a biopsy can be avoided in patients with positive dre and ... cohen a.pdf · •despite the use of...
TRANSCRIPT
A biopsy can be avoided in patients with positive DRE and negative MRI
, Michael Cohen :Disagree Chairman, Dept. of Urol.
Haemek M.C, Afula, Israel
Financial and Other Disclosures Off-label use of drugs, devices, or other agents: None or FILL IN HERE; including your
local regulatory agency, such as FDA, EMA, etc.
Data from IRB-approved human research is not presented
2
I have the following financial
interests or relationships to
disclose:
Disclosure code
UC-care Ltd. O,P, former C
Diagnostic value of Prostate MRI – State of the art 2018
• Rule-in disease - Yes
• Recommended by EAU/AUA / NCCN for improved diagnostic rate / repeat Bx
• Rule-out disease –
No,… Not yet…with great caution
• EAU/AUA+ SAR/NICE
Guidelines 2018 • EAU •NCCN •AUA •NICE
…Whether systematic biopsies can be safely omitted with negative mpMRI depends on the
NPV of the mpMRI.

• A 65 y healthy man presents with PSA=10
• DRE – Suspicious lesion on the Right lobe
• mpMRI (1.5T+ERC) >>> MRI-Targeted Bx+ Syst. Bx
Our (…Real…) world Vs.
published studies……. ?
Patient 1 MP-MRI
Patient 1 MP-MRI
Patient 1 MP-MRI
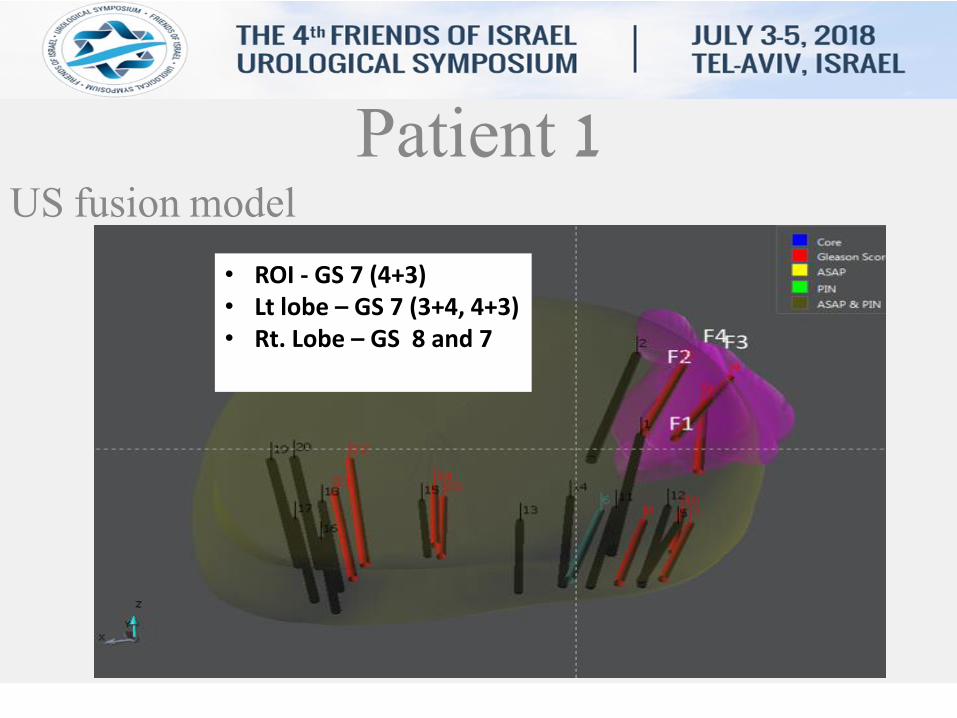
Patient 1 US fusion model
• ROI - GS 7 (4+3)
• Lt lobe – GS 7 (3+4, 4+3) • Rt. Lobe – GS 8 and 7
Guidelines
• EAU • NCCN • AUA • NICE –
5.2.1.Digital rectal examination • Most PCas are located in the peripheral zone and may be detected by DRE
when the volume is ≥ 0.2 mL. • In ~18% of cases, PCa is detected by suspect DRE alone, irrespective of PSA
level [Richie, Urology, 1993]. • The PPV of a suspicious DRE was shown to increase with PSA ,- ( 5%, 14% and
30% with PSA <1, 1-2.5 and 2.6 -4 ng./ml., respectively).[Carvalhal, J Urol, 1999].
• An abnormal DRE is associated with an increased risk of higher GS and is an indication for biopsy [Okotie, Urology, 2007; Gosselaar, Eur Urol, 2008].

Guidelines
• EAU 5.2.4.2 mpMRI –
• PROMIS trial - Designed to evaluate the mpMRI NPV. • 576 men had an mpMRI followed by both TRUS-biopsy and TPM-
biopsy ( reference) . • On TPM-biopsy, overall 71% had cancer; In 40% it was clinically
significant (Gleason score ≥4 + 3 , ≥6mm) . • For clinically significant cancer, mp-MRI had sensitivity of 93%
and specificity of 41%, PPV- 0.51, NPV - 0.89 • mpMRI missed 17 men ( 3%) with csP.Ca • Conclusion - mpMRI, used as a triage test before first prostate
biopsy, could reduce unnecessary biopsies by 27%, and diagnosis of 5% fewer clinically insignificant cancers .
• EAU 5.2.4.2 mpMRI –
• Despite the use of the new PIRADS v2 scoring system ,mpMRI inter-reader reproducibility remains moderate at best [185-188], which currently limits its broad use outside expert centres.
• It is of note that the good results of the PROMIS study were obtained after intensive training of the radiologists involved.
• Non-Reproducibility may lead to a substantial patient mismanagement .
• It is too early to define if quantitative approaches and computer-aided diagnosis (CAD) systems will improve mpMRI accuracy in the future.
185. Rosenkrantz, A.B., et al. Interobserver Reproducibility of the PI-RADS Version 2 Lexicon: A Multicenter Study of Six Experienced Prostate Radiologists. Radiology, 2016. 186. Muller, B.G., et al. Prostate Cancer: Interobserver Agreement and Accuracy with the Revised Prostate Imaging Reporting and Data System at Multiparametric MR Imaging. Radiology, 2015. 187. Zhao, C., et al. The efficiency of multiparametric magnetic resonance imaging (mpMRI) using PI-RADS Version 2 in the diagnosis of clinically significant prostate cancer. Clin Imaging, 2016. 40: 885. https://www.ncbi.nlm.nih.gov/pubmed/27179959 188. Kasel-Seibert, M., et al. Assessment of PI-RADS v2 for the Detection of Prostate Cancer. Eur J Radiol, 2016.
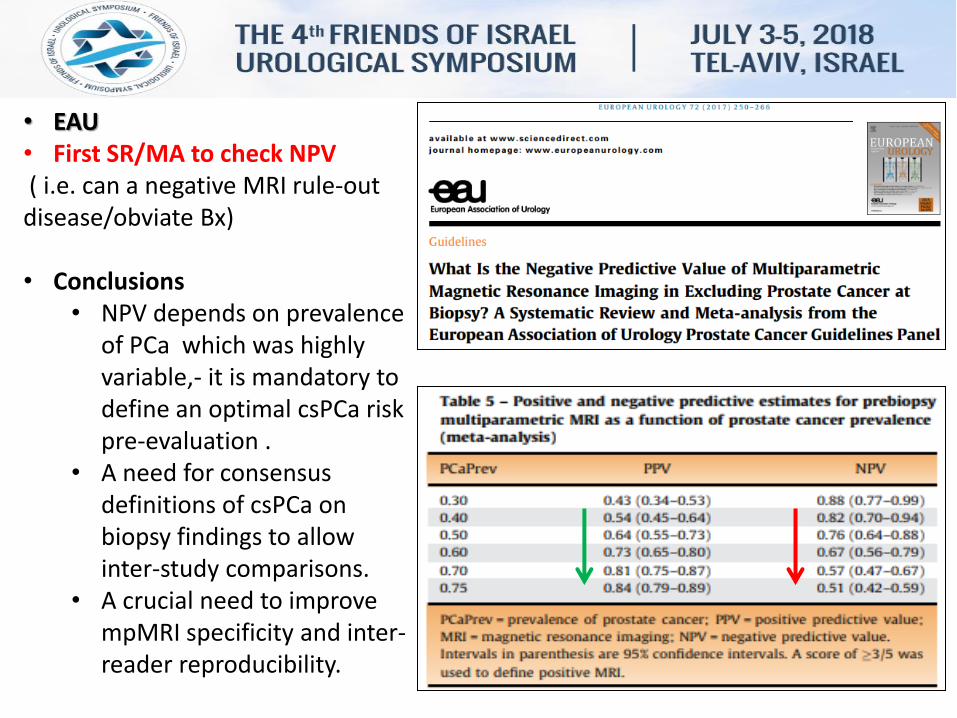
• EAU • First SR/MA to check NPV ( i.e. can a negative MRI rule-out disease/obviate Bx) • Conclusions
• NPV depends on prevalence of PCa which was highly variable,- it is mandatory to define an optimal csPCa risk pre-evaluation .
• A need for consensus definitions of csPCa on biopsy findings to allow inter-study comparisons.
• A crucial need to improve mpMRI specificity and inter-reader reproducibility.
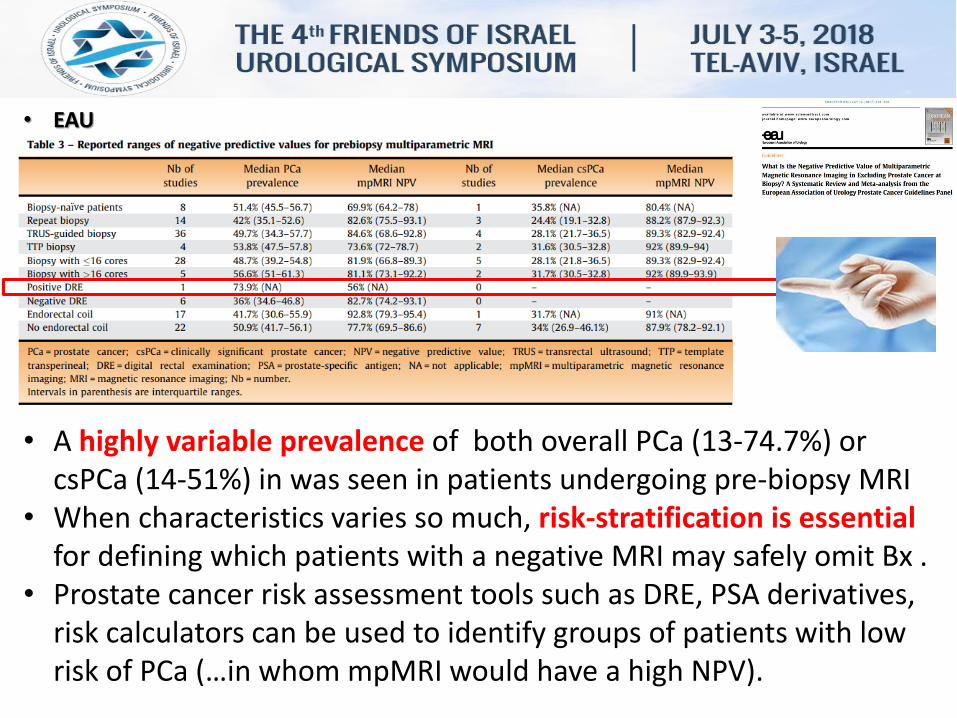
• EAU
• A highly variable prevalence of both overall PCa (13-74.7%) or csPCa (14-51%) in was seen in patients undergoing pre-biopsy MRI
• When characteristics varies so much, risk-stratification is essential for defining which patients with a negative MRI may safely omit Bx .
• Prostate cancer risk assessment tools such as DRE, PSA derivatives, risk calculators can be used to identify groups of patients with low risk of PCa (…in whom mpMRI would have a high NPV).

• EAU
• The impact of these risk-stratification tools on the NPV of pre-biopsy mpMRI needs to be carefully evaluated, both in the biopsy-naïve and in the repeat-biopsy setting.
• For the moment, it is impossible to make any recommendations on the best way to risk stratify patients before referring them for mpMRI
So, … If you suspect a patient for having P.ca >> Do not trust a negative MRI !!!
Guidelines
• NCCN V 2.2018 • Those with a very suspicious DRE should be
considered for biopsy referral regardless of PSA results because it may identify high-risk cancers in such situations.
• DRE should be performed in all men with an abnormal PSA to aid in decisions regarding biopsy.

• Concurrent systematic sampling (…in addition to TBx) – should be considered, case specific, given the number of studies showing a proportion of mpMRI missed csPca.
• Performing solely targeted biopsy should only be
considered once quality assurance efforts have validated the performance of MRI interpretations with results consistent with the published literature.
Guidelines • AUA
Guidelines • NICE –
• 1.2.5 - After initial negative biopsy cancer risk is slightly higher if any of the following exists: • Previous biopsy with HGPIN or ASAP; • Abnormal digital rectal examination.
Magnetic resonance imaging for re-biopsy • 1.2.6 - Consider multiparametric MRI for men with a
previous negative biopsy to determine whether another biopsy is needed.
• 1.2.7 Do not offer another biopsy if the mpMRI is negative, unless any of the risk factors listed in recommendation 1.2.5 are present.
• A biopsy can not be avoided in patients
with positive DRE and negative MRI.
>>> i.e. Do a biopsy ! • A negative MRI should not rule-out cancer
in patients at high risk for P.ca
+ =
conclusion