about back pain
DESCRIPTION
medicineTRANSCRIPT
What is back pain?
Introduction
Most of us have back pain at some time in our lives. Bad back pain can make you feel miserable but it usually clears up on its own.
Here we look at low back pain, which is the type most people get.
Key points for people with back pain
• Back pain is common but normally not serious. Most people get better
within six weeks. • Your doctor probably won't be able to tell you exactly what is causing your
pain. In most people, the cause is never found.
• Nonsteroidal anti-inflammatory drugs ( NSAIDs), such as ibuprofen, can help to relieve back pain.
• If your back pain lasts for more than 12 weeks, exercises to strengthen your back can help.
• Staying in bed does more harm than good.
• Staying active can help you get better faster.
Your back
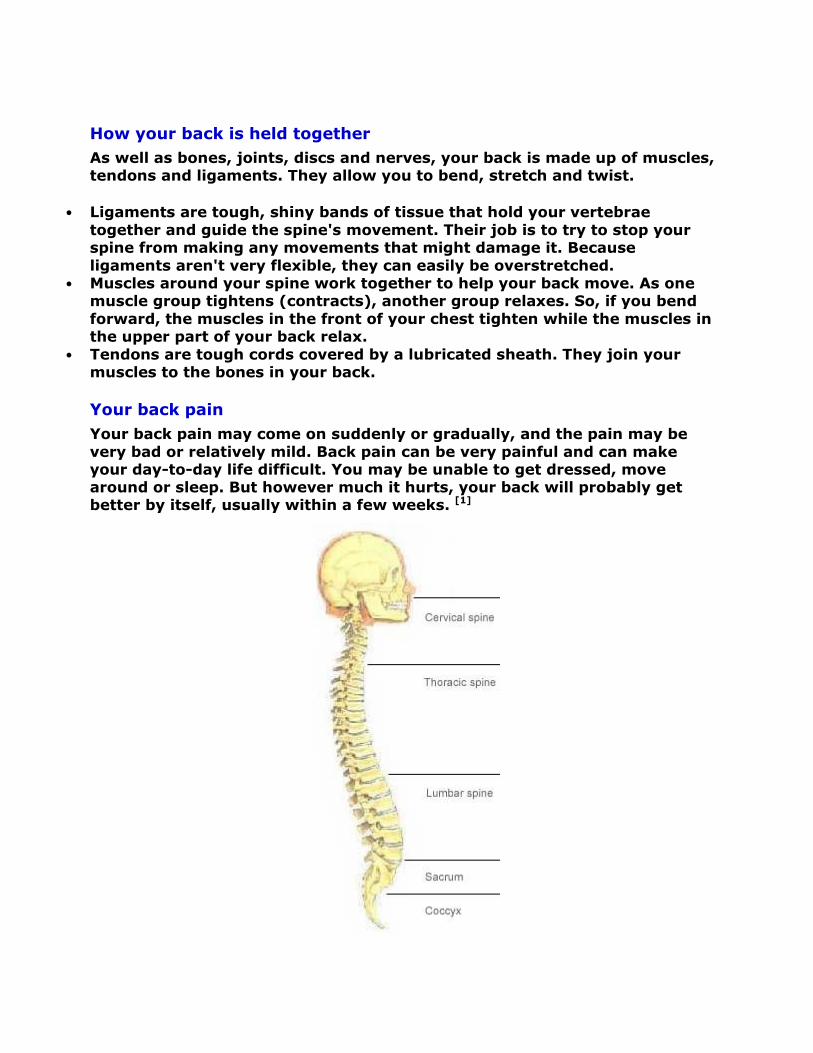
To understand why you get back pain, it helps to know about how your backbone (your spine) works.
• Your spine holds up the weight of your upper body.
• Your spine is like a tower built from 33 small, interlocking bones. These bones are called vertebrae (each individual one is called a vertebra).
• Between each vertebra is a disc. These are round pads of soft, spongy tissue. Each disc has a tough outer ring and a soft, jelly-like centre. The discs cushion the bones in your spine and stop them being damaged when
you jump or run. • Each vertebra is linked to the next one by small joints that lock together.
They are called facet joints. These joints make your spine flexible so you can bend and twist it.
• A bundle of nerves runs down from your brain into the middle of your spine
and goes down to the bottom of it. This is your spinal cord. • Each vertebra has a hole in the middle. The holes make a tunnel all the way
down your back. This is where your spinal cord is. • Nerves from your spinal cord pass through small openings between the
bones in your spine. These nerves branch off to every part of your body.
• Nerves coming out of the base of your spine join up with your sciatic nerves. These are the main nerves in your legs. You have one sciatic nerve
running down each of your legs.
How your back is held together
As well as bones, joints, discs and nerves, your back is made up of muscles, tendons and ligaments. They allow you to bend, stretch and twist.
• Ligaments are tough, shiny bands of tissue that hold your vertebrae
together and guide the spine's movement. Their job is to try to stop your spine from making any movements that might damage it. Because
ligaments aren't very flexible, they can easily be overstretched. • Muscles around your spine work together to help your back move. As one
muscle group tightens (contracts), another group relaxes. So, if you bend
forward, the muscles in the front of your chest tighten while the muscles in the upper part of your back relax.
• Tendons are tough cords covered by a lubricated sheath. They join your muscles to the bones in your back.
Your back pain
Your back pain may come on suddenly or gradually, and the pain may be
very bad or relatively mild. Back pain can be very painful and can make your day-to-day life difficult. You may be unable to get dressed, move around or sleep. But however much it hurts, your back will probably get better by itself, usually within a few weeks. [1]
This is the most common type of back pain. It can either be a sharp pain or a dull pain. It may be mild for some people, but very bad for others. You
may have it all the time or it may come and go. You could find that your back pain gets worse when you do certain things or when you change how you are sitting or standing.
It's not usually possible to know what's causing this type of back pain. It could be a strained muscle in your back. (A strained muscle has been overstretched or torn.) But you'll probably get better without knowing why it happened.
You may have a pain that's just around your legs or a pain in your back as well. The pain could be in your groin, buttock or upper thigh. Sometimes, it can be below your knee. The pain can be dull and achy and it can move
around. It tends to come and go and can vary between being mild to being very bad. You may also get some numbness and tingling.
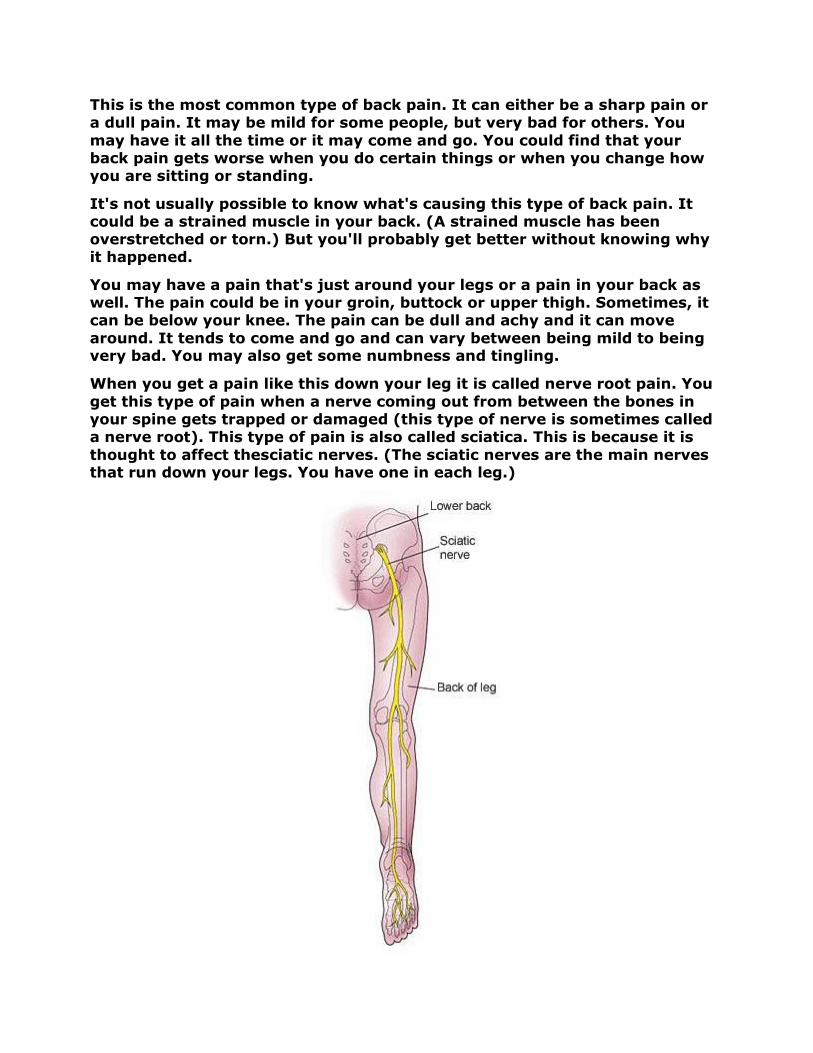
When you get a pain like this down your leg it is called nerve root pain. You
get this type of pain when a nerve coming out from between the bones in your spine gets trapped or damaged (this type of nerve is sometimes called a nerve root). This type of pain is also called sciatica. This is because it is
thought to affect thesciatic nerves. (The sciatic nerves are the main nerves that run down your legs. You have one in each leg.)
Sciatica can be caused by a damaged disc (one of the small cushions that protect the bones in your spine) pressing on a nerve. For more information,
see our pages on Slipped disc. But it can also be caused by other conditions, such as arthritis or diabetes. Or it can happen if nerves in your spine are damaged when you have surgery on your spine.
Your doctor may say your back pain is either acute or chronic. These terms can mean different things to different doctors. But, generally:
• Acute back pain lasts for 12 weeks or less. It is also called short-term back pain.
• Chronic back pain is when you've had pain for more than 12 weeks. It is also called long-term back pain.
If you have had a number of acute bouts of pain, with short periods of relief between them, doctors say that you have recurrent back pain.
What goes wrong?
Your doctor probably won't be able to say exactly what is causing your back
pain. In up to 85 in every 100 people with back pain, no cause is ever found. You may be told you have 'a strain', 'a sprain' or 'lumbago', which are all terms used to describe this type of back pain. [2]
We describe some common causes of back pain below. But please remember that only about 15 in 100 people with back pain will ever find out the exact cause.
Your posture is how you hold different parts of your body when you're
resting or doing things. Poor posture may cause back pain in some people. [3] But there hasn't been much research on this, so we can't be sure
that poor posture causes back pain. You may get poor posture because of a habit, such as always slumping when you sit in a chair or always standing with your shoulders and back hunched. Poor posture can put pressure on
different parts of your back. For example, some muscles may become weaker than others and this means they are more likely to get damaged. If
muscles become weak, it can also affect the position of your spine and this can lead to back pain.
As you get older, the discs in your spine can dry out. If this happens, they can't cushion and protect the bones in your spine (the vertebrae) in the
way they should. The edges of the vertebrae can then wear away, which can cause back pain. The vertebrae may grow small bony bumps called
'spurs'. These spurs can cause pain by pressing on nerves. The pain can travel down your legs, past your knees and into your feet. The general wear and tear of the vertebrae can also cause back pain.
About 8 in 10 men and 6 in 10 women have some wear and tear of the spine
by the time they are 49. By the age of 79, all of us will have some. Your
doctor might call this natural wear and tear of the boneslearn more, see our pages on Osteoarthritis.
Your back pain may be caused by a
muscle. This can happen when you lift something heavy or simply move awkwardly. It can also happen when you use a group of muscles that you're
not used to using. The ligaments that join bones in your back together are not very elastic, so they can be pulled easily.
You can get back pain when a disc in your back is damaged. If a disc tears,
then its jelly-like centre bulges through the tear and maynerves coming out of your spinal cord
may become inflamedand sore. Doctors call this amay hear it called aprolapsedslipped disc because that's the name most people know.
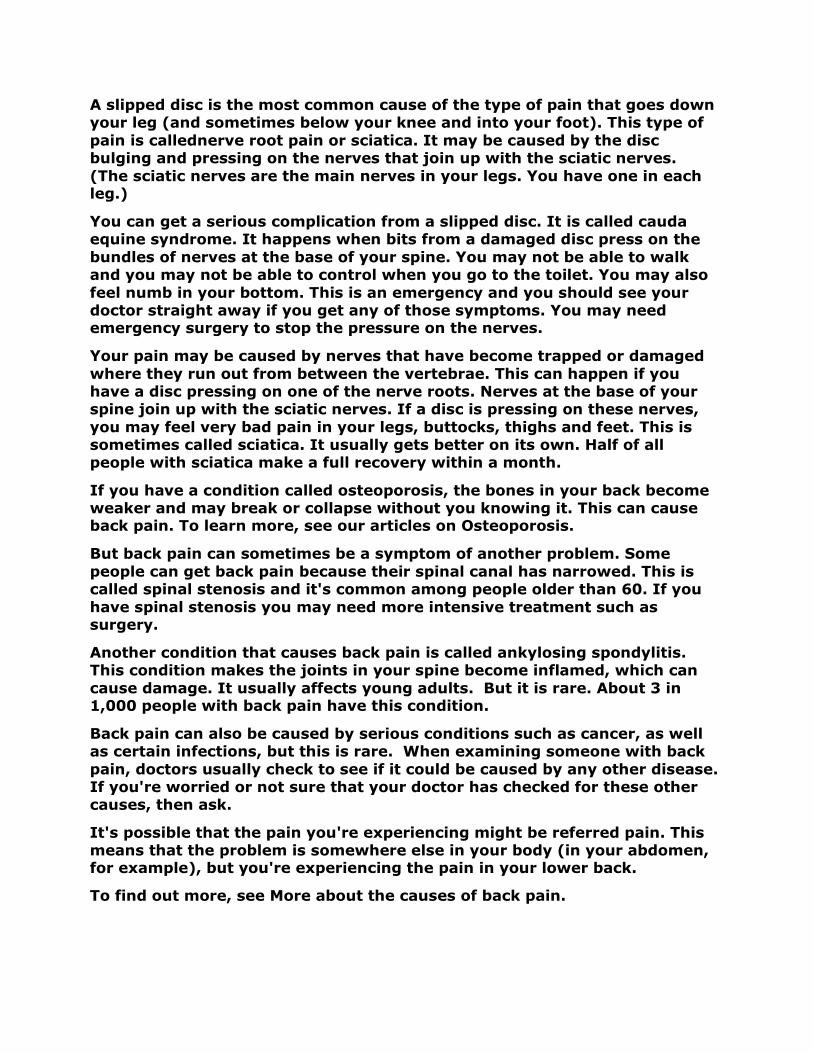
Poor posture or strenuous activity, such as heavy lifting, can damage discs.
Sitting down for long periods of time puts more pressure on the discs and vertebrae in the lower part of your back than standing does. This is because your lower back has to support the whole weight of your upper body when you are sitting, with no help from
Bear in mind that a slipped disc is not a common cause of back pain. Only about 4 in 100 people with back pain caused by a physical problem have a slipped disc.
doctor might call this natural wear and tear of the bones osteoarthritislearn more, see our pages on Osteoarthritis.
pain may be caused by a strained (stretched or torn)
This can happen when you lift something heavy or simply move happen when you use a group of muscles that you're
not used to using. The ligaments that join bones in your back together are not very elastic, so they can be pulled easily.
You can get back pain when a disc in your back is damaged. If a disc tears,
like centre bulges through the tear and may press on the nerves coming out of your spinal cord. Tissues around the damaged disc
nd sore. Doctors call this a herniated discprolapsed or ruptured disc. We have used the term
slipped disc because that's the name most people know.
Poor posture or strenuous activity, such as heavy lifting, can damage discs.
tting down for long periods of time puts more pressure on the discs and vertebrae in the lower part of your back than standing does. This is because your lower back has to support the whole weight of your upper body when you are sitting, with no help from your legs.
Bear in mind that a slipped disc is not a common cause of back pain. Only with back pain caused by a physical problem have a
osteoarthritis. To
(stretched or torn) ligament or
This can happen when you lift something heavy or simply move happen when you use a group of muscles that you're
not used to using. The ligaments that join bones in your back together are
You can get back pain when a disc in your back is damaged. If a disc tears,
press on the . Tissues around the damaged disc
herniated disc, or you . We have used the term
Poor posture or strenuous activity, such as heavy lifting, can damage discs.
tting down for long periods of time puts more pressure on the discs and vertebrae in the lower part of your back than standing does. This is because your lower back has to support the whole weight of your upper body when
Bear in mind that a slipped disc is not a common cause of back pain. Only with back pain caused by a physical problem have a
A slipped disc is the most common cause of the type of pain that goes down your leg (and sometimes below your knee and into your foot). This type of
pain is callednerve root pain or sciatica. It may be caused by the disc bulging and pressing on the nerves that join up with the sciatic nerves.
(The sciatic nerves are the main nerves in your legs. You have one in each leg.)
You can get a serious complication from a slipped disc. It is called cauda equine syndrome. It happens when bits from a damaged disc press on the
bundles of nerves at the base of your spine. You may not be able to walk and you may not be able to control when you go to the toilet. You may also
feel numb in your bottom. This is an emergency and you should see your doctor straight away if you get any of those symptoms. You may need emergency surgery to stop the pressure on the nerves.
Your pain may be caused by nerves that have become trapped or damaged
where they run out from between the vertebrae. This can happen if you have a disc pressing on one of the nerve roots. Nerves at the base of your spine join up with the sciatic nerves. If a disc is pressing on these nerves,
you may feel very bad pain in your legs, buttocks, thighs and feet. This is sometimes called sciatica. It usually gets better on its own. Half of all people with sciatica make a full recovery within a month.
If you have a condition called osteoporosis, the bones in your back become weaker and may break or collapse without you knowing it. This can cause back pain. To learn more, see our articles on Osteoporosis.
But back pain can sometimes be a symptom of another problem. Some
people can get back pain because their spinal canal has narrowed. This is called spinal stenosis and it's common among people older than 60. If you
have spinal stenosis you may need more intensive treatment such as surgery.
Another condition that causes back pain is called ankylosing spondylitis. This condition makes the joints in your spine become inflamed, which can
cause damage. It usually affects young adults. But it is rare. About 3 in 1,000 people with back pain have this condition.
Back pain can also be caused by serious conditions such as cancer, as well as certain infections, but this is rare. When examining someone with back
pain, doctors usually check to see if it could be caused by any other disease. If you're worried or not sure that your doctor has checked for these other causes, then ask.
It's possible that the pain you're experiencing might be referred pain. This means that the problem is somewhere else in your body (in your abdomen, for example), but you're experiencing the pain in your lower back.
To find out more, see More about the causes of back pain.
Why me?
Doctors don't know why some people are more likely to get back pain than
others. Things that increase your chances of getting back pain are called risk factors.
Here are the main risk factors for low back pain:
• Getting older. • Doing heavy physical work, especially if it involves heavy lifting, twisting
and working with vibrating machinery. This can put a lot of strain on your back.
• Staying in one position for a long time. For example, if you have a job that
involves a lot of driving, you could be at risk. • Being obese (being very overweight). Carrying extra weight around can
strain your back. If you want to find out whether you are overweight, you can work out your body mass index (BMI) using our calculator. Your body mass index compares your height with your weight.
• Suffering from stress at work or from mental health problems such as anxiety or depression. These can put you at risk of back pain.
Glossary
NSAIDs
NSAID stands for nonsteroidal anti-inflammatory drug. NSAIDs help with
pain, inflammation and fever. They are called 'nonsteroidal' because they don't contain any steroids. Aspirin and ibuprofen are both NSAIDs.
arthritis
Arthritis is when your joints become inflamed, making them stiff and painful. There are different kinds of arthritis. Osteoarthritis is the most
common type. It happens when the cartilage at the end of your bones becomes damaged and then starts to grow abnormally. Rheumatoid
arthritis happens because your immune system attacks the lining of your joints.
diabetes
Diabetes is a condition that causes too much sugar (glucose) to circulate in the blood. It happens when the body stops making a hormone called insulin (type 1 diabetes) or when insulin stops working (type 2 diabetes).
ligament
A ligament is a strong piece of tissue that connects one bone to another.
For example, ligaments in your ankle connect the bones of your leg to the bones of your heel.
inflammation
Inflammation is when your skin or some other part of your body becomes red, swollen, hot and sore. Inflammation happens because your body is
trying to protect you from germs, from something that's in your body and could harm you (like a splinter) or from things that cause allergies (these
things are called allergens). Inflammation is one of the ways in which your body heals an infection or an injury.
Causes of lower back pain
Back pain causes
Back pain is a symptom. Pain arising from other organs may be felt in the
back. This is called referred pain. Many intra-abdominal disorders – such as
appendicitis, aneurysms, kidney diseases, bladder infections, pelvic infections and ovarian disorders, among others – can cause pain referred to the back. Your doctor will consider this when evaluating your pain.
• Nerve root syndromes are those that produce symptoms of nerve
impingement (a nerve is touched), often due to a herniation (or bulging) of the disc between the lower back bones. Sciatica is an example of nerve root
impingement. Impingement pain tends to be sharp, in one spot and associated with numbness in the area of the leg that the affected nerve
supplies. o Herniated, or slipped, discs are produced as the spinal discs degenerate or
grow thinner. The jelly-like central portion of the disc bulges out of the
central cavity and pushes against a nerve root. Intervertebral discs begin to degenerate by the third decade of life. Slipped discs are found in one-third
of adults older than 20. However only 3% of these produce symptoms of nerve impingement.
o Spinal stenosis occurs as intervertebral discs lose moisture and volume
with age, which decreases the disc spaces. Even minor trauma under these circumstances can cause inflammation and nerve root impingement, which
can produce classic sciatica without disc rupture. o Spinal degeneration is caused by alterations in the disc that progress to
degeneration. This, coupled with disease in joints of the lower back, causes
spinal canal narrowing. These changes in the disc and the joints produce symptoms and can be seen on an X-ray. A person with spinal degeneration
may have morning stiffness or pain while standing for a long time or walking even short distances.
o Cauda equina syndrome is a medical emergency. Disc material expands into
the spinal canal, which compresses the nerves. A person experiences pain, possible loss of sensation and bowel or bladder dysfunction. This can
include inability to control urination, causing incontinence, or the inability to begin urination.
• Musculoskeletal pain syndromes that produce lower back pain include
myofascial pain syndromes and fibromyalgia.

o Myofascial pain is characterised by pain and tenderness over localised areas (trigger points), loss of range of motion in the involved muscle groups and
pain radiating in a characteristic distribution but restricted to a peripheral nerve. Relief of pain is often reported when the involved muscle group is
stretched. o Fibromyalgia is a poorly understood condition defined as causing pain and
tenderness on 11 of 18 ‘tender points’ when touched, one of which is the
lower back area, as described by NHS guidelines. Generalised stiffness, fatigue and muscle ache are reported.
• Other skeletal causes of lower back pain include osteomyelitis or sacroiliitis (infections of the bones of the spine). This pain is usually worse at night and is worse when sitting or standing for a long time.
• Tumours, possibly cancerous, can be a source of skeletal pain.
How can I prevent back pain?
In learning how to prevent back pain, keep your posture in mind. The most
important preventive measure for lower back pain is maintaining a good posture when standing and sitting.
First, analyse your posture by standing with your heels against a wall. Your calves, buttocks, shoulders, and the back of your head should touch the wall. You should be able to slip your hand behind the small of your back.
Now step forwards and stand normally. If your posture changes, correct it. If you stand for long periods of time at work, wear flat shoes with good
arch support and get a box or step about 15 centimetres high to rest one foot on from time to time.
Your sitting posture may be even more important. A good chair bottom supports your hips comfortably but doesn't touch the backs of your knees.
Your chair back should be set at an angle of about 10 degrees and should cradle the small of your back comfortably. If necessary, use a wedge-
shaped cushion or lumbar pad. Your feet should rest flat on the floor. Your forearms should rest on your desk or work surface with your elbows almost at a right angle.
When you have to lift heavy objects, don't bend at the waist. Squat with
your legs and keep your back upright as you grasp the object and stand upright again. Let your legs do the lifting, not your back. Back braces don't actually help protect your back other than reminding you to not bend with
your back. Finally you can ask a physiotherapist about back-strengthening exercises. You might also check with your local gym or health club for back-
strengthening classes. These stretching and strengthening exercises can help chronic back pain and prevent future episodes. Also, some forms of
yoga and t'ai chi can help you learn proper posture and improve strength, balance, and flexibility.
Symptoms & types
Back pain symptoms can range in intensity from mild to severe. Learn the signs to watch out for.
Symptoms Upper, middle, and lower back pain symptoms
What are the symptoms of back pain?
Most people have experienced back pain at some point in their life. The
causes of back pain are numerous, and some are self-inflicted due to a
lifetime of bad habits. Other back pain causes include accidents, muscle strains and sport injuries. Although the causes may be different, the symptoms are usually the same.
The symptoms for back pain are:
• Persistent aching or stiffness anywhere along your spine, from the base of
the neck to the hips. • Sharp localised pain in the neck, upper back or lower back – especially after
lifting heavy objects or engaging in other strenuous activity. • Chronic ache in the middle or lower back, especially after sitting or standing
for extended periods. • Back pain that radiates from the lower back to the buttocks, down the back
of the thigh and into the calf and toes.
• Inability to stand straight without having severe muscle spasms in the lower back.
Call your doctor about back pain if:
• You feel numbness, tingling or loss of control in your arms or legs. This may
signal damage to the spinal cord. • The pain in your back extends downwards along the back of the leg. You
may have sciatica. • The pain increases when you cough or bend forwards at the waist. This can
be the sign of a herniated (slipped) disc. • The pain is accompanied by fever, burning sensation during urination or
strong-smelling urine. You may have a bacterial urinary tract infection.
• You have urine or fecal incontinence. • You have dull pain in one area of your spine when lying in or getting out of
bed. If you are over 50 years old, you may have osteoarthritis.
Warning signs
10 questions to ask your doctor about back pain
When you're experiencing back pain, going to the doctor can be
intimidating. You might feel rushed and forget to ask some important questions about your back pain. It's always a good idea to know what to ask beforehand and to take notes during your visit to the doctor. Some of
the questions below about back pain and its treatment may be worth asking. Print out this page and take it with you to your next appointment.
1. What's causing my back pain? 2. Are there any other symptoms I should be aware of that could indicate a
more serious condition?
3. Are there activities I should temporarily or permanently avoid to ease back pain?
4. Could my work station be affecting my back pain? 5. How much bed rest should I get while I'm suffering from back pain? 6. What treatment options should I consider for my back pain? 7. How long should I take medication or do special exercises for back pain? 8. Are there alternative therapies that I should consider? 9. How long will it take before I notice results, less back pain. 10. What can I do to prevent back pain from persisting or returning?
Chronic back pain? Sudden back pain? You need answers to these 10 questions.
Complications
Cauda equina syndrome overview
The spinal cord extends from the brain down through the spinal canal inside
the vertebral column. The spinal cord is surrounded by dural sacs, which are extensions of the brain-covering membranes. The brain-covering membranes
are called dura mater, arachnoid mater (which contains cerebrospinal fluid) and pia mater. Nerves that branch off the spinal cord (also called nerve roots) are an extension of the spinal cord and are responsible for sending
signals to and from the muscles and other structures throughout the body. These signals allow the brain to interpret information from the body
including pain, touch and sense of position. Outgoing signals allow the brain to control actions of the organs and muscle movements.
The spinal cord ends near the first lumbar vertebra in the lower back, forming the conus medullaris. The fibrous extension of the spinal cord is the
filum terminale. The bundle of nerve roots below the conus medullaris is named the cauda equina.
Compression or inflammation of the nerve roots can cause symptoms of pain, altered reflexes, decreased strength and decreased sensation.
Although these symptoms can become severe, and in some cases disabling, most are self-limiting and respond to conservative care.
This syndrome may require emergency surgery to avoid permanent damage
to bowel and bladder control or even paralysis.
Chronic back pain and sleep
When chronic back pain disturbs your sleep night after night, you might
despair of ever getting a good night's sleep. However, experts say that with proper treatment, the chances are very good that you can get relief from chronic back pain and enjoy normal sleep.
Why sleep is important when you have chronic back pain
The inability to get a good night's sleep hurts – literally. Chronic back pain
prevents you from getting a good night's sleep and you wake up in even more pain.
Pain interferes with the normal cycles of light and deep sleep you need in order to wake up refreshed. This disruption is called ‘alpha delta sleep
disorder’. When back pain prevents you getting adequate deep, or delta sleep, you wake up in the morning tired and sore.
Causes of sleep problems
The chronic back pain itself may cause a sleep problem. Here are some other causes:
• Anxiety and depression can result in the inability to fall asleep or stay
asleep, which will aggravate pain. Anxiety and depression increase a person’s sensitivity and awareness of pain, and the lack of proper sleep
aggravates both the pain and any depression with anxiety. • Breathing-related sleep disorders associated with obesity – such as
obstructive sleep apneoa – can further aggravate pain by causing you to wake frequently throughout the night and by interfering with normal sleep patterns.
• Limb movement disorders – such as restless leg syndrome – may further disrupt the normal sleep pattern. These conditions may be related to
anxiety and depression as well as stress. • Self-medicating with alcohol may help you fall asleep, but you'll probably
wake up tired, grumpy and in pain.
• Some prescription medications can impair the quality of your sleep.
Medications that improve sleep and reduce chronic back pain
Some medications can help you sleep while helping with your chronic back
pain. However some of these medicines have side effects and the potential
for addiction. They should be used as part of a more comprehensive and widespread programme of pain management.
• Newer sedatives including zolpidem tartrate do not have a negative effect
on your sleep. • Over-the-counter pain relievers such as aspirin, paracetamol or ibuprofen
can be effective for short-term use. Use them only as directed and let your doctor know what you are taking.
• Prescription medicines for severe back pain include antidepressants such as doxepin and amitriptyline or a muscle relaxant such as diazepam and baclofen.
Medication should not be used for longer than two to three months except
in rare cases. Long-term use can result in dependence on the drug. The goal of medication should be to help you develop a more normal sleep pattern.
Lifestyle changes for chronic back pain and sleep problems
Here are some tips for getting a good night's sleep with chronic back pain:
Painful, sleepless nights can be the norm for people with chronic pain. Find out how to fight back and get your sleep.
Avoid stress. Stress is the major cause of insomnia. It is also associated with chronic back pain.
Limit or eliminate caffeine. Even moderate caffeine use can cause insomnia and sleep disturbances.
Avoid eating heavily before bedtime. A heavy meal can cause acid reflux (heartburn) and keep you awake. However, though there are no studies to show that it can induce sleep, have a mug of warm milk if it comforts you. The placebo effect can be very powerful.
Don't self-medicate with alcohol. It's worth restating that alcohol impairs the quality of sleep.
Do some soothing exercises. Do these three exercises for several minutes while lying in bed unless it hurts to do them:
• Bring both knees towards your chest (as if doing a bomb in a swimming
pool). • Alternate bringing first one knee, then the other, towards your chest.
• Bring both knees to your chest and twist from one side to the other.
Choose a comfortable mattress and pillow. You don't have to spend vast amounts on a mattress. Studies show that a medium-firm mattress is best
for most people. The key is to use whatever is comfortable for you. If your mattress is too firm, you can add an ‘egg crate’ foam mattress pad. Pillows come in all shapes and sizes. Find the one that's right for you.

Sleep in a comfortable position. Do not sleep on your stomach, as it causes you to arch your back and bending backwards often worsens chronic back
pain. To break the habit wear a sleep shirt with a pocket in front and put a tennis ball in it. For most people the best position is to lie on your side in a
foetal position with a pillow between your legs. If you prefer to lie on your back, put a pillow under your knees.
Establish a bedtime routine. Try to go to bed at the same time each night. Follow a routine such as setting the alarm, putting on your pyjamas and brushing your teeth. Do not read, work or watch TV in bed.
Get rid of chronic back pain
While the best way to get a good night's sleep is to get rid of chronic back
pain, this is not always possible. Other factors such as stress, anxiety and depression that affect sleep and pain may need attention and treatment.
Many people put up with pain when most back pain can be helped and treated successfully – usually without surgery. Don't give up on finding a treatment that can work for you.
Diagnosis & tests
You know your back hurts, but you may not know why, or what to do about
it. Find out how doctors diagnose back problems and what tests may be involved.
Diagnosis
What kind of back problem do you have?
How do I know what kind of back problem I have?
Unless you are totally immobilised from a back injury, your doctor will
probably test your range of motion and nerve function and touch your body to locate the area of discomfort.
Blood and urine tests will make sure the pain is not due to an infection or
other systemic problems. X-rays are useful in pinpointing broken bones or other skeletal defects.
They can sometimes help locate problems in connective tissue. To analyse soft-tissue damage computed tomography (CT) or magnetic resonance
imaging (MRI) scans may be needed. X-rays and imaging studies are generally used only for examining direct trauma to the back, back pain with fever or nerve problems such as extremity weakness or numbness. To
determine possible nerve or muscle damage an electromyogram (EMG) can be useful.

Find out how doctors diagnose back problems.
Exams and tests
Medical history
• Because many different conditions may cause back pain, a thorough
medical history will be recorded as part of the examination. Some of the questions you are asked may not seem pertinent to you but are very important to your doctor in determining the source of your pain.
• Your doctor will first ask you many questions regarding the onset of the pain. (Were you lifting a heavy object and felt an immediate pain? Did the
pain come on gradually?) He or she will want to know what makes the pain better or worse. The doctor will ask you many questions referring to the ‘red flag’ symptoms. He or she will ask if you have had the pain before.
Your doctor will ask about recent illnesses and associated symptoms such as coughs, fevers, urinary difficulties or stomach illnesses. In females the
doctor will want to know about vaginal bleeding, cramping or discharge. Pain from the pelvis, in these cases, is frequently felt in the back.
Physical examination
• To ensure a thorough examination you will be asked to put on a gown. The
doctor will watch for signs of nerve damage while you walk on your heels, toes and soles of the feet. Reflexes are usually tested using a reflex hammer. This is usually done at the knee and behind the ankle. As you lie
flat on your back, one leg at a time is elevated, both with and without the assistance of the doctor. This is done to test the nerves, muscle strength
and assess the presence of tension on the sciatic nerve. Sensation is usually tested using a pin, paperclip, broken tongue depressor or other sharp
object to assess any loss of sensation in your legs. o Depending on what the doctor suspects is wrong with you, he or she may
perform an abdominal examination, a pelvic examination or a rectal
examination. These exams look for diseases that can cause pain referred to your back. The lowest nerves in your spinal cord serve the sensory area and
muscles of the rectum, and damage to these nerves can result in inability to control urination and defecation. This makes a rectal examination essential to make sure that you do not have nerve damage in this area of your body.
Blood and urine tests, stool samples, vaginal swabs
• If your doctor suspects that pain is caused by a problem in the abdomen
such as a kidney or uterine infection he or she may organise a variety of blood, urine, stool or swab samples to exclude these problems.
Imaging
• Doctors can use several tests to ‘look inside you’ to get an idea of what might be causing the back pain. However no single test is perfect in that it
can identify the absence or presence of disease 100% of the time. • The medical literature is very clear: if there are no red flags, there is little
to be gained in imaging acute back pain. Because about 90% of people improve within 30 days of the onset of their back pain, most doctors will
not order tests in the routine evaluation of acute, uncomplicated back pain. • Plain X-rays are generally not considered useful in the evaluation of back
pain, particularly in the first 30 days. In the absence of red flags their use is
discouraged. They are generally used if there is significant trauma, mild trauma in those older than 50, people with osteoporosis and those with
prolonged steroid use. If you do not fall into one of these groups, do not expect an X-ray to be taken.
• Ultrasound of the abdomen organs may have a role in excluding disease
causing pain referred to the back such as kidney stones or infection. • Myelogram is an X-ray study in which a radio-opaque dye is injected
directly into the spinal canal. Its use has decreased dramatically since MRI scanning. This test is now usually done in conjunction with a CT scan, and even then only in special situations when surgery is being planned.
• Magnetic resonance imaging (MRI) scans are a highly sophisticated test and, as such, are very expensive. The test does not use X-rays but very
strong magnets to produce images. Their routine use is discouraged in acute back pain unless a condition is present that may require immediate surgery such as with cauda equina syndrome or when red flags are present
and suggest infection of the spinal canal, bone infection, tumour or fracture.
o MRI may also be considered after one month of symptoms to rule out more serious underlying problems.
o MRIs are not without problems. Bulging of the discs is noted on up to 40%
of MRIs performed on people without back pain. Other studies have shown that MRIs fail to diagnose up to 20% of ruptured discs that are found
during surgery.
Nerve tests
• Electromyogram, or EMG, is a test that involves the placement of very small needles into the muscles. Electrical activity is monitored. Its use is usually
reserved for more chronic pain and to predict the level of nerve root damage. The test is also able to help the doctor distinguish between nerve
root disease and muscle disease.
Treatment & care
Back pain may be constant or sudden, mild or debilitating. Get the facts on back pain treatments, including medication, exercise, and chiropractic care.

Treatment
How do I know what is causing my back pain?
To diagnose back pain – unless you are totally immobilised from a back
injury – your doctor will probably test your range of motion and nerve
function, and touch your body to locate the area of discomfort. Blood and urine tests may be necessary to make sure that the back pain is not caused by an infection or other more widespread medical problems.
X-rays are useful in pinpointing broken bones or other skeletal defects.
They can sometimes help locate problems in connective tissue. To analyse soft-tissue damage computed tomography (CT) or magnetic resonance
imaging (MRI) scans may be needed, and your doctor will usually refer you to a specialist to have these done. X-rays and imaging studies are generally used only for examining direct trauma to the back, back pain with fever or
nerve problems such as extremity weakness or numbness. To determine possible nerve or muscle damage an electromyogram (EMG) can be useful.
X-rays and magnetic resonance imaging (MRI) studies have limitations and
must be interpreted with caution. Back pain may be incorrectly attributed to non-specific and unrelated abnormalities on the images. Ordinary and expected wear and tear in the spine and discs may be mistaken as the
cause of a person’s back pain. Similarly, plain X-rays are not usually helpful in cases of chronic back pain without a significant injury or loss of sensation and movement in the extremities.
Most back pain originates in the soft tissues of the back and not the actual spine. Because most back pain is related to the muscles of the back, the specific cause of most back pain cannot be determined by imaging studies.
What are the treatments for back pain?
Only after determining the cause of the problem can a doctor begin treating back pain.
Rest: The basic treatment for relieving acute back pain from strain or minor injury is a limited period of rest for 24 to 72 hours. An ice pack can be helpful, as can aspirin or another nonsteroidal anti-inflammatory drug
(NSAID) to reduce pain and inflammation. After the inflammation subsides, applying heat can soothe muscles and connective tissue.
Long-term bed rest is no longer considered necessary for most cases of back pain – it can actually be harmful, slowing recovery and potentially
causing new problems. In most cases you will be expected to start normal, non-strenuous activity (such as walking) within 24 to 72 hours. After that
you should begin controlled exercise or physiotherapy. Physiotherapy treatments may employ massage, ultrasound, whirlpool baths, controlled application of heat and individually tailored exercise programmes to help
you regain full use of your back. Strengthening both the abdominal and back muscles helps stabilise the spine. You can prevent further back injury
by learning – and doing – gentle stretching exercises and proper lifting
techniques, as well as maintaining good posture.
Medication: If back pain keeps you from carrying out normal daily activities, your doctor can help by recommending or prescribing pain medications.
Over-the-counter painkillers such as aspirin, paracetamol, ibuprofen or low-dose codeine phophate and paracetamol combinations can be helpful. Your doctor may prescribe prescription strength anti-inflammatories/pain
medicines or may prefer to prescribe a combination of opioid and paracetamol based medications such as higher-dose codeine phosphate and
paracetamol combinations or tramadol (with our without paracetamol). Some doctors also prescribe muscle relaxants. However the main effect of these medications is on the brain, not the muscles, and they often cause drowsiness.
Sometimes, especially in neuropathic back pain, low doses of tricyclic antidepressant medication such as amitriptyline may be added as a pain management addition, though it is not licensed for this use.
Opioids can be addictive when used on a long-term basis and should be
avoided unless a definite cause of back pain related to an injury or a disease can be established. Opioids reduce pain by changing the function of the nervous system and changing negative moods and emotions.
If your doctor isn't able to help you control the pain, he or she may refer you to a back specialist or a pain specialist. Sometimes these doctors will use injections of steroids or anaesthetics to help control the pain or for diagnosis.
The use of injections and procedures in and around the spine is very limited as such treatments provide only temporary relief. The various injection
procedures are costly and have potential side effects, which must be taken into consideration. Often a pain specialist or back specialist will employ rehabilitation and counselling by non-medical personnel such as therapists, counsellors, and patient educators.
TENS: Some doctors advocate using a transcutaneous electrical nerve stimulator (TENS). Electrodes taped to the body carry a mild electric current that helps relieve pain. After appropriate training, patients can use
a TENS on their own to help reduce pain while they recover from strained or moderately injured backs. The value of TENS is still debated as there is not yet a large body of evidence to suggest it is effective.
Surgery: Surgery for non-specific back pain is a last resort. Spinal problems are unlikely to be the cause of chronic non-specific back pain if there is no loss of movement and sensation or there are no other findings such as loss
of muscle bulk and reflexes. In cases where the pain spreads into the extremities and imaging studies reveal compression or damage to nerve
tissue in the spine, surgery remains a consideration if loss of function as well as pain continues after a trial of conservative treatment with medications and activity modification, including a home exercise programme and physiotherapy.

In cases of persistent pain from extreme nerve damage, rhizotomy – surgically severing a nerve – may be necessary to stop the transmission of
pain to the brain. Rhizotomy can correct the symptoms caused by friction between the surfaces in a spinal joint, but it doesn't address other problems such as slipped discs.
Physical therapies including physiotherapy, osteopathy and chiropractic care: Therapists also have a role in the treatment of back pain. The NHS recognises spinal manipulation by physiotherapists, chiropractors and
osteopaths as effective for acute lower back pain, although treatment is not always available through the NHS. Its effectiveness for treating chronic
back pain is less well established. Some researchers suggest that early chiropractic adjustments for acute back pain may prevent chronic problems from developing. Other doctors warn against some chiropractic
manipulations, particularly those that involve rapid twisting of the neck. Physical therapist care can be considered a form of conservative care for
the treatment of acute and chronic back pain as it is not invasive and does not employ prescription medications.
Osteopathic treatment is likely to combine non-prescription drug therapy with spinal manipulation or traction, followed by physical therapy and exercise.
Acupuncture: Acupuncture may bring moderate to complete pain relief for many people with back pain. It can be used alone or as part of a comprehensive treatment plan that includes medications and other body
work. Clinical achievements, along with positive research results, prompted the National Institutes of Health (NIH) in the US to declare acupuncture a
reasonable treatment option for people that have lower back pain. Similarly the NHS website states that studies have shown acupuncture to be an effective means of easing the symptoms of chronic back pain and has
approved it as a cost-effective treatment, according to the May 2009 guidelines from the National Institute for Health and Clinical Excellence
(NICE). Like many treatments, acupuncture usually provides temporary relief from pain symptoms.
CBT: If you consult a psychotherapist for cognitive behavioural therapy (CBT), your treatment may include stress management, behavioural
adaptation, education and relaxation techniques. CBT can lessen the intensity of back pain, alter perceptions about levels of pain and disability,
and even lift depression. According to recent NICE guidelines, CBT is useful for relieving lower back pain.
Other comprehensive behavioural programmes have shown similar success, with participants able to lessen the amount of medication they needed
while improving their outlook and pain-related behaviour. Biofeedback: If lower back pain is related to muscle tension or spasm,
biofeedback can be effective for lessening pain intensity, decreasing medicine use and improving quality of life. Biofeedback may help you train

your muscles to respond better to stress or movement.
Exercise methods: The Alexander Technique, Pilates and the Feldendkrais Method are all specialised forms of body work that can help you learn to
move in a more coordinated, flexible and graceful manner. They may help reduce pain and can relieve stress. Some of the postures of yoga may help diminish lower back pain, improve flexibility, strength and sense of balance.
Yoga is good for stress reduction and can help with the psychological aspects of pain. These non-medical and conservative therapies empower
patients. This empowerment with a self-help plan may reduce feelings of helplessness and pain separate from any effect on body tissues and structures.
Aquatic therapy: Aquatic therapy and exercise can also improve flexibility
and decrease pain for those with chronic lower back problems. The unique properties of water make it an especially safe environment for exercising a sore back: it provides gentle resistance, comfort and relaxation. Fear of
pain associated with movement is a major limiting factor for rehabilitation and exercise therapy. The support and heat of the water enables a person to gradually introduce daily exercise into their treatment.
In many instances knowing the cause of the pain and fixing the problem is not possible, and patients functioning in spite of the pain rather than not functioning because of the pain is the primary goal of pain management treatment.
Chiropractic care for back pain
Among people seeking back pain relief alternatives, most choose
chiropractic treatment. Many patients are seeking relief from various
causes of back pain including accidents, sport injuries and muscle strains. Other complaints include pain in the neck, arms and legs, and headaches.
What is chiropractic care?
Chiropractors use hands-on spinal manipulation and other complementary
treatments, the theory being that proper alignment of the body's
musculoskeletal structure, particularly the spine, will enable the body to heal itself without surgery or medication. Manipulation is used to restore mobility to joints restricted by tissue injury caused by a traumatic event
such as falling or by repetitive stress such as sitting without proper back support.
Chiropractic is primarily used as a pain relief alternative for muscles, joints,
bones and connective tissue such as cartilage, ligaments and tendons. It is sometimes used in conjunction with conventional medical treatment. A chiropractor in the UK must take and pass a course accredited by the General Chiropractic Council (GCC) and then be registered with the GCC.
What does chiropractic care for back pain involve?
A chiropractor first records your medical history and then performs a
physical examination. He or she may use lab tests or diagnostic imaging to determine if treatment is appropriate for your back pain.
The treatment plan may involve one or more manual adjustments in which the chiropractor manipulates the joints, using a controlled sudden force to improve range and quality of motion. Many chiropractors also incorporate
nutritional counselling and exercise/rehabilitation into the treatment plan. The goals of chiropractic care include the restoration of function and prevention of injury in addition to back pain relief.
What are the benefits and risks of chiropractic care?
Spinal manipulation and chiropractic care is considered a safe effective
treatment for acute lower back pain – the type of sudden injury that results from moving furniture or from a sudden jarring in sport. Acute back pain,
which is more common than chronic pain, lasts no more than six weeks and typically gets better on its own.
Research has also shown chiropractic to be helpful in treating neck pain and headaches. Osteoarthritis and fibromyalgia also respond to the
moderate pressure used by both chiropractors and practitioners of deep tissue massage.
Studies have not confirmed the effectiveness of prolotherapy or
sclerotherapy for pain relief, used by some chiropractors, osteopaths and medical doctors to treat chronic back pain – the type of pain that may come on suddenly or gradually and lasts for more than three months. The therapy involves injections to strengthen loosely connected tendons and ligaments.
People who have osteoporosis, spinal cord compression or inflammatory arthritis, or who take blood-thinning medications, should not undergo spinal manipulation.
All treatment is based on an accurate diagnosis of your back pain. The
chiropractor should be well informed regarding your medical history including ongoing medical conditions, current medications,
traumatic/surgical history and lifestyle factors. Although rare, there have been cases in which treatment worsened a slipped disc, or neck manipulation resulted in a stroke or spinal cord injury. To be safe always
inform your doctor whenever you use chiropractic or other pain relief alternatives.
Pain management: Spinal cord stimulation
When other pain treatments have failed, spinal cord stimulation may be an
option.
Spinal cord stimulation is a procedure that delivers low-level electrical
signals to the spinal cord or to specific nerves to block pain signals from reaching the brain.
What happens during the procedure?
In the procedure, a device that delivers the electrical signals is implanted in
the body, either surgically or percutaneously (through the skin). The
patient may turn the current off and on or adjust the intensity of the signals. Most people describe the feelings from the simulator as being pleasant and tingling.
Two kinds of spinal cord stimulation systems are available. The unit that is
more commonly used is fully implanted and has a pulse generator and a non-rechargeable battery. The other system includes an antenna,
transmitter and a receiver that relies upon radio frequency. The latter system’s antenna and transmitter are carried outside the body, while the receiver is implanted inside the body.
When is spinal cord stimulation used?
Spinal cord stimulation is recommended when other treatments have not
been successful, when surgery is not likely to help or when surgery has failed. However, the device is not for everyone; check with your doctor to see if the procedure is right for you.
Care
Lower back pain relief at home
Self-care at home
General recommendations are to resume normal, or near normal, activity as
soon as possible. However stretching or activities that place additional strain on the back are discouraged.
• Sleeping with a pillow between the knees while lying on one side may increase comfort. Some doctors recommend lying on your back with a
pillow under your knees. • No specific back exercises have been found that improve pain or increase
functional ability in people with acute back pain. However exercise may be
useful for people with chronic back pain to help them return to normal activities and work.
• Non-prescription medications may provide relief from pain. o Ibuprofen, available over-the-counter, is an excellent medication for the
short-term treatment of lower back pain. Because of the risk of ulcers and
gastrointestinal bleeding, talk with your doctor about using this medication for a prolonged period of time.
o Paracetamol has been shown to be as effective as ibuprofen in relieving pain.
o Topical agents such as ‘deep heating rubs’ have not been shown to be
effective. • Some people seem to benefit from the use of ice or heat. Their use,
although not proven effective, is not considered to be harmful. Take care: do not use a heating pad on ‘high’ or place ice directly on the skin.
Most experts agree that prolonged bed rest is associated with a longer recovery period. People resting in bed are also more likely to develop
depression, blood clots in the legs and decreased muscle tone. Very few experts recommend more than a 48-hour period of decreased activity or bed rest. In other words get up and get moving as much as you can.
Living & managing
Are you suffering from back pain? You’ll find tips here to help you live with and manage back pain.
Living and coping
Pain management: Living with chronic pain
Chronic pain management can have physical and emotional benefits.
Chronic pain's emotional effects include depression, anger, anxiety and fear of re-injury which may hinder your ability to return to work or to take part in once enjoyable activities.
Additionally, the emotional toll of chronic pain can make pain worse. Anxiety, stress, depression, anger and fatigue interact in complex ways
with chronic pain and may decrease the body's production of natural painkillers; moreover, such negative feelings may increase the level of substances that amplify sensations of pain, causing a vicious cycle of pain.
If you or someone you love suffers from chronic pain it is important to get
help. There are many effective treatments available to relieve pain so that you or your loved one can start living again.
Managing chronic pain
The ideal treatment for chronic pain is a comprehensive approach that
addresses a person's physical, emotional, and cognitive needs. Successful treatment requires choosing a life-long plan of wellbeing that may include:
• Medical services • Physical therapy • Psychological counselling
• Occupational therapy.
If you suffer from chronic pain, the first thing to do is to see a doctor and get treated. Other steps that can make living with chronic pain more tolerable include the following:
• Learn how to relax through deep breathing and other stress-management techniques.
• Set achievable goals and don't overdo it on good days; learn to pace yourself.
• Engage in positive self-talk (statements that reaffirm positive qualities).

• Build rest, exercise and relaxation times into your daily schedule. • Join a chronic pain support group.
• Know your medications, including expected benefits and side effects. When the ‘cost’ exceeds the benefit, ask your doctor if something else might work
better. • Decrease or eliminate alcohol consumption. Pain often disrupts sleep and
alcohol can further disrupt the sleep cycle.
• Give up smoking. Cigarettes can impair healing and have been identified as a risk factor in the development of many diseases including degenerative
disc disease, a leading cause of lower back pain.
Don’t let chronic pain take you out of action.
Exercise, including back exercises, for long-term back pain
Introduction
Yes. An exercise program can help reduce long-term (chronic) back pain and help you get on with your normal activities.
What is it?
If you have long-term back pain, your doctor or physiotherapist may
recommend a structured exercise programme that you can do at home, or under supervision. The programmes can involve bending forward and
straightening your spine, stretching, and strengthening exercises (such as sit-ups).
Some exercise programmes have specific names. The most common are the Williams flexion programme and the McKenzie extension exercises. In the
Williams programme, people with back pain do lots of forward bending (flexion) to strengthen the abdominal muscles and the back muscles responsible for moving the spine. The McKenzie exercises focus on
straightening and extending the spine. Two others, the Mensendieck and Cesar programmes, combine exercises with teaching.
Another option is an aerobic exercise programme. This type of exercise
combines activities such as walking and cycling. It gets your cardiovascular system going so that your heart is beating faster, your blood is flowing and
oxygen is circulating around your body. If you join a gym, make sure you discuss your back problems with trainers there. They will be able to recommend which exercises are best for you.
If your doctor or physiotherapist recommends an exercise programme, they will work with you to draw up a plan that explains the type of exercises you should do, as well as how many repetitions to do and how often to do them.
How can it help?
If you've had back pain for more than three months, exercise programs can help you: [1]
• Feel less pain
• Move around and get on with your normal activities.
The studies lasted six months. The benefits of exercise seemed to last throughout the six months. [1]
Exercise works at least as well as any other usual treatment you might get from your doctor, such as painkillers.
Some research has looked at specific exercises, such as yoga, the Alexander technique or McKenzie exercises. There's some evidence that all these treatments can help. Some studies show that yoga or McKenzie exercises
might even be slightly better than other forms of exercise, but we can't be sure about this.
Why should it work?
The thinking behind exercise programmes is that the exercises will strengthen muscles that support your back, improve your flexibility and
increase your stamina. This will help you develop a stronger and less painful back. It also seems that they prevent symptoms from getting worse, which often happens when people are less active.
Some research has found that people who have long-term back pain have back muscles that aren't very toned. This makes it difficult for the spine to support itself in an upright position. Strengthening the muscles helps to take this stress off the spine.
There is also the 'feel good' factor that comes with exercising and achieving goals. Sometimes people with long-term back pain feel depressed. This can make their pain even worse. Some studies suggest that exercise may help
improve people's mood. This could give a positive boost and may help people to believe that they can manage to do more. Many studies measure how people feel about their pain and their ability to move around.
Can it be harmful?
Studies don't often show the possible harms of exercise programs.
But a few people in the studies found that their back pain got worse or their backs felt sore after exercise.
What's the evidence for exercises, including back exercise, for long-term back pain?
Introduction
There's quite a lot of good-quality evidence to show that exercise programmes can help people with long-term back pain.
We found one big summary of the research (a systematic review) on exercise programmes for long-term back pain. [3] It looked at 43 studies, with nearly 4,000 people in total.
The summary found that, overall, exercise programmes were helpful for people with long-term back pain. But there were some problems with the research studies.
• They looked at different types of back exercises. We don't know which ones
work best. Some studies show that yoga or McKenzie exercises might even be slightly better than other forms of exercise, but we can't be sure about
this. [1] [2] • Some of the studies were small, and some had problems with the way they
were carried out. Only six studies were really good quality.
And not all the studies found that exercise programmes worked. Some found that exercise made no difference.
Glossary
Systematic reviews
A systematic review is a thorough look through published research on a particular topic. Only studies that have been carried out to a high standard
are included. A systematic review may or may not include a meta-analysis, which is when the results from individual studies are put together.
Physiotherapist
A physiotherapist is a health professional who is trained to use physical activity and exercises to help people's bodies heal.
McKenzie exercises
McKenzie exercises are exercises that aim to help with back pain. They may
also be used to try to move pain from your legs to your lower back, where it may be easier to cope with.
Mensendieck therapy
Mensendieck therapy is a training programme. It includes exercises to improve your posture, as well as education about how to move in ways that
won't damage your body. Mensendieck therapy teaches people to take responsibility for their own health as a way of coping with pain or other problems.
Cesar therapy
Cesar therapy involves exercises to improve your posture. The aim is to reduce back pain caused by poor posture.
Information and Exercise Sheet (H013)
BACK PAIN
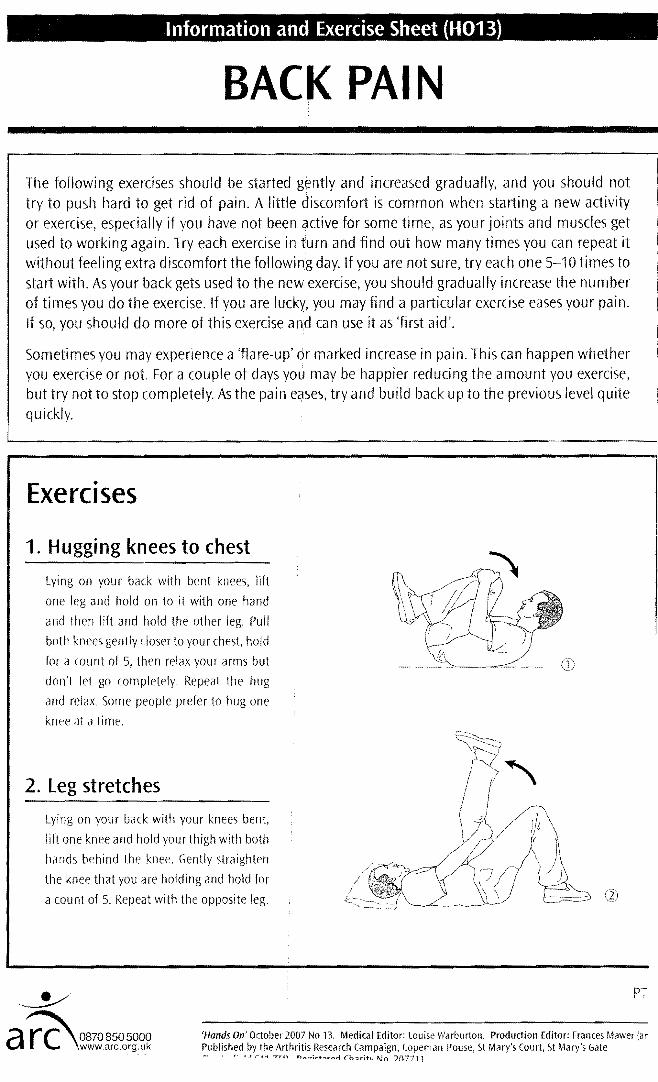
The following exercises should be started gently and increased gradually, and you should not try to push hard to get rid of pain. A little discomfort is common when starting a new activity or exercise, especially if you have not been active for some time, as your joints and muscles get used to working again. Try each exercise in turn and find out how many times you can repeat it without feeli ng extra discomfort the followinig day. If you are not sure, try each one 5-10 times to start with. As your back gets used to the new exercise, you should gradually increase the number of times you do the exercise. If you are lucky, you may find a particular exercise eases your pain. If so, you should do more of this exercise and can use it as 'first aid'.
Sometimes you may experience a 'flare-up' or marked increase in pain. This can happen whether you exercise or not. For a couple of days you may be happier reducing the amount you exercise, but try not to stop completely. As the pain eases, try and build back up to the previous level quite quickly.
Exercises
1. Huggi ng knees to chest
Lying on your back with bent knees, lift
one leg and hold on to it with one hand
and then lift and hold the other leg. Pull
both knees gently closer to your chest, hold
for a count of 5, then relax your arms but
don't let go completely. Repeat the hug
and relax Some people prefer to hug one
knee at a time.
2. leg stretches
Lying on your back with your knees bent,
lift one knee and hold your thigh with both
hands behind the knee. Gently straighten
the knee that you are holding and hold for
a count of 5. Repeat with the opposite leg.
~ PT
a~rc 08708505000rC \www.arc.org.Uk 'Hands On' October 2007 No 13. Medical Editor: louise Warburton. Production Editor: Frances Mawer (ar Published by the Arthritis Research Campaign, Copeman House, 5t Mary's Court. 5t Mary's Gate ~, r' 1,1 '''<1 "TTn n ..... '"";.--+n~ ..... rI rh:uiht /\In ')n7711
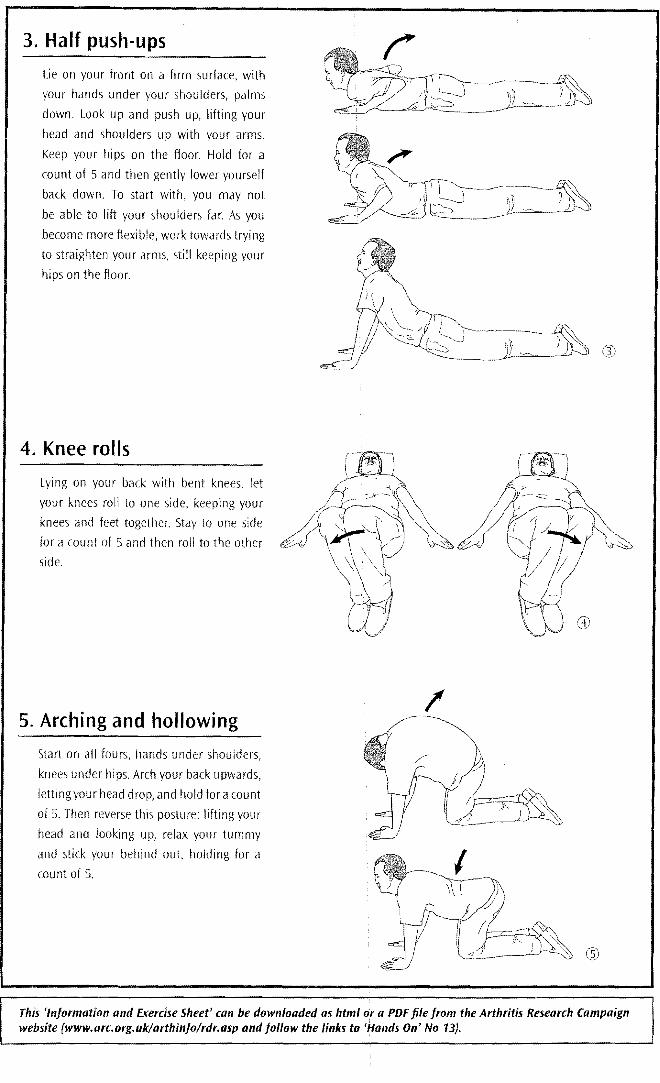
3. Half push-ups
Lie on your front on a firm surface, with
your hands under your shoulders, palms
down. Look up and push up, lifting your
head and shoulders up with your arms.
Keep your hips on the floor. Hold for a
count of 5 and then gently lower yourself
back down. To start with, you may not
be able to lift your shoulders far. As you
become more flexible, work towards trying
to straighten your arms, still keeping your
hips on the floor.
4. Knee rolls
Lying on your back with bent knees, let
your knees roll to one side, keeping your
knees and feet together. Stay to one side
for a count of 5 and then roll to the other
side.
/5. Arching and hollowing
Start on all fours, hands under shoulders,
knees under hips. Arch your back upwards,
letting your head drop, and hold for a count
of 5. Then reverse this posture: lifting your
head and looking up, relax your tummy
and stick your behind out, holding for a
count of 5.
This 'Information and Exercise Sheet' can be downloaded as html or a PDF file from the Arthritis Research Campaign website (www.arc.org.uklarthinfolrdr.aspandfollowthelinksto • .!andson.No13).