a clinical clerkship collaborative program in taiwan ... · students, clinical reasoning, decision...
TRANSCRIPT

Journal of the Formosan Medical Association (2016) 115, 418e425
Available online at www.sciencedirect.com
ScienceDirect
journal homepage: www.jfma-onl ine.com
ORIGINAL ARTICLE
A clinical clerkship collaborative programin Taiwan: Acquiring core clinicalcompetencies through patient careresponsibility
Yong A. Wang a, Cheng-Feng Chen a, Chen-Huan Chen b,c,Ging-Long Wang a, Andrew T. Huang a,d,*
a Koo Foundation Sun Yat-Sen Cancer Center, Taipei, Taiwanb Division of Faculty Development, Department of Medical Education, Taipei Veterans GeneralHospital, Taipei, Taiwanc Faculty of Medicine, National Yang Ming University, Taipei, Taiwand Department of Medicine, Duke University, Durham, NC, USA
Received 17 March 2015; received in revised form 12 May 2015; accepted 13 May 2015
KEYWORDSclinical clerkship;clinical skills;mentorship;patient care;undergraduatemedical education
* Corresponding author. Koo FoundaE-mail address: [email protected]
http://dx.doi.org/10.1016/j.jfma.2010929-6646/Copyright ª 2015, FormosaBY-NC-ND license (http://creativecom
Background/Purpose: Traditionally, clinical clerkship training in Taiwan does not provide med-ical students with sufficient patient care responsibilities and often results in inadequate clin-ical skills.Methods: We implemented a pilot clerkship program at a comprehensive cancer center thatemphasizes core clinical competency through direct patient care and dedicated faculty andmentors. Students were an integral part of the patient care team held accountable forproviding coordinated and holistic care. Students’ self-assessment of clinical competencies,faculty evaluation, and objective structured clinical examination were compared against theirpeers trained by traditional clerkship at a main teaching hospital.Results: Fifty medical students completed the clerkship program in the first 3 years. At the endof the clerkship, participants rated themselves significantly higher than their peers in almostall patient care and clinical skill domains. The most significant areas included physical exam-ination, clinical reasoning, developing management plan, holistic approach, handling ethicalissues, and time management skills. The students rated their clerkship teachers significantlyhigher in time spent with students, skills and enthusiasm in teaching, as well as giving studentsappropriate patient care responsibilities. There was no significant difference in the end-of-clerkship objective structured clinical examination performance, but participants of the pro-gram achieved better grades in their subsequent internship.
tion Sun Yat-Sen Cancer Center, 125 Lih-Der Road, Pei-Tou District, Taipei 11259, Taiwan, ROC.rg (A.T. Huang).
5.05.008n Medical Association. Published by Elsevier Taiwan LLC. This is an open access article under the CCmons.org/licenses/by-nc-nd/4.0/).

A clinical clerkship program in Taiwan 419
Conclusion: This pilot collaborative program presented a successful model for clinical educa-tion in the teaching of core clinical competencies through direct patient care responsibilitiesat the clerkship stage. It is hoped that the project will become a catalyst for medical educationreform in Taiwan and regions with similar traditions.Copyright ª 2015, Formosan Medical Association. Published by Elsevier Taiwan LLC. This is anopen access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Figure 1 Block rotation schedule of the 5th-year clinicalclerkship at the National Yang Ming University. Students weredivided into three groups, each starting with medicine, sur-gery, or a combined obstetrics/gynecology, pediatrics, andradiology (Ob-Gyn/Peds/Rad) rotation. Each rotation was 3months in length. Koo Foundation Sun Yat-Sen Cancer Centeraccepted six students for medicine and surgery in each block.Ob-Gyn/Peds/Rad rotation was offered only at the mainteaching hospital.
Introduction
Taiwan’s medical training consists of 7 years of post-secondary medical school followed by residency andfellowship training. Medical students enter clinical clerk-ship in their 5th year followed by internship. Traditionally,during clinical clerkship, medical students observeattending physicians and residents without being involvedin the direct care of patients.1 Fundamental clinical skillsare acquired through lectures, observations, practicing onpeers, or developed on their own initiative without super-vision rather than hands-on supervised learning throughpatient care. When students enter internship or residency,these skills are no longer emphasized. In addition, clerk-ships have almost always been carried out in academicmedical centers where patient care is highly specializedand clinical faculty lack adequate time and motivation toteach the fundamentals of general medicine. These factorscontributed to poor clinical skills and overreliance on im-aging and laboratory tests when students graduate frommedical school.2,3
Early exposure to specialized practice of medicine dur-ing undergraduate and postgraduate training may havecontributed to the uncoordinated and inefficient healthcare delivery. Patients in Taiwan frequently seek care frommany specialists, resulting in the delay of proper manage-ment and wasteful spending of health care resources.Remedies for the fragmented care include strengtheninggeneral medical training and core clinical competencies,including history taking, physical examination, communi-cation, integrated teamwork, professionalism, medicalhumanities, and essential knowledge and skills of medi-cine.4 The Taiwan Medical College Accreditation Council,which was founded in 1999,5 has been promoting a series ofmedical education reform, one of which is clinical educa-tion that emphasizes essential clinical skills and provision ofholistic medical care.
We report here the first 3 years of a collaborativeclerkship program in which medical students of a nationaluniversity medical school undertook medicine and surgeryclerkship at a comprehensive cancer center. The programfocused on building clinical skills through direct patientcare responsibilities, taught by a group of dedicated clin-ical teachers, and with close mentorship by senior physi-cians. We evaluated the program by comparingparticipating students’ self-assessment of clinical skills,evaluation of their clerkship experience, performance inthe objective structured clinical examinations (OSCEs),6
and pre- and post-clerkship grades with those of theirpeers who had undergone traditional clerkship trainingconcurrently.
Methods
Description of the program
The National Yang Ming University (NYMU) is one of thethree government-funded medical schools in Taiwan. TheKoo Foundation Sun Yat-Sen Cancer Center (KF-SYSCC) is acomprehensive cancer center whose missions are to providestate-of-the-art holistic cancer care and to promoteexcellence in medical education. For years prior to theclerkship program, KF-SYSCC had accumulated a significantnumber of experienced clinician educators and had beenactively involved in medical education reform because itsmembers value medical education as one of the primarymechanisms for solving current issues in health care, inparallel with the views of the Institute of Medicine of theUnited States.7 In 2006, NYMU and KF-SYSCC formalizedtheir educational collaboration by establishing the clerk-ship program aimed at innovation, diversity, discipline inclinical education, and emphasis on humane patient care.The collaborative program had obtained funding from theNational Science Council of Taiwan and approval from theMinistry of Health and Welfare.
The collaborative program established an overall su-pervisor, two clerkship directors (1 for medicine and 1 forsurgery), and a liaison business office. The program pro-vided clerkship rotations lasting 3 months each in generalmedicine and surgery, with the remaining rotations stillcarried out at the main teaching hospital (Figure 1). Thus,NYMU students enrolled in the collaborative program spent6 months at KF-SYSCC for medicine and surgery. The

420 Y.A. Wang et al.
program accepted a maximum of 18 students each year, orsix students per rotation block. These students wereincluded as an integral part of the clinical service teamsand involved in hands-on direct patient care. Clinical skillswere emphasized in teaching sessions and daily patientcare. The goals of clinical competency for the clerkshipwere discussed prior to the start of the rotation.
General medicine clerkship
The basic competencies included history taking, physicalexamination, patient presentation, medical record writing,interpretation of imaging and laboratory tests, clinicalreasoning, communication with patients/families and col-leagues, professionalism, and self-directed learning.Patient-centered approach to learning was accomplished inthe following aspects: (1) team-based care of the patient,(2) integrated and coordinated general medical care su-pervised by teaching physicians, (3) bedside rounds andpatient-based conferences, and (4) participation of caremanagers and nursing service for teaching.
Each team consisted of an attending physician, a resi-dent, interns, two to three clerks, and a nurse care man-ager, and cared for 10e12 patients. Team members rotatedmonthly to expose students to a range of styles in teaching,supervision, and interaction with the other members of theteam and consultants. Attending physicians were selectedfrom a panel of internists enthusiastic in clinical teachingand general medicine inpatient practice. The attendingphysicians held responsibilities for all patients cared for bythe team. During the month, other clinical duties werereduced so that the attending physician could focus onteaching and inpatient care. Although KF-SYSCC is a cancercenter, a clinical service was set up specifically to handlegeneral medical issues. The clinical issues varied signifi-cantly, requiring the team to have a broad knowledge andskill base in all areas of medicine, as well as to understandone’s limitations where consultants were invited to join indecision-making and management. The teaching physicianstailored their teaching with a general medicine approachfocusing on foundations of medicine. Periodically,renowned clinical educators from abroad, mainly theUnited States, were invited for a 2-week visiting profes-sorship demonstrating clinical teaching, giving both teach-ers and students valuable opportunities for growth.
Each day, the team met for work rounds, teachingrounds, and radiology rounds that lasted the entire morn-ing. The rounds centered around patient presentations bystudents, clinical reasoning, decision making, issues andtopics arising during the care of the patients, and commu-nication with patients and their families. Clinical pharma-cists, nurse care managers, nutritionists, and social workersalso participated. The students learned through activeparticipation on rounds and interaction with consultantsand other health care disciplines.
Each student took care of one to three patientsconcurrently. Continuous and in-depth involvement in thecare of their assigned patients from admission to dischargewas emphasized, including presenting on daily rounds, dailyclinical care needs, communication with consultants, dailynotes, and acquisition of relevant clinical knowledge.
Students were given progressive patient care responsibilityin both quantity and quality across the clerkship months.Through the direct responsibility for patient care and self-directed learning, students acquired all essential clinicalskills.
A full-time nurse care manager in each team assisted themedical students and helped in coordinating patient care.She also helped the students to adjust to the clinicalenvironment, communicate with other team members andpatients, and understand nursing issues. A nursing unit wasdesignated for the program. Almost all inpatients cared forby the teaching teams were located on the same unit. Thepatients were informed of the arrangement at the time ofadmission. The nursing staff became familiar with the teammodel so that students received support from all patientcare disciplines.
We designed clerk-level patient-based conferences tohelp students reflect on their experiences and learn certainskills in depth. These included observed history taking andphysical examination on admitted patients followed bygroup discussion, disease-specific physical examinationwith didactics and applications on patients with real ab-normalities, clinical reasoning through student case pre-sentations, cardiac auscultation using Harvey (acardiopulmonary simulator), and interpretation of elec-trocardiograms and chest X-rays.
Chart writing has always been a major area of weaknessin physician training in Taiwan because English is not thecountry’s primary language yet medical care is documentedin English. Our students’ notes were extensively reviewedand commented on by several experienced physicians.After each correction, students were expected to demon-strate improvement on subsequent write-ups.
Surgery clerkship
Surgery rotation resembled medical clerkship in itsemphasis on basic clinical skills. In addition, core compe-tencies included general surgical principles, basic surgicaltechniques, preoperative evaluation, and postoperativecare. The program also emphasized critical appraisal ofsurgical literature and communication pertaining toinformed consent and surgical care.
Each clinical team consisted of two attending physi-cians, a resident, and two clinical clerks. The inclusion oftwo attending physicians per month increased case varietyand teaching styles. Similar to medicine, students wereassigned patients so they could assume direct supervisedresponsibilities in preoperative preparation and post-operative care. Students attended daily teaching roundsand chief resident rounds. In addition, students assistedduring surgical procedures performed by the attendingphysicians on the team and sometimes by other surgeons.Basic surgical skills such as sterile and suture techniqueswere taught in the operating room.
An important component in surgical clerkship was theoutpatient clinic. Students participated in the initial eval-uation of ambulatory patients in clinics, where they learnedindications and contraindications for surgery, informedconsent, clinical assessment, and workup in patients withan unestablished diagnosis.

A clinical clerkship program in Taiwan 421
Clerk-level conferences included observed bedsideevaluation, case presentation, critical appraisal of researchliterature, chart writing, and small group topic seriesfocused on general surgical concepts. Students were askedto keep a “learning diary” to reflect on ongoing issues,solutions, or experiences. These were reviewed weekly bythe surgical clerkship director, and sometimes shared withthe student group anonymously if the student author hadagreed. Students also kept a procedure log to keep track ofbasic surgical skills.
Medical humanities, evaluation, and mentorship
Medical humanity was a key element of the clerkship pro-gram at KF-SYSCC and represented a common learningmodule continuing throughout rotations in medicine andsurgery. At the cancer center, students frequentlyencountered life-changing events, extreme emotions, andethical challenges. Biweekly humanities-in-medicineseminar moderated by psychiatrists and senior cliniciansallowed students to discuss humanity issues encountered inthe care of their patients. An optional module was offeredto students to follow a cancer patient over the entireclerkship period. Participating students would select awilling patient they had taken care of early on during theirrotation, keep regular contact with them, and accompanythe patient to appointments as time permitted. Theyshared their experiences in biweekly meetings.
We placed a strong emphasis on formative evaluations.At the end of each month, all clinical team members mettogether in an evaluation meeting and discussed each stu-dent’s performance from various perspectives of theattending physician, the resident, the care manager, andseminar moderators. The meeting allowed the programdirectors and teachers to discuss the progress of the stu-dents and foster continuity of teaching tailored to eachstudent. The clerkship director then gave one-on-onefeedback of the collective evaluation to the student.Ongoing feedback allowed both faculty and students toidentify the problems early and offer opportunities fortargeted improvement. Formative evaluation was also donewith feedback often given in real time in specific areasincluding case write-up, clinical evaluation exercise (mini-CEX), and direct observation of procedural skills.
Summative evaluations were carried out at the end ofthe rotation for clinical performance, chart writing, andOSCE, and were identical for the entire medical schoolclass. Students were also asked to evaluate their teachersand the program. In addition, a student representative atKF-SYSCC was asked to render collective feedback to theprogram directors and mentors.
Mentorship is especially important in the early phase ofthe clinical career of physicians-in-training. In addition toan academic mentor (clerkship director), we assigned aseparate mentor for each student for the entire duration ofthe clerkship year. These mentors were selected from apanel of senior physicians in medicine, psychiatry, radi-ology, and pathology, who were passionate about medicaleducation but were not involved in evaluating the student’sclinical performance. They met with their mentee(s)
regularly and provided guidance and support, sometimeseven beyond clerkship.
Selection of students
For program Year 1, all applicants were accepted. For Year2, the success of the 1st year led more students to expressinterest, which exceeded the maximum capacity of 18.After prospective students were informed of the proposedselection process through application and interview, only18 officially applied and all were then accepted. For Year 3,we held an information session for all interested studentsand formalized the application process. Written applicationand in-person interviews were conducted. Students wereaccepted based on personal attributes, enthusiasm forlearning, and expectations for the clerkship, but not onpreclinical academic performance.
Evaluation of program performance
At the end of the clerkship, all students from both the mainteaching hospital and KF-SYSCC were asked to anonymouslyfill out self-assessment questionnaires on knowledge, skills,and attitudes developed during the clerkship, and to eval-uate faculty teaching. The questions were rated on a 5-point Likert-type scale with 5 being excellent and 1 beingpoor. For self-assessment questions, we calculated theproportions of scores 4 and 5 (good and excellent), andobtained p values using Chi square test comparing studentsfrom the two sites. For faculty evaluation questions, wegrouped the ratings into threedexcellent (5), good (4), andaverage or below (� 3). We separated scores 4 and 5 here,because they represented the vast majority of ratings inboth sites. We obtained the proportions of each ratinggroup and p values using Chi square test comparing the twosites. Students in each of the 3-month blocks from bothsites took the same OSCE developed by the faculty of themain teaching hospital at the end of medicine or surgeryclerkship. We compared those scores using a two-sample ttest with unequal variance. Student characteristics andgrades before, during, and after the 5th year clerkship werecompared between the two sites using Chi square test forcategorical measures and two-sample t test for continuousmeasures. For all tests, we defined an alpha value of 0.05for the level of significance.
Results
A total of 50 students out of 351 NYMU medical studentsfrom three consecutive classes undertook medicine andsurgery clerkship at the KF-SYSCC. The characteristics andacademic performance of students at the two clerkshipsites are summarized in Table 1. No significant differencewas found in terms of age, sex, type of admission to theschool, or premedical course grades between students atthe two clerkship sites, but the KF-SYSCC group had slightlyhigher grades in the preclinical years. During this 3-yearperiod, the number of students interested in and applyingto the KF-SYSCC clerkship increased (Table 2), suggestingstudent appreciation for the program. This may reflect

Table 1 Student characteristics and academic performance.
KF-SYSCC (n Z 50) Main hospital (n Z 301) pa
Age, mean (SD) 23.0 (0.79) 23.2 (1.44) 0.28Sex 0.29Male 29 (58.0) 198 (65.8)Female 21 (42.0) 103 (34.2)
Type of admission to medical schoolb 0.73Via application/interview 16 (32.0) 89 (29.6)Via written entry exam 34 (68.0) 212 (70.4)
Grades (0e100), mean (SD)Year 1e2 (premedical) 84.86 (5.07) 83.55 (4.64) 0.09Year 3e4 (preclinical) 81.61 (3.84) 80.20 (4.62) 0.02Year 5 (clerkship) 85.45 (2.70) 84.17 (2.77) 0.003Year 6e7 (internship) 89.35 (1.37) 88.72 (1.66) 0.004
Data are presented as n (%) unless otherwise indicated.KF-SYSCC Z Koo Foundation Sun Yat-Sen Cancer Center; SD Z standard deviation.a The p values were obtained using the Chi-square test for sex and type of admission to medical school, and two-sample t test for age
and grades in medical school.b Admission to medical schools in Taiwan is traditionally based on national college entrance examination (written) scores. Medical
education reform introduced a new type of admission process wherein some students are admitted through applications and personalinterviews.
422 Y.A. Wang et al.
greater selectivity and motivation in participating studentsduring Year 2 and Year 3.
Student self-assessment
Questions on the “Readiness for Clinical Career” surveytaken at the end of the clerkship year are listed in Figure 2.As students were moving on to the next stage of the clinicaltraining, those who had clerkship at KF-SYSCC felt moreready to take on patient care responsibilities than theirpeers. A higher percentage of students rated themselves ashaving good to excellent preparation in areas of patientcare, communication with colleagues, dealing with clinicaluncertainty and ethics, and ability in self-directed learningand time management. The most statistically significantdifferences were in “compassion for patients” (98% vs. 74%,pZ 0.001), “holistic patient care” (98% vs. 59%, p < 0.001),“time management skills” (68% vs. 39%, p < 0.001), and“handling issues in medical ethics” (90% vs. 51%, p < 0.001).The area where KF-SYSCC students felt less prepared was in“understanding Taiwan’s health care system” (29% vs. 55%,p Z 0.002), as during the clerkship training KF-SYSCC hadplaced more emphasis on patient care than on the insur-ance reimbursement scheme.
In acquisition of clinical skills, KF-SYSCC students alsorated themselves significantly better in the majority ofareas (Figure 3). The difference in physical examination
Table 2 Number of applicants for the KF-SYSCC clerkshipprogram.
Program Expressedinterest
Submittedapplication
Accepted
Year 1 14 14 14Year 2 25 18 18Year 3 35 25 18
KF-SYSCC Z Koo Foundation Sun Yat-Sen Cancer Center.
was particularly significant (93% vs. 48%, p < 0.001), whichhad been a weak area in traditional clerkship programs inTaiwan. Moreover, encouraging students to think throughclinical problems and develop management plans wasemphasized during teaching rounds at KF-SYSCC, and thiswas reflected in the student assessmentd“clinicalreasoning” (78% vs. 45%, p < 0.001) and “developing man-agement plans” (66% vs. 30%, p < 0.001). These two areaswere more difficult for beginners, and we observed a lowerabsolute percentage, but a much larger margin of differ-ence, in comparison with their peers at traditional clerk-ship. The other substantial areas of difference were “casepresentation and oral communication” (78% vs. 49%,p Z 0.001), “history taking” (95% vs. 79%, p Z 0.014), and“chart writing and written communication” (85% vs. 66%,p Z 0.014). Overall, the results aligned with the programgoal for the learners, which was to acquire core clinicalcompetency and to provide holistic patient care.
Evaluation of clinical faculty
Student evaluations of medicine and surgery faculty werecompared (Figure 4). In the area of clinical knowledge,there was no difference between the percentages in the“excellent” category in KF-SYSCC faculty and the mainteaching hospital faculty. However, the KF-SYSCC facultyhad much higher percentages of “excellent” rating in theaspects of attitudes, skills, enthusiasm and time spent inteaching, and giving students appropriate clinical re-sponsibilities (all p < 0.001).
Student performance in OSCE and clinical grades
OSCE was the only short-term assessment of student’sclinical performance that was identical for both sites andmay be relatively standardized. It was designed anddeveloped by the faculty at the main teaching hospital.Stations included evaluation of one standardized patient
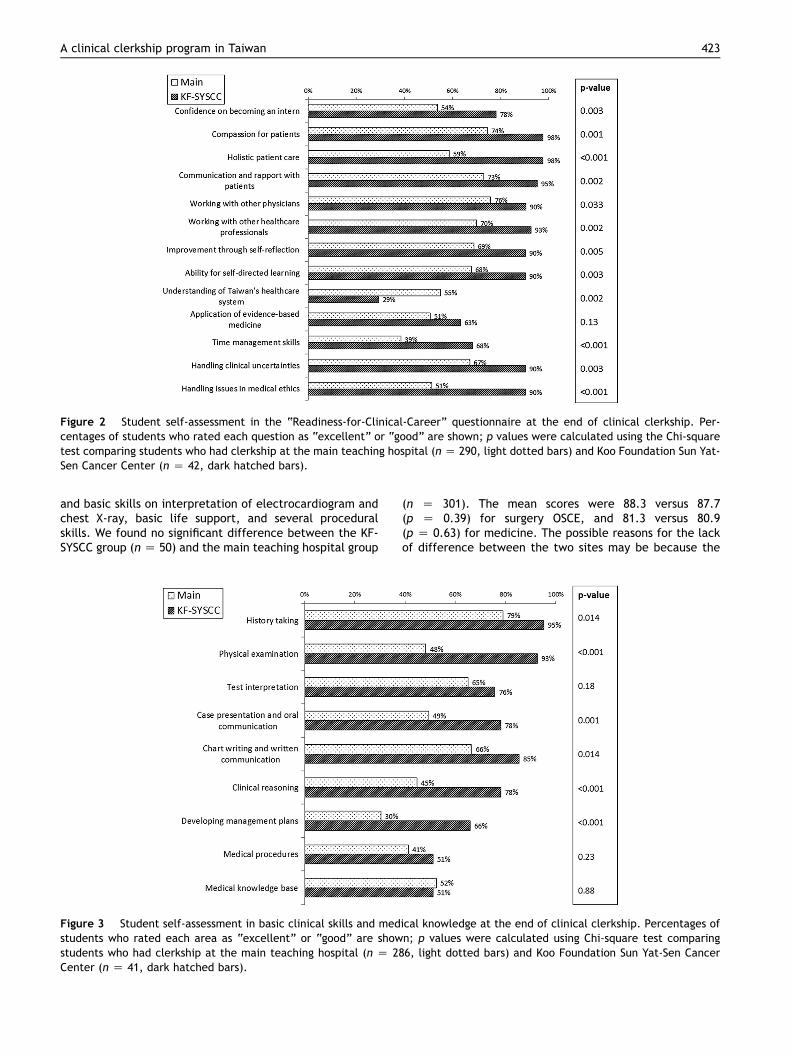
Figure 2 Student self-assessment in the “Readiness-for-Clinical-Career” questionnaire at the end of clinical clerkship. Per-centages of students who rated each question as “excellent” or “good” are shown; p values were calculated using the Chi-squaretest comparing students who had clerkship at the main teaching hospital (n Z 290, light dotted bars) and Koo Foundation Sun Yat-Sen Cancer Center (n Z 42, dark hatched bars).
A clinical clerkship program in Taiwan 423
and basic skills on interpretation of electrocardiogram andchest X-ray, basic life support, and several proceduralskills. We found no significant difference between the KF-SYSCC group (n Z 50) and the main teaching hospital group
Figure 3 Student self-assessment in basic clinical skills and medstudents who rated each area as “excellent” or “good” are showstudents who had clerkship at the main teaching hospital (n Z 28Center (n Z 41, dark hatched bars).
(n Z 301). The mean scores were 88.3 versus 87.7(p Z 0.39) for surgery OSCE, and 81.3 versus 80.9(p Z 0.63) for medicine. The possible reasons for the lackof difference between the two sites may be because the
ical knowledge at the end of clinical clerkship. Percentages ofn; p values were calculated using Chi-square test comparing6, light dotted bars) and Koo Foundation Sun Yat-Sen Cancer

Figure 4 Student evaluation of medicine and surgery faculty at the end of each 3-month clerkship rotation. Percentages ofstudents who rated each category as “excellent” (black), “good” (gray), and “average” or worse (white) are shown. The p valueswere calculated using Chi-square test comparing student evaluations for the main teaching hospital (n Z 286, upper bar for eachcategory) and for Koo Foundation Sun Yat-Sen Cancer Center (KF-SYSCC; n Z 46, lower bar for each category).
424 Y.A. Wang et al.
OSCE, as designed by the faculty of the main teachinghospital, contained only one station that evaluated skills inapproaching a (standardized) patient whereas theremainder were procedure- or skill-based, and that thescoring for each station was given by a single faculty raterfrom the main teaching hospital. It is known that the reli-ability and accuracy of the OSCE for clinical skill evaluationcan be difficult to assess, and depend on the number ofstations, the number of raters per station, and other designfeatures.8
We also compared clinical grades in the clerkship andsubsequent internship years (Table 1). The grades werelargely based on the supervising physicians’ evaluations.We found statistically significantly higher average scores forthe KF-SYSCC students compared with their counterparts atthe main teaching hospital: clerkship (85.45 vs. 84.17,p Z 0.003) and internship (89.35 vs. 88.72, p Z 0.004).However, the differences were small, and the scores fellwithin a very narrow range, suggesting the limitation ofinterpreting these grades.
Discussion
We successfully implemented a clinical clerkship collabo-rative program with dedicated clinician educators, anddemonstrated the effectiveness of clinical learning inte-grated with patient care responsibilities. The results fromthe first 3 years were promising and aligned with the pro-gram goal of emphasizing core clinical skills. At the end ofthe clerkship, students were more confident in their own
clinical skills and were more ready to take on advancedpatient care roles than their peers at traditional clerkship.
Similar to most programs in the United States and Can-ada,4,9,10 our clerkship program used a block rotationdesign for students to become integrated within inpatientcare teams. The distinctive features of our programincluded: (1) explicitly specifying and enthusiasticallyimplementing requirements and goals for students andfaculty in patient care responsibilities and core clinicalskills, (2) having care managers in bridging education andpatient care, (3) frequent multifaceted feedback, and (4)dual mentorship.
Clerkship alumni at various stages of their trainingreturned in yearly reunions and gave us feedback thatfurther reinforced the value of in-depth involvement inpatient care and strong clinical foundations during clerk-ship. Faculty surveys from various specialties and disci-plines showed agreement on the program’s positive impacton personal reward, self-improvement, quality of patientcare, and improvement on medical education. Patientsatisfaction was monitored on a regular basis and consis-tently showed high ratings.
Through these multidimensional evaluations, we identi-fied six key components for the successful implementationof the clerkship program. First, KF-SYSCC had beenconsistently committed to medical education and identifiedfaculties enthusiastic in clinical teaching. The clear insti-tutional policy played a key role in disseminating theeducational culture. A significant amount of manpowerwent into this educational program, with an estimatedequivalent of 13 million TWD (New Taiwan Dollar) per yearinfused into the program by the cancer center. The reason

A clinical clerkship program in Taiwan 425
behind a large financial support to this endeavor is ourwillingness to provide for the students a more conduciveenvironment that could facilitate learning. Coordination bynursing administrators, encouragement by physicianleaders, and designation of supporting nursing units forteaching helped the nursing and operating room staff tobecome accustomed to having medical students in routinepatient care. Second, regular faculty development work-shops and meetings not only improved teaching skills butalso built consensus in educational goals. One such examplewas to emphasize oral presentations during rounds andconsistency in presentation style. Third, patient care re-sponsibility was tailored to clinical maturity of the stu-dents. Students at various stages of the clerkship (Figure 1)had varying degrees of clinical maturity, and we catered toindividual differences. We progressively increased the levelof patient care responsibility, and gave a more advancedcurriculum of bedside teaching to students who had beenthrough prior clinical rotations. Fourth, early and regularformative evaluation was recognized as key steps to traineematuration. We moved the first “end-of-the-month” eval-uation and studentsefaculty feedback to an earlier time.Through two-way feedbacks, evaluation discussions, andmentorestudent encounters, we were able to identifyproblems earlier and allow sufficient time to show im-provements. Fifth, we optimized quantity, time, format,and content of the clerkship seminars to balance patientcontact and didactic learning based on iterative studentand faculty feedback. Finally, dual mentorship providedclose and comprehensive support to students when facedwith changing needs in academic growth, professionalism,ethics, and personal growth.
In summary, this pilot clerkship program provided anurturing environment for learning and direct involvementin patient care where medical students acquired importantclinical skills in their 1st year of entering clinical training.Students felt significantly better prepared for their clinicalcareer after the 6-month curriculum. Although this programwas tailored to the domestic culture and deficiencies inTaiwan’s medical educational system, similar awarenessand reform have been undertaken in other Asiancountries.11e13 It is hoped that the NYMUeKF-SYSCCcollaborative model for clinical clerkship could be dissem-inated while Taiwan and similar countries explore their ownmedical educational reform.
Acknowledgments
This work was supported in part by a grant from the TaiwanMinistry of Science and Technology (formally the National
Science Council; NSC 95-2516-S-368-001-MY3). The authorsthank Zhao-Rong Wu for helping to coordinate the clerkshipprogram and collect data at KF-SYSCC, and Dr Shuu-JiunWang and Mei-Tsu Liu for organizing and providing studentdata from NYMU. The authors express their gratitude andrespect to all the faculty and mentors for their devotion tothe training program, and to all the past and presenttrainees for their valuable feedback to the program.
References
1. Huang KY, Lai CW. Taiwan white paper for medical education.Taipei: Ministry of Education; 2003.
2. Chan WP, Wu TY, Hsieh MS, Chou TY, Wong CS, Fang JT, et al.Students’ view upon graduation: a survey of medical educationin Taiwan. BMC Med Educ 2012;12:127e34.
3. Chu TS, Weed HG, Wu CC, Hsu HY, Lin JT, Hsieh BS. A pro-gramme of accelerated medical education in Taiwan. MedTeach 2009;31:e74e8.
4. Goroll AH, Morrison G, Bass EB, Jablonover R, Blackman D,Platt R, et al. Reforming the core clerkship in internal medi-cine: the SGIM/CDIM Project. Society of General InternalMedicine/Clerkship Directors in Internal Medicine. Ann InternMed 2001;134:30e7.
5. Lai CW. Experiences of accreditation of medical education inTaiwan. J Educ Eval Health Prof 2009;6:2e4.
6. Gaur L, Skochelak S. Evaluating competence in medical stu-dents. JAMA 2004;291:2143.
7. Institute of Medicine. Academic health centers: leading changein the 21st century. Washington, D.C.: National Academy Press;2003.
8. Brannick MT, Erol-Korkmaz HT, Prewett M. A systematic reviewof the reliability of objective structured clinical examinationscores. Med Educ 2011;45:1181e9.
9. Whelan A, Appel J, Alper EJ, De Fer TM, Dickinson TA, Fazio SB,et al. The future of medical student education in internalmedicine. Am J Med 2004;116:576e80.
10. Veale P, Carson J, Coderre S, Woloschuk W, Wright B,McLaughlin K. Filling in the gaps of clerkship with a compre-hensive clinical skills curriculum. Adv Health Sci Educ TheoryPract 2014;19:699e707.
11. Farrell SE, Takada K, Armstrong EG, Tanaka Y, Aretz HT. Re-form of a traditional clinical curriculum in Japan: experiencesat Tokyo Medical and Dental University. Med Teach 2009;31:947e9.
12. Lai NM, Sivalingam N, Ramesh JC. Medical students in theirfinal six months of training: progress in self-perceived clinicalcompetence, and relationship between experience and confi-dence in practical skills. Singapore Med J 2007;48:1018e27.
13. Yu F, Xu L, Lu D, Luo W, Wang Q. The integrated clerkship: aninnovative model for delivering clinical education at the Zhe-jiang University School of Medicine. Acad Med 2009;84:886e94.