abraxane-gemcitabina ¿ha cambiado la historia del … · ¿ha cambiado la historia del cáncer de...
TRANSCRIPT
Abraxane-Gemcitabina ¿ha cambiado la historia
del cáncer de páncreas metastásico?
Berta Laquente
Oncología Médica. Hospital Duran y Reynals.
Institut Català d Oncologia


PANCREATIC CANCER IN NUMBERS
Pancreatic cancer is the seventh most prevalent cancer in Europe and accounts for
2.8% of cancers in men and 3.4 per cent in women.
Pancreatic cancer is the fourth deadliest cancer, with more than 95 per cent of those
affected dying from the disease.
According to the European Cancer Observatory there are 103,773 people are
currently living with pancreatic cancer in Europe.
According to a Eurocare study, the overall one-year survival rate in Europe ranges
from 11.5 per cent to 28.3 per cent.
Patients continue to die soon after being diagnosed; research has shown that only
5.7per cent of people diagnosed with pancreatic cancer in Europe are still alive five
years after diagnosis. This means that for every 20 people diagnosed with
pancreatic cancer, only one can expect to still be alive five years later.

¿Ha cambiado la historia del cáncer de páncreas metastásico?
Desarrollo del fármaco
Eficacia del esquema
Perfil de seguridad
Factores pronósticos/predictivos
Nuevo tratamiento estándar
Conclusiones

¿Ha cambiado la historia del cáncer de páncreas metastásico?
Desarrollo del fármaco
Eficacia del esquema
Perfil de seguridad
Factores pronósticos/predictivos
Nuevo tratamiento estándard
Conclusiones

Formulation of nab®Paclitaxel
Albumin-bound paclitaxel particle with a mean size of 130 nm1,2
nab-Paclitaxel is the first nanotechnology-derived agent approved for the treatment of breast and pancreatic cancer
This formulation exhibits linear pharmacokinetics over a clinically relevant dose range3 = predictable drug exposure with dose modification
1. Desai et al. SABCS. 2004 [abstract 1071].
2. Kratz et al. J Control Release. 2008;132(3):171-183.
3. Ibrahim et al. Clin Cancer Res. 2002;8(5):1038-1044. nab® is a registered trademark of Celgene Corporation.
Albumin
Paclitaxel
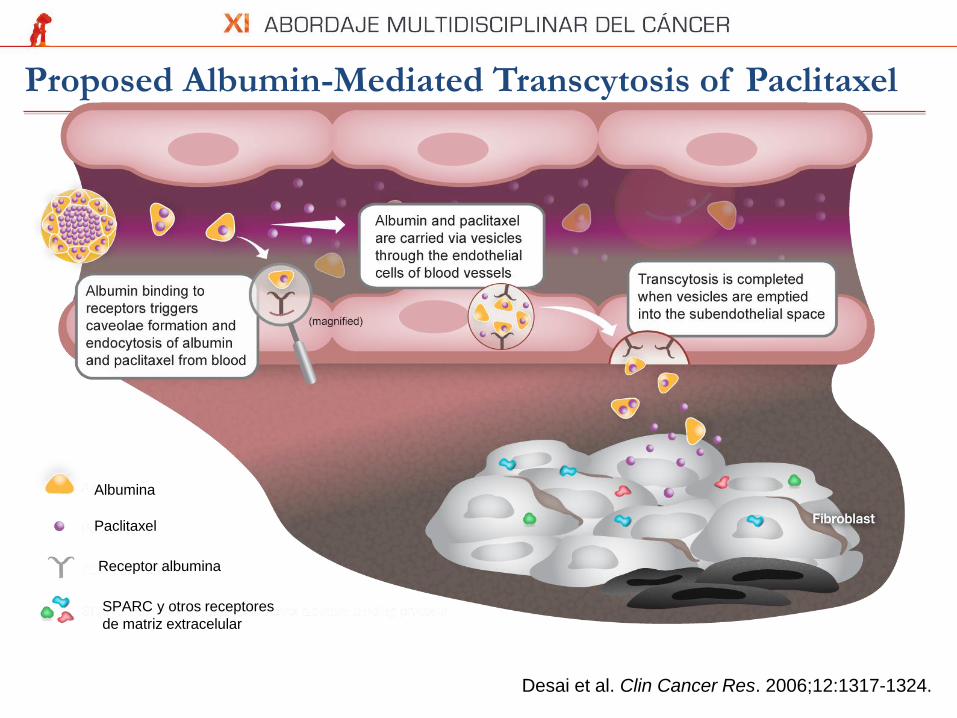
Proposed Albumin-Mediated Transcytosis of Paclitaxel
SPARC, Secreted Protein Acidic and Rich in Cysteine.
Tumor cells
Subendothelial space
Investigation of the functional importance of SPARC with
respect to nab-paclitaxel is ongoing.
Desai et al. Clin Cancer Res. 2006;12:1317-1324.
Albumina
Paclitaxel
Receptor albumina
SPARC y otros receptores
de matriz extracelular

Intratumoral drug concentration (xenografts)
D. Von Hoff et al, JCO 2011,29:4548-4554

Cycle 7: 04.13.2009
Baseline: 9.10.2008
D. Von Hoff et al. JCO 2011; 29(34):4548-54
Esquema recomendado para fase II-III: Abraxane 125 mg/m2 + Gemcitabina 1000 mg/m2
Administración semanal x 3 semanas, cada 4 semanas. Toxicidad limitante de dosis: Neutropenia
67-patient Phase I-II


¿Ha cambiado la historia del cáncer de páncreas metastásico?
Desarrollo del fármaco
Eficacia del esquema
Perfil de seguridad
Factores pronósticos/predictivos
Nuevo tratamiento estándar
Conclusiones

GEM+ Nab-PACLITAXEL trial: MPACT Phase 3
861 pts

GEM+ Nab-PACLITAXEL trial: MPACT Phase 3
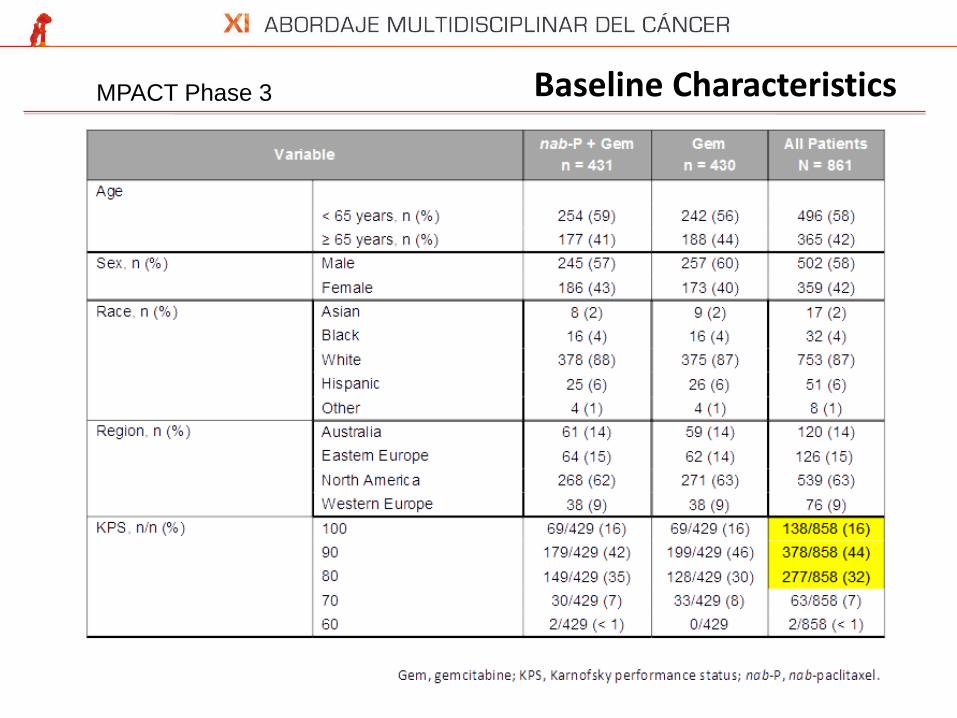
Baseline Characteristics MPACT Phase 3

Baseline Characteristics: cont’ MPACT Phase 3

Von Hoff DD, Ervin T, Arena FP, et al. Randomized Phase III Study of Weekly nab-Paclitaxel plus Gemcitabine vs Gemcitabine Alone in Patients with
Metastatic Adenocarcinoma of the Pancreas (MPACT) [abstract LBA148]. Oral presentation at: The Gastrointestinal Cancers Symposium 2013;
January 24-26; San Francisco, CA. 1
7
Gem, gemcitabine; nab-P, nab-paclitaxel.
Overall Survival
MPACT Phase 3 Overall Survival

MPACT Phase 3 OS Prespecified Subgroups

GEM+ Nab-PACLITAXEL trial: MPACT Phase 3 PFS

20 Von Hoff DD, Ervin T, Arena FP, et al. Randomized Phase III Study of Weekly nab-Paclitaxel plus Gemcitabine vs Gemcitabine Alone in Patients
with Metastatic Adenocarcinoma of the Pancreas (MPACT) [abstract LBA148]. Oral presentation at: The Gastrointestinal Cancers Symposium
2013; January 24-26; San Francisco, CA.
a Includes CR + PR + SD ≥ 16 weeks.
CR, complete response; Gem, gemcitabine; nab-P, nab-paclitaxel; PR, partial response; SD, stable disease.
Variable nab-P + Gem
n = 431
Gem
n = 430 P Value
Overall response rate
Independent review, %
(95% CI)
Investigator assessment, %
(95% CI)
23
(19.1 - 27.2)
29
(25.0 - 33.8)
7
(5.0 - 10.1)
8
(5.3 - 10.6)
1.1 × 10−10
3.3 × 10−16
Disease control rate by
independent review, a %
(95% CI)
48
(43.0 - 52.6)
33
(28.4 - 37.5)
7.2 × 10−6
Response Rates
GEM+ Nab-PACLITAXEL trial: MPACT Phase 3

¿Ha cambiado la historia del cáncer de páncreas metastásico?
Desarrollo del fármaco
Eficacia del esquema
Perfil de seguridad
Factores pronósticos/predictivos
Nuevo tratamiento estándar
Conclusiones

GEM+ Nab-PACLITAXEL trial: MPACT Phase 3 Safety

QoL
¿Ha cambiado la historia del cáncer de páncreas metastásico?
Desarrollo del fármaco
Eficacia del esquema
Perfil de seguridad
Factores pronósticos/predictivos
Nuevo tratamiento estándar
Conclusiones

30% of MPACT Patients Were Evaluable for the Stromal SPARC Biomarker Analysis
861
376
256
131 nab-P +
Gem
125 Gem
13% pancreas
50% liver mets
20% other mets
17% tissue of unknown origin
All patients (ITT
population) 100%
Patients with biomarker samples
Stromal SPARC evaluable
44%
30%
10% pancreas
55% liver mets
17% other mets
18% tissue of unknown
origin
Sample
tissue of
origin
Hidalgo M, Plaza C, Illei PB, et al. SPARC analysis in the phase III MPACT trial of nab-paclitaxel plus gemcitabine vs Gem alone for patients with metastatic
pancreatic cancer. Oral presentation at: 16th World Congress on Gastrointestinal Cancer; June 25-28, 2014; Barcelona, Spain [abstract O-0004].

Stromal SPARC Not Prognostic of Overall Survival in MPACT With Clinical Trial Assay
Stromal SPARC IHC SCORE
SPARC level High Low
n (%) 71 (28) 185 (72)
HR high vs low (95% CI) 1.019 (0.750 - 1.386)
P value (log rank) 0.9026
Pro
po
rtio
n o
f S
urv
ival
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0 0 6 12 18 24 30 36
Months
Hidalgo M, Plaza C, Illei PB, et al. SPARC analysis in the phase III MPACT trial of nab-paclitaxel plus gemcitabine vs Gem alone for patients with metastatic
pancreatic cancer. Oral presentation at: 16th World Congress on Gastrointestinal Cancer; June 25-28, 2014; Barcelona, Spain [abstract O-0004].

0.00
0.25
0.50
0.75
1.00
0 5 10 15 20 25 30 35
Stromal SPARC Not Predictive of Survival in Either Treatment Arm With Clinical Trial Assay
nab-P + Gem low SPARC (n = 97)
nab-P + Gem high SPARC (n = 34)
Gem low SPARC (n = 88)
Gem high SPARC (n = 37)
Stratification Factors,
n (%)
Stromal SPARC High Stromal SPARC Low
nab-P + Gem
n = 34
Gem
n = 37
nab-P + Gem
n = 97
Gem
n = 88
KPS 90 - 100
KPS 70 - 80
17 (50)
17 (50)
25 (68)
12 (32)
58 (60)
39 (40)
58 (66)
30 (34)
Liver metastasis 32 (94) 30 (81) 85 (88) 70 (80)
Pro
po
rtio
n o
f S
urv
iva
l
Months
High vs Low SPARC HR (95% CI)
nab-P + Gem 1.505 (0.978 - 2.315)
Gem alone 0.658 (0.423 - 1.023)
Hidalgo M, Plaza C, Illei PB, et al. SPARC analysis in the phase III MPACT trial of nab-paclitaxel plus gemcitabine vs Gem alone for patients with metastatic
pancreatic cancer. Oral presentation at: 16th World Congress on Gastrointestinal Cancer; June 25-28, 2014; Barcelona, Spain [abstract O-0004].


Prognostic factors

Goldstein D, et al. JNCI 2015,1-10
OS benefit in poor prognostic subgroups; post-hoc analysis
p < 0.001
p = 0.079

¿Ha cambiado la historia del cáncer de páncreas metastásico?
Desarrollo del fármaco
Eficacia del esquema
Perfil de seguridad
Factores pronósticos/predictivos
Nuevo tratamiento estándar
Conclusiones

Trials in PC involving Abraxane
Trial MOA Company Development Phase
Status Line of Therapy
PEGPH20 ± Abraxane + Gem
Pegylated hyaluronadase stimulant
Halozyme Therapeutics
Phase 2 Currently Recruiting
1st line advanced panc
GDC-0449 + Abraxane + Gem
Hedgehog inhibitor
Roche/Johns Hopkins Onc Center
Phase 2 Currently Recruiting
1st line advanced panc
ODSH ± Abraxane + Gem
2-0, 3-0 desulfated heparin
ParinGenix Phase 2 Currently Recruiting
1st line advanced panc
OGX-427 + Abraxane or Gem
HSP 27 antagonist
OncoGenex Phase 2 Currently Recruiting
1st line advanced panc
M402 + Abraxane + Gem vs Gem monotherapy
Heparin sulfate mimetic
Momenta Pharmaceuticals
Phase 1/2 Currently Recruiting
1st line advanced panc
Ruxolitinib + Gem with or without Abraxane
JAK 1,2 inhibitor Incyte Corporation Phase 1 Currently Recruiting
Any advanced pancreatic cancer
PLX7486 + Abraxane + Gem
Trk A/B/C kinase inhibitor
Daiichi Sankyo Phase I Currently Recruiting
1st line or 2nd line or greater
Source: TrialTrove, ClincalTrials.gov

Trials in PC involving Abraxane
Trial MOA Company Development Phase
Status Line of Therapy
OMP-59R5 ± Abraxane + Gem
Anti-Notch 2,3 Pathway Inhibitor
OncoMed Pharma
Phase 1b/2 Currently Recruiting
1st line advanced panc
LCL161 + Abraxane + Gem
IAP antagonist Novartis Phase 1 Planned 1st line advanced panc
Alisertib (MLN8237) + Abraxane
Aurora Kinase Inhibitor
Takeda/ Millennium
Phase 1 Currently Recruiting
1st or 2nd line in solid tumors that cannot be removed by surgery
GS-5745 with various chemotherapies, including Abraxane
Matrix metalloproteinase MAb
Gilead Phase 1 Currently Recruiting
Being tested in PC, NSCLC, and esophagogastric cancer
Source: TrialTrove, ClincalTrials.gov

¿Ha cambiado la historia del cáncer de páncreas metastásico?
Desarrollo del fármaco
Eficacia del esquema
Perfil de seguridad
Factores pronósticos/predictivos
Nuevo tratamiento estándar
Conclusiones
QoL?
SI

CASO CLÍNICO
Berta Laquente
Oncología Médica. Hospital Duran y Reynals

CASO CLÍNICO
Varón 46 años al diagnóstico.
Antecedentes familiares: Abuelo materno: Cáncer de colon
Laboral: Administrativo.
ANTECEDENTES PATOLÓGICOS
-Alergia a tetraciclinas.
-Hábitos tóxicos: Fumador activo. Desde los 14 años a los 40 de un paquete diario.
Actualmente, 10 cigarrillos/día.
-DLP en tratamiento médico. No HTA, o DM. No obesidad.
-No cardiopatías conocidas.
-Asma bronquial en tratamiento con corticoides inhalados. Descompensaciones en
invierno que habían requerido visita en Urgencias.
- Macrodenoma hipófisis de 2 cm con test hormonales normales y clínica visual.
• IQ en 7/2003 con AP de tumor productor de ACTH. Panhipop. anterior y post. tras la
IQ.
• En 2006 RM con por crecimiento del resto tumoral se reIQ (positivo para GH, ACTH
y PRL, ki67 7%) + RDT 50 Gy a finales 2006. Respuesta tumoral. Seguimiento por
Endocrino y Oncología Radioterápica.

HISTORIA ONCOLOGICA ACTUAL
-Primer síntoma (Agosto'13):
Lumbalgia por la que consulta en diversas ocasiones, diarrea y síndrome tóxico
(15Kgs en 2.5 meses). Derivado a Reumatología quien solicita 1ª EECCs Nov’13
Lesión cuerpo-cola: 80x51 mm
Adenopatías retroperitoneales,
15 mm diám. máximo
Metástasis pulmonares
Adenopatías mediastínicas, 36 mm
CA 19.9 239

VALORACION ONCOLOGIA MEDICA NOV’13
PAAF ECOENDOSCOPIA NOV ‘13: ADENOCARCINOMA
SINTOMAS
- Dolor lumbar controlado con analgesia 1er escalón
- No síntomas respiratorios
- Cuadro constitucional (peso habitual 100 Kg, peso PV 75 Kg) y astenia hasta grado
2
- Esteatorrea en tto sustitutivo enzimático
- PS1 Kf 80%

¿Qué tratamiento plantearías al paciente?
a) Quimioterapia esquema FOLFIRINOX
b) Quimioterapia esquema Gemcitabina en monoterapia
c) Quimioterapia esquema Gemcitabina más Abraxane
d) Ensayo fase III primera línea de tratamiento con nueva molécula en combinación
con tratamiento estándar vs tratamiento estándar

TRATAMIENTO
El paciente no pudo ser seleccionado para ensayo fase III por medicación necesaria
para hipopituitarismo.
TRATAMIENTO INDICADO
GEMCITABINA 1000 mg/m2 días + Abraxane 125 mg/m2 días 1,8 y 15 cada 28 d.
Inicio 1er ciclo: 8/12/2013
VALORACION TRAS 1ER CICLO:
- Paciente SIN dolor: ha suspendido analgesia 1er escalón
- Único síntoma: esteatorrea que obliga a aumento pauta enzimática
CA 19.9. 67

EVOLUCION
Tras 3 ciclos: EE radiológica, Peso 90, Kf 90%
El paciente continúa tratamiento hasta JULIO’2014 (7 ciclos).
El paciente quiere irse el mes de agosto de vacaciones
CA 19.9 30
Nov 2013 Julio 2014
CA 19.9 239

EVOLUCION
Septiembre 2014: PROGRESION PULMONAR. CA 19.9 756
¿Qué tratamiento plantearías al paciente?
a) El paciente ha progresado al mes y medio de suspender 1ª línea. Indicamos
tratamiento de segunda línea con FOLFOX
b) Reiniciamos tratamiento con el mismo esquema Gemcitabina + Abraxane
c) El paciente está asintomático, esperamos hasta progresión clínica.
d) Iniciamos tratamiento con capecitabina 1000 mg/m 2 cada 12 horas
EVOLUCION
Candidato a FOLFOX 6 Inicio 1/10/2014.
Tras 3 ciclos: CA 19.9 1792
PROGRESION PANCREATICA Y PULMONAR
Peso 80, Kf 80%

¿Qué tratamiento plantearías al paciente?
a) Planteamos ensayo fase I
a) Dado el beneficio clínico y la respuesta bioquímica previas, reiniciamos tratamiento
con el mismo esquema Gemcitabina + Abraxane
b) El paciente está asintomático, esperamos hasta progresión clínica.
c) Iniciamos tratamiento con capecitabina 1000 mg/m 2 cada 12 horas

EVOLUCION
Reiniciamos tratamiento con el mismo esquema Gemcitabina + Abraxane
1er ciclo re-tto Gemcitabina + Abraxane 3/12/2014. Tras 3 ciclos: peso 90, Kf 90%

GRACIAS!