a complex patient with type 2 diabetes and moderate ckd...
TRANSCRIPT

A Complex Patient With Type 2 Diabetes and Moderate CKD –Clinical Consult Case 2
1
The following is a transcript from a web-based CME-certified multimedia activity.
This enduring activity is provided by Joslin Diabetes Center in collaborationwith Haymarket Medical Education.
This enduring activity is supported by an educational grant from AstraZeneca, LP.
DR. JEFFREY R. UNGER: Welcome to Clinical Consult Case 2. I’m Dr. Jeff Unger, Assistant ClinicalProfessor of Family Medicine at Loma Linda University School of Medicine in Loma Linda, California.
With me today are Drs. Robert Stanton and Vivian Fonseca. Dr. Stanton is Associate Professor of Medicineat Harvard Medical School and Chief of the Nephrology Section at Joslin Diabetes Center in Boston.Dr. Fonseca is Professor of Medicine and Pharmacology and Chief, Section of Endocrinology, at TulaneUniversity Health Sciences Center in New Orleans.
So we are here to discuss a male patient with type 2 diabetes and complications of moderate chronickidney disease.
Jeffrey R. UngerProgram ChairAssistant Clinical Professorof Family Medicine
Loma Linda UniversitySchool of Medicine
Loma Linda, CAChino Medical Group Inc.Chino, CA
Vivian FonsecaProfessor of Medicineand PharmacologyTullis Tulane AlumniChair in DiabetesChief, Sectionof Endocrinology
Tulane University HealthSciences CenterNew Orleans, LA
Robert Stanton, MDAssociate Professor,Department of MedicineHarvard Medical SchoolActive Staff, NephrologyBeth Israel DeaconessMedical Center
Kidney andHypertension Division
Joslin Diabetes CenterBoston, MA

Let me introduce you to this patient. He is an African American man, 67 years of age, diagnosed with type 2diabetes about 10 years ago. I switched him from oral hypoglycemic agents, which were pioglitazone,glimepiride, and metformin, to insulin treatment, where he was maintained on metformin and glimepirideuntil 1 year ago. Then he had an acute myocardial infarction.
The patient has gained about 15 pounds over the past year. He has had frequent episodes of mild hypo-glycemia over the past year as well, and 1 severe episode of hypoglycemia that required him to be takento the emergency room.
His physical exam is: height 5 feet, 9 inches; BMI 33.9, putting him in the overweight category. His bloodpressure is elevated at 145/95. His cardiopulmonary exam is normal. He has mild edema over the anklesbut no other signs of congestive heart failure.
These are his chemistries: His fasting glucose level is 130 mg/dL; 2-hour postprandial is 210. His A1C is9.2%. LDL is 68, HDL 41, triglycerides 151. Total cholesterol is 139. Serum creatinine is 1.4 and his urinealbumin/creatinine ratio is 250 mg/g. His GFR is only 48.
So, with this information that we have so far, Vivian, can you comment on the A1C—and what would youput his target at if he has already had an MI and that was 1 year ago?
A Complex Patient With Type 2 Diabetes and Moderate CKD –Clinical Consult Case 2
2

DR. VIVIAN A. FONSECA: This is a challenging patient and we see many of them like this. He hasmultiple comorbidities. But I think the most complex of all is the presence of chronic kidney disease thatis reaching to a point where you have to start thinking about giving him the appropriate medication thatcan be used and what cannot be used in his treatment.
He has also had a myocardial infarction, which puts him at risk of another MI. You put him at risk forheart failure, depending on your choice of medication. He is at risk of something really bad happeningto him. Yet you want to halt the progression of his disease.
For that, I think you have to have personalized goals or individualized goals. I would try to bring his A1Cdown; it is really very high: 9.2. Even though you are worried about giving him a myocardial infarctionor increasing mortality if you bring him down too aggressively, at 9.2 he is at risk of progression of hiskidney disease and progression of his retinopathy and maybe neuropathy you are developing.
DR. JEFFREY R. UNGER: He told me that he is deathly afraid of hypoglycemia. In fact, he is so afraid ofhypoglycemia that sometimes he stops using his insulin because he doesn’t want to go low. We know thatthere is a higher risk of death due to hypoglycemia based on the ACCORD trials. So what would I tell him?
DR. VIVIAN A. FONSECA: It’s very scary to patients and maybe should be scary to physicians as well, be-cause you are identifying somebody who is at risk of a lot of bad things happening to them. Actually, whathe just told me is not uncommon; people don’t take their medication when they see the side effects. Thisalso explains partly the discrepancy. His fasting glucose is not that high, whereas his A1C is quite high. Sohe is probably skipping his insulin off and on and testing only when he takes it so he gets a good result.
DR. JEFFREY R. UNGER: What would you want his A1C to be according to the ADA guidelines?
DR. VIVIAN A. FONSECA: I think if you consider this concept of individualization, I’m comfortable withhim being in the 7.5 to 8.0 percent range. Above 8.0 percent, he is at risk of progression of those compli-cations I mentioned. Below 7.5 percent, the risk of hypoglycemia and the kind of problems that occurredin the ACCORD trial may be a little on the high side. I would still be wary about drugs that cause hypo-glycemia. So he is on insulin and glimepiride. I think we need to be a little cautious about that.
DR. JEFFREY R. UNGER: Absolutely. And so, Bob, I’m so happy you’re here because you’re a nephrol-ogist and it’s very unusual to have Dr. Fonseca and you here in my office at the same time. But this guy’sgot chronic kidney disease. Tell me about chronic kidney disease and where we are in the course of thispatient’s diagnosis and treatment strategy. And also, what about what Vivian said about glimepiride, asulfonylurea, using it in a patient with stage 3 chronic kidney disease?
DR. ROBERT C. STANTON: As you said, he falls in the stage 3 at this point, which is between GFRs of30 and 59, as such. There’s a lot of debate about what is… when you call somebody kidney disease or not,because as we age, GFR, like everything in life, goes down: GFR goes down and so your kidney disease…kidney function declines normally. But at 48 or 50 at the GFRs, that’s not normal at this point. Certainlyanybody less than 45 is clearly abnormal at any age, as such.
As far as the drug, first, is concerned, all the drugs start to last longer as your kidney disease gets worse.That is probably the easiest way to remember it. So the risk of the hypoglycemia becomes that muchgreater, especially with sulfonylureas, but a lot of the drugs will last longer. Even insulin, when you getto end-stage kidney disease, lasts. That often happens, and people say, “I need less insulin.” It’s actuallythat your kidney disease got so bad—so that’s not really a good thing at that point. But that’s the maineffect there.
As far as interventions here, you really want to get involved as soon as possible to get [a] slowdown ofprogression of disease. It’s good to look back and see how much has changed. It’s an interesting pointhere: his creatinine is in a pretty good range, and if you don’t do the calculation, you may think he is alot better off than he is. And that is very typical of people as we age; again, you need to do the calculationof the GFR to know where they are.
A Complex Patient With Type 2 Diabetes and Moderate CKD –Clinical Consult Case 2
3

So the main goals here for him are as Vivian said. Glucose is number one, even for a type 2 patient here,because it is significantly elevated. The range, I would agree with from the kidney, looks like when youget below 8 percent, the actual benefit for kidney disease is small, if at all. So that’s the target for there.But as you go up, there are significant changes.
The blood pressure—especially for type 2 patients—you are really looking for a significant lowering ofblood pressure. And lastly, if he is not on an ACE or an ARB, with his—I would say mild-to-moderate—elevation of protein in the urine, you would want to start him on an ACE or ARB. They are very useful ifyou have protein in the urine. This is kind of an intermediate range. If it was higher, you would definitelybe sure that you would be on it, but for most people here I would say you would want to be on an ACE/ARB.
DR. JEFFREY R. UNGER: I would think that as a primary care physician I would need to be a little bitmore aware of renal function so that I could tell my patient at an earlier stage of the disease so somethingcould be done. Am I right in this assumption?
DR. ROBERT C. STANTON: You are absolutely correct. I instituted at Joslin Diabetes Center many yearsago graphs. But what can happen over time is if you can graph the GFR particularly—what looks like paintdrying over years—you will see a steady decline. The graphs showing the patient all along the way look likethere was not much change 6-month periods apart. But over 4 or 5 years, there was a very steady decline.
So it is very important to start as early as possible. USRDS data, which is the United States Renal DataSurvey, comes out every year. You can look it up online. But they had a rather stunning statistic: thepercent of patients who started dialysis who never saw a kidney doctor until they started dialysis was42 percent in the United States. And within 12 months of starting dialysis, was near 30 percent.
Almost 75 percent of the patients never saw a kidney doctor until they started dialysis, until within12 months of starting dialysis. So to me, that represents that people are just not thinking about it untilit’s often too late.
DR. JEFFREY R. UNGER: So Vivian wants the A1C to be 7.5 percent. His lipids are at target. His LDLis at 68. Where would you want his blood pressure?
DR. ROBERT C. STANTON: That’s a very interesting subject right now. Every guideline is all over theplace. Some of the guideline committees I think have gone a little crazy here, because it comes downto randomized controlled trials, double-blinded. It’s the only thing everybody is looking at. So they arethrowing out all these other studies.
A Complex Patient With Type 2 Diabetes and Moderate CKD –Clinical Consult Case 2
4
The current guideline says 140/80 or better, things like this. I am looking definitely below that. But myproblem with the current recommendations is that it’s really less than 140/80, so it is really between130 and 140 over 75 to 80. That’s where you’re looking for. So in my mind, as a primary care doctor, Iwould think 130/80 as my goal just to make sure I am getting below the 140/80, not the 140/80—unlessyou might think that 145 or 85 is good. It’s not. You want to get it down lower.
DR. JEFFREY R. UNGER: That’s what the ADA says.
DR. VIVIAN A. FONSECA: Yes, but although that’s a general goal, isn’t it true that in people with kidneydisease, established kidney disease that’s progressing, a lower goal might help slow that progression?
DR. ROBERT C. STANTON: Now I’m a fan of 130/80 or better, but there is actually a lot of discussionright now ongoing of “do we really have the data to support lower blood pressures based on that samelogic?”. There are lots of smaller studies suggesting lower is better in many combinations, but the big,large, randomized, controlled trial to say that less than 130/80 is definitely better is not there.
The feeling is, as protein levels rise, you get to 500 mg or 1000 mg, and then you should be lowering yourblood pressures more. But it is now quite a debate in the world. But I would say lower; in my general view,130/80 is a very fine target.
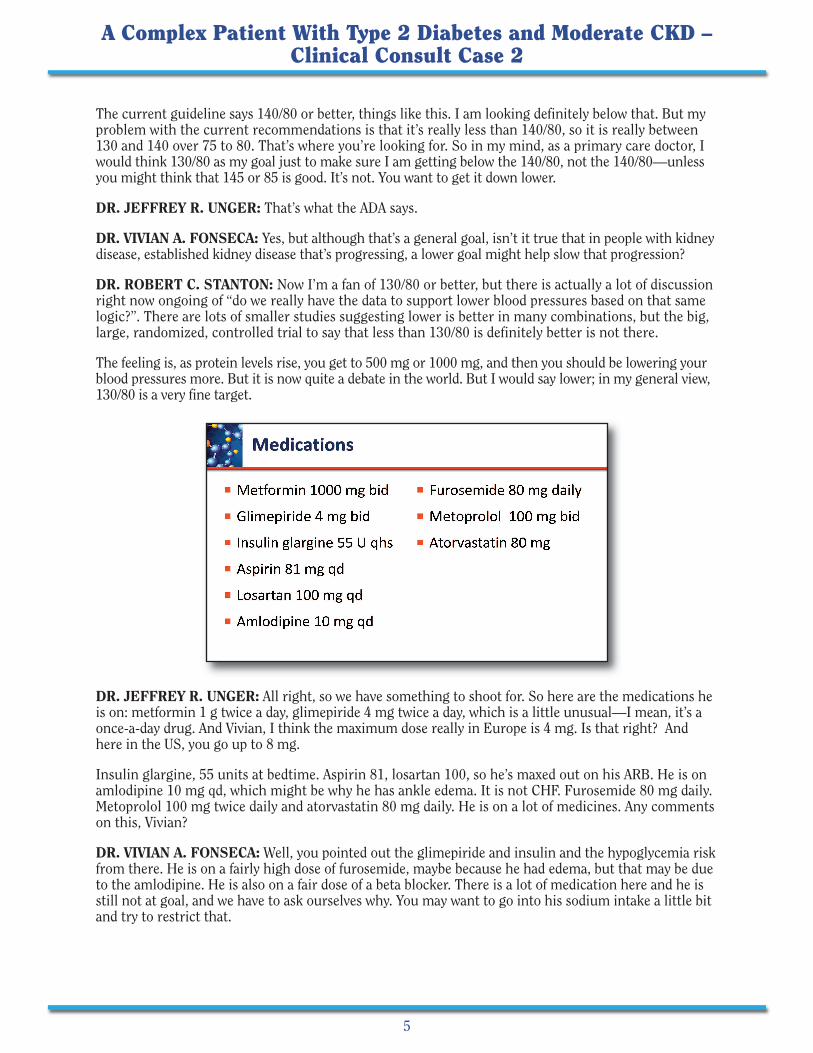
DR. JEFFREY R. UNGER: All right, so we have something to shoot for. So here are the medications heis on: metformin 1 g twice a day, glimepiride 4 mg twice a day, which is a little unusual—I mean, it’s aonce-a-day drug. And Vivian, I think the maximum dose really in Europe is 4 mg. Is that right? Andhere in the US, you go up to 8 mg.
Insulin glargine, 55 units at bedtime. Aspirin 81, losartan 100, so he’s maxed out on his ARB. He is onamlodipine 10 mg qd, which might be why he has ankle edema. It is not CHF. Furosemide 80 mg daily.Metoprolol 100 mg twice daily and atorvastatin 80 mg daily. He is on a lot of medicines. Any commentson this, Vivian?
DR. VIVIAN A. FONSECA: Well, you pointed out the glimepiride and insulin and the hypoglycemia riskfrom there. He is on a fairly high dose of furosemide, maybe because he had edema, but that may be dueto the amlodipine. He is also on a fair dose of a beta blocker. There is a lot of medication here and he isstill not at goal, and we have to ask ourselves why. You may want to go into his sodium intake a little bitand try to restrict that.
A Complex Patient With Type 2 Diabetes and Moderate CKD –Clinical Consult Case 2
5

DR. JEFFREY R. UNGER: One of the other things we see in primary care that I think is often missed: ifyou have a persistent rise in A1C and it is not coming down, not only are we looking at adherence but alsodepression. You can get depressed after an MI. And this has to be looked into as well. If you are depressed,you might be distressed about even having diabetes, and these things need to be looked into.
So this is what we did.
We put him on liraglutide, which is a GLP-1 receptor agonist. We started him at 0.6 mg, then uptitratedhim to 1.8 mg over about a 3-week period of time. And then, Vivian, he developed nausea and stoppedthe drug. Didn’t like that. So the insulin glargine was reduced while we started the GLP-1 to 45 units.And after liraglutide was abandoned, the patient was instructed to uptitrate the glargine dose to a fastingglucose of around 130. So now he is up to 60 units a day, and I want you to comment on this particulardose and what the best way would be to dose insulin glargine at this point.
DR. VIVIAN A. FONSECA: I think to titrate glargine is very appropriate and can be done in practice;can be done by patients themselves using the fasting glucose. But you have a situation here where youare limited by 2 things. One is, the fasting is not too bad, assuming he’s brought it down recently, buthe is also getting hypoglycemia. And it’s very challenging in that situation.
A Complex Patient With Type 2 Diabetes and Moderate CKD –Clinical Consult Case 2
6

Not only should we uptitrate, we should also downtitrate when patients get hypoglycemia. So if he isgetting either recording of less than 80 or he’s getting symptoms, we need to back off a little bit. So weneed to look at other alternative therapies here because he is still higher than what we want him to be.
DR. JEFFREY R. UNGER: Yes, fortunately his A1C is coming down after 3 months. It’s down from 9.2to 8.3 percent, so we are making some progress. So the decision now is made—because we are worriedabout hypoglycemia and worried about weight gain and some of these other issues, and the patient isstill reporting episodes of hypoglycemia. So let’s do this. Let’s add canagliflozin 100 mg every day andthen we are going to decrease the insulin dose—the glargine—to 50 units at bedtime.
And then we follow up 6 months later and things look pretty good. So, Bob, what do you think of this?A1C is 7.4 percent. He has no episodes of hypoglycemia. He has actually lost some weight. His bloodpressure is looking good. But golly gee whiz, his GFR is down to 42 and his creatinine has gone up to1.7. As a primary care doctor, I’m a little bit worried. Am I making the kidneys sicker?
DR. ROBERT C. STANTON: So anytime the creatinine increases, GFR goes down. You always want tothink about, is there something in the kidney that’s going on that is not related to your first thought,which may be a drug-related effect? So you always want to look at urinalysis to look for the causes,things like general practice.
Beyond that, if this is related to the drug treatments, there are a couple of things that have taken place.The SGLT2 inhibitor tends to cause a modest or small increase in creatinine, though usually not thismuch. But it does also cause fluid loss through an osmotic diuresis, and that can lead to moderatedehydration. And depending on the effect of that—based on, I believe, he is also on furosemide—youcould get a combined effect of getting possibly too dehydrated.
Then, on top of that, he’s on losartan. And losartan, by blocking angiotensin-2 effect, interferes with thenormal kidney autoregulation that would maintain GFR. So if that is what took place and it is stable at1.7, then actually this is a combination of events that would suspect stability. The only way to find thatout would be: Don’t do anything necessarily. Check it 2 weeks later, a month later, and recheck it. If it isalways 1.7, then he’s at a steady state based on all these new changes. If you are concerned that this isgetting worse or dehydration is too much or something like that, then maybe you may want to make adrug dose change.
DR. JEFFREY R. UNGER: Let’s go back to the initial issue here. I’m starting an SGLT2 inhibitor. Areall SGLT2s inhibitors appropriate for patients that have moderate kidney disease?
A Complex Patient With Type 2 Diabetes and Moderate CKD –Clinical Consult Case 2
7

DR. ROBERT C. STANTON: The concern over SGLT2s and moderate kidney disease at this point is, one,do they lose efficacy as the GFR decreases? And that may be due to: you do not have as many nephrons inplace, so you don’t really get the effect. That seems to be the case, that they are not as effective.
Another concern is whether when you constantly give glucose to a distal part of the tubules that usuallysee glucose, will that be a problem in the long run? Nobody knows the answer to that, to that effect. Atthe moment, SGLT2 inhibitors are not indicated, depending on the drug, either for GFRs of less than 60or GFRs of less than 45. At this point, I would follow that treatment. That is why it is also important tocalculate GFRs on all these people, rather than just using the creatinines. There are a number of studiesgoing on now with lower GFRs and kidney disease, but until we get some results there, I would not usethem except as they are recommended right now.
DR. JEFFREY R. UNGER: So Vivian, what drugs can we use with a GFR less than 60?
DR. VIVIAN A. FONSECA: Dapagliflozin in its label is indicated only for people with a GFR above 60,so I would not have used it here. And you were very right in choosing canagliflozin only 100 mg,because that’s the usual starting dose. But I notice you did not go up to 300, because between 45 and60 it is recommended you only use 100 mg. You can use 300 if it is over 60.
There are other considerations when you start getting renal impairment. You should be very cautiouswith GLP-1 receptor agonists because you get nausea that might dehydrate the patient. And he hasstopped his medication. If he had continued with nausea and vomiting, he might have had that problem.
DPP-4 inhibitors—except with linagliptin—with all the others, you have to reduce the dose as yourGFR keeps dropping. You go down from 100 of sitagliptin to 50, and then as you get GFR below 30, youreduce it further to 25. That requires a fair amount of monitoring, and it’s a challenge for the patientand the physician. So I think in relation to SGLT2 inhibitors, you use the lower dose of canagliflozinand empagliflozin when the GFR is between 45 and 60 and do not use dapagliflozin.
DR. JEFFREY R. UNGER: So the side effects of SGLT2 inhibitors include dry mouth, orthostatic hyper-tension, [and] possible dehydration. There are also urinary tract infections and fungal infections. Thispatient has a GFR of now 42. Is he going to get more side effects because of that GFR, Vivian? Do I needto do something?
DR. VIVIAN A. FONSECA: Well, I think now it’s fallen below 45. However, it’s happened very acutely andhe’s on a high dose of a loop diuretic. And his blood pressure is falling a lot, so that makes me worriedabout him being a little dehydrated. And I wonder if we rehydrate him whether the GFR will come up, andmaybe Bob could comment on that.
DR. ROBERT C. STANTON: I would agree. I think that, again, we are weighing what is the cost-benefithere. An easy thing to do would be just to cut back on the furosemide, especially if he doesn’t have otheredema or anything else. Just cut back on the furosemide and see what happens.
DR. JEFFREY R. UNGER: I’m really nervous about the metformin, too. I’ve read some stuff about [how]with GFRs less than 45, you should not continue metformin. What is your thought on that?
DR. ROBERT C. STANTON: Metformin has been around a long time, and the main concern is the lacticacidosis that people worry about. Again, when the drugs were first developed, it was phenformin whenthey first came out and reused that had the higher rates of lactic acidosis. Metformin clearly has a rate oflactic acidosis, except it seems to be quite low.
The situation here that’s a little different is that the kidney function has gotten worse. If it is getting worse,the question is, how fast is that changing? There is pretty good evidence that if creatinine is rising, GFR isdropping. If that happens fairly acutely, you should stop the metformin, because that is the situation wherewe often do see the lactic acidosis. But if this is a chronic stable effect, then maybe just cutting back thedose. I believe he’s on—
DR. JEFFREY R. UNGER: He’s at 1 g twice daily.
A Complex Patient With Type 2 Diabetes and Moderate CKD –Clinical Consult Case 2
8
DR. ROBERT C. STANTON: Twice a day, so going to maybe 1 g once a day is okay. Some of us arerecommending maybe even GFRs down to 30. When you get below 50, go to 1 g a day total, 500 twicea day. And that’s what is being done in Canada and Australia and other places’ recommendations. So inthis case, if you think it’s going to be in the 40s, I might cut back from bid to qd.
DR. JEFFREY R. UNGER: Vivian, I see you getting a little antsy here. What would you do with hismetformin, 42 GFR?
DR. VIVIAN A. FONSECA: Well, first I’m hoping that if you take him off his furosemide or reduce thedose, the GFR will come up a little bit and you will be able to continue because it’s a real challenge. Ifyou stop his metformin and you stop his SGLT2 inhibitor and he’s getting hypoglycemia from hisglimepiride—which, by the way, is not metabolized in the kidney to the same degree as glyburide, soit’s the better drug—but still he’s getting hypoglycemia. And the insulin action is being prolonged.You’re between a rock and hard place here with this guy. He needs a lot of medications and you can’tuse some. It becomes very, very challenging. So I would see him fairly frequently until he’s stabilized,make adjustments in his medications, and hope that you can keep him stable with a reasonable GFR.
DR. JEFFREY R. UNGER: All good advice. So there are a lot of questions here. Do we continue with theSGLT2 inhibitor? I would say yes, we need to do that. We probably ought to cut back on the metforminfrom 1 g twice a day to 1 g a day. We would maintain his insulin dose with frequent monitoring, at leastfasting and possibly even bedtime monitoring, making sure that he is not getting hypoglycemic overnight.We would stop the furosemide and add chlorthalidone 25 mg, and then see him back in 6 weeks.
So we see him back in 6 weeks—Bob, this guy would make you happy. His blood pressure is now 134/84,which I think is close to target and blood pressure varies throughout the day. If we are getting this, he’slooking pretty good. The GFR has magically gone back up to 49. His creatinine has gone up a little bit, 1.5,but actually it’s down from 1.7. So I think we have saved the day with you guys serving as our surrogateadvisors here, which is really nice.
DR. VIVIAN A. FONSECA: No magic, Jeff, we gave you good advice.
DR. JEFFREY R. UNGER: Which I will certainly pay for! (Laughter) So this is a very typical case thatwe see in primary care because nothing stays the same in diabetes, as you know. It’s always different, soit’s a fluid situation.
Sometimes—interestingly, from my point—patients kind of get nervous if they come in one time, Vivian,and we put them on a drug A, and then the next time they’re seen we have to say, “No, stop A, let’s go todrug B.” And then 6 months later, we’re back to drug A. They think we’re crazy and don’t know whatwe’re doing. What do you think? How do you manage that?
DR. VIVIAN A. FONSECA: I think it’s very important for patients to be told that they have a complexdisease; that they’re going to need adjustments, particularly a guy like this at this stage. It’s going tokeep happening. And, as Bob was pointing out, you can plot the decline in GFR over time, and you wantto keep him aware of what is going on so you can prepare him—eventually he’s going to need dialysis.And prepare him for that. Hopefully you can slow it down, slow that progression for as long as possible.But it’s challenging.
DR. JEFFREY R. UNGER: I think on the other hand, the worst thing we can do is do nothing, to justleave him alone—because studies have also shown that it could take years, sometimes 7 to 10 years, tointensify somebody’s diabetes control when their A1C is above 8. And that does nobody any good at all.So we need to get the show on the road. We need to try something. We need to get the blood pressureunder control, the lipids under control, and the glycemic control improved as well over time.
So this highlights some of the issues we can consider in adding an SGLT2 inhibitor to the treatmentregimen of a patient with very complicated diabetes.
Thank you very much for joining us today. I also urge you to participate in the first Clinical Consult Caseand the Medically Speaking Roundtable webcast on SGLT2 inhibitors on myCME.com. Thank you again.
A Complex Patient With Type 2 Diabetes and Moderate CKD –Clinical Consult Case 2
9