changes.
Neoplasms of the
Skin, Malignant and
Premalignant
Squamous cell
carcinoma
Removed "Plastic Surgeon" from the list of
specialists appropriate for referral for
“Periodic Assessment”
The dermatologist, not the surgeon who
removed the patient's lesion, would
periodically assess the patient.
Neoplasms of the
Skin, Malignant and
Premalignant
Basal cell
carcinoma
Removed "Plastic Surgeon" from the list of
specialists appropriate for referral for
“Periodic Assessment”
The dermatologist, not the surgeon who
removed the patient's lesion, would
periodically assess the patient.
Neoplasms of the
Skin, Malignant and
Premalignant
Periodic skin
screening
examination for
high−risk patient
Changed “Frequent sunburns/chronic sun
exposure by Hx” to “Frequent sunburns or
chronic sun exposure or indoor tanning
bed use by history”
The use of indoor tanning booths, as well as
frequent sunburns or chronic sun exposure, can
put the patient at increased risk of developing
skin cancer.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 18
Subset Indication Revision Rationale
Neoplasms of the
Skin, Malignant and
Premalignant
Periodic skin
screening
examination for
high−risk patient
Changed "Oculocutaneous albinism by Hx"
to "Oculocutaneous albinism or basal cell
nevus syndrome by history or physical
examination"
Basal cell nevus syndrome can put a young
adult at risk for the early development of basal
cell carcinoma.
Neoplasms of the
Skin, Malignant and
Premalignant
Periodic skin
screening
examination for
high−risk patient
Added "Red hair color or multiple freckles
by physical examination" and
"Immunocompromised patient"
These findings put the individual at higher risk of
developing skin cancer and periodic
assessment by the dermatologist is
appropriate.
Psoriasis Psoriasis by
physical
examination
Added "≥ 10% body surface area (BSA),"
"Guttate or pustular or nail psoriasis,"
"Localized disease causing functional
impairment or affecting hands or feet or
face or genitals or intertriginous areas," and
"Psoriatic arthritis present"
These findings justify referral to a dermatologist
without any treatment by the primary care
provider prior, as these findings require
treatment with therapies provided by the
specialist (e.g., phototherapy, biologic
agents).

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 19
Subset Indication Revision Rationale
Psoriasis Psoriasis by
physical
examination
Added "Treatment x 2 weeks and face or
genitalia or flexures involved" under
"Continued findings after topical
corticosteroid"
Topical corticosteroid use should be limited to
2 weeks when treating psoriasis of the face,
genitals, or flexure surfaces.
Seborrheic
Dermatitis
Added indication "Seborrheic dermatitis by
history"
Periodic assessment by a dermatologist is
reasonable for individuals with seborrheic
dermatitis who require maintenance therapy.
Seborrheic
Dermatitis
Seborrheic
dermatitis by
physical
examination
Changed "Continued findings after
antiseborrheic shampoo/cream ≥ 2 wks" to
"Scalp and ketoconazole or zinc pyrithione
or selenium sulfide or ciclopirox shampoo ≥
4 weeks" and "Non scalp and
ketoconazole and hydrocortisone cream ≥
4 weeks" under "Localized and continued
findings after treatment"
Evidence supports these first-line treatments
and recommends at least 4, not 2, weeks of
therapy prior to considering second-line
medications.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 20
Subset Indication Revision Rationale
Seborrheic
Dermatitis
Seborrheic
dermatitis by
physical
examination
Added "Distribution," "Widespread or
severe disease," and "Localized and
continued findings after treatment"
Early referral is appropriate for severe or
widespread disease without the need for
treatment by the primary care provider prior to
referral.
Skin
Symptoms/Findings,
Unknown Etiology
Changed indications "Localized pruritus"
and "Diffuse pruritus" to "Acute pruritus" and
"Chronic pruritus"
The work-up of pruritus is typically based on
duration, not location, of the pruritus.
Skin
Symptoms/Findings,
Unknown Etiology
Acute pruritus Added "Pruritus < 6 weeks" Acute pruritus is defined as itching lasting less
than 6 weeks.
Skin
Symptoms/Findings,
Unknown Etiology
Acute pruritus Added "Aggravating medications or
substances," "Avoidance ≥ 2 weeks," and
"Not applicable"
This change was made to address any
medications or substances, if applicable, that
could be causing pruritus.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 21
Subset Indication Revision Rationale
Skin
Symptoms/Findings,
Unknown Etiology
Chronic pruritus Added "Pruritus ≥ 6 weeks" Chronic pruritus is defined as itching lasting 6 or
more weeks.
Skin
Symptoms/Findings,
Unknown Etiology
Chronic pruritus Added "Aggravating medications or
substances," "Avoidance ≥ 2 weeks," and
"Not applicable"
This change was made to address any
medications or substances, if applicable, that
could be causing pruritus.
Skin
Symptoms/Findings,
Unknown Etiology
Exanthematous
or morbilliform or
maculopapular
eruption
Added "Generalized or widespread
eruption" under "Findings"
Immediate referral without a period of
observation is appropriate if the skin eruption is
widespread.
Skin
Symptoms/Findings,
Unknown Etiology
Petechiae Added "Hematologist" to the list of
specialists appropriate for referral
A hematologist may be helpful in the
evaluation of petechiae, as they may be
secondary to vasculitis or thrombocytopenia.
Urticaria and
Angioedema
Acute urticaria Removed "Oral corticosteroid," "Rx ≥ 1 wk,"
and "Contraindicated/not tolerated" under
Antihistamine monotherapy is preferred for
treating acute urticaria; corticosteroids would

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 22
Subset Indication Revision Rationale
"Continued symptoms or findings after
treatment"
only be necessary if there were respiratory
symptoms.
Urticaria and
Angioedema
Acute urticaria Changed "Antihistamine ≥ 1 wk" to
"Antihistamine ≥ 2 weeks"
Acute urticaria will usually resolve with
treatment in 10 to 14 days, so 2 weeks, not 1
week, of treatment should be tried before
considering referral.
Urticaria and
Angioedema
Chronic urticaria Added “Continued symptoms or findings
after treatment” and "Antihistamine ≥ 2
weeks"
Antihistamine treatment is standard in cases of
chronic urticaria and should be tried by the
primary care provider prior to referral.
Urticaria and
Angioedema
Angioedema
with systemic
symptoms
Added "Critical Care Specialist" to the list of
specialists appropriate for referral
Patients with angioedema with systemic
symptoms are at risk of airway edema and the
need for mechanical ventilation and may
require management in the intensive care unit.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 23
Subset Indication Revision Rationale
Vasculitis Involving
the Skin
Suspected
vasculitis
Added "Hepatitis B and C serology," "HIV,"
"Streptococcal titer," and "Chest x-ray"
under "Test results available"
These tests, in addition to the others listed,
should be done to evaluate the presence of
infection or hepatitis as a cause of the
vasculitis.
Category: Endocrine Disorders
Subset Indication Revision Rationale
Adrenal
Disorders
Changed indication "Incidental unilateral
adrenal mass" to "Incidental adrenal mass"
Evaluation by a specialist is appropriate for both
unilateral and bilateral incidental masses.
Adrenal
Disorders
Incidental adrenal
mass
Changed “24 hr urine VMA/metanephrine”
or "24-hour urine total catecholamines" to
“24-hour urinary fractionated metanephrine”
or "24-hour urinary total catecholamines"
under “Pheochromocytoma screening
results available”
24-hour urinary fractioned metanephrine is
preferred over a VMA test to screen for
pheochromocytoma. Either test is appropriate
to have available for pheochromocytoma
screening prior to referral to a specialist for an
incidental adrenal mass.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 24
Subset Indication Revision Rationale
Adrenal
Disorders
Incidental adrenal
mass
Added Endocrinologist to the list of specialists
appropriate for referral under “≥ 4 cm or
malignant appearing” for “By imaging”
Although masses 4 cm or greater are typically
removed, intermediate sized masses (4 to 6 cm) may
be monitored with imaging if they are benign
appearing and have not changed in size.
Adrenal
Disorders
Enlarging adrenal
mass
Changed “24-hr urine VMA/metanephrine” or
"24-hour urine total catecholamines" to “24-hour
urinary fractionated metanephrine” or "24-hour
urinary total catecholamines" under
“Pheochromocytoma screening results available”
24-hour urinary fractioned metanephrine is preferred
over a VMA test to screen for pheochromocytoma.
Either test is appropriate to have available for
pheochromocytoma screening prior to referral to a
specialist for an adrenal incidental mass.
Adrenal
Disorders
Pheochromocy-
toma
Changed “24 hr urine VMA/metanephrine” to
“24-hour urinary fractionated metanephrine”
under “Pheochromocytoma screening results
available”
24-hour urinary fractioned metanephrine is preferred
over a VMA test to screen for pheochromocytoma.
Adrenal
Disorders
Pheochromocy-
toma
Changed “Plasma catecholamine > normal” to
“Plasma free metanephrine > normal”
Plasma free metanephrine is preferred over plasma
catecholamine as the initial serum test for
pheochromocytoma.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 25
Subset Indication Revision Rationale
Adrenal
Disorders
Cushing syndrome Changed “24 hour urine free cortisol” or “Late-
night salivary cortisol” and “Abnormal low-dose
dexamethasone suppression test” to ’24-hour
urine free cortisol’ or “Late-night salivary cortisol”
or “Abnormal low-dose dexamethasone
suppression test”
Specialty referral is indicated based on an abnormal
24-hour urine free cortisol or late-night salivary cortisol
test without the additional testing with a low-dose
dexamethasone suppression test.
Adrenal
Disorders
Hypoaldosteronism Changed “K ≥ 4.8” to “K ≥ 5.5 mEq/L (5.5
mmol/L)” under “Suspected hypoaldosteronism”
An elevated potassium (5.5) is an indication of
hypoaldosteronism.
Diabetes
Insipidus (DI)
Diabetes Insipidus
(DI)
Changed “Polyuria ≥ 2.5 L/day” to “Polyuria ≥ 3.0
L/day”
Diabetes insipidus is suspected in adults when the
urine output is 3 liters or more per day.
Diabetes
Insipidus (DI)
Diabetes Insipidus
(DI)
Changed “Serum osmolality ≥ 280 mOsm/kg (300
mmol/kg)” to “Serum osmolality ≥ 300 mOsm/kg
(300 mmol/kg)”
A serum osmolality of 300 or greater, with a urine
osmolality of less than 200, is an indication of diabetes
insipidus.
Diabetes
Mellitus (DM)
Added "Continuous glucose monitoring (CGM)" Decisions regarding the use of continuous glucose
monitoring should involve a diabetes specialist.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 26
Subset Indication Revision Rationale
Diabetes
Mellitus (DM)
Diabetic
ketoacidosis (DKA)
Changed "Glucose > 200 mg/dL (11.0 mmol/L)" to
"Glucose > 250 mg/dL (13.88 mmol/L)"
Glucose levels are generally greater than 250 mg/dL,
not 200 mg/dL, in patients with diabetic ketoacidosis.
Diabetes
Mellitus (DM)
Diabetic
ketoacidosis (DKA)
Changed "≥ 2 episodes w/in 6 mos" to "≥ 2
episodes"
Patients who have had recurrent episodes of diabetic
ketoacidosis should be evaluated by a diabetes
specialist for education on risk factors and
medication adherence, regardless of when the
episodes occurred.
Diabetes
Mellitus (DM)
Hyperosmolar
hyperglycemic state
Added "No acidosis," "Ketones absent,"
"Venous/arterial pH ≥ 7.3," and "No anion gap"
Hyperosmolar hyperglycemia is usually distinguished
from diabetic ketoacidosis because there is no
acidosis by testing.
Diabetes
Mellitus (DM)
Poorly controlled
diabetes mellitus
(DM)
Removed "Requiring insulin ≥ 6 mos" under "Type 2
DM"
The PCP should be able to manage a Type 2 diabetic
patient who requires insulin.
Diabetes
Mellitus (DM)
Poorly controlled
diabetes mellitus
(DM)
Changed "Erratic glucose measurements ("brittle"
Type 1 DM)" to "Erratic glucose measurements
(brittle DM)"
Some experts believe that brittle diabetes can occur
in patients with Type 2, as well as Type 1, diabetes
mellitus.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 27
Subset Indication Revision Rationale
Diabetes
Mellitus (DM)
Pregnancy Removed "Ophthalmologist" from the list of
specialists appropriate for referral for “Current
pregnancy and diabetes mellitus (DM) by history”
An ophthalmologist would only need to be involved in
the care of a diabetic woman if she had eye
problems, regardless of whether she was pregnant or
not.
Diabetes
Mellitus (DM)
Pregnancy Removed "Ophthalmologist" from the list of
specialists appropriate for referral for “Pregnancy
planned within 12 weeks and diabetes mellitus
(DM) by history”
An ophthalmologist would only need to be involved in
the care of a diabetic woman if she had eye
problems, regardless of whether she was planning on
getting pregnant or not.
Diabetes
Mellitus (DM)
Diabetic neuropathy Added "Co-Management" as a reason for
specialty involvement for “Peripheral neuropathy
with continued symptoms or findings after
treatment”
Because diabetic neuropathy is a chronic condition,
the specialist may need to manage the patient with
the PCP.
Diabetes
Mellitus (DM)
Foot care Added "Nail clipping/callus trimming" under
"Periodic assessment, high-risk patient"
Nail and callus care by a foot care specialist may
prevent foot ulceration.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 28
Subset Indication Revision Rationale
Diabetes
Mellitus (DM)
Perioperative
management
Changed "Perioperative management of Type 1
DM" to "Perioperative management"
All patients with diabetes, not only those with Type 1
diabetes mellitus, should be monitored before and
after surgery.
Diabetes
Mellitus (DM)
Diabetes education Changed “Periodic Assessment" to "Limited
Management" as a reason for specialty
involvement for "New onset DM (Type 1/Type 2)"
Education for the individual with new onset diabetes
would occur over a few visits. Their continued
education would then be covered by the "Periodic
diabetes education" criteria.
Diabetes
Mellitus (DM)
Peripheral arterial
disease (PAD) with
claudication
Changed "Smoking cessation or reduction ≥ 6
months or nonsmoker" to "Smoking cessation or
reduction ≥ 12 weeks or nonsmoker"
Referral to a specialist is appropriate after 12 weeks,
rather than 6 months, of documented smoking
cessation or reduction in a smoker.
Diabetes
Mellitus (DM)
Peripheral arterial
disease (PAD) with
claudication
Changed "Cholesterol management ≥ 6 months"
to "Statin ≥ 12 weeks or contraindicated or not
tolerated"
Statin therapy improves cardiovascular and limb
outcomes in patients with claudication and other
cholesterol medications have not been shown to
have the same effect. Twelve weeks, rather than 6
months, is sufficient to determine if treatment is
effective.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 29
Subset Indication Revision Rationale
Diabetes
Mellitus (DM)
Peripheral arterial
disease (PAD) with
claudication
Changed "Medication," "Cilostazol or
pentoxyfilline ≥ 6 months," and "Contraindicated
or not tolerated" to Cilostazol ≥ 12 weeks or
contraindicated or not tolerated"
Pentoxyfilline is not effective in the treatment of
claudication. Twelve weeks, rather than 6 months, is
sufficient to determine if treatment is effective.
Hypoglycemia Hypoglycemia,
nondiabetic patient
Changed "Glucose ≤ 50 mg/dL (2.8 mmol/L) to
"Glucose ≤ 55 mg/dL (3 mmol/L)”
Hypoglycemia in a nondiabetic patient is defined as
glucose ≤ 55 mg/dL, not 50 mg/dL.
Hypoglycemia Hypoglycemia,
nondiabetic patient
Changed "Glucose > 50 mg/dL (2.8 mmol/L) and
< 70 mg/dL (3.8 mmol/L) ≥ 1 episode" to "Glucose
> 55 mg/dL (3 mmol/L) and < 70 mg/dL (3.8
mmol/L)"
Referral may be appropriate for any episode of mild
hypoglycemia defined as a glucose between 55
mg/dL (not 50 mg/dL) and 70 mg/dL.
Hypoglycemia Hypoglycemia,
nondiabetic patient
Added "Whipple triad," "Symptoms consistent with
hypoglycemia," "Low plasma glucose
concentration," and "Resolution of symptoms
after plasma glucose concentration raised to
normal level"
The Whipple triad defines true hypoglycemia which
requires further investigation.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 30
Subset Indication Revision Rationale
Hypoglycemia Hypoglycemia,
nondiabetic patient
Changed "Aggravating medications
identified/withdrawn" to "Aggravating
medications or substances," "Identified and
withdrawn," and "Not applicable”
This change was made to cover cases when there
are no medications or substances responsible for
causing the hypoglycemia.
Paget Disease
of Bone
Changed subset title "Paget's Disease" to "Paget
disease of bone"
This change was made to clarify that these criteria
address Paget's disease of the bone and do not
include Paget's disease of the breast.
Paget Disease
of Bone
Changed indication "Paget's disease with
complications" to "Untreated Paget disease of
bone" and "Retreatment of Paget disease of
bone planned"
This change was made to allow for specialist
involvement when the patient requires retreatment of
their Paget disease of bone.
Paget Disease
of Bone
Untreated Paget
disease of bone
Added "Fracture" under "Symptomatic" Involvement of bone by Paget disease can result in
fracture.
Paget Disease
of Bone
Untreated Paget
disease of bone
Added "Rheumatologist" to the list of specialists
appropriate for referral
A rheumatologist, in addition to an endocrinologist,
may evaluate a patient with Paget disease of bone
who develops arthritis.
2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 31
Subset Indication Revision Rationale
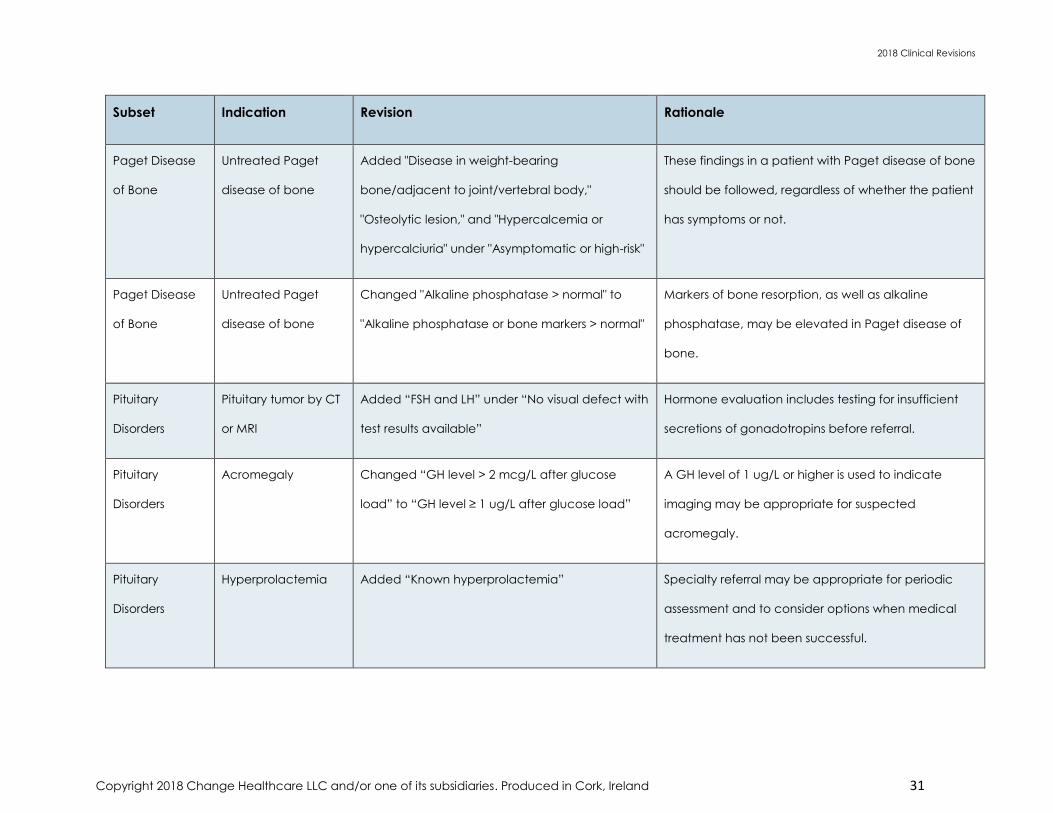
Paget Disease
of Bone
Untreated Paget
disease of bone
Added "Disease in weight-bearing
bone/adjacent to joint/vertebral body,"
"Osteolytic lesion," and "Hypercalcemia or
hypercalciuria" under "Asymptomatic or high-risk"
These findings in a patient with Paget disease of bone
should be followed, regardless of whether the patient
has symptoms or not.
Paget Disease
of Bone
Untreated Paget
disease of bone
Changed "Alkaline phosphatase > normal" to
"Alkaline phosphatase or bone markers > normal"
Markers of bone resorption, as well as alkaline
phosphatase, may be elevated in Paget disease of
bone.
Pituitary
Disorders
Pituitary tumor by CT
or MRI
Added “FSH and LH” under “No visual defect with
test results available”
Hormone evaluation includes testing for insufficient
secretions of gonadotropins before referral.
Pituitary
Disorders
Acromegaly Changed “GH level > 2 mcg/L after glucose
load” to “GH level ≥ 1 ug/L after glucose load”
A GH level of 1 ug/L or higher is used to indicate
imaging may be appropriate for suspected
acromegaly.
Pituitary
Disorders
Hyperprolactemia Added “Known hyperprolactemia” Specialty referral may be appropriate for periodic
assessment and to consider options when medical
treatment has not been successful.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 32
Subset Indication Revision Rationale
Pituitary
Disorders
Cushing disease Added “Periodic assessment” as a reason for
specialty involvement for “Known Cushing
disease”
Specialty referral may be appropriate to monitor
medication management or post surgery follow-up.
Pituitary
Disorders
Hypogonadotropic
hypogonadism
Changed “FSH or LH inappropriately low” to “FSH
or LH inappropriately low related to low
testosterone level” under “Male”
A low FSH or LH level may suggest a pituitary problem
when it is related to a low testosterone level.
Pituitary
Disorders
Hypogonadotropic
hypogonadism
Changed “Estrogen < normal” to “Estrogen ≤
normal” under “Premenopausal female” and
“Postmenopausal female”
A normal estrogen level in conjunction with a low FSH
or LH may warrant specialist evaluation for a pituitary
disorder.
Category: Gastroenterologic Disorders
Subset Indication Revision Rationale
Cancer
Surveillance
Changed indication "Screening exam for patient
age ≥ 50 and ≤ 75 with no risk factors" to
Average-risk patients with gastrointestinal symptoms
should receive diagnostic testing instead of screening
and would be covered in another subset.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 33
Subset Indication Revision Rationale
"Screening examination for asymptomatic patient
age ≥ 50 and ≤ 75 with no risk factors"
Cancer
Surveillance
Changed indication "Surveillance exam for high-
risk patient with familial syndrome" to "Surveillance
examination for high-risk patient with polyposis or
nonpolyposis syndrome"
Not all polyposis or nonpolyposis syndromes (e.g.,
serrated polyposis syndrome) have a proven genetic
component and referral to the specialist for
colonoscopy may be appropriate for any of these
syndromes.
Cancer
Surveillance
Colonic polyp Added "New polyp by barium enema or CT
colonograpy"
Any new polyp found by barium enema or CT
colonography necessitates colonoscopic follow up.
Cancer
Surveillance
Colonic polyp Changed “New adenomatous polyp by
BE/sigmoidoscopy” to “Adenomatous polyp by
sigmoidoscopy”
Any adenomatous polyps found by sigmoidoscopy
necessitates examination of the remaining colon for
additional polyps or cancer.
Cancer
Surveillance
Colonic polyp Changed "Incomplete excision of adenomatous
polyp" to Incomplete excision of adenomatous or
large polyp"
A follow-up post procedure is recommended for any
large colonic polyp to evaluate for, or remove, any
remaining polyp tissue.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 34
Subset Indication Revision Rationale
Cancer
Surveillance
Screening
examination for
patient with
positive family
history
Changed “Age ≥ 40” to “Age ≥ 40 and ≤ 85”
under “Colorectal cancer by history in ≥ 2 first
degree relatives and”
Evidence does not support colorectal screening in
patients 85 or older who have family risk factors in first
degree relatives.
Cancer
Surveillance
Screening
examination for
patient with
positive family
history
Changed “Age ≥ 40” to “Age ≥ 40 and ≤ 85”
under “First degree relative with colorectal cancer
onset or adenomatous colonic polyp diagnosed
age < 60 and”
Evidence does not support colorectal screening in
patients 85 or older who have family risk factors in first
degree relatives.
Cancer
Surveillance
Surveillance
examination for
high−risk patient
with polyposis or
nonpolyposis
syndrome
Added “Serrated polyposis syndrome by
colonoscopy”
Serrated polyposis syndrome is a polyposis syndrome
that needs referral for closer surveillance with
colonoscopy than the randomly appearing polyps.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 35
Subset Indication Revision Rationale
Dysphagia Changed indication "Neuromuscular or transfer
dysphagia" to "Oropharyngeal dysphagia"
This change was made to reflect current medical
terminology, as well as to address mechanical, not
only neuromuscular, disorders.
Dysphagia Oropharyngeal
dysphagia
Changed "CVA by Hx" to "Neurologic disorder by
history"
Other neurologic conditions (e.g., amyotrophic lateral
sclerosis, multiple sclerosis, Parkinson disease), not only
stroke, can cause dysphagia.
Dysphagia Oropharyngeal
dysphagia
Changed “Nasal regurgitation” to “Oral or nasal
regurgitation”
Patients with oropharyngeal dysphagia may have
oral, as well as nasal, regurgitation.
Dysphagia Changed indication "Dysphagia with known
esophageal disease" to "Esophageal dysphagia"
This change was made to reflect current medical
terminology.
Dysphagia Esophageal
dysphagia
Changed "Stricture" to "Esophageal stricture or
web or ring"
Esophageal webs and rings, as well as strictures, can
cause dysphagia.
Dysphagia Esophageal
dysphagia
Added "Esophagitis or esophageal cancer" and
"Radiation or caustic injury or esophageal surgery
by history"
Dysphagia caused by any of these conditions should
be evaluated by the specialist.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 36
Subset Indication Revision Rationale
Nausea and
Vomiting
Nausea and
vomiting, unknown
etiology
Changed "Amylase normal" to "Amylase or lipase
normal"
Lipase, as well as amylase, can be done to exclude
pancreatitis as a cause of the patient's symptoms.
Nausea and
Vomiting
Nausea and
vomiting, unknown
etiology
Added "TSH normal" Hypothyroidism can result in nausea and vomiting.
Nausea and
Vomiting
Nausea and
vomiting, unknown
etiology
Added "Medications deemed noncontributory" Certain medications can result in nausea and
vomiting and should be excluded prior to referral to a
specialist.
Weight Loss,
Involuntary
Involuntary weight
loss, unknown
etiology
Changed "Involuntary weight loss > 10 lbs (4.5 kg)
w/in 12 wks" to "Involuntary weight loss > 10 lbs (4.5
kg) or ≥ 5% within 12 weeks"
An unexpected weight loss of 5% or more (not only 10
pounds of weight loss) in 3 months is worrisome and
should be evaluated.
Weight Loss,
Involuntary
Involuntary weight
loss, unknown
etiology
Removed "HIV," "Negative," and "Not indicated"
under "Lab tests normal"
HIV testing should only be considered in a patient who
has risk factors, not in everyone with involuntary weight
loss.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 37
Subset Indication Revision Rationale
Weight Loss,
Involuntary
Involuntary weight
loss, unknown
etiology
Removed "UGI" under "Imaging studies
nondiagnostic for etiology of weight loss"
The decision on whether an UGI is necessary in the
work-up of involuntary weight loss is best left to the
specialist.
Weight Loss,
Involuntary
Involuntary weight
loss, unknown
etiology
Changed "Abdominal US/CT" to "Abdominal CT" CT is more informative than abdominal ultrasound in
patients with involuntary weight loss.
Category: Pulmonary Disorders
Subset Indication Revision Rationale
Asthma Asthma with
complication or
comorbidity
Changed "Pco2 ≥ 40 mmHg (5.3 kPa)" to "Pco2 ≥
45 mmHg (5.3 kPa)" under "Acute respiratory
compromise"
This value more accurately reflects respiratory distress.
Asthma Asthma with
complication or
comorbidity
Changed "Mechanical ventilation w/in 5 yrs by
Hx" to "ICU admission or mechanical ventilation by
history"
Referral is reasonable for a patient with asthma who
required mechanical ventilation or needed intensive
care at any time in the past.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 38
Subset Indication Revision Rationale
Asthma Asthma with
complication or
comorbidity
Added "High-risk Obstetrician" to the list of
specialists appropriate for referral for “Pregnancy”
The obstetrician should work with the pulmonologist to
determine if a change in management is necessary.
Asthma Continued asthma
after treatment
Changed "Nighttime awakenings ≥ 2 w/in 1 wk" to
"Nighttime awakenings"
Any awakening at night due to asthma indicates poor
control and referral is reasonable.
Chronic
Obstructive
Pulmonary
Disease (COPD)
Chronic obstructive
pulmonary disease
(COPD) with
complication or
comorbidity
Changed "Mechanical ventilation w/in 5 yrs by
Hx" to "ICU admission/mechanical ventilation by
history"
Referral is reasonable for a patient with chronic
obstructive pulmonary disease who required
mechanical ventilation or needed intensive care at
any time in the past.
Chronic
Obstructive
Pulmonary
Disease (COPD)
Chronic obstructive
pulmonary disease
(COPD) with
complication or
comorbidity
Added "High-risk Obstetrician" and removed
"Critical Care Specialist" from the list of specialists
appropriate for referral for "Pregnancy"
An obstetrician, not a critical care specialist, may
need to work with the pulmonologist to determine if a
change in management is necessary.
Chronic
Obstructive
Continued chronic
obstructive
Changed "Beta-agonist ≥ 8 wks" and
"Anticholinergic ≥ 8 wks" to "Beta-agonist ≥ 4
Referral may be appropriate when the patient with
chronic obstructive pulmonary disease continues to

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 39
Subset Indication Revision Rationale
Pulmonary
Disease (COPD)
pulmonary disease
(COPD) after
treatment
weeks" and "Anticholinergic ≥ 4 weeks," under
"Therapy"
have symptoms after at least 4, not 8, weeks of
treatment.
Chronic
Obstructive
Pulmonary
Disease (COPD)
Chronic
corticosteroid use
Removed "Inhaled corticosteroids ≥ 4 wks" The PCP can manage the patient with chronic
obstructive pulmonary disease who is on inhaled
corticosteroids.
Cough,
Unknown
Etiology
Changed indications "Daily cough > 3 weeks and
no smoking by history" and "Daily cough > 3
weeks and smoking by history" to "Subacute or
chronic cough (daily cough > 3 weeks) and no
smoking by history" and "Subacute or chronic
cough (daily cough > 3 weeks) and smoking by
history"
This change was made to clarify that referral is being
made for aid in the treatment and diagnosis of a
subacute or chronic cough. The primary care provider
can manage an acute cough without the need for
specialist involvement.
Cough,
Unknown
Etiology
Subacute or chronic
cough (daily cough
Added "Diagnosis" as a reason for specialty
involvement
A pulmonologist may be helpful in establishing the
diagnosis of a cough lasting more than 3 weeks when

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 40
Subset Indication Revision Rationale
> 3 weeks) and no
smoking by history
the primary care physician has not been able to
make a definitive diagnosis.
Cough,
Unknown
Etiology
Subacute or chronic
cough (daily cough
> 3 weeks) and no
smoking by history
Changed "Intranasal corticosteroid or cromolyn
spray" to "Intranasal corticosteroid"
Cromolyn is not as effective as intranasal
corticosteroids in the treatment of cough.
Cough,
Unknown
Etiology
Subacute or chronic
cough (daily cough
> 3 weeks) and no
smoking by history
Changed "Beta-agonist ≥ 2 wks" to "Beta-agonist
use ≥ 3 doses/week" when "Symptoms of asthma
present after treatment"
This dose of beta-agonists more accurately reflects
poor asthma control necessitating specialist
involvement.
Cough,
Unknown
Etiology
Subacute or chronic
cough (daily cough
> 3 weeks) and
smoking by history
Changed "Inhaled corticosteroid ≥ 2 wks" to
"Corticosteroids ≥ 4 weeks" when "Symptoms of
asthma present after treatment"
Referral is reasonable if at least 4, not 2, weeks of
corticosteroids, not only inhaled but oral as well, do
not control the patient's asthma.
Cough,
Unknown
Etiology
Subacute or chronic
cough (daily cough
Changed "Beta-agonist ≥ 2 wks" to "Beta-agonist
use ≥ 3 doses/week" when "Symptoms of asthma
present after treatment"
This dose of beta-agonists more accurately reflects
poor asthma control necessitating specialist
involvement.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 41
Subset Indication Revision Rationale
> 3 weeks) and
smoking by history
Hemoptysis Blood-streaked
sputum
Changed “Continued blood-streaked sputum
after Abx Rx ≥ 10 days” to “Continued blood-
streaked sputum after antibiotic treatment
completed” under “Findings” under “Nonsmoker
and”
Duration of antibiotic treatment may vary and referral
to the specialist is appropriate following completion of
the antibiotic course.
Imaging Study
Abnormalities
(Pulmonary
Disorders)
Changed indication “Thorax bone abnormality”
to “Thoracic bone abnormality by imaging”
An abnormality of a bone in the thoracic region may
be discovered by either CT or x-ray.
Imaging Study
Abnormalities
(Pulmonary
Disorders)
New nodule or mass Added “Spiculated margins” under “Suspicious
morphology” under “Lung” under “Findings”
Benign nodules typically have smooth margins,
whereas a nodule with spiculated margins is more
likely to be malignant.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 42
Subset Indication Revision Rationale
Imaging Study
Abnormalities
(Pulmonary
Disorders)
New nodule or mass Added “History of emphysema or pulmonary
fibrosis” and “Nodule located in upper lobe”
under “Lung” under “Findings”
History of emphysema or pulmonary fibrosis or a
nodule located in the upper lobe are all risk factors for
malignancy and referral to the specialist is
appropriate if these findings are present with a new
lung nodule on imaging.
Imaging Study
Abnormalities
(Pulmonary
Disorders)
New nodule or mass Added “Interventional Radiologist” to the list of
specialists appropriate for referral for “New
nodule or mass” for “Hilum” and “Mediastinum”
An interventional radiologist, in addition to a
pulmonologist or thoracic surgeon, may be
involved in the evaluation of patients with a
hilar or mediastinal nodule or mass.
Imaging Study
Abnormalities
(Pulmonary
Disorders)
Lymphadenopathy
by chest x-ray or CT
Added “Interventional Radiologist” to the list of
specialists appropriate for referral
An interventional radiologist, in addition to a
pulmonologist or thoracic surgeon, may be involved
in the evaluation of patients with hilar or mediastinal
lymphadenopathy.
Imaging Study
Abnormalities
Pneumothorax by x-
ray
Changed “Not resolved by CXR ≥ 2 wks” to “Not
resolved by x-ray ≥ 1 week” under “< 20%
pneumothorax”
If a small pneumothorax has not resolved within 1
week, referral to a specialist is appropriate as there is
risk for expansion to a larger pneumothorax.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 43
Subset Indication Revision Rationale
(Pulmonary
Disorders)
Imaging Study
Abnormalities
(Pulmonary
Disorders)
Vascular
abnormality
Removed “Aortic abnormality by CT/MRA/MRI” The user should refer to the indication “Aortic
abnormality” within the “Imaging Study Abnormalities
(Cardiovascular Disorders)” criteria subset.
Imaging Study
Abnormalities
(Pulmonary
Disorders)
Vascular
abnormality
Added “Interventional Radiologist” to the list of
specialists appropriate for referral for “Hilar vessel
abnormality by CT or MRI”
An interventional radiologist, in addition to a vascular
surgeon, cardiologist, or cardiothoracic surgeon, may
be involved in the evaluation of patients with a hilar
vessel abnormality.
Imaging Study
Abnormalities
(Pulmonary
Disorders)
Vascular
abnormality
Added “Pulmonary arteriovenous malformation
(AVM) by testing”
Referral to a specialist is appropriate to diagnose and
manage a pulmonary arteriovenous malformation
observed by testing.
Imaging Study
Abnormalities
Thoracic bone
abnormality
Added “Thoracic Surgeon” to the list of specialists
appropriate for referral
A thoracic surgeon, in addition to an orthopedic
surgeon, oncologist, or interventional radiologist, may

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 44
Subset Indication Revision Rationale
(Pulmonary
Disorders)
be involved in the evaluation of patients with a
thoracic bone abnormality.
Pleural Effusion Added indication “Pleural effusion by chest x-ray
or CT, unknown etiology”
Referral to a specialist is appropriate for a
thoracentesis to determine the type of pleural effusion
present on imaging.
Pleural Effusion Changed indication “Suspected hemothorax” to
“Hemothorax” and added “Suspected
hemothorax by chest x-ray or CT” and “Known
hemothorax by thoracentesis”
This change was made to more clearly indicate that
referral to a specialist is appropriate for either a
suspected or known hemothorax. Thoracentesis may
not be required for a hemothorax that is suspected
based on imaging findings and the patient's history,
and treatment of the hemothorax may be required
urgently.
Pleural Effusion Changed indication “Empyema” to “Known
empyema by thoracentesis”
This change was made to more clearly indicate that a
thoracentesis has been done and, therefore, referral
to the specialist is appropriate to manage the
empyema.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 45
Subset Indication Revision Rationale
Pleural Effusion Changed indication “Exudative effusion,
unknown etiology” to “Known exudative effusion
by thoracentesis”
This change was made to more clearly indicate that a
thoracentesis has been done and, therefore, referral
to the specialist is appropriate to manage the
exudative effusion.
Pleural Effusion Changed indication “Transudative effusion” to
“Known transudative effusion by thoracentesis”
This change was made to more clearly indicate that a
thoracentesis has been done and, therefore, referral
to the specialist is appropriate to manage the
transudative effusion.
Pleural Effusion Changed indication “Chylous effusion” to
“Known chylous effusion by thoracentesis”
This change was made to more clearly indicate that a
thoracentesis has been done and, therefore, referral
to the specialist is appropriate to manage the chylous
effusion.
Pleural Effusion Removed indication “Thoracentesis not yet
performed”
Thoracentesis is usually performed by the specialist,
not by the PCP.
Pleural Effusion Malignant effusion Changed “Newly discovered” to “Initial
malignant effusion by thoracentesis”
This change was made to more clearly indicate that a
thoracentesis has been done and, therefore, referral

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 46
Subset Indication Revision Rationale
to the specialist is appropriate to manage the initial
malignant effusion.
Pleural Effusion Malignant effusion Changed “Recurrent” to “Recurrent malignant
effusion by chest x-ray or CT”
In a patient with a previous malignant pleural effusion,
a recurring effusion on imaging is likely to be
malignant and referral to the specialist is appropriate
without a repeat thoracentesis.
Pleural Effusion Malignant effusion Added “Pulmonologist” and “Interventional
Radiologist” to the list of specialists appropriate
for referral for “Initial malignant effusion by
thoracentesis”
A pulmonologist and interventional radiologist, in
addition to a thoracic surgeon, radiation oncologist,
and oncologist, may be involved in the management
of patients with a malignant effusion.
Pleural Effusion Malignant effusion Changed “Surgeon” to “Thoracic Surgeon” in the
list of specialists appropriate for referral for “Initial
malignant effusion by thoracentesis”
Referral to a thoracic surgeon, rather than a surgeon,
is appropriate to manage a malignant pleural
effusion.
Pleural Effusion Malignant effusion Added “Periodic Assessment” as a reason
for specialty involvement for “Recurrent
malignant effusion by chest x-ray or CT”
Periodic assessment may be appropriate for
patients with recurrent malignant effusions as
these are likely to keep recurring.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 47
Subset Indication Revision Rationale
Pleural Effusion Malignant Effusion Added “Pulmonologist,” “Interventional
Radiologist,” “Radiation Oncologist,” and
“Oncologist” to the list of specialists appropriate
for referral for “Recurrent malignant effusion by
chest x-ray or CT”
A pulmonologist, interventional radiologist, radiation
oncologist, and oncologist, in addition to a thoracic
surgeon, may be involved in the evaluation of
patients with a recurrent malignant effusion.
Pleural Effusion Known empyema by
thoracentesis
Added “Pulmonologist” to the list of specialists
appropriate for referral
A pulmonologist, in addition to a thoracic surgeon,
interventional radiologist, and infectious disease
specialist, may be involved in the management of
patients with an empyema.
Pleural Effusion Known exudative
effusion by
thoracentesis
Removed “Sputum cytology negative,” “CXR
nondiagnostic for etiology of effusion,” “Chest CT
nondiagnostic for etiology of effusion,” and
“Thoracentesis performed and pleural fluid tests
available”
Referral to the specialist is appropriate to determine
the etiology of a known exudative effusion and
ordering the appropriate testing is best left to the
specialist.
Pleural Effusion Known exudative
effusion by
thoracentesis
Removed “Diagnosis” and added “Limited
Management” as a reason for specialty
involvement
Referral is for management, not diagnosis, of an
exudative effusion.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 48
Subset Indication Revision Rationale
Pleural Effusion Known exudative
effusion by
thoracentesis
Removed “Thoracic Surgeon” from the list of
specialists appropriate for referral
A pulmonologist, not thoracic surgeon, would be
appropriate for the management of an exudative
effusion.
Pleural Effusion Known transudative
effusion by
thoracentesis
Changed “Not on peritoneal dialysis” to “Not on
dialysis”
Patients on hemodialysis, as well as peritoneal dialysis,
are at risk for development of a transudative effusion.
Pleural Effusion Known transudative
effusion by
thoracentesis
Removed “Thoracentesis performed and pleural
fluid cytology negative”
Referral to the specialist may be appropriate to
determine the etiology of a transudative effusion
diagnosed by thoracentesis and ordering the
appropriate testing is best left to the specialist.
Pleural Effusion Known transudative
effusion by
thoracentesis
Removed “Diagnosis” and added “Limited
Management” as a reason for specialty
involvement
Referral is for management, not diagnosis, of a known
transudative effusion.
Pleural Effusion Known chylous
effusion by
thoracentesis
Added “Pulmonologist” and “Interventional
Radiologist” to the list of specialists appropriate
for referral
A pulmonologist and interventional radiologist, in
addition to a thoracic surgeon, may be involved in
the management of patients with a chylous effusion.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 49
Subset Indication Revision Rationale
Pneumonia Pneumonia with
complication or
comorbidity
Changed "Systolic BP < 100 mmHg" to "Systolic BP
< 90 mmHg or < 110 mmHg with chronic
hypertension" and added "HR > 120/min,
sustained," "Orthostatic changes," "Sustained
decrease in systolic BP ≥ 20 mmHg within 3
minutes of sitting or standing," and "Sustained
decrease in diastolic BP ≥10 mmHg within 3
minutes of sitting or standing" under
"Hemodynamic instability"
These criteria more accurately reflect the findings
seen in individuals with hemodynamic instability.
Pneumonia Pneumonia with
complication or
comorbidity
Changed "COPD with FEV1 < 1.5 L" to "Asthma or
chronic obstructive pulmonary disease with FEV1
< 1.5 L" and added "Sleep apnea" under
"Comorbidity" and "Pulmonary disease"
Patients with asthma or sleep apnea are at risk of
developing complications from pneumonia.
Pneumonia Pneumonia with
complication or
comorbidity
Added "Chronic liver or kidney disease" and
"Diabetes mellitus" under "Comorbidity"
Patients with these conditions are at risk of developing
complications from pneumonia.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 50
Subset Indication Revision Rationale
Pneumonia Pneumonia with
complication or
comorbidity
Added "Multi-drug resistant organism" under
"Unusual infection" and "Organism"
Specialist input may be helpful when the patient has
pneumonia secondary to infection with a multi-drug
resistant organism.
Pneumonia Pneumonia with
complication or
comorbidity
Removed "Osteomyelitis" under "Pneumonia with
infectious complication" and removed
“Orthopedic Surgeon” from Purpose of Specialist
Involvement note
Osteomyelitis would be a very rare complication of
pneumonia.
Pneumonia Pneumonia with
complication or
comorbidity
Added "Pleural effusion" under "Pneumonia with
infectious complication"
Evidence shows worse outcomes in patients who
present with both pleural effusion and pneumonia.
Pneumonia Pneumonia,
nonresponsive to
treatment
Changed "Temperature ≥ 100.4 F (38 C)" to
"Temperature ≥ 100.4 F (38 C) increasing" under
"Findings"
Referral would only be necessary if the patient with
pneumonia had worsening of their fever, not just a
persistent fever.
Pneumonia Pneumonia,
unresolved
Changed "Antibiotics (intravenous/oral) ≥ 10
days" to "Antibiotics (intravenous/oral) ≥ 7 days"
One week, not 10 days, of antibiotics should be
sufficient to see improvement.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 51
Subset Indication Revision Rationale
Pneumonia Pneumonia,
unresolved
Changed "Dyspnea increasing by history or
physical examination" to "Dyspnea by history or
physical examination" under "Findings"
Any dyspnea, not just dyspnea that is worsening,
could be evaluated by a specialist.
Pneumonia Pneumonia,
unresolved
Changed "PO2 or O2 sat decreasing" to "PO2 or
O2 sat decreased"
Referral is appropriate when the patient treated for
pneumonia has decreased oxygenation, not
necessarily oxygenation that is getting worse.
Preoperative
Evaluation
(Pulmonary
Disorders)
Abnormal
pulmonary function
Changed "DLCO ≥ 60% predicted" to "Abnormal
DLCO" and “≥ 60% predicted” OR "Dyspnea by
history"
Referral is appropriate for any DLCO abnormality, not
only when 60% or less, if the patient has shortness of
breath.
Preoperative
Evaluation
(Pulmonary
Disorders)
Abnormal
pulmonary function
Added "FEV1/FVC ratio < 0.7" This value represents airway restriction and evaluation
by a pulmonologist is justified.
Preoperative
Evaluation
High−risk surgery Removed "Age ≥ 60" under "Risk factors" Age alone is not a risk factor for postoperative
pulmonary complications.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 52
Subset Indication Revision Rationale
(Pulmonary
Disorders)
Preoperative
Evaluation
(Pulmonary
Disorders)
High−risk surgery Added "Anticipated surgical duration ≥ 3 hours"
under "Risk factors"
There is a greater risk of pulmonary complications the
longer the duration of upper abdominal or thoracic
surgery.
Pulmonary
Embolism (PE)
Suspected
pulmonary embolism
(PE)
Added “Urgent” designation A suspected pulmonary embolism requires immediate
attention and preauthorization may not be able to be
done prior to referral to the specialist.
Pulmonary
Embolism (PE)
Suspected
pulmonary embolism
(PE)
Added “Interventional Radiologist” to the list of
specialists appropriate for referral
An interventional radiologist, in addition to a
pulmonologist or cardiologist, may be involved in the
evaluation of patients with suspected pulmonary
embolism.
Pulmonary
Embolism (PE)
Suspected
pulmonary embolism
(PE)
Added “Tachycardia,” “Hypotension,” and “New
cough” under “Symptoms or findings”
People with pulmonary embolism commonly present
with these symptoms or findings.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 53
Subset Indication Revision Rationale
Pulmonary
Embolism (PE)
Suspected
pulmonary embolism
(PE)
Removed “Suspected DVT by exam and LE
duplex US nondiagnostic for DVT” and “Known
DVT by imaging and”
When pulmonary embolism is suspected in a patient
with tachycardia or new cough, referral to a specialist
is appropriate independent of suspicion or presence
of a deep vein thrombosis.
Pulmonary
Embolism (PE)
Suspected
pulmonary embolism
(PE)
Changed “CTA nondiagnostic for PE” to “CTA or
MRA or V/Q scan nondiagnostic for pulmonary
embolism (PE)”
Referral to a specialist is appropriate for a patient with
a suspected pulmonary embolism and a
nondiagnostic MRA or V/Q scan, not just CTA.
Pulmonary
Embolism (PE)
Pulmonary embolism
(PE) by imaging
Added “Urgent” designation A known pulmonary embolism requires immediate
attention and preauthorization may not be able to be
done prior to referral to the specialist.
Pulmonary
Embolism (PE)
Pulmonary embolism
(PE) by imaging
Added “Interventional Radiologist” to the list of
specialists appropriate for referral
An interventional radiologist, in addition to a critical
care specialist, pulmonologist, or thoracic surgeon,
may be involved in the evaluation of patients with
pulmonary embolism by imaging.
Pulmonary
Embolism (PE)
Pulmonary embolism
(PE) by imaging
Removed “Vascular Surgeon” from the list of
specialists appropriate for referral
An interventional radiologist, critical care specialist,
pulmonologist, or thoracic surgeon would be

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 54
Subset Indication Revision Rationale
consulted regarding pulmonary embolism, not a
vascular surgeon.
Pulmonary
Function Test
(PFT)
Abnormalities
Abnormal
pulmonary function
tests
Added "Peak expiratory flow ≥ 60% predicted"
and "FEV1/FVC ratio < 0.7"
These values represent airway restriction and
evaluation by a pulmonologist is justified.
Tuberculosis (TB) TST ≥ 5 mm and high
risk for tuberculosis
Added "Silicosis” Silicosis puts a patient at high risk for developing
tuberculosis.
Tuberculosis (TB) TST ≥ 10 mm and < 15
mm and low to
intermediate risk for
tuberculosis
Removed "Silicosis" under "Medical conditions
which increase the risk of tuberculosis"
Silicosis puts a patient at high, not low or intermediate,
risk for developing tuberculosis and this condition is
now covered under "TST ≥ 5 mm and high risk for
tuberculosis."
Tuberculosis (TB) IGRA positive or
indeterminate or
borderline
Added indication "IGRA positive or indeterminate
or borderline"
The interferon gamma release assay (IGRA) test may
be done for tuberculosis screening instead of a
tuberculin skin test (TST).

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 55
Subset Indication Revision Rationale
Tuberculosis (TB) Suspected
tuberculosis
Added "Cavitary air space disease" under "By
imaging"
This is an imaging finding associated with active
tuberculosis.
Tuberculosis (TB) Suspected
tuberculosis
Changed "PPD" "Reactive" to "TST reactive" under
"Screening test"
This change was made to reflect current medical
terminology.
Tuberculosis (TB) Suspected
tuberculosis
Changed "PPD nonreactive in high-risk group" to
"TST nonreactive or IGRA negative in high-risk
group"
This change was made to reflect current medical
terminology. IGRA was added, as it is an option to
tuberculin skin testing.
Tuberculosis (TB) Suspected
tuberculosis
Added "IGRA positive or indeterminate or
borderline" under "Screening test"
IGRA was added, as it is an option to tuberculin skin
testing.
Tuberculosis (TB) Suspected
tuberculosis
Added "Chest x-ray results available" CXR should always be done in the evaluation of
suspected tuberculosis.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 56
Category: Renal & Urologic Disorders
Subset Indication Revision Rationale
Hematuria Gross hematuria Removed "CT nondiagnostic for etiology of
hematuria"
CT is not necessary prior to referral for gross
hematuria.
Hematuria Microscopic
hematuria
Removed "Prostatitis," "Excluded by Hx & PE,"
and "Not indicated"
Evaluation for prostatitis is not routinely done prior
to referral to a specialist for hematuria.
Nephrolithiasis
(Kidney/Ureteral/Bladder
Stones)
Nephrolithiasis
without
obstruction
Changed "Aggressive Hydration 24 hrs" to
"Hydration 24 hours" under "Continued
symptoms after treatment"
Hydration for 24 hours or longer is appropriate but
the nature of that hydration would be
determined on a case by case basis.
Nephrolithiasis
(Kidney/Ureteral/Bladder
Stones)
Recurrent
nephrolithiasis
Changed "Medications deemed
noncontributory" to "Medications necessary
or deemed noncontributory"
Medications may continue to be necessary
regardless of their contribution to the condition.
Proteinuria Non−nephrotic
proteinuria of
unknown etiology
Removed "Urine protein electrophoresis"
under "Test results available"
Urine protein electrophoresis is not routinely
tested prior to specialty referral.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 57
Subset Indication Revision Rationale
Proteinuria Non−nephrotic
proteinuria of
known etiology,
worsening after
treatment
Removed "BP controlled" under "Worsening
proteinuria after treatment" under "Therapy"
Blood pressure does not need to be controlled
prior to referral to a specialist.
Proteinuria Nephrotic−range
proteinuria
Removed "Urine protein electrophoresis"
under "Test results available"
Urine protein electrophoresis is not necessary
prior to referral to a specialist.
Renal Insufficiency Acute renal failure
without
obstruction
Changed "Creatinine increase 0.5 mg/dL
(44 µmol/L) over 24 hours" to Creatinine
increase 0.3 mg/dL (26.5 µmol/L) over 48
hours" under "Acute creatinine elevation"
A creatinine elevation of 0.3 mg/dL over
48 hours is considered an acute elevation and
demonstrates acute renal failure appropriate for
specialty referral.
Renal Insufficiency Acute renal failure
without
obstruction
Added "Creatinine 1.5 fold from baseline
within 7 days" under "Acute creatinine
elevation"
Creatinine 1.5 fold from baseline within 7 days is
an indicator of acute renal failure and justifies
further evaluation.

2018 Clinical Revisions
Copyright 2018 Change Healthcare LLC and/or one of its subsidiaries. Produced in Cork, Ireland 58
Subset Indication Revision Rationale
Renal Insufficiency Acute renal failure
with obstruction
Changed "Creatinine increase 0.5 mg/dL
(44 µmol/L) over 24 hours" to Creatinine
increase 0.3 mg/dL (26.5 µmol/L) over 48
hours" under "Acute creatinine elevation"
A creatinine elevation of 0.3 mg/dL over 48 hours
is considered an acute elevation that justifies
further evaluation.
Renal Insufficiency Acute renal failure
with obstruction
Added "Creatinine 1.5 fold from baseline
within 7 days" under "Acute creatinine
elevation"
Creatinine 1.5 fold from baseline within 7 days is
an indicator of acute renal failure.
Renal Insufficiency Chronic renal
insufficiency
Added "GFR below normal" Referral to a specialist is appropriate for patients
with a below normal glomerular filtration rate.