abnormal pregnancy
DESCRIPTION
Abnormal Pregnancy. CAPT Mike Hughey, MC, USNR. Incidence of Miscarriage. 1 in every 6 pregnancies Risk of subsequent miscarriage 1/6 Bedrest will not prevent miscarriage but may postpone it. Causes of Miscarriage. 60% chromosome abnormalities 30% placental malformation - PowerPoint PPT PresentationTRANSCRIPT

Operational Obstetrics & Gynecology · Bureau of Medicine and Surgery · 2000 Slide 1
Abnormal Pregnancy
CAPT Mike Hughey, MC, USNR
Operational Obstetrics & Gynecology · Bureau of Medicine and Surgery · 2000 Slide 2
Incidence of Miscarriage
• 1 in every 6 pregnancies
• Risk of subsequent miscarriage 1/6
• Bedrest will not prevent miscarriage but may postpone it

Operational Obstetrics & Gynecology · Bureau of Medicine and Surgery · 2000 Slide 3
Causes of Miscarriage• 60% chromosome abnormalities
• 30% placental malformation
• 10% miscellaneous, but not: -trauma -climbing mountains -intercourse -medication -too much activity, etc.

Operational Obstetrics & Gynecology · Bureau of Medicine and Surgery · 2000 Slide 4
Threatened Abortion
• 1 in every 4 pregnancies
• 1st TM bleeding/cramping
• Half will abort, Half will be OK
• Bedrest will not prevent abortion but may postpone it.

Operational Obstetrics & Gynecology · Bureau of Medicine and Surgery · 2000 Slide 5
Complete Abortion
• Passage of all tissue
• Rest for a day or two
• Ergotrate, Oxytocin
• Antibiotics
• Rhogam
• D&C?9-week spontaneous complete abortion

Operational Obstetrics & Gynecology · Bureau of Medicine and Surgery · 2000 Slide 6
Incomplete Abortion: Diagnosis
• Some tissue remains behind
• Continuing bleeding/cramping
• Tissue in cervical os
• Uterus tender
• Fever if infection present
• Ultrasound helpful if available

Operational Obstetrics & Gynecology · Bureau of Medicine and Surgery · 2000 Slide 7
Incomplete Abortion: Treatment• Convert it to a Complete
Abortion
• If tissue visible in the os, remove it
• Ergotrate, Oxytocin
• Antibiotics
• Rhogam
• D&C
Tissue removed from os
Tissue still inside uterus

Operational Obstetrics & Gynecology · Bureau of Medicine and Surgery · 2000 Slide 8
Inevitable Abortion
• No tissue has been passed
• Cervix dilated or hemorrhage
• Ergotrate, Oxytocin
• Antibiotics
• Rhogam
• D&C
Operational Obstetrics & Gynecology · Bureau of Medicine and Surgery · 2000 Slide 9
Septic Abortion
• Any abortion complicated by infection
• Fever, Tenderness
• Ergotrate, Oxytocin
• Antibiotics
• MEDEVAC
• D&C

Operational Obstetrics & Gynecology · Bureau of Medicine and Surgery · 2000 Slide 10
Septic Abortion: Antibiotics
• Clindamycin & Gentamicin IV
• Flagyl & Gentamicin IV
• Cefoxitin IV

Operational Obstetrics & Gynecology · Bureau of Medicine and Surgery · 2000 Slide 11
Unruptured Ectopic Pregnancy
• + HCG
• Unilateral pelvic pain and tenderness
• ±Pelvic mass?
• DD: CL cyst, Appy, PID
• Lie still
• MEDEVAC

Operational Obstetrics & Gynecology · Bureau of Medicine and Surgery · 2000 Slide 12
Ruptured Ectopic: Diagnosis• Pelvic & right shoulder pain• Sudden onset• Shock• Positive pregnancy test• Rebound & Rigidity late• Ultrasound• Culdocentesis

Operational Obstetrics & Gynecology · Bureau of Medicine and Surgery · 2000 Slide 13
Ruptured Ectopic: Treatment
• Surgery
• MEDEVAC
• IVs, oxygen, lie still
• Maintain urine output(Foley)
• MAST suit?

Operational Obstetrics & Gynecology · Bureau of Medicine and Surgery · 2000 Slide 14
Blood Transfusion
• O Negative blood
• Blood collection bags
• Direct Donor to Patient #16 needle 3-4 feet gravity feed 10 minutes
• Have a plan before you need it
Operational Obstetrics & Gynecology · Bureau of Medicine and Surgery · 2000 Slide 15
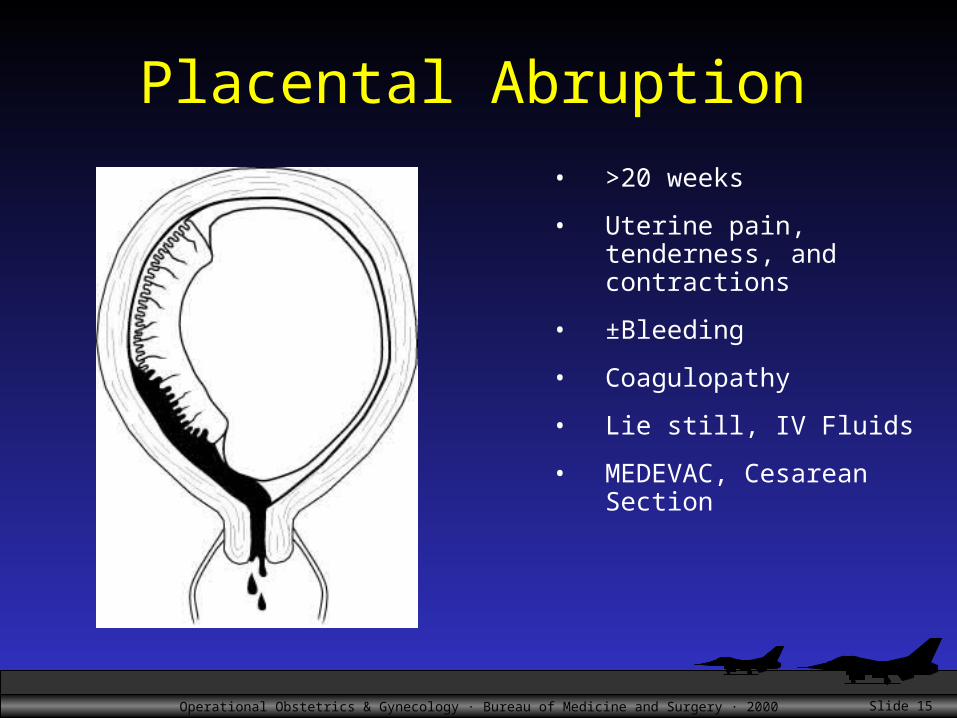
Placental Abruption
• >20 weeks
• Uterine pain, tenderness, and contractions
• ±Bleeding
• Coagulopathy
• Lie still, IV Fluids
• MEDEVAC, Cesarean Section
Operational Obstetrics & Gynecology · Bureau of Medicine and Surgery · 2000 Slide 16
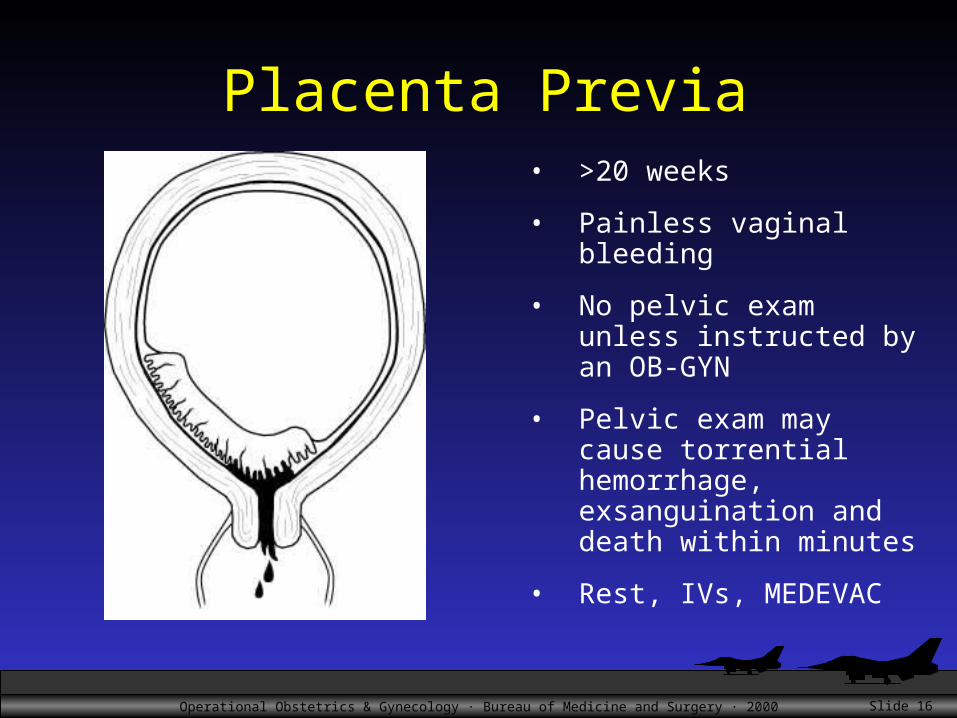
Placenta Previa• >20 weeks
• Painless vaginal bleeding
• No pelvic exam unless instructed by an OB-GYN
• Pelvic exam may cause torrential hemorrhage, exsanguination and death within minutes
• Rest, IVs, MEDEVAC
Operational Obstetrics & Gynecology · Bureau of Medicine and Surgery · 2000 Slide 17
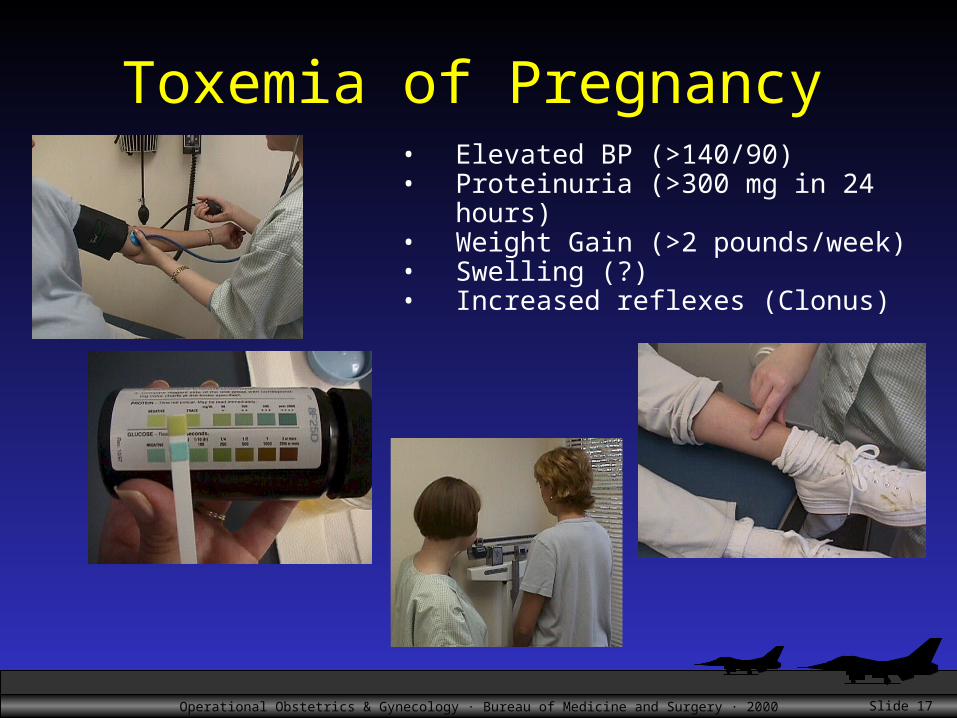
Toxemia of Pregnancy• Elevated BP (>140/90)• Proteinuria (>300 mg in 24 hours)• Weight Gain (>2 pounds/week)• Swelling (?)• Increased reflexes (Clonus)
Operational Obstetrics & Gynecology · Bureau of Medicine and Surgery · 2000 Slide 18
Pre-Eclampsia
• BP, Protein• Stable and unstable• Risk of IUGR• Risk of Abruption• Risk of maternal seizures• Risk of HELLP syndrome
• Hemolysis• Elevated Liver Enzymes• Low Platelets
Naval Hospital Jacksonville

Operational Obstetrics & Gynecology · Bureau of Medicine and Surgery · 2000 Slide 19
Eclampsia
• Siezures• Risk of maternal death• Risk of HELLP syndrome
• Hemolysis• Elevated Liver Enzymes• Low Platelets
Naval Hospital Guam
Operational Obstetrics & Gynecology · Bureau of Medicine and Surgery · 2000 Slide 20
Treatment of Toxemia of Pregnancy
• Delivery is definitive treatment
• If delivery is to be postponed (prematurity), then consider hospitalization for unstable patients
• Magnesium sulfate
• Watch for HELLP syndrome

Operational Obstetrics & Gynecology · Bureau of Medicine and Surgery · 2000 Slide 21