3. sudden death realted to coronary
DESCRIPTION
gdhgggghghghjhbTRANSCRIPT

The American Journal of Forensic Medicine and Pathology 22(3):225–227, 2001. ©2001 Lippincott Williams & Wilkins, Inc., Philadelphia
225
Two cases of sudden death of young people in apparentlygood health are reported. The only pathologic changefound was a fibromuscular dysplasia of the artery supply-ing the conduction system of the heart with an importantnarrowing of the lumen and strong thickening of the arte-rial wall. The first case was of a 12-year-old girl who diedsuddenly while skiing; the second was of a 32-year-oldman who died while talking to his wife. No other patho-logic changes were found at autopsy, and the results oftoxicologic analysis were negative. There was no individ-ual or family history of cardiac diseases. These cases il-lustrate the importance of an analysis of the conductionsystem, including examination of the intramural coronaryarteries supplying the conduction system.Key Words: Sudden death—Fibromuscular dysplasia—Conduction system—Coronary artery.
Fibromuscular dysplasia was first described by Lead-better and Burkland in 1938 as a disease of renal arteries,after it was also observed in cervical and other arteries. Itis a nonatheromatous, noninflammatory disease of the ar-teries with segmental stenosis (1). According to James(2), the focal fibromuscular dysplasia of small coronaryarteries rarely extends more than a few millimeters alongthe course of an artery. The typical lesion is often entirelywithin the tunica media, including both fibrous and mus-cular components, and the histologic organization is sodisorderly that it is considered a dysplastic process. Auniform histologic classification of fibromuscular dyspla-sia of coronary arteries does not exist (1).
The physiologic consequence of focal fibromusculardysplasia with the synergistic combination of local spasmhas been discussed by James and Bruschke (3), who re-ported that for a small coronary artery with 50% narrow-ing of the radius of the lumen, only a 9% decrease of theexternal radius by spasm is sufficient to obliterate thelumen completely. An obstruction of the arteries supply-ing the conduction system may have caused the electricalinstability of the heart with arrhythmia and sudden death.
Thickening of the small intramural coronary arterieshas been reported in some cases of sudden death (4), butthere are very few reports of death in young persons re-lated to focal fibromuscular dysplasia of coronary arter-ies supplying the conduction system (1,5,6).
CASE REPORTS
Case 1An apparently healthy 12-year-old girl died suddenly
while skiing. No family history of cardiac disease was re-ported. The decedent was 1.40 m tall and weighed 32 kg.The heart was mildly enlarged and weighed 150 g. Aslight hypertrophy of the left ventricle was noticed. Wealso observed signs of mitral valve prolapse: the posteriorleaflet of the mitral valve was slightly dome-shaped andshortened, and the left atrium was mildly enlarged, withthe endocardium diffusely thickened and whitened.
The conduction system was studied as follows: first,five blocks containing the atrioventricular node, the bun-
Sudden Death Related to Small Coronary Artery Disease
K. Michaud, M.D., N. Romain, M.D., C. Brandt-Casadevall, M.D., and P. Mangin, Ph.D.
Manuscript received November 30, 2000; accepted January5, 2001.
From the Institut Universitaire de Médecine Légale, Lau-sanne, Switzerland.
Address correspondence and reprint requests to K. Michaud,Institut Universitaire de Médecine Légale, Bugnon 21, 1005Lausanne, Switzerland.
Am J Forensic Med Pathol, Vol. 22, No. 3, September 2001
dle of His, and the proximal part of the right and left bun-dle branches were obtained and then cut along planesperpendicular to the anulus of the valve from anterior toposterior, and at least two sections were prepared fromeach block. The sections were stained with hematoxylinand eosin, and some were stained with Masson trichromeand elastic van Gieson.
Microscopy revealed focal fibromuscular dysplasia ofthe atrioventricular artery with focal very narrowedlumen (Figs. 1 and 2), destruction of the internal elasticlamina (Fig. 3), and focal fibrosis of the summit of theventricular septum, suggesting previous ischemia. Therewere also some contraction bands of the working myo-cardium. The arterial walls of other organs were normal.The results of toxicologic analysis (immunoassays andgas chromatography/mass spectrometry drug screening)were negative.
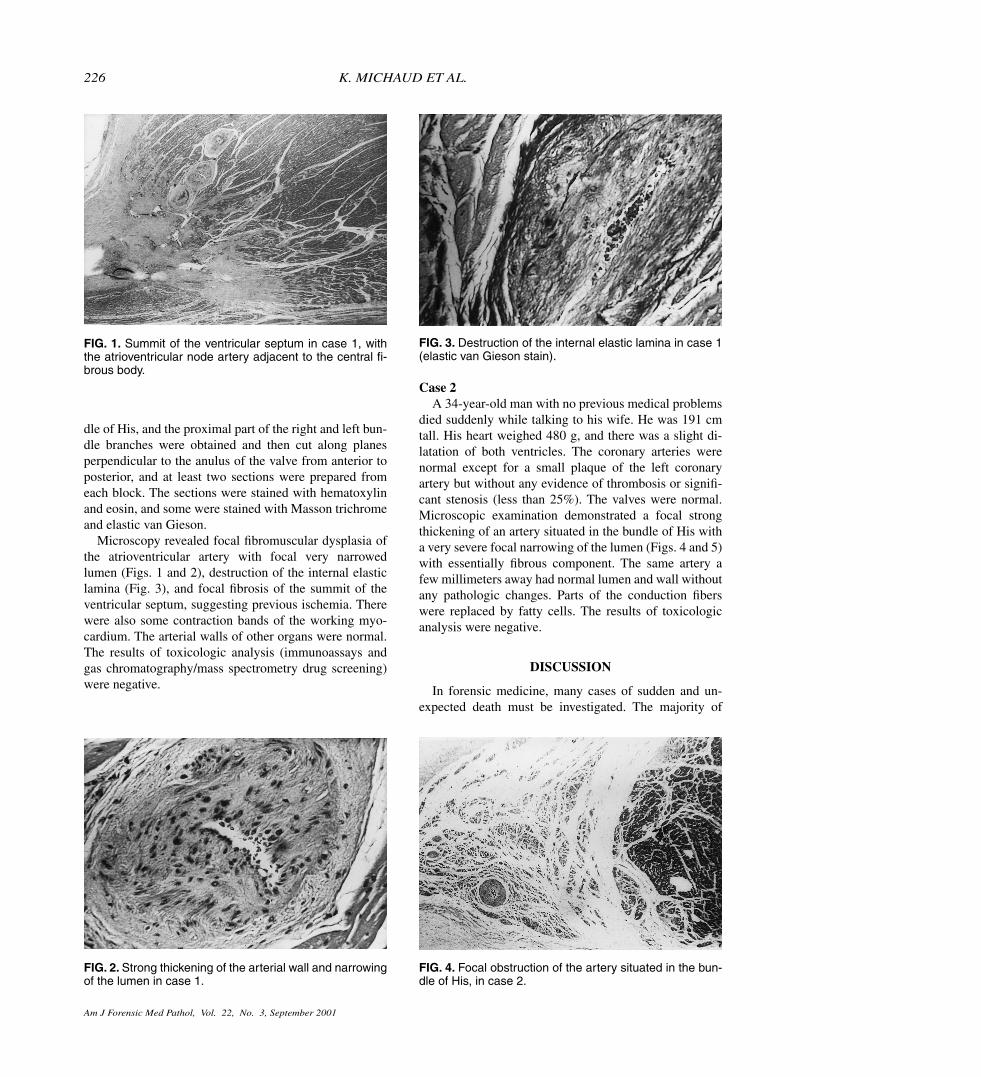
Case 2A 34-year-old man with no previous medical problems
died suddenly while talking to his wife. He was 191 cmtall. His heart weighed 480 g, and there was a slight di-latation of both ventricles. The coronary arteries werenormal except for a small plaque of the left coronaryartery but without any evidence of thrombosis or signifi-cant stenosis (less than 25%). The valves were normal.Microscopic examination demonstrated a focal strongthickening of an artery situated in the bundle of His witha very severe focal narrowing of the lumen (Figs. 4 and 5)with essentially fibrous component. The same artery afew millimeters away had normal lumen and wall withoutany pathologic changes. Parts of the conduction fiberswere replaced by fatty cells. The results of toxicologicanalysis were negative.
DISCUSSION
In forensic medicine, many cases of sudden and un-expected death must be investigated. The majority of
226 K. MICHAUD ET AL.
FIG. 3. Destruction of the internal elastic lamina in case 1(elastic van Gieson stain).
FIG. 2. Strong thickening of the arterial wall and narrowingof the lumen in case 1.
FIG. 1. Summit of the ventricular septum in case 1, withthe atrioventricular node artery adjacent to the central fi-brous body.
FIG. 4. Focal obstruction of the artery situated in the bun-dle of His, in case 2.

Am J Forensic Med Pathol, Vol. 22, No. 3, September 2001
cases of witnessed collapse or of an individual foundunder apparently natural circumstances can be resolvedafter autopsy when a natural cause appears, for exam-ple, internal hemorrhage. Some cases of sudden death,usually those occurring during stress or physical activ-ity, can be compatible with sudden cardiac death. Someof them can be explained by obvious cardiac pathologicchanges found at autopsy, such as atherosclerotic coro-nary disease, valve disease, or myocardial disease, orafter histologic examination. However, even after acomplete autopsy with toxicologic analysis, somedeaths remain unexplained. Moreover, it is well knownthat disturbances of cardiac rhythm are a commonpathophysiologic mechanism responsible for suddendeath. In some cases, such as in long QT and Brugadasyndromes, these disturbances are only functional anddo not involve morphologic changes. In others, a con-genital or acquired lesion affecting the conduction sys-tem of the heart can be found, which can explain theclinical signs.
The common features in our two cases were suddenunexpected death, a morphologically normal heart show-ing only a strong focal narrowing of the artery supplyingthe conduction system, no other pathologic lesions, andnegative results of toxicologic analysis.
Although another origin of death cannot be excluded,as for example rhythm disturbances of physiologic ori-gin, it is important to notice that gene defects in ion chan-nels, as in long QT syndrome or Brugada syndrome, arefrequently related to electrocardiographic abnormalitiesrevealed earlier in the subject’s life or in family members.In the cases discussed here, there was no individual orfamily history of cardiac disease.
Moreover, the mitral valve prolapse observed in thefirst case may not have been the only cause of the death,the more so because mitral valve prolapse (floppy mitralvalve) with a minor degree of prolapse is very common inthe normal population, as is shown by echocardiographicsurveys of young subjects (7). However, Burke et al. (8)reported that arterial dysplasia in mitral valve prolapsemay contribute to sudden cardiac death mediated by ven-tricular fibrosis.
Burke et al. (9) compared the atrioventricular nodeartery in 27 patients who died of unexplained suddendeath with 17 normal control subjects and demonstrateda quantitative difference between the degree of atrioven-tricular node artery narrowing in both groups. Moreover,the authors observed that sudden death was often associ-ated with exercise and a family history of unexplainedsudden death.
Therefore, considering the physiologic consequencesof a local spasm in a small coronary artery with a nar-rowed lumen, it can be concluded that in our cases a focalnarrowing of the arteries supplying the conduction sys-tem of the heart might have led to lethal arrhythmia.
In addition, these two cases illustrate the importance ofan analysis of the conduction system, including an exam-ination of the intramural coronary arteries supplying theconduction system, particularly in cases of sudden andunexpected deaths of young people who die without anyobvious case of death.
REFERENCES1. Zack F, Terpe H, Hammer U, et al. Fibromuscular dysplasia
of coronary arteries as a rare cause of death. Int J Leg Med1996;108:215–8.
2. James TN. Morphologic characteristics and functional sig-nificance of focal fibromuscular dysplasia of small coro-nary arteries. Am J Cardiol 1990;65:12G–22G.
3. James TN, Bruschke AVG. The spectrum of diseases ofsmall coronary arteries and their physiologic consequences.J Am Coll Cardiol 1990;15:63–74.
4. Burke AP, Virmani R. Intramural coronary artery dysplasiaof the ventricular septum and sudden death. Hum Pathol1998;29:1124–7.
5. Anderson R, Bowie J, Dempster AG, et al. Sudden deathfrom occlusive disease of the atrioventricular node artery.Pathology 1981;13:417–21.
6. Jing HL, Hu BJ. Sudden death caused by stricture of thesinus node artery. Am J Forensic Med Pathol 1997;18:360–2.
7. Davies MJ. The investigation of sudden cardiac death.Histopathology 1999;34:93–8.
8. Burke AP, Farb A, Tang A, et al. Fibromuscular dysplasia ofsmall coronary arteries and fibrosis in the basilar ventricu-lar septum in mitral valve prolapse. Am Heart J 1997;134:282–91.
9. Burke AP, Subramanian R, Smialek J, et al. Nonatheroscle-rotic narrowing of the atrioventricular node artery and sud-den death. J Am Coll Cardiol 1993;21:117–22.
SUDDEN DEATH RELATED TO SMALL CORONARY ARTERY DISEASE 227
FIG. 5. Strong thickening of the arterial wall and narrowingof the lumen in case 2.