9780387220895-c1
TRANSCRIPT

Chapter 13Placental Shape Aberrations
General Considerations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 208Multilobed Placentas . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 208
Bilobed Placenta . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 208Succenturiate Lobes (Accessory Lobes, Placenta Succenturiata) . . . . 210
Circumvallate and Circummarginate Placentas . . . . . . . . . . . . . . . . . . . 211Extramembranous Pregnancy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 215Placenta Membranacea (Placenta Diffusa) . . . . . . . . . . . . . . . . . . . . . . . 218Miscellaneous Shape Abnormalities . . . . . . . . . . . . . . . . . . . . . . . . . . . . 219Placenta Previa . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 219Selected References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 221
General Considerations
Round or oval placentas are the predominant human placental form,but many other shapes exist (Figure 13.1). When the placenta is irreg-ular, its shape is presumably determined by location, atrophy, andperhaps the manner of original implantation. Anomalies may developfrom abnormal fetal genes expressed by the placenta, an abnormalmaternal environment, or an abnormal fetal–maternal interaction.Interestingly, for each aberrant placental shape in humans, there is acounterpart in animals. Thus, the placenta membranacea is similar tothe normally diffuse placenta in equines; the zonary placenta is typicalof carnivores, and so on.
Multilobed Placentas
Bilobed Placenta
Pathologic FeaturesOne of the most striking abnormalities is the bilobed placenta (pla-centa bilobata), in which two roughly equal sized lobes are separated by asegment of membranes (Figures 13.1, 13.2). It is present in 2% to 8% ofplacentas. The umbilical cord may insert in either of the lobes or in avelamentous fashion (see Chapter 15), in between the lobes, the latter

being the most common arrangement. Even if the cord insertion is notvelamentous, there are always membranous vessels connecting the twolobes. If one lobe is much smaller than the other, then the placenta issaid to have a succenturiate or accessory lobe (see below).
PathogenesisMultilobed placentas are thought to arise due to implantation in areasof decreased uterine perfusion. An example is lateral implantation inbetween the anterior and posterior walls of the uterus with one lobeon the anterior and one on the posterior wall. Other local factorsleading to multilobation are implantation over leiomyomas, in areas of
Multilobed Placentas 209
Figure 13.1. Diagram depicting placental shape abnormalities including multilobation (bilobed placenta and succenturiate placenta), placenta fenestrata, placenta membranacea, and ring or zonaryplacenta.

previous surgery, in the cornu, or over the cervical os. After implantation,there is preferential growth in areas of superior perfusion and atrophyin areas of poor perfusion. This is called trophotropism. Indeed, inter-mediate forms exist in which there are two lobes, with partial or complete infarction of residual villous tissue between the lobes. Thisfinding suggests that normal discoidal placentation was originallypresent but local factors led to atrophy or infarction, resulting in multilobation.
Clinical Features and ImplicationsThe membranous vessels connecting the two lobes occasionally throm-bose, rupture, become compressed, or present clinically as vasa previa withbleeding. Vasa previa occurs when the membranous vessels present“previous” to the delivering part of the baby (see Chapter 15). Bothbilobed placentas and succenturiate lobes are associated with multi-parity, antenatal bleeding, placenta previa, and retained placental tissue.
Succenturiate Lobes (Accessory Lobes, Placenta Succenturiata)
Succenturiate lobes have an incidence of approximately 5% to 6%.They may be single or multiple and differ from bilobed placentas onlyin the size and number of accessory lobes (Figures 13.1, 13.3). Approx-imately half are associated with infarction or atrophy of the succenturiate lobes,much higher than the overall incidence of infarction, which is esti-
210 Chapter 13 Placental Shape Aberrations
Figure 13.2. Bilobed placenta. Membranous vessels course from the velamentous cord insertion inbetween the two lobes.

mated to be 13%. As with bilobed placentas, membranous vessels arealways present connecting each lobe and thus may be susceptible todamage. The umbilical cord most commonly inserts into the dominantlobe.
Circumvallate and Circummarginate Placentas 211
Suggestions for Examination and Report: Bilobed Placenta andPlacenta with Succenturiate Lobes
Gross Examination: Each lobe should be measured and weighedindividually. The integrity of the membranous vessels connectingthe lobes should be evaluated, and it is recommended that sec-tions be taken of the vessels if they are ruptured, show grossthrombosis, or there is hemorrhage into the adjacent membranes.The vessels may be included in a separate membrane roll.
Comment: If membranous vessels are present and associatedwith thrombosis, rupture, or hemorrhage into the membranes, thepossibility of fetal hemorrhage should be considered.
Figure 13.3. Succenturiate lobes in an immature placenta, with infarction ofsome of the lobes.
Circumvallate and Circummarginate Placentas
Pathologic FeaturesIn circumvallate placentas, the membranes of the chorion laeve do notinsert at the edge of the placenta but rather at some inward distancefrom the margin, toward the umbilical cord (Figure 13.4). At themargin, one usually finds variable amounts of fibrin, recent clot, and

old blood. In complete circumvallates, there is a complete circumfer-ential ring that restricts the total surface of the chorion frondosum(Figures 13.5, 13.6). At the periphery, “naked” placental tissue pro-trudes. The fibrin that is present at the insertion of the membranescauses plication of the membranes, which is characteristic of circum-vallates (Figure 13.7). The amnion may follow the chorion into this plica, or most commonly, it flatly covers the plica without infolding. When no plication of the membranes occurs, it is called a
212 Chapter 13 Placental Shape Aberrations
Figure 13.4. Diagram of circummarginate and circumvallate membrane inser-tion. In both, the fetal membranes do not insert at the edge of the placenta butrather at some point inwards. In circumvallation there is a plication of themembranes evident as a fibrin ridge on gross examination. In circummargina-tion, the membrane insertion is flat and a ridge is not present.
Figure 13.5. Typical circumvallate placenta with prominent ridge of fibrin atthe periphery.

Circumvallate and Circummarginate Placentas 213
Figure 13.6. Plica of circumvallate margin with a wire holding up the over-hanging margin of the membrane insertion.
Figure 13.7. Margin of circumvallate placenta. The gray homogeneous mate-rial under the plica represents fibrin and degenerated blood.

circummarginate placenta (Figures 13.4, 13.8). These two forms blendinto each other, and partial forms are common.
Gross examination of the placenta shows yellow-brown marginal fibrinperipheral to the fibrin present at the membrane insertion. In caseswhere there is midtrimester hemorrhage and premature delivery, theremay be substantial blood at the margin. Hemorrhage may underminethe margin of the placenta, thus imitating abruptio placentae. Onmicroscopic examination, sections taken from the margin of the placenta will show absence of membranous covering peripherally with hemosiderin deposition and fibrin (Figure 13.7).
Clinical Features and ImplicationsThe incidence of circumvallation is from 1.0% to 6.5%, and the inci-dence of circummargination is up to 25% of placentas. They are rarelyfound in the first trimester. The most common complications of cir-cumvallation are antenatal bleeding and premature delivery. Additional,uncommon associations include premature membrane rupture, perinataldeath, congenital anomalies, single umbilical artery, and intrauterine growthrestriction. Cases with extensive hemorrhage and marginal hematomasmay lead to significant clinical bleeding. Large hematomas may elevatethe chorion laeve from its insertion site and cause disruption of the fetalvessels. Thus, the vaginal bleeding in these cases is frequently amixture of maternal and fetal blood. Significant neonatal anemia mayresult. It has been suggested that circummargination has little clinicalimpact while circumvallation has some important clinical associations.However, we prefer to view these two entities as aspects of the sameprocess.
214 Chapter 13 Placental Shape Aberrations
Figure 13.8. Sickle-shaped circummarginate placenta.

PathogenesisSeveral opposing theories have been presented as to the origin of cir-cumvallation. One theory is that circumvallation occurs due to mar-ginal hemorrhage, which undermines the membranes and pushes themover the chorionic plate. Another theory is that circumvallates developbecause the embryo implants too superficially and grows outward ina “polypoid” fashion or that it implants too deep. It is possible thatthere may be different types and origins of circumvallation, and thisissue is yet to be resolved.
Extramembranous Pregnancy
PathogenesisIn extramembranous or extrachorial pregnancy, there is early ruptureof both the amnion and chorion, leading to escape of the fetus into the uterinecavity (Figure 13.9). Evidence that the fetus must have escaped out of
Extramembranous Pregnancy 215
Figure 13.9. Extramembranous pregnancy with fetus. Note the size of fetusand the membrane opening. The placenta shows marked circumvallation.

the membranes much earlier is manifested by the diminutive holethrough the membranes, which may barely admit the umbilical cord,let alone the fetus (Figure 13.9). It is a rare condition, and as with otherconditions associated with early membrane rupture, such as amnionicbands (see Chapter 14), the etiology remains obscure.
Pathologic FeaturesThe placenta shows marked circumvallation (Figure 13.10), the cord maybe short, and the fetal surface shows lack of membranous covering, beingcovered instead with fibrin and a brownish discoloration consistentwith hemosiderin (Figure 13.11). The remaining membranes are rela-tively normal. Microscopically, one finds substantial quantities of post-hemorrhagic hemosiderin in the membranes. There also may be sparseamnion nodosum (see Chapter 14) over the placental tissue, but this isusually not striking.
Clinical Features and ImplicationsBecause of membrane rupture and loss of amniotic fluid, extramem-branous pregnancies are usually associated with prolonged amniorrheaas a result of periodic fetal urination. In addition, there are severe positional deformities of the fetus and pulmonary hypoplasia due to the oligohydramnios. Ascending infection is occasionally associated withextramembranous pregnancy, but this is not a constant finding. Themajority of these pregnancies abort or terminate prematurely, and suchfetuses only occasionally survive.
216 Chapter 13 Placental Shape Aberrations
Figure 13.10. Extramembranous pregnancy with circumvallation and diminu-tive opening.

Extramembranous Pregnancy 217
Suggestions for Examination and Report: Circumvallate Placenta, Circummarginate Placentas, and Extramembranous Pregnancy
Gross Examination: Extent of the circumvallation should benoted as well as a lack of amnion over the fetal surface and thepresence of hemosiderin (brown discoloration) and fibrin. Itshould also be noted whether there is plication or the membranes(circumvallate) or not (circummarginate). The presence of exten-sive marginal hemorrhage (marginal hematoma) and disruptionof fetal vessels should also be noted.
Comment: A comment is not necessary except when disruptedfetal vessels are present. In this case, the possible role of circum-vallation in the etiology may be suggested. If extreme circum-vallation and an extramembranous pregnancy are present, acomment may be made on the association with a history ofchronic leakage of amniotic fluid prior to delivery, oligohydram-nios, fetal positional deformities, and pulmonary hypoplasia.
Figure 13.11. Membrane insertion in the extramembranous pregnancy shownin Figure 13.9. Below is the villous tissue, membranes folded at top right, andthe fetus lay in space F. A = amnion nodosum.
Placenta Membranacea (Placenta Diffusa)
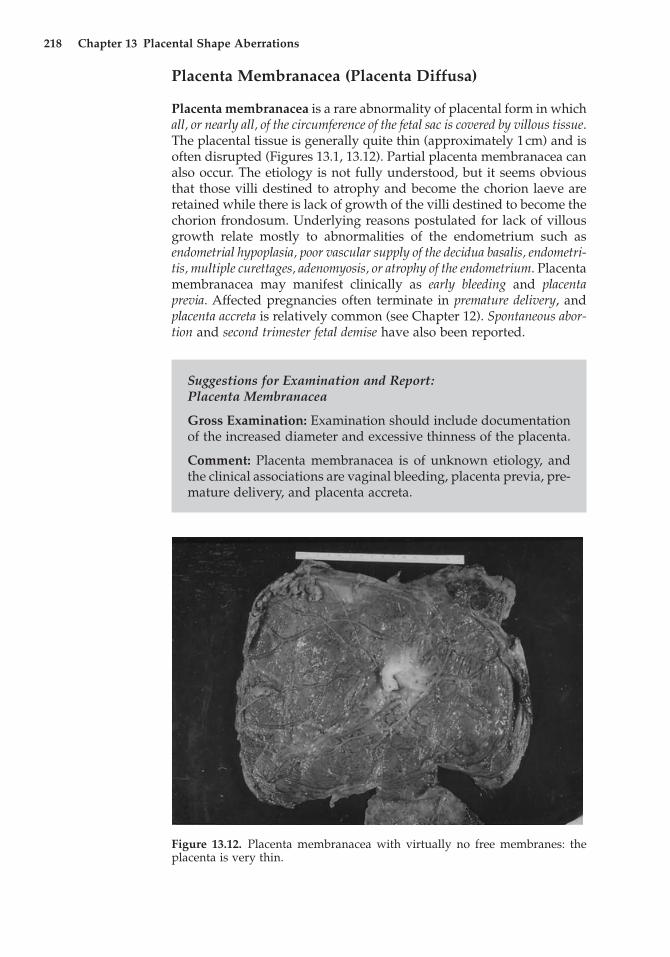
Placenta membranacea is a rare abnormality of placental form in whichall, or nearly all, of the circumference of the fetal sac is covered by villous tissue.The placental tissue is generally quite thin (approximately 1cm) and isoften disrupted (Figures 13.1, 13.12). Partial placenta membranacea canalso occur. The etiology is not fully understood, but it seems obviousthat those villi destined to atrophy and become the chorion laeve areretained while there is lack of growth of the villi destined to become thechorion frondosum. Underlying reasons postulated for lack of villousgrowth relate mostly to abnormalities of the endometrium such asendometrial hypoplasia, poor vascular supply of the decidua basalis, endometri-tis, multiple curettages, adenomyosis, or atrophy of the endometrium. Placentamembranacea may manifest clinically as early bleeding and placentaprevia. Affected pregnancies often terminate in premature delivery, andplacenta accreta is relatively common (see Chapter 12). Spontaneous abor-tion and second trimester fetal demise have also been reported.
218 Chapter 13 Placental Shape Aberrations
Figure 13.12. Placenta membranacea with virtually no free membranes: the placenta is very thin.
Suggestions for Examination and Report: Placenta Membranacea
Gross Examination: Examination should include documentationof the increased diameter and excessive thinness of the placenta.
Comment: Placenta membranacea is of unknown etiology, andthe clinical associations are vaginal bleeding, placenta previa, pre-mature delivery, and placenta accreta.

Miscellaneous Shape Abnormalities
In placenta fenestrata, a central area of the placenta is atrophied sufficiently to leave only membranes (Figures 13.1, 13.13). One must be careful to rule out the possibility of a missing cotyledon. The etiol-ogy is unknown but may be secondary to implantation over a leiomy-oma or cornual tube orifice. Zonary (annular) placentas have a ringshape (Figure 13.1, 13.14). They are likely derived from a placentaprevia with focal atrophy of the low-lying villous tissue covering theinternal os.
Placenta Previa
PathogenesisThe term placenta previa refers to the location of the placenta over theinternal os. The placenta is thus “previous” to the delivering part of thebaby. The overall incidence is somewhere between 0.3% and 1%. When,during early pregnancy, a placenta previa is unmistakably diagnosedthere is often conversion to a “marginal” or higher-lying placenta. Theincidence at midtrimester is 5%, but more than 90% of these “convert”to a non-previa by term. Serial ultrasound examinations throughoutpregnancy have shown that the placenta actually “wanders,” a phe-nomenon referred to as “dynamic placentation.” This placental move-ment is not accomplished, of course, by the placenta unseating and
Placenta Previa 219
Figure 13.3. Placenta fenestrata. The central area of the placenta has a distinct defect, only chorionicmembranes being present. (Courtesy of Dr. L.F. Moreno, Caracas, Venezuela.)

relocating itself, but rather through marginal atrophy on one side andgrowth and expansion on the other, a process called trophotropism.
Pathologic FeaturesIt has become customary to subdivide placenta previa into several cat-egories, such as “central” (total) and “partial” (lateral or marginal) pla-centa previa. The former generally poses the greater threat and requiresearly diagnosis. Vaginal delivery is usually permitted only in a mar-ginal previa. In the vaginally delivered marginal placenta previa, themembranes have no free margin and the edge of the placenta fre-quently is disrupted and hemorrhagic. There are often old clots at thissite, varying from firm, laminated, and brown to friable loose clots or partlynecrotic material that is sometimes green or brown. The fetal vessels of thechorionic surface, when at the edge, may be also disrupted. Portions ofplacenta are occasionally either atrophied or infarcted.
Clinical Features and ImplicationsPlacenta previa is more common in older women, and it is also associ-ated with multiparity, previous abortion, previous cesarean section, and maleinfants. Placenta previa is associated with a higher risk for abruptio, fetalmalpresentation, postpartum hemorrhage, fetal and perinatal mortality, fetalgrowth restriction, fetal anomalies, prolapsed umbilical cord, and, of course,cesarean section. It is one of the principal causes of third trimester bleed-
220 Chapter 13 Placental Shape Aberrations
Figure 13.14. Zonary placenta showing a ringlike configuration. The placentahas been placed on its edge to demonstrate the unusual shape. The membranesruptured and the infant delivered through the opening. The cord inserted tothe side (not seen in this figure).

ing and often necessitates an emergency cesarean section as bothmother and fetus may experience life-threatening hemorrhage. Mater-nal hemorrhage may originate from the placental margin or from thedisrupted intervillous space. Significant neonatal anemia may resultfrom bleeding that occurs from disrupted placental villous vessels orfetomaternal hemorrhage (see Chapter 20).
Placenta previa is often associated with placenta accreta and then is called placenta previa accreta (see Chapter 12). In placenta previa,there is implantation in the lower uterine segment and cervix wherethere is a lack of normal endometrium, and the mucosa does notrespond well to the normal hormonal signals for decidualization. Thus,decidualization is deficient, which is the underlying mechanism in pla-centa accreta. Although placenta previa accreta and cervical pregnancyare relatively rare, the clinical consequences may be dire due to massivehemorrhage and other complications of blood loss.
Selected References 221
Suggestions for Examination and Report: Placenta Previa
Gross Examination: In a vaginal delivery, membrane rupture siteat the placental margin is consistent with a marginal placentalprevia and should be recorded.
Comment: None.
Selected References
PHP4, Chapter 13, pages 399–418 (Placental Shape Aberrations), and Chapter11, pages 320–322 (Extramembranous Pregnancy).
Ahmed A, Gilbert-Barnass E. Placenta membranacea. A developmentalanomaly with diverse clinical presentation. Pediatr Dev Pathol 2003;6:201–202.
Benirschke K. Effects of placental pathology on the embryo and the fetus. In:Wilson JG, Fraser FC (eds) Handbook of teratology, vol 3. New York: PlenumPress, 1977:79–115.
Finn JL. Placenta membranacea. Obstet Gynecol 1954;3:438–440.Fox H, Sen DK. Placenta extrachorialis. A clinico-pathologic study. J Obstet
Gynaecol Br Commonw 1972;79:32–35.Fujikura T, Benson RC, Driscoll SG. The bipartite placenta and its clinical fea-
tures. Am J Obstet Gynecol 1970;107:1013–1017.Lademacher DS, Vermeulen RCW, Harten JJ, et al. Circumvallate placenta and
congenital anomalies. Lancet 1981;1:732.Mathews J. Placenta membranacea. Aust NZ J Obstet Gynaecol 1974;14:45–47.Naeye RL. Placenta previa: predisposing factors and effects on the fetus and
surviving infants. Obstet Gynecol 1978;52:521–525.Naftolin F, Khudr G, Benirschke K, et al. The syndrome of chronic abruptio
placentae, hydrorrhea, and circumvallate placenta. Am J Obstet Gynecol1973;116:347–350.
Perlman M, Tennenbaum A, Menash M, et al. Extramembranous pregnancy:maternal, placental and perinatal implications. Obstet Gynecol 1980;55:34S–37S.

Steemers NY, De Rop C, Van Assche A. Zonary placenta. Int J Gynecol Obstet1995;51:251–253.
Torpin R. Placenta circumvallata and placenta marginata. Obstet Gynecol 1955;6:277–284.
Torpin R. Human placental anomalies: etiology, evolution and historical back-ground. Mo Med 1958;55:353–357.
222 Chapter 13 Placental Shape Aberrations