abstract of dissertation entitled - school of nursing ka yui.pdf · abstract of dissertation...
TRANSCRIPT

1
Abstract of dissertation entitled
“An evidence-based programme for promoting active
video games to reduce weight among the overweight or
obese adolescents”
Submitted by
LEUNG KA YUI
for the degree of Master of Nursing
at The University of Hong Kong
in July 2015
Overweight or obese in adolescents become an epidemic in worldwide. Hong
Kong experiences the same issue too. Although there is weight management
programme for overweight or obese adolescents in Hong Kong, the prevalence
of overweight or obesity among adolescents keeps rising. It is not only arising
health impact among overweight or obese adolescents but also increasing the
2
economic burden and affecting the health policies in Hong Kong. To tackle this
problem, it is a need to develop a new evidence-based weight reduction
programme for these adolescents.
An active video game weight reduction programme is a potential innovation for
managing this issue. The players of the active video game can physically interact
with the screen image and increase the amount of physical activities and improve
the body composition. Some of the programme had been conducted in United
States and Australia already.
Integrated reviews were conducted to translate the best evidence to apply in the
current practice. Five randomized controlled trials (RCTs) studies were identified
from PubMed and CINAHL and evaluated by a critical appraisal tool, the
Scottish Intercollegiate Guidelines Network (SIGN). Three studies reported that
active video game is an effective innovation to reduce weight and increases the
duration of performing physical activity among overweight or obese adolescents.
In this thesis, it included an integrated reviews for active video game weight
reduction programme for overweight or obese adolescents; an evidence-based
3
guideline for implementing the active video game weight reduction programme
among overweight or obese adolescents; an implementation plan to propose
communication strategies, to initiate and sustain the active video game weight
reduction programme for overweight or obese adolescents; an evaluation plan for
evaluating the outcomes of the innovation.
Therefore, an active video game weight reduction programme among overweight
or obese adolescents would be an effective and practical innovation to be applied
in Hong Kong.

4
An evidence-based programme for promoting active video games to reduce
weight among the overweight or obese adolescents
By
Leung Ka Yui
BN;RN
A thesis submitted in partial fulfillment of the
Requirements for
the Degree of Master of Nursing
at The University of Hong Kong
July 2015
5
Declaration
I declared that this dissertation represents my own work, except where due
acknowledgement is made, and that it has not been previously included in a thesis,
dissertation or report submitted to this University or to any other institution for a degree,
diploma or other qualifications.
Signed
Leung Ka Yui
6
Acknowledgements
I would like to thank for all those whose gave supporting and encouragement in the
process of writing this thesis. I would like to extend my appreciation especially to my
project supervisor, Dr Janet Wong for the supervision and guidance. She provided great
inspirations for my thesis and spent her valuable time to give me suggestions from the
beginning to the end of writing this thesis.
I would like to thank all my colleagues in the Student Health Service, friends, parents
and classmates for their invaluable support and encouragement; otherwise I was not
able to complete my thesis on my own.
7
Table of Contents
Page
Abstract 1 - 3
Title Page 4
Declaration 5
Acknowledgements 6
Table of Contents 7 - 10
CHAPTER 1: INTRODUCTION
1.1 Background 11 - 13
1.2 Affirming the needs 13 - 14
1.3 Objectives and Significance 15
CHAPTER 2: CRITICAL APPRAISAL
2.1 Search and Appraisal strategies 16 -18
2.2 Results 19 - 23
2.3 Summary and Synthesis 24- 29
8
CHAPTER 3: TRANSLATION AND APPLICATION
3.1 Assessing Implementation potential
I. Transferability of the findings 30 – 35
II. Feasibility 35 – 38
III. Cost/ Benefit Ratio of the innovation 38 – 42
3.2 Developing evidence base practice guidelines 42 – 44
CHAPTER 4: IMPLEMENTATION PLAN
4.1 Communication Plan
I. Stakeholders Identification 45 – 46
II. Communication strategies to initiate change 46 – 49
III. Communication strategies to sustain change 50 – 51
4.2 Pilot Study Plan 51 – 54
4.3 Evaluation Plan
I. Outcome Evaluation 55 – 56
II. Determination the time for measuring the outcomes 57
III. Criteria and recruitment for the eligible students 57
9
IV. Data Analysis and sample size calculation 58
4.4 The basis for Implementation 59
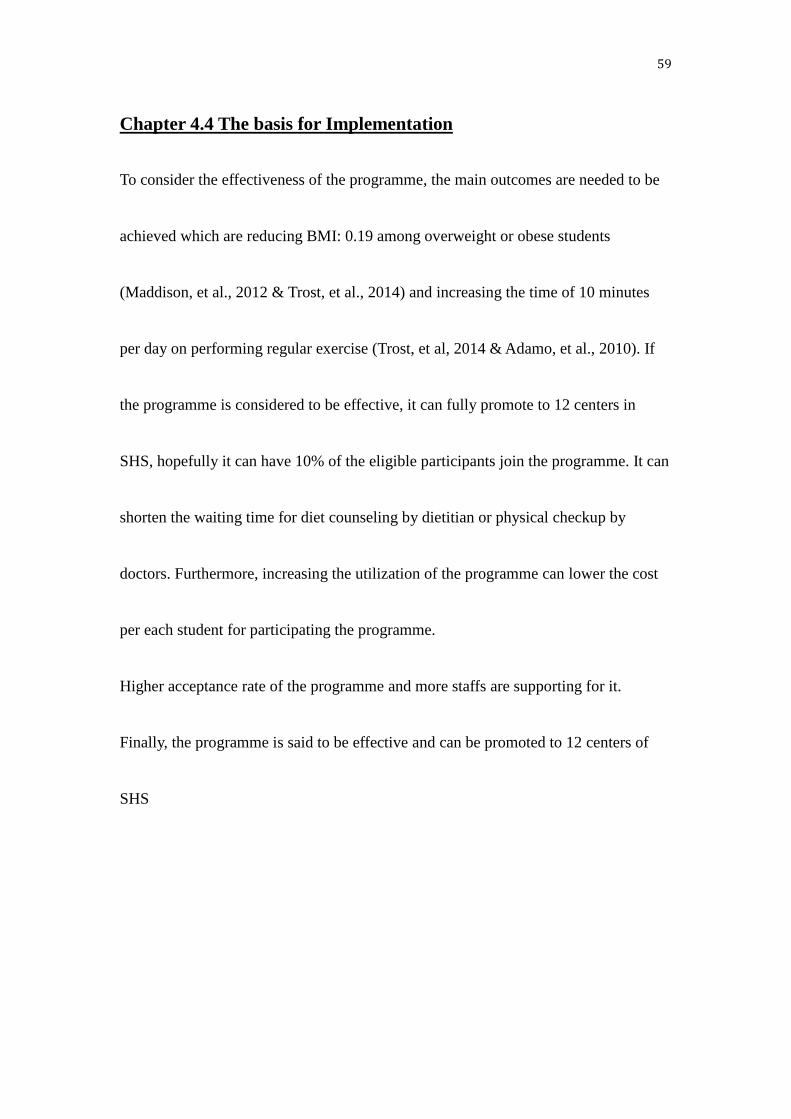
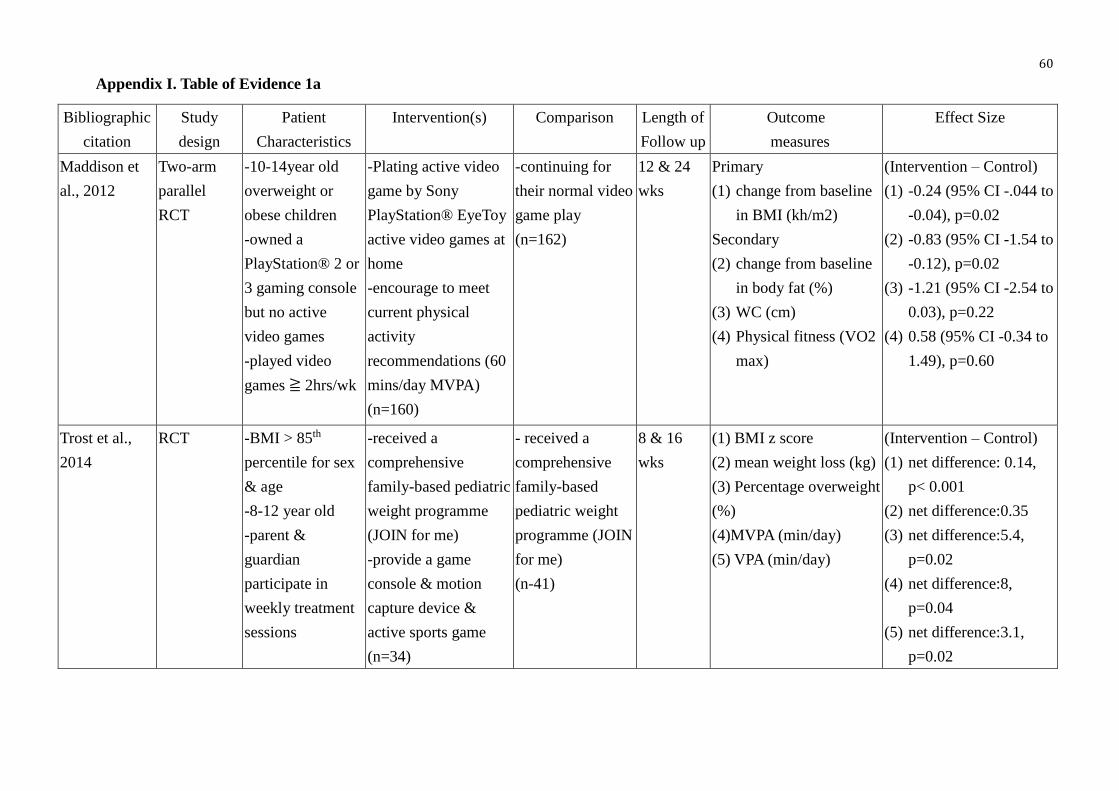
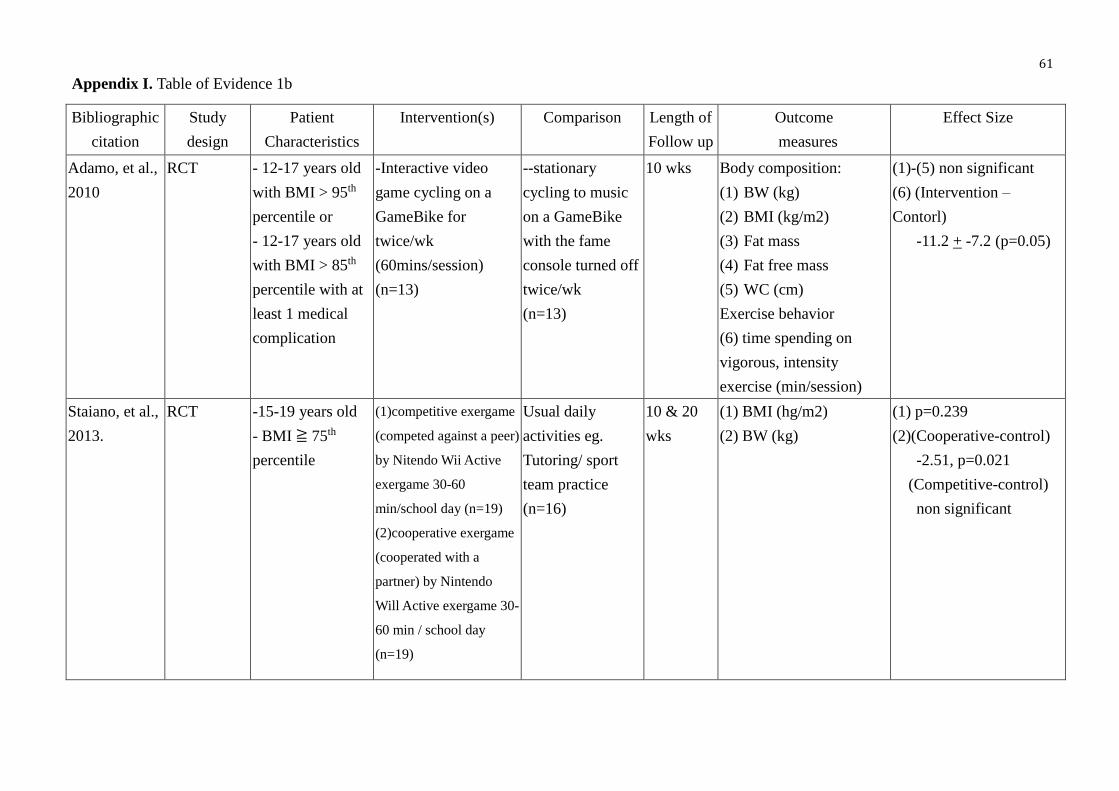
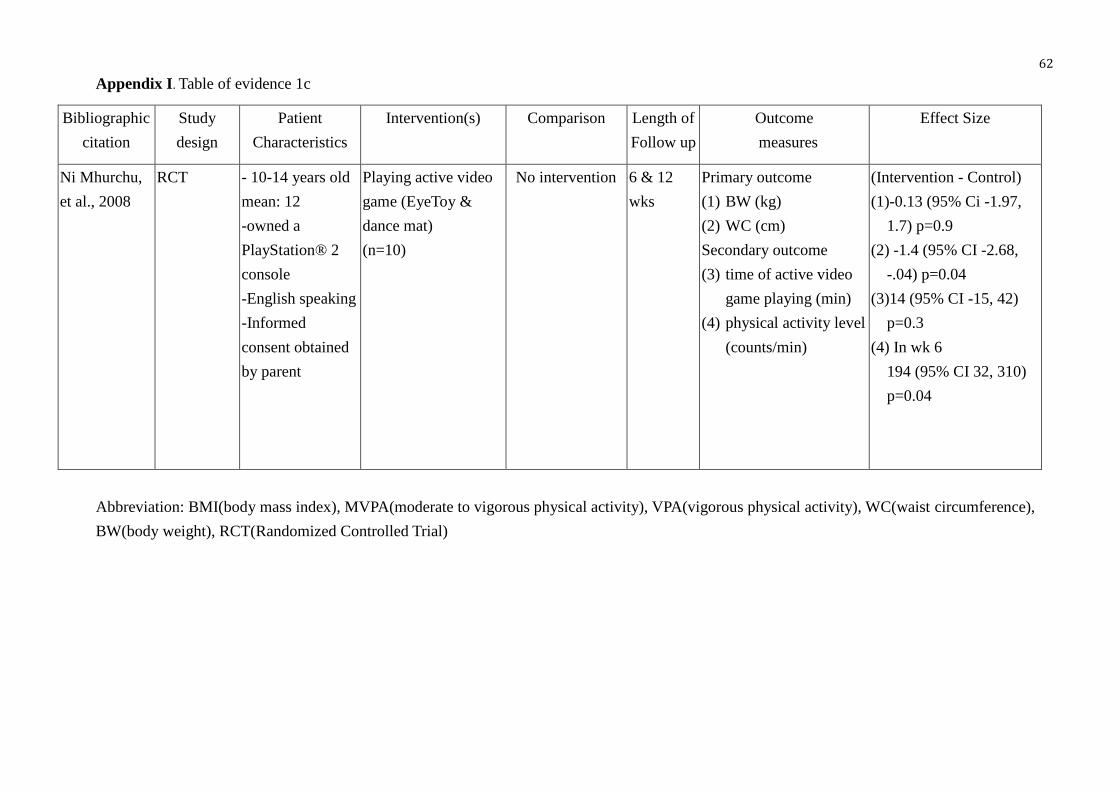
Appendix I. Table of Evidence 60 – 62
II. SIGN checklists 63 – 73
III. PRISMA 2009 Flow Diagram 74
IV. Cost on preparation and implementation active
video game weight reduction programme on
overweight or obese students 75
V. Benefit for implementing of active video game
to the overweight or obese adolescents in
SHSC, center X 76
VI. Time frame for implementing the programme 77
VII. Levels of Evidence 78
VIII. Grades of recommendations 79
IX. Guidelines on active video game reduction programme among overweight
or obese adolescents 80 – 86
10
X. References of the clinical Guidelines 87 – 88
References 89 – 93
11
Chapter 1: Introduction
Chapter 1.1 Background
Overweight and obese in adolescent become a serious problem in worldwide.
Overweight can be defined as “having excess body weight for a particular height from
fat, muscle, bone, water, or a combination of these factors”(National Institute of
Health, National Heart, Lung, and Blood institute, 2010 cited in Centers for Disease
Control and Prevention, 2014). The prevalence of childhood overweight and obese
had increased from 4.2 % in 1990 to 6.7% in 2010 globally (de Onis, Blössner &
Borghi, 2010). More than one third of children and adolescents were overweight or
obese in 2012 in the United States (Ogden, Carroll, Kit & Flegal, 2014). Likewise, in
Hong Kong the prevalence of overweight and obese students in primary and
secondary school increased from 15.7% in the school year of 1997-1998 to 20.3% in
2010-2011 (Department of Health, 2012). It relates to the unbalance diet of the
students, they eat fast food or junk food that is containing high in fat and sugar and
lack of dietary fiber intake. Besides the duration of the physical education (PE) in the
local school of Hong Kong is very limited, which only involves 2 lessons weekly and
12
the duration last for 35-40 minutes in each lesson (Education Bureau, 2002). With
excessive energy intake and without energy expenditure of the students, situation of
overweight or obese students becomes an epidemic in Hong Kong.
In Hong Kong, the Student Health Service (SHS) of the Department of Health (DH)
provides the physical and psychosocial assessment for the primary and secondary
school students once a year. It screens out the overweight or obese students from the
annual visit. The sex-specific reference charts of weight for height conducted by the
Hong Kong Growth Survey in 1993 is used to assess the weight status of the students
in SHS. The obesity of the student can be defined as weight greater than the median
weight for height X 120% (Department of Health, 2012).
The main duties of nurses in SHS are:
1. Providing health talks to all the students and parents and drawing their attention
on the importance of having balance diet and how to eat properly;
2. Providing individual counseling on weight control annually to the overweight or
obese students. The counseling guide on weight control in SHS bases on the diet
advises by the food pyramid and performing physical activity for 60 minutes daily
13
that was recommended by World Health Organization (WHO);
3. Referring to the dietitian and conduct advance diet counseling for overweight or
obese students and;
4. Providing the school-based health talk of “飲食習慣與健康”to the primary school
which is high prevalence of overweight or obese students.
However, the prevalence of overweight of obese student in Hong Kong keep
increasing, the current practice of weight control programme is said to be
unsuccessful.
Chapter 1.2 Affirming the needs
The overweight or obese students will have higher risk to suffer from chronic disease,
like heart disease and diabetes mellitus. Greater the body mass index (BMI) or waist
circumference (WC) has a strong correlation on hypertension in Chinese children and
adolescents (Lu, et al., 2013). Therefore it may increase the economic burden of the
government on the medical cost to tackle the chronic disease. Besides that 46.9% of
adolescent between 13-19 years old perform less than 10 minutes of moderate to
14
vigorous level of physical activity everyday. The reasons are having heavy workload
of schoolwork, feeling tired and not interested in doing exercise (Leisure and Cultural
Service Department & Community Sports Committee of the Sports Commission,
2012).
To address the awareness of the overweight or obese adolescent to perform regular
exercise for weight control, it is a must to promote alternative innovation for weight
control for the overweight or obese students. Active video game is one of the potential
innovations. The player of active video games can physically interact with screen
images (Maddison, et al., 2009). Therefore the players can increase the amount of
physical activities and improve body composition. Since education programme such
as health talks and diet counseling is the only method for weight control among the
overweight or obese student in SHS, there is no physical activity programme
conducted in SHS before. Active video game can be an alternative weight reduction
programme for the overweight or obese students. It is important to search for related
evidence to support the innovation.
15
Chapter 1.3 Objectives and Significance
This thesis aims at translating the evidence for active video games as an innovation
for weight reduction in overweight or obese adolescents.
The main objectives of this thesis were:
1. Conducting systematic reviews on implementing active video game for weight
reduction among overweight of obese adolescent;
2. Determining the possibility to implement active video game for weight
reduction among overweight or obese adolescents in Hong Kong and;
3. Developing an evidence-based active video game programme for weight
reduction in overweight or obese adolescents.
The prevalence of overweight or obese students will be reduced after implementing
the programme definitely. It can also lower the risk to have chronic disease earlier
when they are in adulthood. The survival rate of the overweight or obese population
can be increased and the mortality rate of them can be lowered. Therefore, does active
video game act as a potential innovation for weight reduction in overweight or obese
adolescents in Hong Kong?
16
Chapter 2: Critical Appraisal
Chapter 2.1 Search and Appraisal Strategies
A. Searching Criteria
A systematic review was needed to obtain related evidence for using active video
games as the weight reduction innovation among overweight or obese students. Some
inclusion or exclusion criteria were needed to develop for identifying for the potential
studies and extracting out the evidence to support the possibility of the innovation.
For increasing the power of the evidence, the studies with randomized controlled
trials were included in searching. There was no restriction on the year of publication,
duration, sample size and language for publication of the potential studies. Moreover,
the aims of the potential studies should be weight control for the overweight or obese
adolescent and improve their health status.
The inclusion criteria are:
1. The participants were overweight or obese adolescent between 8-18 years old;
2. Receiving active video game as an innovation for weight control and;
3. Primary outcomes measure would be the body weight, BMI or WC or the duration
17
to perform physical activity of the participants but there were no restriction on the
secondary outcomes.
The exclusion criteria are:
1. The overweight or obese adolescents with long-term medication;
2. Already follow up by any specialty for weight control or even attending other
weight management programme.
B. Searching Strategies
The electronic searching database: PubMed and CINAHL were used for identifying
the potential articles with the following keywords: Obesity or Overweight or weight
management and Adolescents or Pediatric or Teenagers and Active video game or
Computer games or electronic games.
For the potential articles, they were reviewed in details and extracting the data into the
Table of Evidence. The citation, study design, subject characteristics, intervention
group, comparison group, length of follow-up, outcome measures and effect size were
analyzed in the table of evidence which were attached in the Appendix I (1a-1c).
18
C. Tools for the quality assessment in the reviewed studies
To ensure the quality of the relevant studies, critical appraisal tool was used to
analyze the studies. The Critical Appraisal Skills Programme (CASP) was developed
at the Public Health Resource Unit, Oxford in United Kingdom in 1993 (Critical
Appraisal Skills Programme, 2013). The aim of the programme enables health care
professionals to develop the skills on usage of research evidence and generate the
knowledge into their own practice. It provides critical appraisal checklist for the
people to criticize the reliability, validity of the studies. The level of evidence was
rated by the guidelines from the Scottish Intercollegiate Guidelines Network (SIGN).
SIGN develops evidence base guidelines for the National Health Service (NHS) in
Scotland and helps the health care professional to generate the new knowledge into
their practice and benefit to their patients or clients. The randomized controlled trails
checklist by SIGN Version 2.0 was used to appraise the quality of the studies (Scottish
Intercollegiate Guidelines Network, 2012).
19
Chapter 2.2 Results
A. Flows for searching the reviewed studies
A systematic review was performed from 15th May 2014 to 15th August 2014 to
extract the eligible articles for determining the effectiveness of the innovation. 700
articles were found based on the keyword searching. 280 and 420 articles were found
from CINAHL and PubMed respectively. After reviewing the title of the identified
articles, 126 articles were screened out. Then 72 articles were identified after
reviewing the abstracts of them. Afterwards these articles were reviewed in details
including the articles in their references and randomized controlled trials (RCT)
studies were included only. 25 eligible articles were extracted out and finally five
articles were found after eliminating the duplication of all the articles. The history of
the systematic search was summarized and presented in the flowchart that was
attached in the Appendix III.
B. Searching results
Five RCTs studies (Maddison, et al., 2012; Ni Mhurchu, et al., 2008; Trost, Sundal,
Foster, Lent & Vojta, 2014; Adamo, Rutherford & Goldfield, 2010; Stiano, Abraham
20
& Calvert, 2013) were viewed in details and all the data were summarized into the
Table of evidence and attached in the Appendix I (1a-1c). Two studies were conducted
in New Zealand (Maddison, et al., 2012; Ni Mhurchu, et al., 2008) and the other three
studies were conducted in United States of America (Trost, Sundal, Foster, Lent &
Vojta, 2014; Adamo, Rutherford & Goldfield, 2010; Stiano, Abraham & Calvert,
2013). The participants in one study was recruited randomly from school and child
center (Trost, Sundal, Foster, Lent & Vojta, 2014), one was from a clinic (Adamo,
Rutherford & Goldfield, 2010) and the other three were recruited from schools. One
of the studies (Maddison et al., 2012) was a home-based programme, one of them was
a clinic-based programme (Adamo, Rutherford & Goldfield, 2010) and the others
were the school-based programme. The study from Trost, Sundal, Foster, Lent &
Vojta, 2014 involved family members in the programme and the others were involved
by the participants only. All the studies fulfilled the inclusion criteria of age between
8-18 years old adolescents with no medication required, following up in specialty for
weight control and attending other weight management programme. The aims of all
studies wanted to explore the effectiveness of using active video game in weight
21
control among adolescents and three of them also explored the duration on
performing physical activity after implementing the innovation (Trost, Sundal, Foster,
Lent & Vojta, 2014; Adamo, Rutherford & Goldfield, 2010; Ni Mhurchu, et al., 2008).
The duration of all the studies were performed between 10 to 24 weeks respectively.
All the studies were conducted in RCT that can provide a stronger level of the
evidence to evaluate the effectiveness of the innovation to the target population. It is
important to allocate the subjects into intervention or control group randomly in a
study. The process of randomization is essential. Two studies (Maddison, et al., 2012;
Trost, Sundal, Foster, Lent & Vojta, 2014) reported that using the computerized
central system for randomization, one study (Adamo, Rutherford & Goldfield, 2010)
reported that an independent statistician conducted the randomization process. And
the others did not clearly state the process of randomization.
Calculation of the sample size is important in a study too, so the readers can
understand the truth effectiveness and statistically validity of the studies. However,
one study (Maddison, et al., 2012) clearly stated that the method of calculation of the
sample size by estimated to provide ≥90% power at a 5% level of significance. And
22
one study (Trost, Sundal, Foster, Lent & Vojta, 2014) reported the sample size
calculation by setting the power at ≥80%. But the others did not report the method for
sample size calculation, they might under the risk of Type 2 error and underestimate
the result of the studies.
And two studies (Maddison, et al., 2012; Trost, Sundal, Foster, Lent & Vojta, 2014)
reported that an intention to treat analysis was used as a sensitive analysis to minimize
the bias on loss of follow-up or missing data. But the other studies did not report for
this analysis. Furthermore, all studies reported that the baseline characteristics of the
participant in either intervention or control groups were not significantly difference
(p< 0.05) at the beginning of the studies. Also, the methods of the data collection were
reported clearly in all studies and they collected the data objectively for baseline and
follow-up measure to minimize the bias and maintain the consistency in the process of
data collection. Since implementing active video game for weight control among
adolescent were the behavioral intervention, all studies reported that they could not
blind the participants. To minimize the bias of the studies, all the studies reported that
independent data collectors, data analyzers, programme conductors or participant
23
recruiters were used in each stage of the studies.
C. Quality assessment of the reviewed studies
The checklist of SIGN rated the quality of the five eligible studies, the details of the
methodology of the studies were presented in the Appendix II. All the studies reported
that they could not blind the participants for allocating them into intervention or
control group respectively, but all the studies reported that they tried other method to
minimize the bias. Two studies (Maddison, et al, 2012; Trost, Sundal, Foster, Lent &
Vojta, 2014) were rated to have stronger evidence (Level 1 ++) than the others.
Because these two studies fulfilled almost all the criteria in the SIGN checklist, they
had clearly stated the randomization process, sample size calculation and using the
intention-to-treat analysis. The rest of the studies rated less evidence (Level 1+), they
all had mild weakness in the methodology that was small simple size, without
explaining the method for calculation of the sample size, shorter duration of follow-up
or conducted in one site only.
24
Chapter 2.3 Summary and Synthesis
A. Effectiveness of the reviewed studies
Five RCTs studies were reviewed in full paper, different outcomes were measured to
indicate that active video game is a potential innovation for weight management
among adolescent. The amount of weight loss, WC and BMI are the common
indicator to measure the effectiveness on weight control in the participants. The
amount of weight loss and BMI were also used in the outcome measure in all these
five studies and significant results were obtained in three of the studies (Maddison, et
al., 2012; Trost, Sundal, Foster, Lent & Vojta, 2014; Stiano, Abraham & Calvert,
2013). And since two of theses studies (Maddison, et al., 2012; Trost, Sundal, Foster,
Lent & Vojta, 2014) reported clearly about the randomization process and the method
to calculate the sample size, a stronger level of evidence were found in these two
studies to provide the effectiveness of the innovation. The other studies (Adamo,
Rutherford & Goldfield, 2010; Ni Mhurchu, et al., 2008) reported non-significance
result in weight loss or BMI among the adolescents, it might relate to the small
sample size with n=13, n=10 respectively in each of the intervention or control group
25
of the studies. Small sample size might underestimate the outcome of the innovation,
the studies had less power to represent the truth effectiveness of the innovation in the
target population. The studies might be at risk in Type 2 error. Moreover, only one out
of three studies (Ni Mhurchu, et al., 2008) reported to have a significant result
(p=0.04) on reducing the WC after implementing the innovation. The other two
studies with small sample size and short duration of the innovation might affect the
outcome of the studies. Therefore it can proof that active video game is an effective
innovation for weight management among adolescent.
Besides implementing active video game for weight reduction among the participants,
encouraging the adolescents to perform physical activity regularly is the one of the
aims of this thesis. Duration of moderate to vigorous physical activity (MVPA) and
vigorous physical activity (VPA) were measured as the secondary outcomes on three
of the studies (Trost, Sundal, Foster, Lent & Vojta, 2014; Adamo, Rutherford &
Goldfield, 2010; Ni Mhurchu, et al., 2008). All these studies reported to have a
significant result of increasing the time spending on MVPA or VPA in the intervention
groups. Although there were small amount of weight loss in the participants in these
26
studies, increasing the amount of duration on performing MVPA or VPA can increase
the level of energy expenditure by the participants. Since the duration of these studies
were short (10-16 weeks), better outcome of weight control among the adolescents
might be resulted after prolonging the period of the innovation. As a result, active
video game is an effective innovation to encourage the overweight or obese
adolescent sustaining and increasing the initiative to perform physical activity. And
active video game may be an effective innovation for conducting a long-term weight
reduction programme for the overweight or obese adolescents.
Moreover, one study (Stiano, Abraham & Calvert, 2013) measured the peer support,
self-efficacy and self-esteem of the participants after playing for active video game.
No significant result was found among the relationship between weight loss and self-
efficacy or self-esteem between intervention or control group of the study. A
significant result (p =0.01) was found in increasing the peer support in the cooperative
intervention group than the control group and the higher of the peer support would
lose more weight over time in this study. It was mainly due to the cooperative
intervention group required a partner to play with the active video game, the
27
participant could form a team during the intervention period, they could support each
other, sustain to perform active video game and increase the amount of energy
expenditure to achieve the goal for weight loss. Therefore, cooperative active video
game can provide a social reinforcement to sustain performing physical activity
among adolescent. Cooperative active video game can be a new element for weight
control among overweight or obese adolescents.
B. The needs for implementing the innovation
Although there was no active video game study or programme conducted in Hong
Kong for evaluating the effectiveness on weight reduction in overweight or obese
adolescent, five eligible studies had been conducted in New Zealand or United States
of America already. Since New Zealand and United States of America are the
developed countries, the characteristic of the participants of these studies may be
similar to the adolescent in Hong Kong. Besides that the design of the five eligible
studies were RCT study, they are located on the level II of the evidence hierarchy. It
can provide a strong evidence to support the effectiveness of the innovation in one
study. Therefore, it can conclude that active video game is an effective innovation for
28
weight reduction among overweight or obese adolescents, and it can be the potential
innovation to be applied in Hong Kong.
C. Possibility to be implemented to current practice
To implement the active video game for weight reduction the overweight or obese
adolescent in Hong Kong, some modifications are required according to the study
result of the five eligible studies. Most of the studies were a school-based programme,
student can perform physical activity at school more conveniently. Also, the study of
Stiano, Abraham & Calvert, 2013 reported that peer support and social reinforcement
could enhance the adolescents to sustain for doing physical activity and receive a
better outcome for weight control, therefore it was better to play with a partner when
implementing the innovation. Moreover, one of the studies (Trost, Sundal, Foster,
Lent & Vojta, 2014) also included parent or guardian in the programme, the roles of
the parent or guardian were encouraging their children for weight control, acting an
model or changing the home environment like eating habit. And the result of this
study gave a significant outcome for weight loss among the participant in the
intervention group. So involving parent in the programme might receive a better
29
outcome for the innovation.
Although few studies were addressing the effectiveness of active video game for
weight reduction among overweight or obese adolescents, five eligible studies were
conducted in New Zealand and United States of America to provide strong evidence
for supporting this innovation. Active video game is identified as a new method for
weight management in overweight or obese adolescent in these few years. It is a
reliable and practical innovation and can be applied into the setting of Hong Kong. To
summarize all the findings in the five eligible studies, a school based active video
game programme, a longer duration of the innovation, performing active video game
with a partner and involving the parent for supporting and monitoring in the
programme can obtain a better outcome for weight control among the target
population. To conclude, a more details and structural programme is required to be
designed for implementing active video game on weight redcution among overweight
or obese adolescents in Hong Kong.
30
Chapter 3: Translation and Application
This chapter intends to explore the implementation potential of promoting active video
game to reduce weight among overweight or obese adolescents in Hong Kong.
Evidence-based guidelines are attached in this chapter to support for the
recommendation on the proposed innovation.
3.1. Assessing implementation potential
Ⅰ.Transferability of the findings
To implement the active video game weight reduction programme in Hong Kong,
Student Health Service (SHS) might be a suitable place to adopt this innovation.
Philosophy of care
SHS was established in 1995 by the Department of Health (DH) in Hong Kong. SHS
aims to monitor the physical and psychological health of the school aged children by
health promotion and disease prevention, enabling them to gain the maximum benefit
from the education system and develop their full potential (Department of Health, 2012).
In addition, SHS wants to promote self-reliance and self-care in prevention of ill health
31
and maintenance of health in children, early detection of disease and disease prevention
are the ultimate goals in SHS.
Target audience and setting
The target population of SHS is all primary one to secondary six students (6 to 18 years
old) of day schools, including special schools and international schools. SHS contains
12 centers. Every eligible student will attend an annual visit in Student Health Service
Center (SHSC). During the annual visit, vision screening, hearing screening, growth
monitoring, blood pressure taking, screening for scoliosis, assessment of psychosocial
health and individual health counseling will be provided to students by nurses or
doctors in SHSC. Therefore, SHS contains the health status of the school-aged students
mostly in Hong Kong. It is a compatible environment to implement the innovation.
Besides, assessing the health status of the students physically and psychosocially,
nurses use to provide health talks to the students and draw their awareness of disease
prevention and maintain healthy lifestyle.
32
Similarity of the innovation in the proposed setting
Programme for active video game for weight reduction among overweight or obese
adolescents is proposed to implement in one of the SHSC, center X. 50,893 students
enrolled in center X in the school year of 2012/2013, 37,979 students attended the
annual visit, the attendance rate was 65.4% in the school year of 2012/2013 in center X
(Department of Health, 2013). The sex-specific reference chart of weight to height
conducted by the Hong Kong Growth Survey in 1993 is used to assess the weight of
the students. The overweight or obese students can be defined as weight greater than
the median weight for height X 120% or BMI ≥ 23. And the prevalence of overweight
or obese students was 20.3% in 2010/2011 (Department of Health, 2012). Large amount
of students were classified as overweight or obese, it is a serious situation in Hong
Kong. Active video game weight reduction programme has been used for few years in
Australia and United States of America. Few studies had been conducted to examine
the effectiveness of the programme (Maddison, et al., 2012, Trost, et al., 2014, Adamo,
et al., 2010, Staiano, et al., 2013 & Ni Mhurchu, et al., 2008). The review studies
targeted mainly on 10-18 years old overweight or obese students with BMI ≥ 85
33
percentile with no medical complication and were conducted in school or clinic basic.
Although no previous studies or programme has been conducted in SHS of Hong Kong
before, the characteristics of the population in the review studies were similar as the
overweight or obese adolescents attending SHSC, center X in Hong Kong.
Number of overweight or obese adolescents benefit in the programme
As mentioned before, there are around 35000 students attending SHSC, center X every
year, and approximate 20% of overweight or obese students are in Hong Kong every
year (Department of Health, 2012). Moreover, for students aged (≥10 and < 18) with
BMI ≥97th percentile for age and sex specific index or students aged 18 or above with
BMI ≥25, screening of urine sugar will be required. 1,356 students were required for
urine sugar test in 2012/2013 in SHSC, center X. The overweight or obese students will
be referred to the Special Assessment Center (SAC) for diet counseling by the dietitian
in the current practice, but there are only 6 SACs that provide this service. Since there
is high prevalence of overweight or obesity among students but with limited resources,
the students are required to wait few months for the diet counseling. Therefore, many
parents refuse to attend the diet counseling by dietitian since they require waiting for a
34
couple of months.
Active video game weight reduction programme is proposed to implement twice a year
in SHSC, center X. 30 overweight or obese students will be recruited in each time. It
may provide an alternative innovation for the overweight or obese students for better
weight control. Hopefully, it may decrease the workload of the diet counseling by the
dietitian and the waiting time to consult dietitian.
Time frame for implementation
According to the evidence of the review studies, the entire programme will last for 6
months, including 1 month for recruiting eligible cases, 16 weeks for the innovation
and 1 month between the stage of recruiting case and innovation. Also, 2 months for
communicating with the administrators and setting up for the programme are required
respectively, a Gantt chart was attached in Appendix IV for showing the time frame for
implementation of the programme. Enrolled students require to measure body weight
and height in each annual visit routinely. To access the effectiveness of the programme,
the body weight, body height and waist circumference (WC) of the students can be
simply measured at week 8, 16 and the end of the innovation and the annual visit in the
35
next school year.
II. Feasibility
Response from the nursing staffs and administrators
Since SHS is a well-structured service and does no harm to the public, the pros and
cons of the innovation are required to consider comprehensively by administrators.
Thus, there is no freedom for making the decision for implementing the innovation in
SHSC, center X by frontline staffs, but the administrators welcome the staffs to express
their opinion in improving the quality of the service and benefit to the clients. And DH
shows that she has determined to tackle the child obesity since 2006, the
"[email protected]" campaign was held to promote healthy eating at school for
children’s growth, prevention of chronic disease and obesity (Department of Health,
2012). The administrators will support for the innovation but a well-planned proposal
is required to submit to the administrators. The rational for the innovation, the resource
requires, the cost effectiveness and the content of the programme are required to state
clearly in the proposal.
36
However, the response from the frontline nurses may vary individually. Some nurses
are willing to implement the proposed innovation. Since the current practice for weight
control on overweight or obese students have been used for a long time but the
prevalence for overweight or obese students keeps increasing. These nurses will support
for the innovation definitely. They want to achieve a better outcome for weight
reduction among overweight or obese students. On the other hand, some nurses have
been adopting the current practice for a long time and they may reluctant to change. It
may increase their workload and spend much more time to learn new knowledge. To
tackle this problem, the administrator and the programme conductor require supporting
the nurses by giving appropriate training and enough time for them to adopt the new
practice.
Interference on the staffs and the organization
To implement the innovation, nurses need to have half day training on how to operate
the active video game consoles. The training is organized on Saturday that is out of
official working hour. The administrators should be notified so that the compensation
of working overtime could be granted to the nurses. Moreover, the innovation will be
37
hold for 20 hours per month, six registered nurses in center X will share the workload
of the programme. The registered nurses in SHSC, center X have already trained for
delivering health message to the students. They can continue to educate the students on
how to eat healthily. One registered nurse will hold the progamme in each session; each
nurse may work for 3.3 hours more after implementation the programme per month.
After the programme is implemented, the number of referral to the dietitian for diet
counseling will decrease. So the burden of the dietitian will be lowered and the waiting
time for counseling dietitian will be shortened too. In addition, there was evidence on
the effectiveness of the innovation for weight reduction among overweight or obese
students, the specialty referrals for further management of this issue will definitely
decrease.
Resources for implementation and evaluation of the programme
A computer, screen, loudspeaker, room facilities and personnel are required in the
programme and they are already available in center X. However, the programme
conductors require obtaining an approval from the administrators for purchasing the
active video game consoles and games. For evaluation of the programme, electronic
38
stadiometer for measuring body height and weight, a tape measure for measuring the
WC are also available in center X.
III. Cost/ Benefit Ratio of the innovation
Risk and benefit for implementation of the innovation
From the studies reviewed, they had not reported any risk for implement active video
game for weight reduction among overweight or obese students. However, they had
reported several strengths for the innovation. Firstly, two studies reported that the BMI
of the overweight or obese students had a significant decrease after playing active video
game (Maddison, et al., 2012 & Trost, et al., 2014). And three studies reported that the
time on spending vigorous, intensity exercise was increased significantly too (Trost, et
al., 2014, Ademo, et al., 2010 & Ni Mhurchu, et al., 2008). Increasing the time spending
on vigorous, intensity exercise can definitely increase the energy expenditure. It can
achieve the goal for weight reduction among overweight or obese students. Since the
innovation has significant effect on weight reduction among overweight or obese
students, it can promote to other SHSC or even schools. The prevalence of overweight
or obese students in Hong Kong can be decreased gradually. Besides, good control of
39
body weight can also improve the self-confidence of the students so that can be
beneficial to their psychological health.
However, there are some risks if SHS keeps the current practice. The prevalence of
overweight or obese students will keep increasing. These students will increase the risk
to suffer from chronic disease like hypertension, diabetes mellitus or heart disease
(Maggio, et al., 2014). As a result, the economic burden of the government of Hong
Kong to tackle the chronic disease among will be definitely increased.
Cost for the proposed innovation
For implementing the innovation, some material or nonmaterial cost are required to be
considered. For material cost, a quality trainer like physiotherapist for introducing how
to operate the active video game console should be recruited. Also, 6 registered nurses
from SHSC, center X require to work overtime on the half day training programme, the
compensation of working overtime will be calculated based on the master pay scale by
the government of Hong Kong (Civil Service Bureau, 2013). The active video game
console and the games are required to purchase for the programme. For the details of
the expense of the programme is attached in the Appendix Ⅳ.
40
On the other hand, there are also some nonmaterial costs for implementing the
innovation. To implement a new practice in a workplace, it is not easy to be accepted
by the nurses. Nurses require extra training for the innovation, they may spend extra
time for learning skills and adopt the innovation. Stress may be resulted. Also,
increasing the workload and expectation by the administrators without any
reinforcement to the nurses, the staff morale will be lowered and turnover rate will be
increased finally.
Costs for the current practice
If the current practice remains unchanged, material and nonmaterial costs will be
resulted. Overweight or obese students will be referred to the dietitians for diet
counseling in current practice. However, students may spend longer waiting time for
counseling dietitians due to limited resources in SHS. To improve this situation, SHS
may require recruiting more dietitians for a long run. Furthermore, SHS will require
increasing the printing fee for distributing the pamphlets for weight control among
overweight or obese students. One pamphlet may cost $0.5 for printing and 1,356
students in 2012/2013 with body weight ≥ 120 % median weight for height index in
41
SHSC, center X, the printing fee will be approximately $ 678 per year. For the details
of the benefit of not implementing the innovation, it is attached at Appendix Ⅴ. The
cost/ benefit ratio of the programme is 0.7 to 1.0.
For the nonmaterial cost on not implementing the innovation, it will properly increase
the interviewing time by nurses for diet advise for the overweight or obese students, the
consulting time by the doctor for the physical examination, the time by the clerical clerk
for booking the appointment to consult dietitian and making the referral for other
specialties for further managing the overweight or obese students.
Nonmaterial benefit for implementing the proposed innovation
From the reviews studies, they had already proved that active video game is an effective
innovation for weight reduction among overweight or obese students. To implement
this innovation in SHSC, center X, it will definitely reduce the body weight of the
overweight or obese students. Having a significant outcome of the programme that is
organized by the nurses, staff-fulfillment may be easily achieved. Nurses may be more
likely to work in their workplace and finally the turnover rate will decrease and increase
the staff morale of the nurses.
42
3.2. Developing evidence base practice guideline
Introduction
The evidence from the reviews studies suggested that active video game weight
reduction programme was an effective innovation for weight reduction in overweight
or obese students, so it is required to develop guidelines for this programme in Hong
Kong.
Users of the guidelines
Registered nurses in the SHSC, center X.
Target Audience
10-18 years old adolescents who attend the SHS in the annual visit with weight for
height ≥ 120% of median weight for height form the sex-specific growth chart by
Hong Kong Growth Survey in 1993 with no medical complication. Also consent
from the parent is required and agree to attend all the sessions of the programme.
Target Setting
43
Health education room in SHSC, center X
Methodology
To criticize the quality of the reviews studies, the critical appraisal tool from Critical
Appraisal Skills Programme (CASP) was used. The level of the evidence was rated by
the guidelines from the Scottish Intercollegiate Guidelines Network (SIGN) that was
attached in Appendix Ⅶ (Scottish Intercollegiate Guidelines Network, 2012).
And the Rating Scheme for the Strength of the Recommendation of SIGN (Attached
in Appendix Ⅷ) was used to rating the grades of the evidence from the reviews
studies to formulate recommendations is the evidence guidelines for the programme.
Clinical Guidelines for the programme
The guidelines was established and attached at the Appendix Ⅸ for providing
guidelines to the nurses in SHSC, center X for implementing active video game for an
innovation to reduce weight among overweight or obese adolescents.
Importance of tackling children’s overweight or obesity and programme components
and benefit to the audience are the main elements in the content of the guidelines. For
44
the importance of tackling children’s overweight or obesity, it includes complication
for overweight or obese in adolescents, elements for control body weight and the
definition of overweight or obesity in children or adolescents. For the programme
components and benefit to the audience, it includes peer or parent in the programme,
encouraging the target audience to sustain performing regular exercise, modifying the
eating habit of the target audience and even promoting active video game into the
home setting environment. The references for establishing the clinical guidelines were
attached on the Appendix Ⅹ.
45
Chapter 4: Implementation Plan
To better implement the proposed intervention to the local setting, a well-designed
implementation plan is required. The communication plan includes identification of
the stakeholders, communication strategies, how to sustain the changes and a pilot
testing.
Chapter 4.1 Communication Plan
I. Stakeholders Identification
To implement the active video game programme for weight reduction among
overweight or obese adolescents successfully, it may require collaboration of different
stakeholders. Therefore, gathering concerns from the stakeholders can help in
understanding what the changes are needed, and how to benefit for the target
population. It is important to convince the stakeholders to support the proposed
innovation, otherwise they may become the obstacles in the implementation process.
The proposed innovation will be conducted in Student Health Service (SHS), center X
which is 1 out of 12 centers in SHS. There are 21 staffs in the center X of SHS
46
including 2 medical officers (MOs), 2 nursing officers (NOs), 6 registered nurses
(RNs), 3 enrolled nurses (ENs), 4 clerical staffs and 4 workmen. Their duties are
providing quality of service to monitor the growth and psychological health for the
students. The stakeholders of the proposed innovation are senior medical officer
(SMO) and senior nursing officers (SNOs) in headquarter of SHS, NOs, MOs and
RNs in center X, the overweight or obese students who attend the annual checkup of
the center X and their parents. It is necessary to know the concerns of each
stakeholders and creating a well communication strategies to initiate and sustain the
changes.
II. Communication strategies to initiate change
The programme proposer should create the communication strategies to gain the
support from the stakeholders. To facilitate the communication, a communication
team should be built up as the following orders.
1. Center Administrators (NOs & NOs in the center X of SHS)
The programme proposer is one of the RN in the center X of SHS, she realizes that
47
there is a need to change the current practice for managing overweight or obese
students. To implement the programme to the center X, she should achieve the
support from center administrators. Firstly, an informal meeting would be set up
for them. Programme proposer would briefly introduce seriousness of the situation
among overweight or obese students in Hong Kong, the disadvantages of the
current strategies for managing the overweight or obese students by simply
providing health education talks or diet counseling by dietitian. For better
understanding the proposed intervention, the characteristic of the intervention, the
programme protocol, timeframe of the programme, manpower and resources of the
innovation and any disturbance of the routine service would be explained. After
obtaining the support by them, a communication team including MOs, NOs and
programme proposer would be formed. The role of the team would facilitate the
communication between different stakeholders and implement the proposed
programme smoothly.
2. Senior Administrators (SMO & SNOs) in headquarter
After obtaining the support from the MOs & NOs in the center X of SHS, it was
48
necessary to get the permission from the senior administrators, the proposed
innovation could not be implemented without their approval. The MOs and NOs
from the communication team will present the proposed innovation with the senior
administrator to get their approval and support by regular senior staffs meeting.
During the presentation, they will state the rationale, timeframe, guidelines and
content of the programme clearly. Since some equipment is needed and training
sessions are required on Saturday for the programme implementers, approval from
the senior staffs must be obtained. Therefore the proposer has resources to spend
on the expenses and compensation time-off could be granted for the implementers.
3. Programme implementers (RNs from the center X of SHS)
After gaining the support and approval by the senior administrators, the
implementers who are registered nurses (RNs) in the center X of SHS will be
notified. An informal meeting will be held to discuss why change is needed, the
effectiveness of the programme and whether there is extra workload for them. A
comprehensive manual including
1. The programme guidelines
49
2. Research studies about the proposed intervention
3. The background information of overweight or obese student in Hong Kong
4. The timeframe of the programme
5. The table of evidence
6. The nursing audit chart
Will be provided. Furthermore, a training session for implementers will be held in
non-office hour to equip themselves for better operating the active video game
console and compensation time-off will be given to them. Therefore it might
enhance their acceptance and lower the obstacle for programme implementation.
4. Parents of the overweight or obese students
The parents’ support and consent for the overweight and obese students’
participation in the programme is a must. A programme leaflet will be given to the
eligible parents, so they can better understand the aim and effectiveness of the
programme, the time schedule of the programme and application procedures.
50
Ⅲ. Communication strategies to sustain change
A pilot test will be held before fully-implementation of the proposed progamme.
Therefore, gathering the feedback from the stakeholders can understand any weakness
of the programme design and make further improvement on the contents and
guidelines. To monitor the compliance for applying the programme guidelines by the
implementers and whether they have sufficient skills to instruct the eligible students,
the NOs in the center X will act as an internal auditor for quality assurance of the
programme by nursing audit chart. The chart includes whether the implementers
follow the guidelines and timeframe of the programme. For the outcome measure will
be the overweight status and increase the time spending on performing regular
exercise of the eligible students.
A sharing session will be held in each month of the center meeting. The proposer can
gather all the feedback from the implementers. Finally, a report including the
compliance of the implementers, feedback from them and the outcome evaluation of
the programme can be generated. Revision of the programme guidelines and contents
can be made based on that evidence.
51
Finally, the report and successful cases can share in the formal senior administrator
meeting by MOs or NOs, the senior administrators can know the feasibility to fully
implement the programme.
Chapter 4.2 Pilot study plan
A pilot study is a preliminary study for a small group of participants before fully
implementing the programme in a real setting. Therefore the proposer can gather all
the data from the pilot study to identify the weakness and feasible to be promoted in
real setting. Improvement can be made before full-scale implementation of the
programme.
1. Objectives of the pilot proposed programme
a. Having knowledge, skills or being confident to perform the programme by
implementers
b. Implementer’s satisfaction on the programme content and guidelines
c. Eligible students and their parent satisfaction of the programme
52
2. Programme protocol & characteristic of the eligible students of the pilot proposed
programme
The pilot weight reduction active video game programme is for overweight or
obese students in the center X. The target students for the pilot programme will be
the overweight or obese students who are weight ≥ 120% weight for height from
Hong Kong Growth Survey in 1993 (Departement of Health, 2012). 10 eligible
students will be recruited during the annual checkup by MOs or RNs after
obtaining the consent by their parent. Also, the eligible students should not have
any medical complication, follow-up in any specialty or participating any weight
reduction programme at the same time. For the pilot programme, it will last for 8
weeks with 1-hour session per week and conducted by RNs in the center X. RNs
will briefly introduce how to eat healthy and instruct the eligible students how to
use the active video game console appropriately.
The body weight (BW), body height (BH) and the waist circumference (WC) will
be measured in biweekly. Finally, body mass index (BMI) of the students can be
calculated and compared at the end of the pilot programme. Besides that the time
53
on spending to perform regular exercise of the students will be collected by asking
their parent via phone biweekly.
3. Measurements
Three types of measurements will be collected during and at the end of the pilot
programme.
a. Knowledge of the programme implementers
It is important to know whether the nurses have enough skills or knowledge to
implement the programme. To ensure the competency of the pilot programme,
the proposer or NOs in the center X should assess them by using self-
administered questionnaire. The questionnaire may cover the knowledge of
how to eat healthy and properly, skills on using active video game console,
how to instruct the participants performing the active video game exercise
safely. A refreshment training will be given to the nurses who are classified as
unsatisfaction to perform the programme.
54
b. Staff satisfaction on using the programme protocol or guidelines
A formal meeting will be held after the pilot programme to assess the
satisfaction and the confidence of the nurses on using the programme protocol.
All the nurses will be invited to attend the meeting and some questions will be
asked during the meeting:
i. What were the difficulties during implementation of the programme?
ii. Which part of the programme or programme protocol can be improved and
will you recommend to others?
c. Parents & eligible participants satisfaction on attending the pilot programme
The satisfaction of the eligible participants and their parents are the concern of
the pilot programme too. A sharing session will be held after the programme
and collection their opinions.
4.3 Evaluation Plan
After gathering the evidence for revised the contents of the progranmme, it can be
fully implemented in the center X of SHS. It is necessary to identify the outcomes of
55
the progamme whether considering being effectiveness. Three aspects are included in
outcome evaluation.
Ⅰ. Outcome Evaluation
1. Patient outcomes
To evaluate the programme outcomes, body mass index (BMI) and time spending
on performing exercise will be measured. BMI was used as an outcome measure
in the previous studies for assessing the effectiveness of active video game for
weight reduction (Maddison, et al., 2012 & Trost, et al., 2014). The effectiveness
of the programme can be decided by observing the change of BMI. Performing
regular exercise is a method to good control of the BW, the evidence had already
shown that active video game encouraged the students to increase time to perform
exercise. (Trost et al., 2014 & Adamo, et al., 2010). Therefore a chart for
documenting the time on performs exercise daily will be given to the students.
And they need to complete and hand it at the end of the programme.
2. Health care provider outcomes
The NOs in the center X will be the internal auditor to assure the nurses whether
56
they follow the programme proctocol and provide good quality of care to the
participants. A nursing audit chart will be created to assess the compliance of the
nurses. The critical points of the programme protocols and some instructions or
skill supposed to be performed during the programme by the implementers are
included in the chart. The auditor will have on-site observation and staff interview
during or after the pilot programme. Comments and refreshment training will be
given to the unqualified nurses.
3. System outcomes
For the usual practice for handling overweight or obese adolescents in the center
X, health counseling by nurses, physical examination by the doctors, diet
counseling by the dietitian is used. To assess the effectiveness of the programme
to the current setting, the waiting time to counsel doctors for physical checkup,
diet counseling by the dietitian and costs for recruiting for more dietitians or
doctors can be measured. Besides that the sick leave rate of the staffs can be
observed too, the proposer can know whether there is positive or negative impact
for the frontline staffs after implementing the programme.
57
Ⅱ. Determination the time for measuring the outcomes
The duration of the innovation in the programme will be lasted for 16 weeks. For the
integrated reviews studies, the effectiveness of the innovation would be seen between
6 to 10 weeks. To be conservative, 8 and 16 week will be considered as the time for
measuring the immediate outcomes. For evaluation of the long-term outcome for the
programme, the next annual check-up which is 12 month after the programme will be
considered. The baseline information of the paritcipants should be measured at the
first session of the programme to compare the effect of the programme.
Ⅲ. Criteria and recruitment for the eligible students
The criteria for the eligible students are the same as the pilot programme. 10-18 years
old adolescents who attend the SHS in the annual visit with body weight ≥ 120% of
median weight for height form the sex-specific growth chart by Hong Kong Growth
Survey in 1993 (Department of Health, 2012). And consents should be obtained from
their parent. The eligible participants should not have any medical complication,
follow-up in any specialty or participating in any weight reduction programme.
58
Ⅳ. Data analysis and sample size calculation
The primary outcome of the programme is weight reduction among overweight or
obese participants. BMI will be used for observing the change of the overweight or
obese status of the participants. Therefore, BW and BH will be measured at baseline,
week 8, week 16 and 12 month by using electronic stadiometer in the center X.
Convenience sampling will be used to recruitment during the annual checkup by
nurses or doctors. It is important to have adequate sample size for the programme.
Two-tail t-test will be used as the method to calculate the sample size of the
participants.
The computer software of Java Applets for Power and Sample Size will be used
(Lenth, 2006-9). Level of significance and power will be set as 0.05 and 80%
respectively based on the conventional standard in most studies. From one of the
reviews studies with significant result for weight reduction among participants, effect
size can be considered as 0.8, sigma can be as 2.0 (Maddison, et al., 2012). Finally,
sample size of 51 is estimated. To consider of having 20% dropout rate, 62 of the
samples are required.
59
Chapter 4.4 The basis for Implementation
To consider the effectiveness of the programme, the main outcomes are needed to be
achieved which are reducing BMI: 0.19 among overweight or obese students
(Maddison, et al., 2012 & Trost, et al., 2014) and increasing the time of 10 minutes
per day on performing regular exercise (Trost, et al, 2014 & Adamo, et al., 2010). If
the programme is considered to be effective, it can fully promote to 12 centers in
SHS, hopefully it can have 10% of the eligible participants join the programme. It can
shorten the waiting time for diet counseling by dietitian or physical checkup by
doctors. Furthermore, increasing the utilization of the programme can lower the cost
per each student for participating the programme.
Higher acceptance rate of the programme and more staffs are supporting for it.
Finally, the programme is said to be effective and can be promoted to 12 centers of
SHS
60
Appendix I. Table of Evidence 1a
Bibliographic
citation
Study
design
Patient
Characteristics
Intervention(s)
Comparison
Length of
Follow up
Outcome
measures
Effect Size
Maddison et
al., 2012
Two-arm
parallel
RCT
-10-14year old
overweight or
obese children
-owned a
PlayStation® 2 or
3 gaming console
but no active
video games
-played video
games ≧ 2hrs/wk
-Plating active video
game by Sony
PlayStation® EyeToy
active video games at
home
-encourage to meet
current physical
activity
recommendations (60
mins/day MVPA)
(n=160)
-continuing for
their normal video
game play
(n=162)
12 & 24
wks
Primary
(1) change from baseline
in BMI (kh/m2)
Secondary
(2) change from baseline
in body fat (%)
(3) WC (cm)
(4) Physical fitness (VO2
max)
(Intervention – Control)
(1) -0.24 (95% CI -.044 to
-0.04), p=0.02
(2) -0.83 (95% CI -1.54 to
-0.12), p=0.02
(3) -1.21 (95% CI -2.54 to
0.03), p=0.22
(4) 0.58 (95% CI -0.34 to
1.49), p=0.60
Trost et al.,
2014
RCT -BMI > 85th
percentile for sex
& age
-8-12 year old
-parent &
guardian
participate in
weekly treatment
sessions
-received a
comprehensive
family-based pediatric
weight programme
(JOIN for me)
-provide a game
console & motion
capture device &
active sports game
(n=34)
- received a
comprehensive
family-based
pediatric weight
programme (JOIN
for me)
(n-41)
8 & 16
wks
(1) BMI z score
(2) mean weight loss (kg)
(3) Percentage overweight
(%)
(4)MVPA (min/day)
(5) VPA (min/day)
(Intervention – Control)
(1) net difference: 0.14,
p< 0.001
(2) net difference:0.35
(3) net difference:5.4,
p=0.02
(4) net difference:8,
p=0.04
(5) net difference:3.1,
p=0.02
61
Appendix I. Table of Evidence 1b
Bibliographic
citation
Study
design
Patient
Characteristics
Intervention(s)
Comparison
Length of
Follow up
Outcome
measures
Effect Size
Adamo, et al.,
2010
RCT - 12-17 years old
with BMI > 95th
percentile or
- 12-17 years old
with BMI > 85th
percentile with at
least 1 medical
complication
-Interactive video
game cycling on a
GameBike for
twice/wk
(60mins/session)
(n=13)
--stationary
cycling to music
on a GameBike
with the fame
console turned off
twice/wk
(n=13)
10 wks
Body composition:
(1) BW (kg)
(2) BMI (kg/m2)
(3) Fat mass
(4) Fat free mass
(5) WC (cm)
Exercise behavior
(6) time spending on
vigorous, intensity
exercise (min/session)
(1)-(5) non significant
(6) (Intervention –
Contorl)
-11.2 + -7.2 (p=0.05)
Staiano, et al.,
2013.
RCT -15-19 years old
- BMI ≧ 75th
percentile
(1)competitive exergame
(competed against a peer)
by Nitendo Wii Active
exergame 30-60
min/school day (n=19)
(2)cooperative exergame
(cooperated with a
partner) by Nintendo
Will Active exergame 30-
60 min / school day
(n=19)
Usual daily
activities eg.
Tutoring/ sport
team practice
(n=16)
10 & 20
wks
(1) BMI (hg/m2)
(2) BW (kg)
(1) p=0.239
(2)(Cooperative-control)
-2.51, p=0.021
(Competitive-control)
non significant
62
Appendix I. Table of evidence 1c
Abbreviation: BMI(body mass index), MVPA(moderate to vigorous physical activity), VPA(vigorous physical activity), WC(waist circumference),
BW(body weight), RCT(Randomized Controlled Trial)
Bibliographic
citation
Study
design
Patient
Characteristics
Intervention(s)
Comparison
Length of
Follow up
Outcome
measures
Effect Size
Ni Mhurchu,
et al., 2008
RCT - 10-14 years old
mean: 12
-owned a
PlayStation® 2
console
-English speaking
-Informed
consent obtained
by parent
Playing active video
game (EyeToy &
dance mat)
(n=10)
No intervention 6 & 12
wks
Primary outcome
(1) BW (kg)
(2) WC (cm)
Secondary outcome
(3) time of active video
game playing (min)
(4) physical activity level
(counts/min)
(Intervention - Control)
(1)-0.13 (95% Ci -1.97,
1.7) p=0.9
(2) -1.4 (95% CI -2.68,
-.04) p=0.04
(3)14 (95% CI -15, 42)
p=0.3
(4) In wk 6
194 (95% CI 32, 310)
p=0.04
63 Appendix II
File name : Checklist 2 – Controlled Trials Version 2.0 28/05/2012
Produced by: Carolyn Sleith Page 63 of 93
Review date: None
S I G N
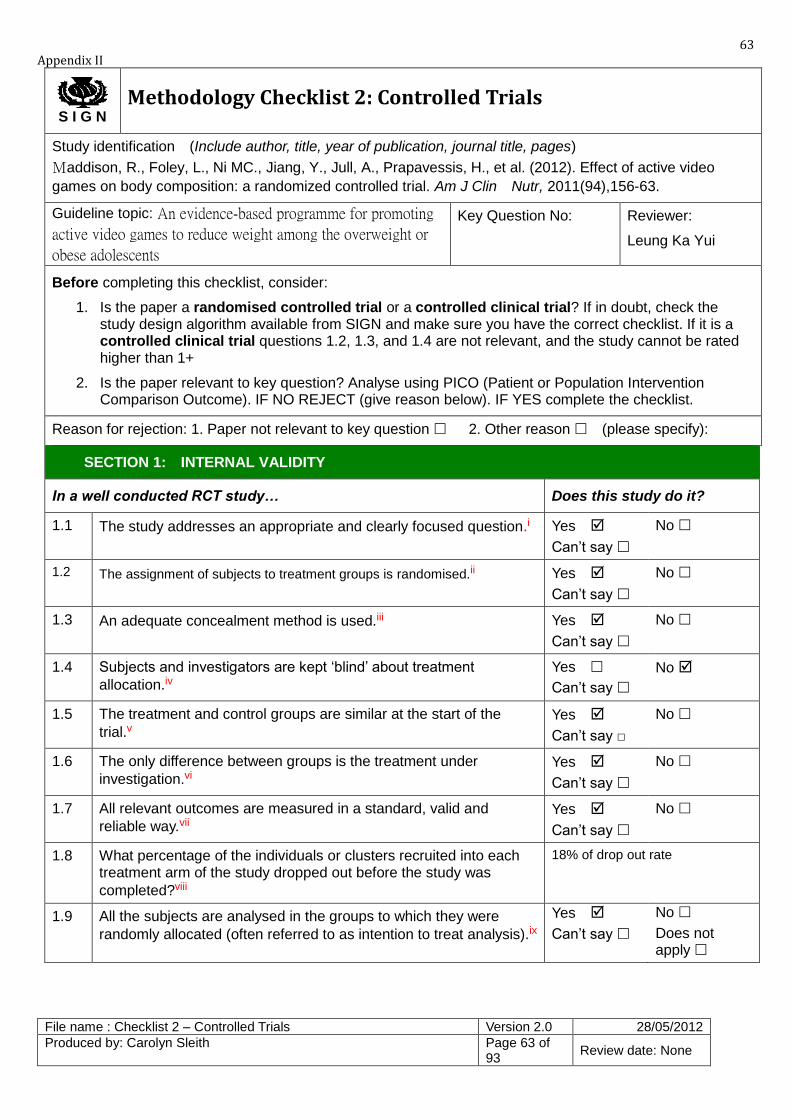
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Maddison, R., Foley, L., Ni MC., Jiang, Y., Jull, A., Prapavessis, H., et al. (2012). Effect of active video
games on body composition: a randomized controlled trial. Am J Clin Nutr, 2011(94),156-63.
Guideline topic: An evidence-based programme for promoting
active video games to reduce weight among the overweight or
obese adolescents
Key Question No: Reviewer:
Leung Ka Yui
Before completing this checklist, consider:
1. Is the paper a randomised controlled trial or a controlled clinical trial? If in doubt, check the study design algorithm available from SIGN and make sure you have the correct checklist. If it is a controlled clinical trial questions 1.2, 1.3, and 1.4 are not relevant, and the study cannot be rated higher than 1+
2. Is the paper relevant to key question? Analyse using PICO (Patient or Population Intervention Comparison Outcome). IF NO REJECT (give reason below). IF YES complete the checklist.
Reason for rejection: 1. Paper not relevant to key question 2. Other reason (please specify):
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.i
Yes
Can’t say
No
1.2 The assignment of subjects to treatment groups is randomised.ii
Yes
Can’t say
No
1.3 An adequate concealment method is used.iii
Yes
Can’t say
No
1.4 Subjects and investigators are kept ‘blind’ about treatment
allocation.iv
Yes
Can’t say
No
1.5 The treatment and control groups are similar at the start of the
trial.v
Yes
Can’t say □
No
1.6 The only difference between groups is the treatment under
investigation.vi
Yes
Can’t say
No
1.7 All relevant outcomes are measured in a standard, valid and
reliable way.vii
Yes
Can’t say
No
1.8 What percentage of the individuals or clusters recruited into each treatment arm of the study dropped out before the study was
completed?viii
18% of drop out rate
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat analysis).ix
Yes
Can’t say
No
Does not apply
64
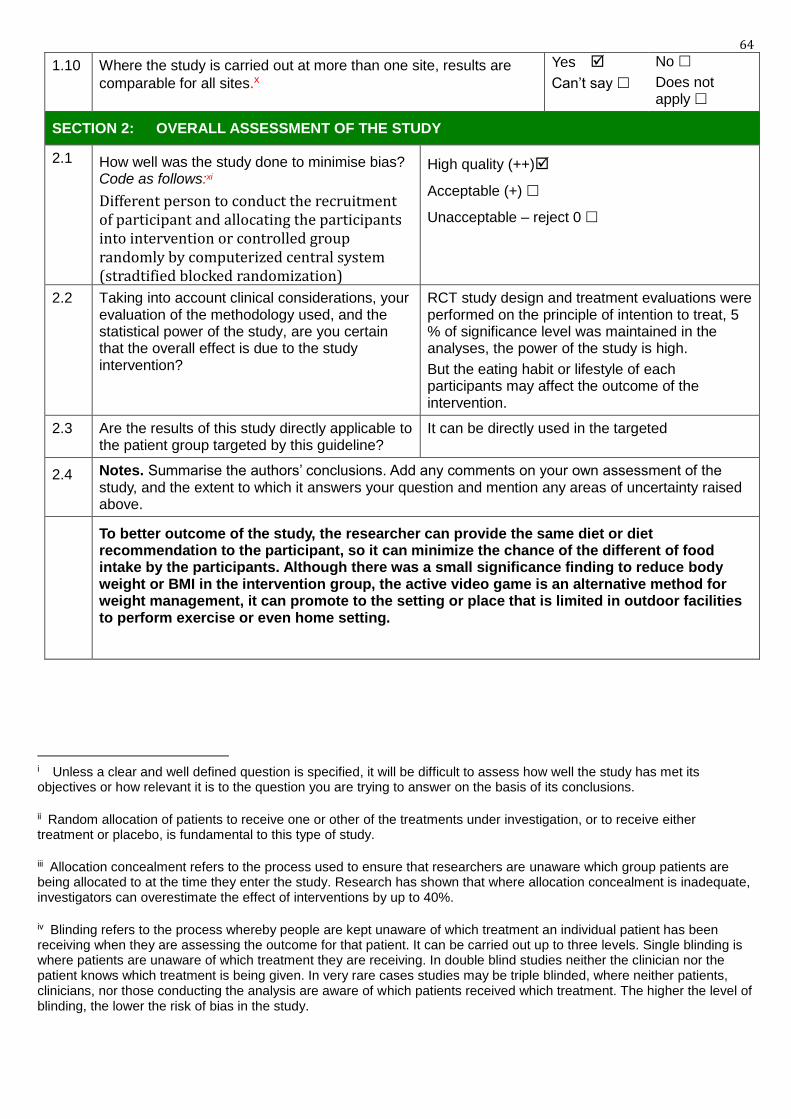
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.x
Yes
Can’t say
No
Does not apply
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias? Code as follows:xi
Different person to conduct the recruitment of participant and allocating the participants into intervention or controlled group randomly by computerized central system (stradtified blocked randomization)
High quality (++)
Acceptable (+)
Unacceptable – reject 0
2.2 Taking into account clinical considerations, your evaluation of the methodology used, and the statistical power of the study, are you certain that the overall effect is due to the study intervention?
RCT study design and treatment evaluations were performed on the principle of intention to treat, 5 % of significance level was maintained in the analyses, the power of the study is high.
But the eating habit or lifestyle of each participants may affect the outcome of the intervention.
2.3 Are the results of this study directly applicable to the patient group targeted by this guideline?
It can be directly used in the targeted
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to which it answers your question and mention any areas of uncertainty raised above.
To better outcome of the study, the researcher can provide the same diet or diet recommendation to the participant, so it can minimize the chance of the different of food intake by the participants. Although there was a small significance finding to reduce body weight or BMI in the intervention group, the active video game is an alternative method for weight management, it can promote to the setting or place that is limited in outdoor facilities to perform exercise or even home setting.
i Unless a clear and well defined question is specified, it will be difficult to assess how well the study has met its objectives or how relevant it is to the question you are trying to answer on the basis of its conclusions.
ii Random allocation of patients to receive one or other of the treatments under investigation, or to receive either treatment or placebo, is fundamental to this type of study.
iii Allocation concealment refers to the process used to ensure that researchers are unaware which group patients are being allocated to at the time they enter the study. Research has shown that where allocation concealment is inadequate, investigators can overestimate the effect of interventions by up to 40%.
iv Blinding refers to the process whereby people are kept unaware of which treatment an individual patient has been receiving when they are assessing the outcome for that patient. It can be carried out up to three levels. Single blinding is where patients are unaware of which treatment they are receiving. In double blind studies neither the clinician nor the patient knows which treatment is being given. In very rare cases studies may be triple blinded, where neither patients, clinicians, nor those conducting the analysis are aware of which patients received which treatment. The higher the level of blinding, the lower the risk of bias in the study.
65
v Patients selected for inclusion in a trial must be as similar as possible. The study should report any significant differences in the composition of the study groups in relation to gender mix, age, stage of disease (if appropriate), social background, ethnic origin, or co-morbid conditions. These factors may be covered by inclusion and exclusion criteria, rather than being reported directly. Failure to address this question, or the use of inappropriate groups, should lead to the study being downgraded.
vi If some patients received additional treatment, even if of a minor nature or consisting of advice and counselling rather than a physical intervention, this treatment is a potential confounding factor that may invalidate the results. If groups were not treated equally, the study should be rejected unless no other evidence is available. If the study is used as evidence it should be treated with caution.
vii The primary outcome measures used should be clearly stated in the study. If the outcome measures are not stated, or the study bases its main conclusions on secondary outcomes, the study should be rejected. Where outcome measures require any degree of subjectivity, some evidence should be provided that the measures used are reliable and have been validated prior to their use in the study.
viii The number of patients that drop out of a study should give concern if the number is very high. Conventionally, a 20% drop out rate is regarded as acceptable, but this may vary. Some regard should be paid to why patients dropped out, as well as how many. It should be noted that the drop out rate may be expected to be higher in studies conducted over a long period of time. A higher drop out rate will normally lead to downgrading, rather than rejection of a study.
ix In practice, it is rarely the case that all patients allocated to the intervention group receive the intervention throughout the trial, or that all those in the comparison group do not. Patients may refuse treatment, or contra-indications arise that lead them to be switched to the other group. If the comparability of groups through randomisation is to be maintained, however, patient outcomes must be analysed according to the group to which they were originally allocated irrespective of the treatment they actually received. (This is known as intention to treat analysis.) If it is clear that analysis was not on an intention to treat basis, the study may be rejected. If there is little other evidence available, the study may be included but should be evaluated as if it were a non-randomised cohort study.
x In multi-site studies, confidence in the results should be increased if it can be shown that similar results were obtained at the different participating centres.
xi Rate the overall methodological quality of the study, using the following as a guide: High quality (++): Majority of criteria met. Little or no risk of bias. Results unlikely to be changed by further research. Acceptable (+): Most criteria met. Some flaws in the study with an associated risk of bias, Conclusions may change in the light of further studies. Low quality (0): Either most criteria not met, or significant flaws relating to key aspects of study design. Conclusions likely to change in the light of further studies.
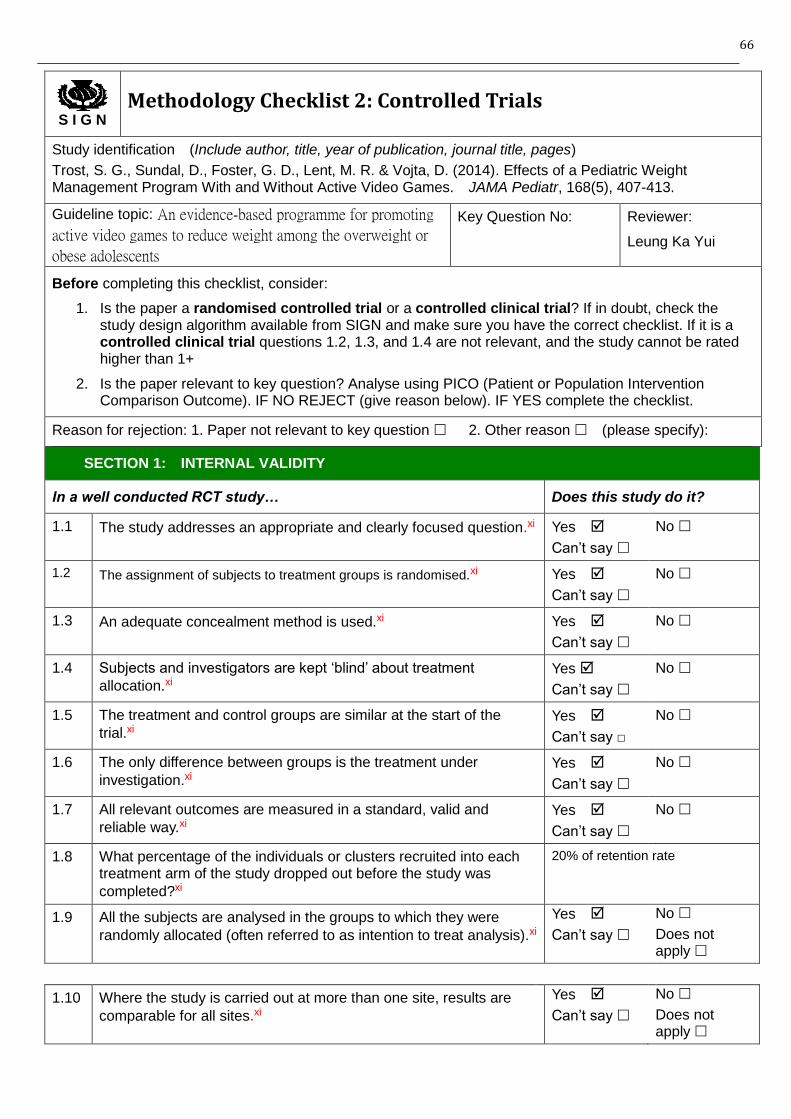
66
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Trost, S. G., Sundal, D., Foster, G. D., Lent, M. R. & Vojta, D. (2014). Effects of a Pediatric Weight Management Program With and Without Active Video Games. JAMA Pediatr, 168(5), 407-413.
Guideline topic: An evidence-based programme for promoting
active video games to reduce weight among the overweight or
obese adolescents
Key Question No: Reviewer:
Leung Ka Yui
Before completing this checklist, consider:
1. Is the paper a randomised controlled trial or a controlled clinical trial? If in doubt, check the study design algorithm available from SIGN and make sure you have the correct checklist. If it is a controlled clinical trial questions 1.2, 1.3, and 1.4 are not relevant, and the study cannot be rated higher than 1+
2. Is the paper relevant to key question? Analyse using PICO (Patient or Population Intervention Comparison Outcome). IF NO REJECT (give reason below). IF YES complete the checklist.
Reason for rejection: 1. Paper not relevant to key question 2. Other reason (please specify):
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.xi
Yes
Can’t say
No
1.2 The assignment of subjects to treatment groups is randomised.xi
Yes
Can’t say
No
1.3 An adequate concealment method is used.xi
Yes
Can’t say
No
1.4 Subjects and investigators are kept ‘blind’ about treatment
allocation.xi
Yes
Can’t say
No
1.5 The treatment and control groups are similar at the start of the
trial.xi
Yes
Can’t say □
No
1.6 The only difference between groups is the treatment under
investigation.xi
Yes
Can’t say
No
1.7 All relevant outcomes are measured in a standard, valid and
reliable way.xi
Yes
Can’t say
No
1.8 What percentage of the individuals or clusters recruited into each treatment arm of the study dropped out before the study was
completed?xi
20% of retention rate
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat analysis).xi
Yes
Can’t say
No
Does not apply
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.xi
Yes
Can’t say
No
Does not apply
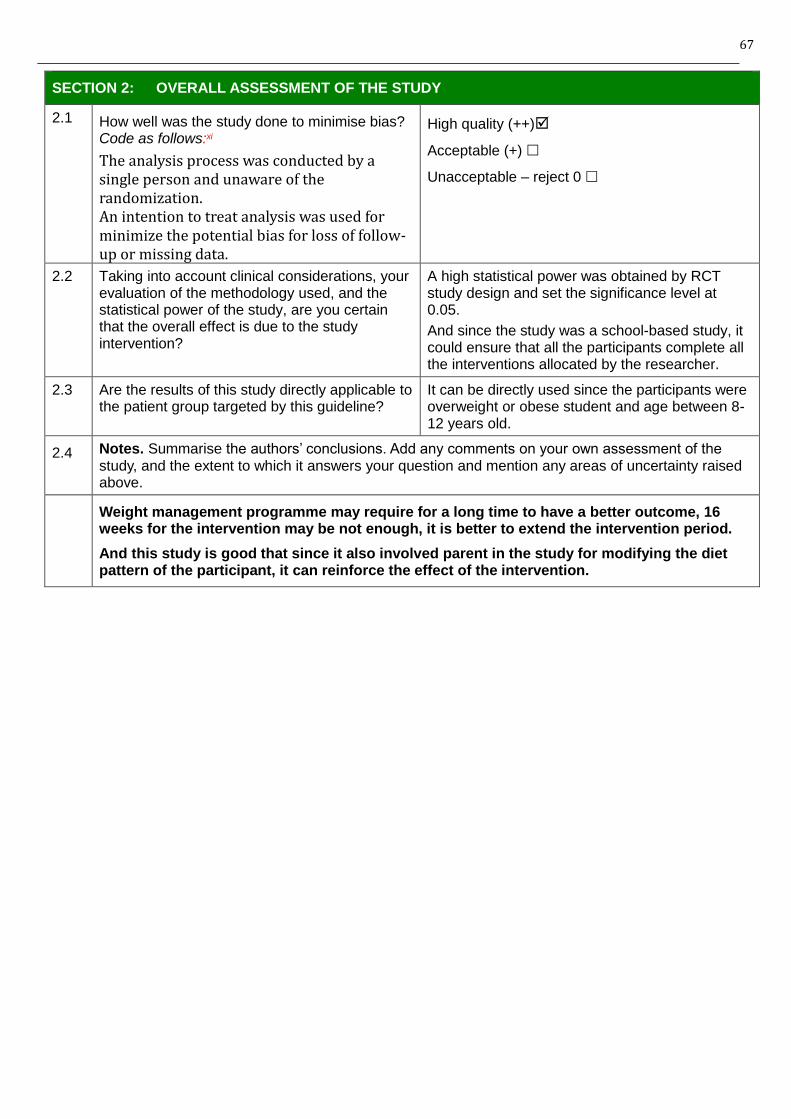
67
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias? Code as follows:xi
The analysis process was conducted by a single person and unaware of the randomization. An intention to treat analysis was used for minimize the potential bias for loss of follow-up or missing data.
High quality (++)
Acceptable (+)
Unacceptable – reject 0
2.2 Taking into account clinical considerations, your evaluation of the methodology used, and the statistical power of the study, are you certain that the overall effect is due to the study intervention?
A high statistical power was obtained by RCT study design and set the significance level at 0.05.
And since the study was a school-based study, it could ensure that all the participants complete all the interventions allocated by the researcher.
2.3 Are the results of this study directly applicable to the patient group targeted by this guideline?
It can be directly used since the participants were overweight or obese student and age between 8-12 years old.
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to which it answers your question and mention any areas of uncertainty raised above.
Weight management programme may require for a long time to have a better outcome, 16 weeks for the intervention may be not enough, it is better to extend the intervention period.
And this study is good that since it also involved parent in the study for modifying the diet pattern of the participant, it can reinforce the effect of the intervention.
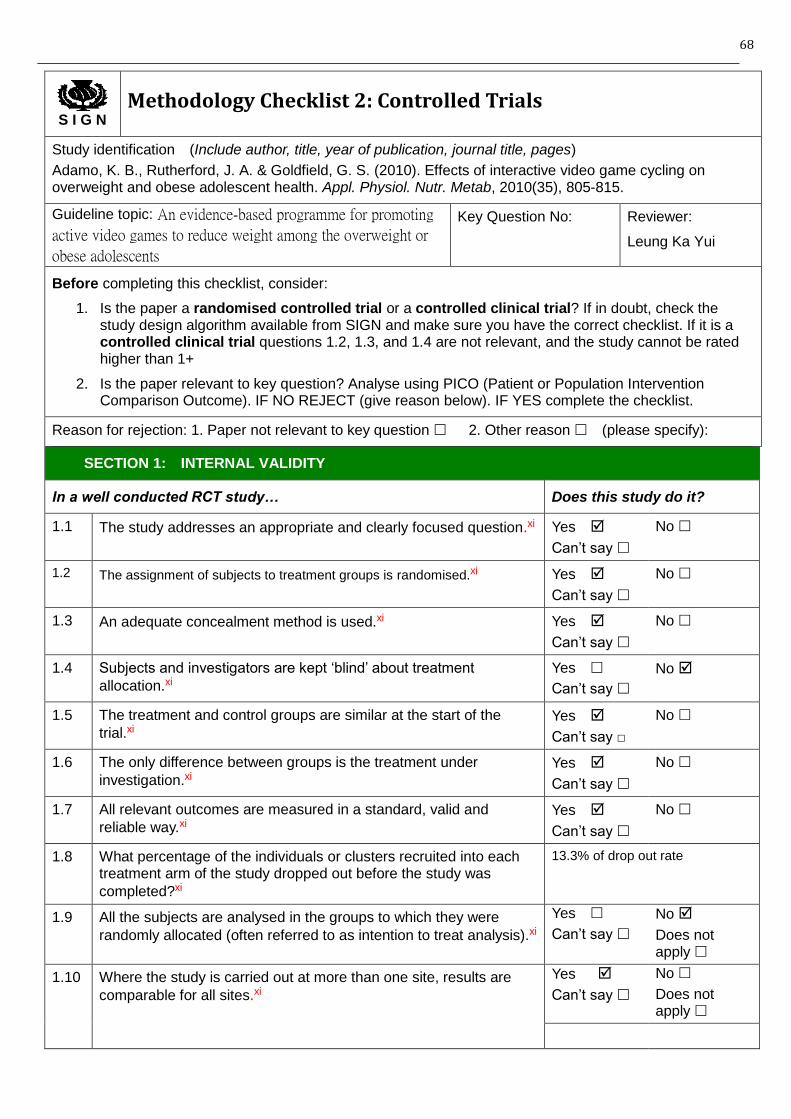
68
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Adamo, K. B., Rutherford, J. A. & Goldfield, G. S. (2010). Effects of interactive video game cycling on overweight and obese adolescent health. Appl. Physiol. Nutr. Metab, 2010(35), 805-815.
Guideline topic: An evidence-based programme for promoting
active video games to reduce weight among the overweight or
obese adolescents
Key Question No: Reviewer:
Leung Ka Yui
Before completing this checklist, consider:
1. Is the paper a randomised controlled trial or a controlled clinical trial? If in doubt, check the study design algorithm available from SIGN and make sure you have the correct checklist. If it is a controlled clinical trial questions 1.2, 1.3, and 1.4 are not relevant, and the study cannot be rated higher than 1+
2. Is the paper relevant to key question? Analyse using PICO (Patient or Population Intervention Comparison Outcome). IF NO REJECT (give reason below). IF YES complete the checklist.
Reason for rejection: 1. Paper not relevant to key question 2. Other reason (please specify):
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.xi
Yes
Can’t say
No
1.2 The assignment of subjects to treatment groups is randomised.xi
Yes
Can’t say
No
1.3 An adequate concealment method is used.xi
Yes
Can’t say
No
1.4 Subjects and investigators are kept ‘blind’ about treatment
allocation.xi
Yes
Can’t say
No
1.5 The treatment and control groups are similar at the start of the
trial.xi
Yes
Can’t say □
No
1.6 The only difference between groups is the treatment under
investigation.xi
Yes
Can’t say
No
1.7 All relevant outcomes are measured in a standard, valid and
reliable way.xi
Yes
Can’t say
No
1.8 What percentage of the individuals or clusters recruited into each treatment arm of the study dropped out before the study was
completed?xi
13.3% of drop out rate
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat analysis).xi
Yes
Can’t say
No
Does not apply
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.xi
Yes
Can’t say
No
Does not apply
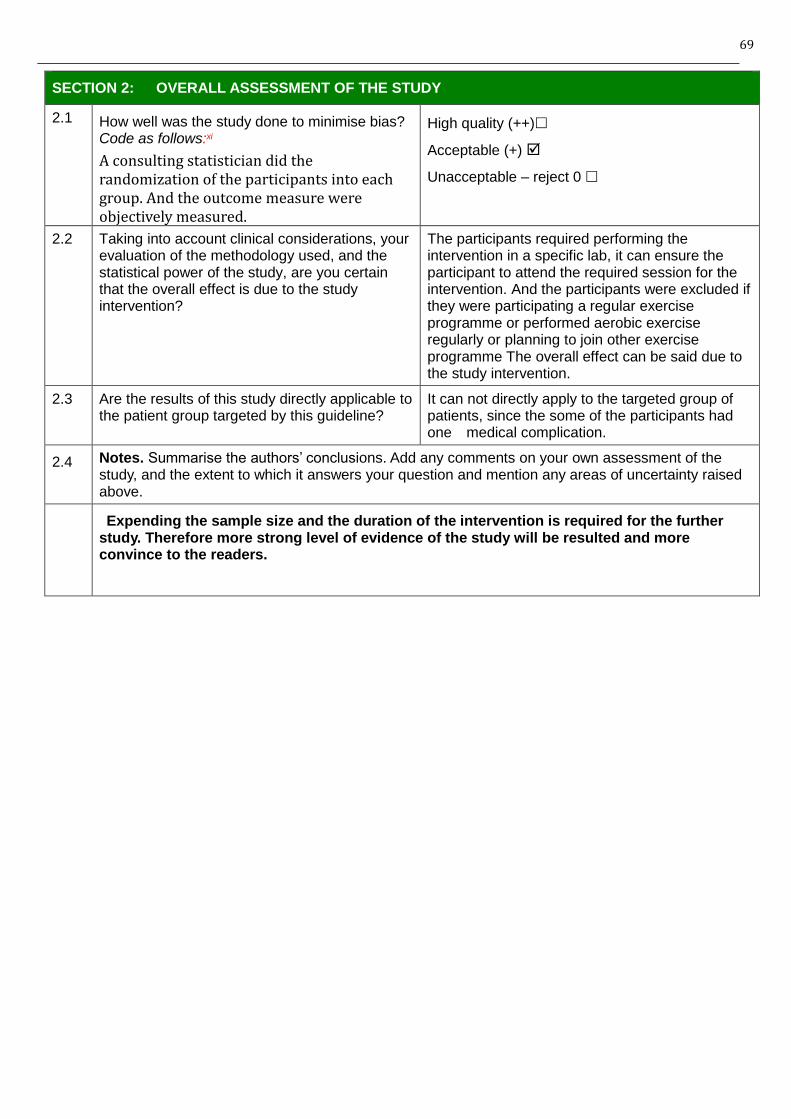
69
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias? Code as follows:xi
A consulting statistician did the randomization of the participants into each group. And the outcome measure were objectively measured.
High quality (++)
Acceptable (+)
Unacceptable – reject 0
2.2 Taking into account clinical considerations, your evaluation of the methodology used, and the statistical power of the study, are you certain that the overall effect is due to the study intervention?
The participants required performing the intervention in a specific lab, it can ensure the participant to attend the required session for the intervention. And the participants were excluded if they were participating a regular exercise programme or performed aerobic exercise regularly or planning to join other exercise programme The overall effect can be said due to the study intervention.
2.3 Are the results of this study directly applicable to the patient group targeted by this guideline?
It can not directly apply to the targeted group of patients, since the some of the participants had one medical complication.
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to which it answers your question and mention any areas of uncertainty raised above.
Expending the sample size and the duration of the intervention is required for the further study. Therefore more strong level of evidence of the study will be resulted and more convince to the readers.
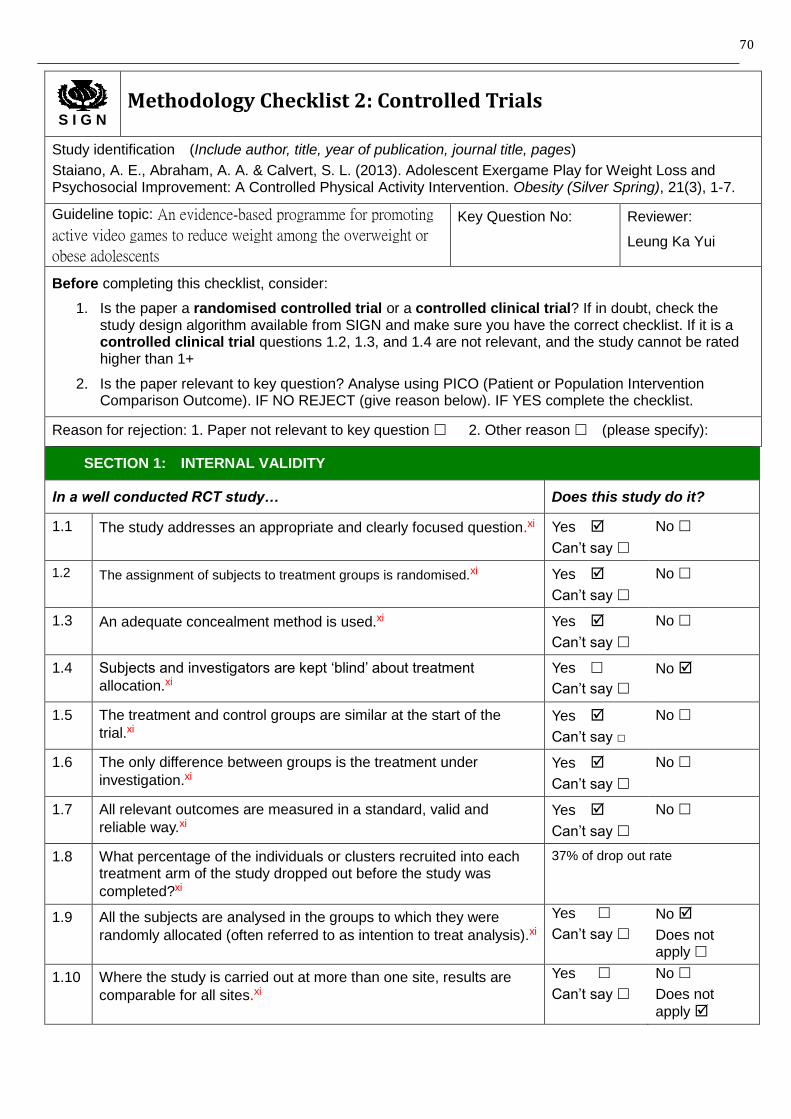
70
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Staiano, A. E., Abraham, A. A. & Calvert, S. L. (2013). Adolescent Exergame Play for Weight Loss and Psychosocial Improvement: A Controlled Physical Activity Intervention. Obesity (Silver Spring), 21(3), 1-7.
Guideline topic: An evidence-based programme for promoting
active video games to reduce weight among the overweight or
obese adolescents
Key Question No: Reviewer:
Leung Ka Yui
Before completing this checklist, consider:
1. Is the paper a randomised controlled trial or a controlled clinical trial? If in doubt, check the study design algorithm available from SIGN and make sure you have the correct checklist. If it is a controlled clinical trial questions 1.2, 1.3, and 1.4 are not relevant, and the study cannot be rated higher than 1+
2. Is the paper relevant to key question? Analyse using PICO (Patient or Population Intervention Comparison Outcome). IF NO REJECT (give reason below). IF YES complete the checklist.
Reason for rejection: 1. Paper not relevant to key question 2. Other reason (please specify):
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.xi
Yes
Can’t say
No
1.2 The assignment of subjects to treatment groups is randomised.xi
Yes
Can’t say
No
1.3 An adequate concealment method is used.xi
Yes
Can’t say
No
1.4 Subjects and investigators are kept ‘blind’ about treatment
allocation.xi
Yes
Can’t say
No
1.5 The treatment and control groups are similar at the start of the
trial.xi
Yes
Can’t say □
No
1.6 The only difference between groups is the treatment under
investigation.xi
Yes
Can’t say
No
1.7 All relevant outcomes are measured in a standard, valid and
reliable way.xi
Yes
Can’t say
No
1.8 What percentage of the individuals or clusters recruited into each treatment arm of the study dropped out before the study was
completed?xi
37% of drop out rate
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat analysis).xi
Yes
Can’t say
No
Does not apply
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.xi
Yes
Can’t say
No
Does not
apply
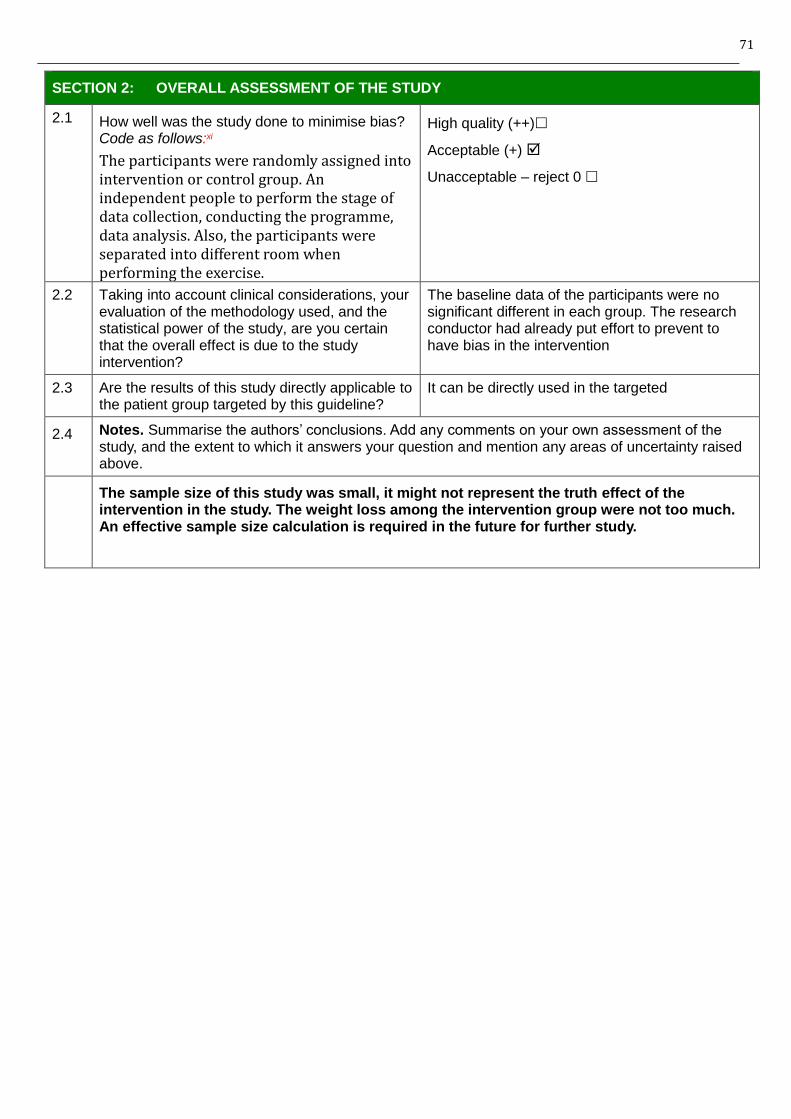
71
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias? Code as follows:xi
The participants were randomly assigned into intervention or control group. An independent people to perform the stage of data collection, conducting the programme, data analysis. Also, the participants were separated into different room when performing the exercise.
High quality (++)
Acceptable (+)
Unacceptable – reject 0
2.2 Taking into account clinical considerations, your evaluation of the methodology used, and the statistical power of the study, are you certain that the overall effect is due to the study intervention?
The baseline data of the participants were no significant different in each group. The research conductor had already put effort to prevent to have bias in the intervention
2.3 Are the results of this study directly applicable to the patient group targeted by this guideline?
It can be directly used in the targeted
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to which it answers your question and mention any areas of uncertainty raised above.
The sample size of this study was small, it might not represent the truth effect of the intervention in the study. The weight loss among the intervention group were not too much. An effective sample size calculation is required in the future for further study.
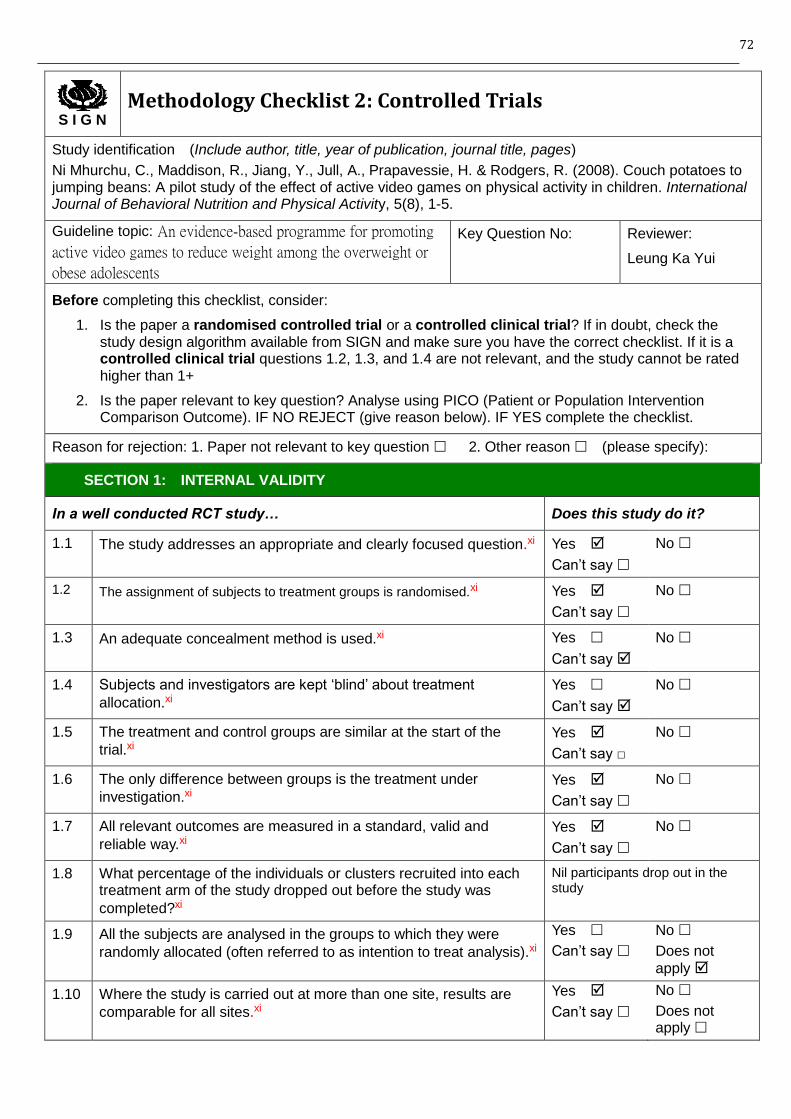
72
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Ni Mhurchu, C., Maddison, R., Jiang, Y., Jull, A., Prapavessie, H. & Rodgers, R. (2008). Couch potatoes to jumping beans: A pilot study of the effect of active video games on physical activity in children. International Journal of Behavioral Nutrition and Physical Activity, 5(8), 1-5.
Guideline topic: An evidence-based programme for promoting
active video games to reduce weight among the overweight or
obese adolescents
Key Question No: Reviewer:
Leung Ka Yui
Before completing this checklist, consider:
1. Is the paper a randomised controlled trial or a controlled clinical trial? If in doubt, check the study design algorithm available from SIGN and make sure you have the correct checklist. If it is a controlled clinical trial questions 1.2, 1.3, and 1.4 are not relevant, and the study cannot be rated higher than 1+
2. Is the paper relevant to key question? Analyse using PICO (Patient or Population Intervention Comparison Outcome). IF NO REJECT (give reason below). IF YES complete the checklist.
Reason for rejection: 1. Paper not relevant to key question 2. Other reason (please specify):
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.xi
Yes
Can’t say
No
1.2 The assignment of subjects to treatment groups is randomised.xi
Yes
Can’t say
No
1.3 An adequate concealment method is used.xi
Yes
Can’t say
No
1.4 Subjects and investigators are kept ‘blind’ about treatment
allocation.xi
Yes
Can’t say
No
1.5 The treatment and control groups are similar at the start of the
trial.xi
Yes
Can’t say □
No
1.6 The only difference between groups is the treatment under
investigation.xi
Yes
Can’t say
No
1.7 All relevant outcomes are measured in a standard, valid and
reliable way.xi
Yes
Can’t say
No
1.8 What percentage of the individuals or clusters recruited into each treatment arm of the study dropped out before the study was
completed?xi
Nil participants drop out in the study
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat analysis).xi
Yes
Can’t say
No
Does not
apply
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.xi
Yes
Can’t say
No
Does not apply
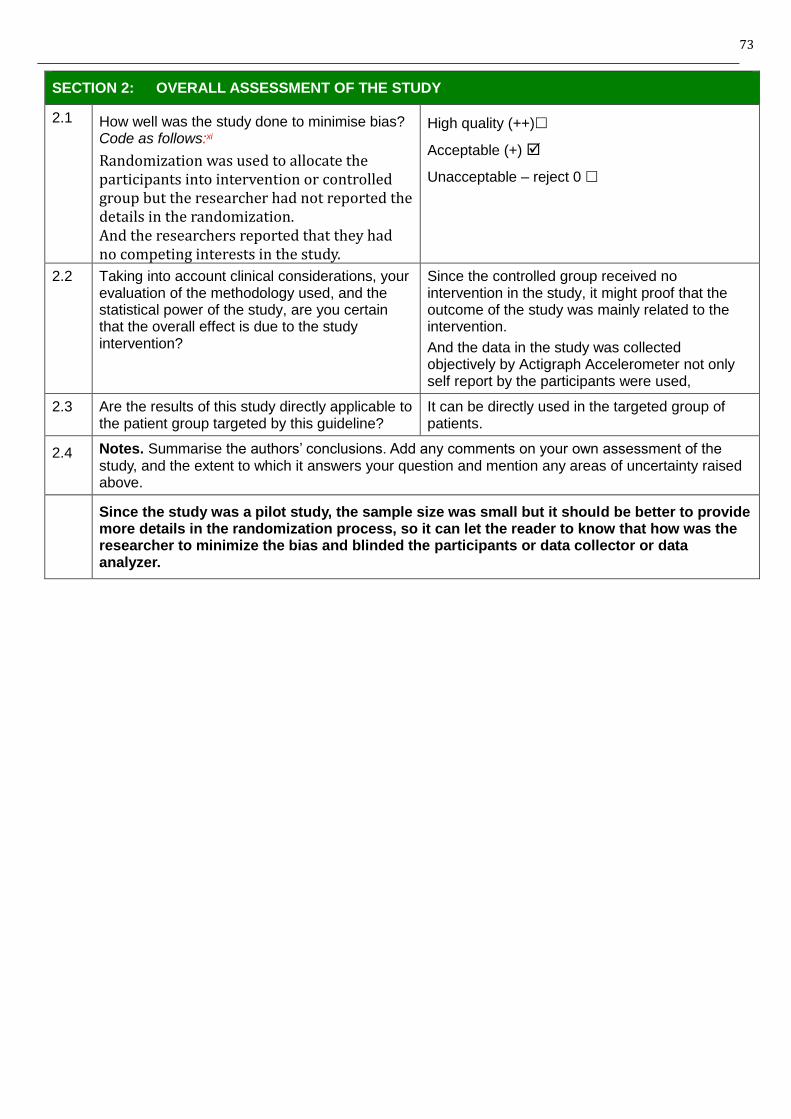
73
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias? Code as follows:xi
Randomization was used to allocate the participants into intervention or controlled group but the researcher had not reported the details in the randomization. And the researchers reported that they had no competing interests in the study.
High quality (++)
Acceptable (+)
Unacceptable – reject 0
2.2 Taking into account clinical considerations, your evaluation of the methodology used, and the statistical power of the study, are you certain that the overall effect is due to the study intervention?
Since the controlled group received no intervention in the study, it might proof that the outcome of the study was mainly related to the intervention.
And the data in the study was collected objectively by Actigraph Accelerometer not only self report by the participants were used,
2.3 Are the results of this study directly applicable to the patient group targeted by this guideline?
It can be directly used in the targeted group of patients.
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to which it answers your question and mention any areas of uncertainty raised above.
Since the study was a pilot study, the sample size was small but it should be better to provide more details in the randomization process, so it can let the reader to know that how was the researcher to minimize the bias and blinded the participants or data collector or data analyzer.
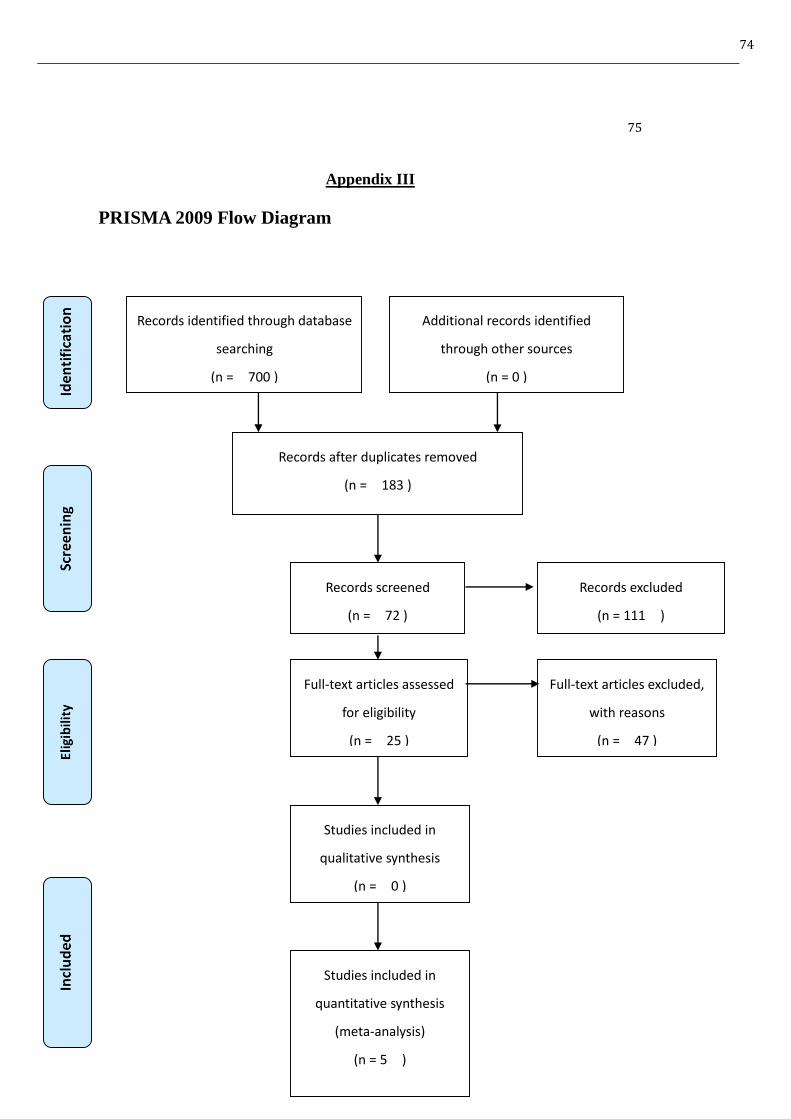
74
75
Appendix III
PRISMA 2009 Flow Diagram
Records identified through database
searching
(n = 700 )
Additional records identified
through other sources
(n = 0 )
Records after duplicates removed
(n = 183 )
Records screened
(n = 72 )
Records excluded
(n = 111 )
Full-text articles assessed
for eligibility
(n = 25 )
Full-text articles excluded,
with reasons
(n = 47 )
Studies included in
qualitative synthesis
(n = 0 )
Studies included in
quantitative synthesis
(meta-analysis)
(n = 5 )
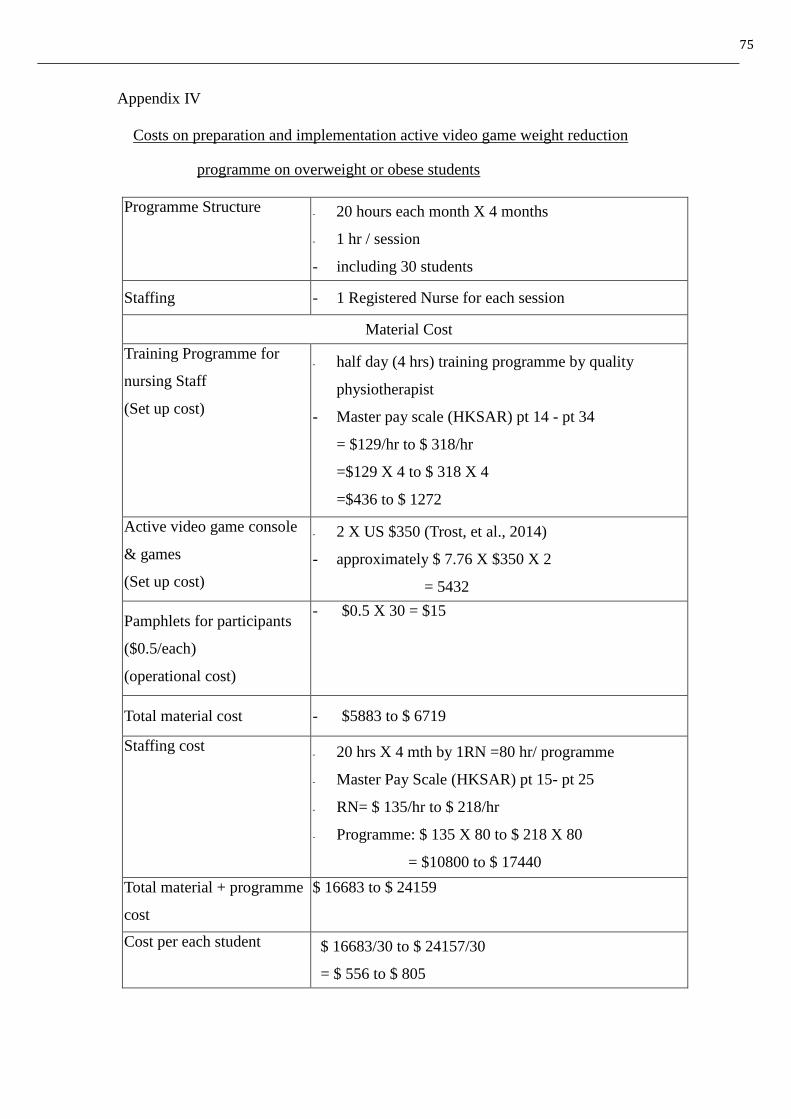
75
Appendix IV
Costs on preparation and implementation active video game weight reduction
programme on overweight or obese students
Programme Structure - 20 hours each month X 4 months
- 1 hr / session
- including 30 students
Staffing - 1 Registered Nurse for each session
Material Cost
Training Programme for
nursing Staff
(Set up cost)
- half day (4 hrs) training programme by quality
physiotherapist
- Master pay scale (HKSAR) pt 14 - pt 34
= $129/hr to $ 318/hr
=$129 X 4 to $ 318 X 4
=$436 to $ 1272
Active video game console
& games
(Set up cost)
- 2 X US $350 (Trost, et al., 2014)
- approximately $ 7.76 X $350 X 2
= 5432
Pamphlets for participants
($0.5/each)
(operational cost)
- $0.5 X 30 = $15
Total material cost - $5883 to $ 6719
Staffing cost - 20 hrs X 4 mth by 1RN =80 hr/ programme
- Master Pay Scale (HKSAR) pt 15- pt 25
- RN= $ 135/hr to $ 218/hr
- Programme: $ 135 X 80 to $ 218 X 80
= $10800 to $ 17440
Total material + programme
cost
$ 16683 to $ 24159
Cost per each student $ 16683/30 to $ 24157/30
= $ 556 to $ 805
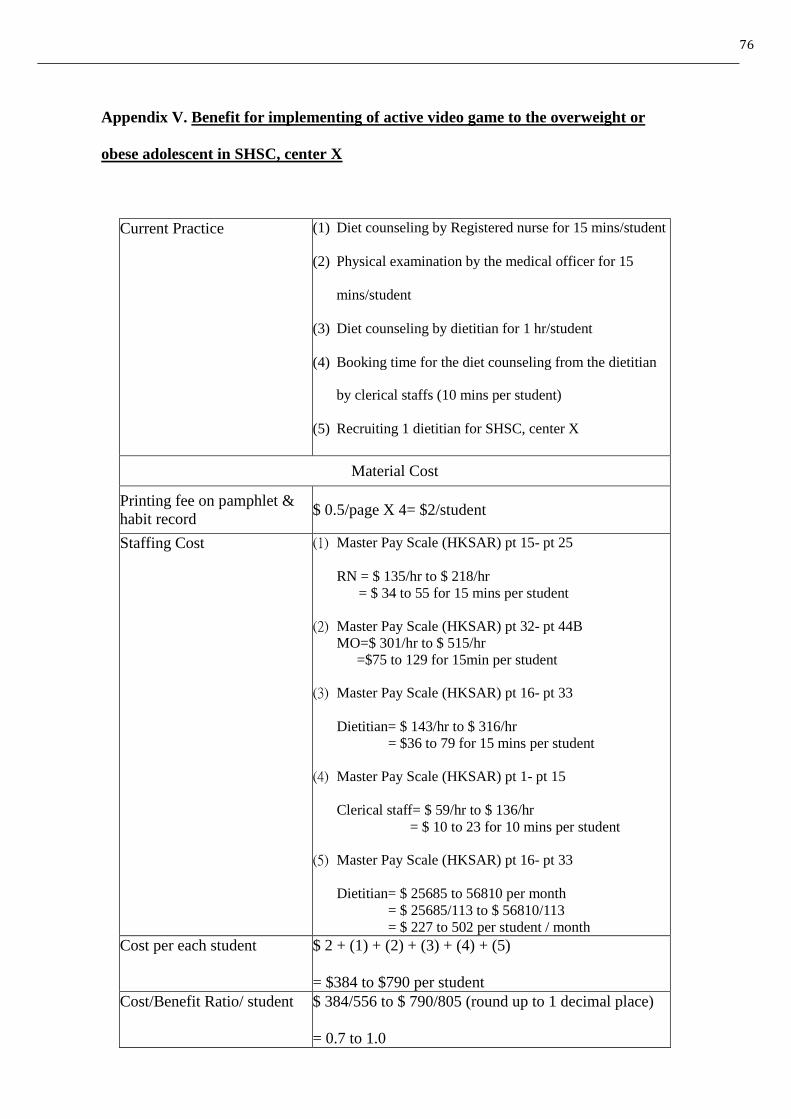
76
Appendix V. Benefit for implementing of active video game to the overweight or
obese adolescent in SHSC, center X
Current Practice (1) Diet counseling by Registered nurse for 15 mins/student
(2) Physical examination by the medical officer for 15
mins/student
(3) Diet counseling by dietitian for 1 hr/student
(4) Booking time for the diet counseling from the dietitian
by clerical staffs (10 mins per student)
(5) Recruiting 1 dietitian for SHSC, center X
Material Cost
Printing fee on pamphlet &
habit record $ 0.5/page X 4= $2/student
Staffing Cost (1) Master Pay Scale (HKSAR) pt 15- pt 25
RN = $ 135/hr to $ 218/hr
= $ 34 to 55 for 15 mins per student
(2) Master Pay Scale (HKSAR) pt 32- pt 44B
MO=$ 301/hr to $ 515/hr
=$75 to 129 for 15min per student
(3) Master Pay Scale (HKSAR) pt 16- pt 33
Dietitian= $ 143/hr to $ 316/hr
= $36 to 79 for 15 mins per student
(4) Master Pay Scale (HKSAR) pt 1- pt 15
Clerical staff= $ 59/hr to $ 136/hr
= $ 10 to 23 for 10 mins per student
(5) Master Pay Scale (HKSAR) pt 16- pt 33
Dietitian= $ 25685 to 56810 per month
= $ 25685/113 to $ 56810/113
= $ 227 to 502 per student / month
Cost per each student $ 2 + (1) + (2) + (3) + (4) + (5)
= $384 to $790 per student
Cost/Benefit Ratio/ student $ 384/556 to $ 790/805 (round up to 1 decimal place)
= 0.7 to 1.0
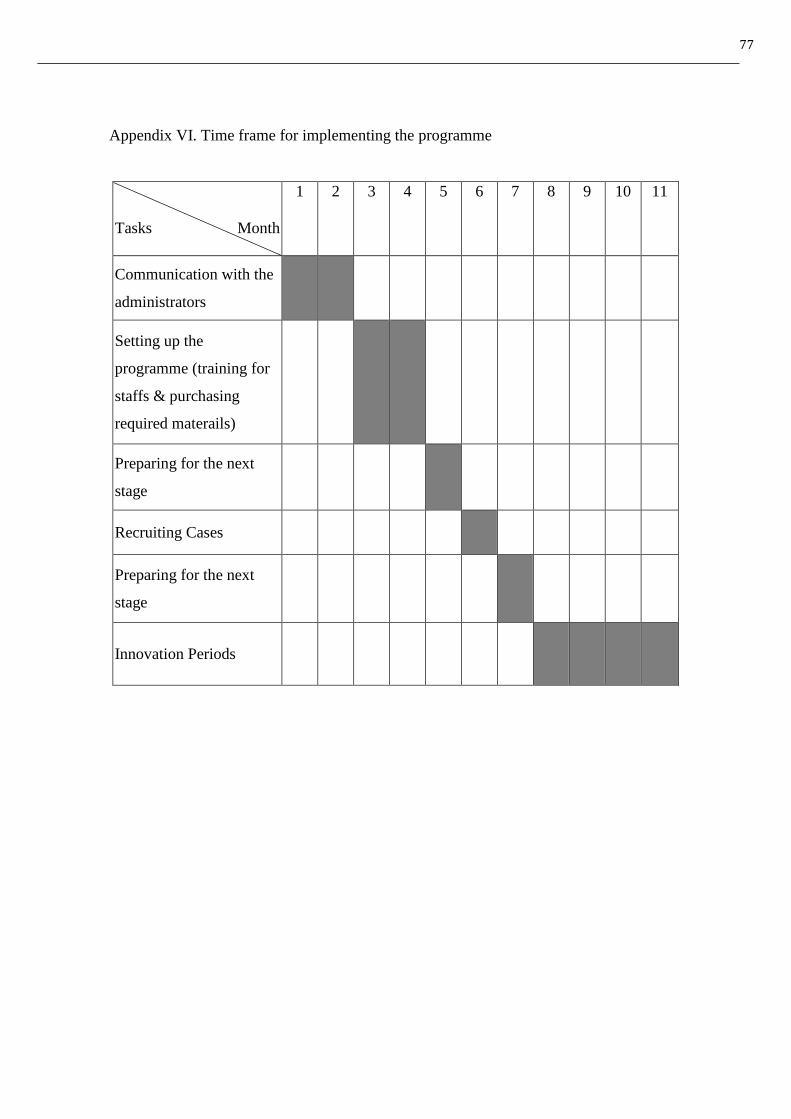
77
Appendix VI. Time frame for implementing the programme
Tasks Month
1 2 3 4 5 6 7 8 9 10 11
Communication with the
administrators
Setting up the
programme (training for
staffs & purchasing
required materails)
Preparing for the next
stage
Recruiting Cases
Preparing for the next
stage
Innovation Periods
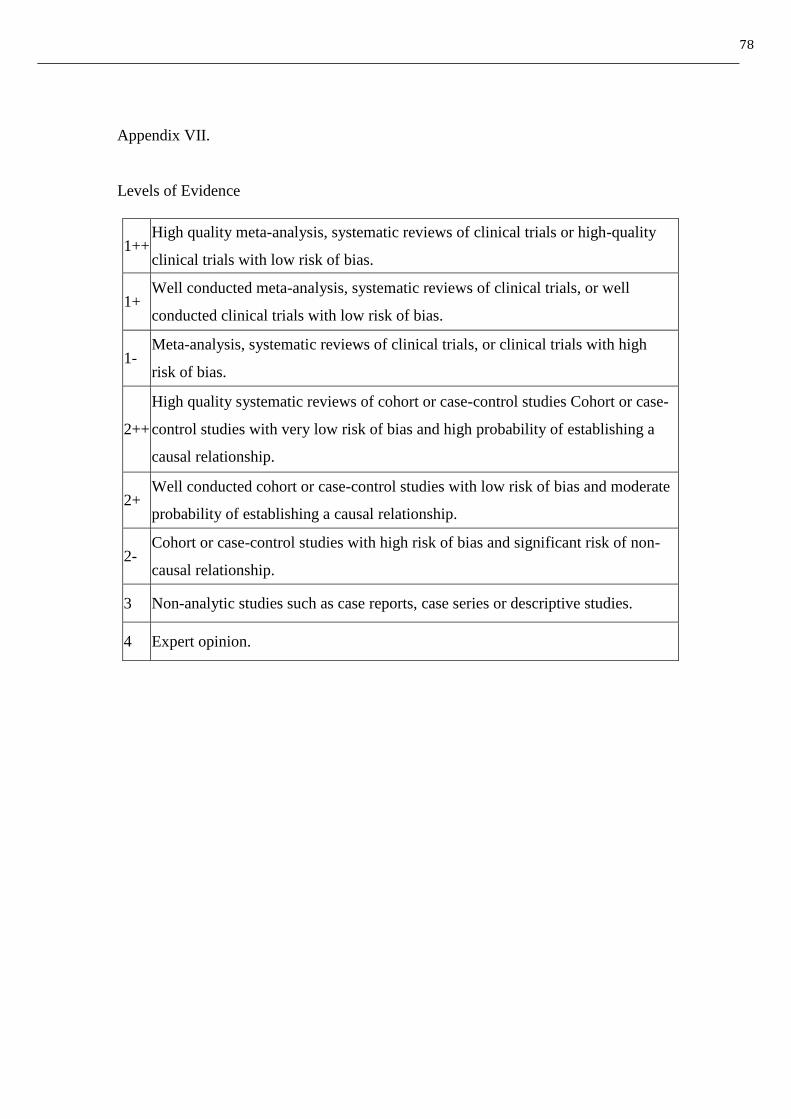
78
Appendix VII.
Levels of Evidence
1++ High quality meta-analysis, systematic reviews of clinical trials or high-quality
clinical trials with low risk of bias.
1+ Well conducted meta-analysis, systematic reviews of clinical trials, or well
conducted clinical trials with low risk of bias.
1- Meta-analysis, systematic reviews of clinical trials, or clinical trials with high
risk of bias.
2++
High quality systematic reviews of cohort or case-control studies Cohort or case-
control studies with very low risk of bias and high probability of establishing a
causal relationship.
2+ Well conducted cohort or case-control studies with low risk of bias and moderate
probability of establishing a causal relationship.
2- Cohort or case-control studies with high risk of bias and significant risk of non-
causal relationship.
3 Non-analytic studies such as case reports, case series or descriptive studies.
4 Expert opinion.
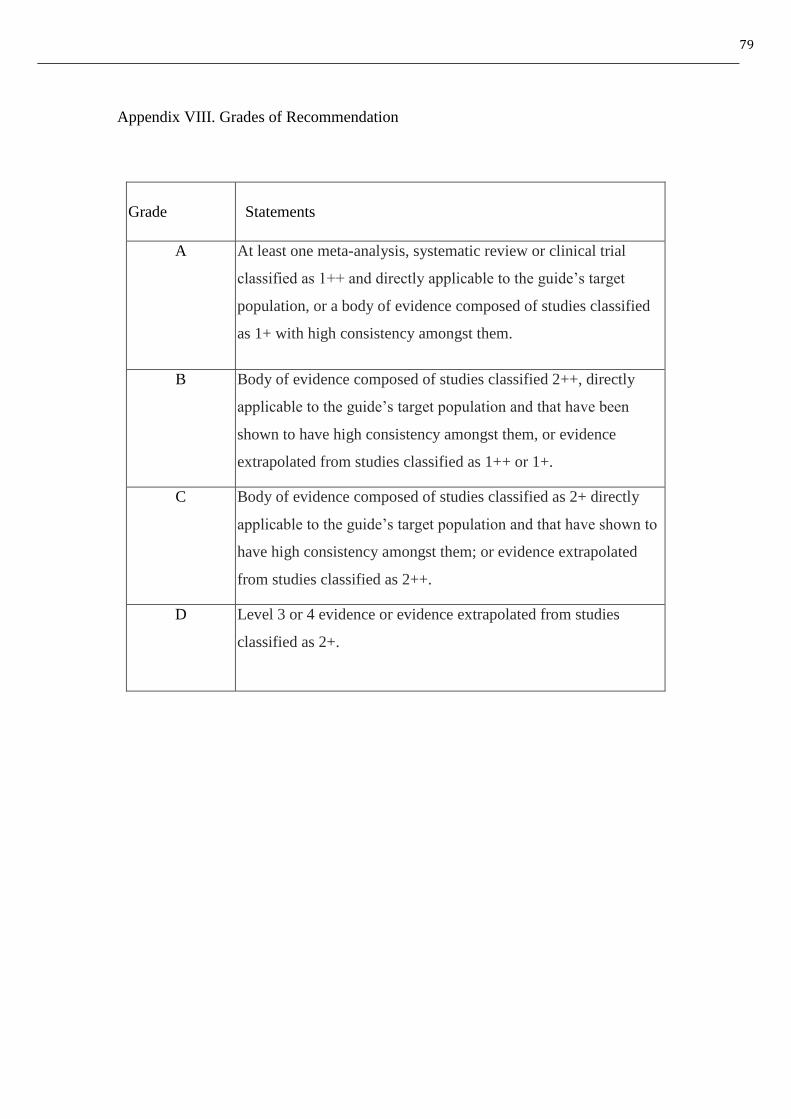
79
Appendix VIII. Grades of Recommendation
Grade Statements
A At least one meta-analysis, systematic review or clinical trial
classified as 1++ and directly applicable to the guide’s target
population, or a body of evidence composed of studies classified
as 1+ with high consistency amongst them.
B Body of evidence composed of studies classified 2++, directly
applicable to the guide’s target population and that have been
shown to have high consistency amongst them, or evidence
extrapolated from studies classified as 1++ or 1+.
C Body of evidence composed of studies classified as 2+ directly
applicable to the guide’s target population and that have shown to
have high consistency amongst them; or evidence extrapolated
from studies classified as 2++.
D Level 3 or 4 evidence or evidence extrapolated from studies
classified as 2+.
80
Appendix Ⅸ.
Guidelines on Active video game reduction programme among overweight or obese
adolescent
Title: Guidelines on Active video game reduction programme among overweight or
obese adolescent in Hong Kong
Aim: To reduce the weight and improve the health status of the target populations
Objectives:1. To encourage the sustainability performing regular exercise of the target
population
2. To maintain the health eating habit of the target population
3. To lower the risk of the target population to suffer from chronic disease
81
Target Population: Overweight or obese adolescents with weight for height ≥ 120%
of median weight for height form the sex-specific growth chart by Hong Kong Growth
Survey in 1993 and who attend the service in the SHSC, center X with no medical
complication
Venue: Health Education Room in SHSC, center X
Duration for the programme: 16 weeks
Numbers of participants for the programme: 30 adolescents
Organizers: Registered Nurses from SHSC, center X
1. Importance for tackling children’s overweight or obesity
(a) Draw the awareness on the target population about the complication on
children’s overweight or obesity
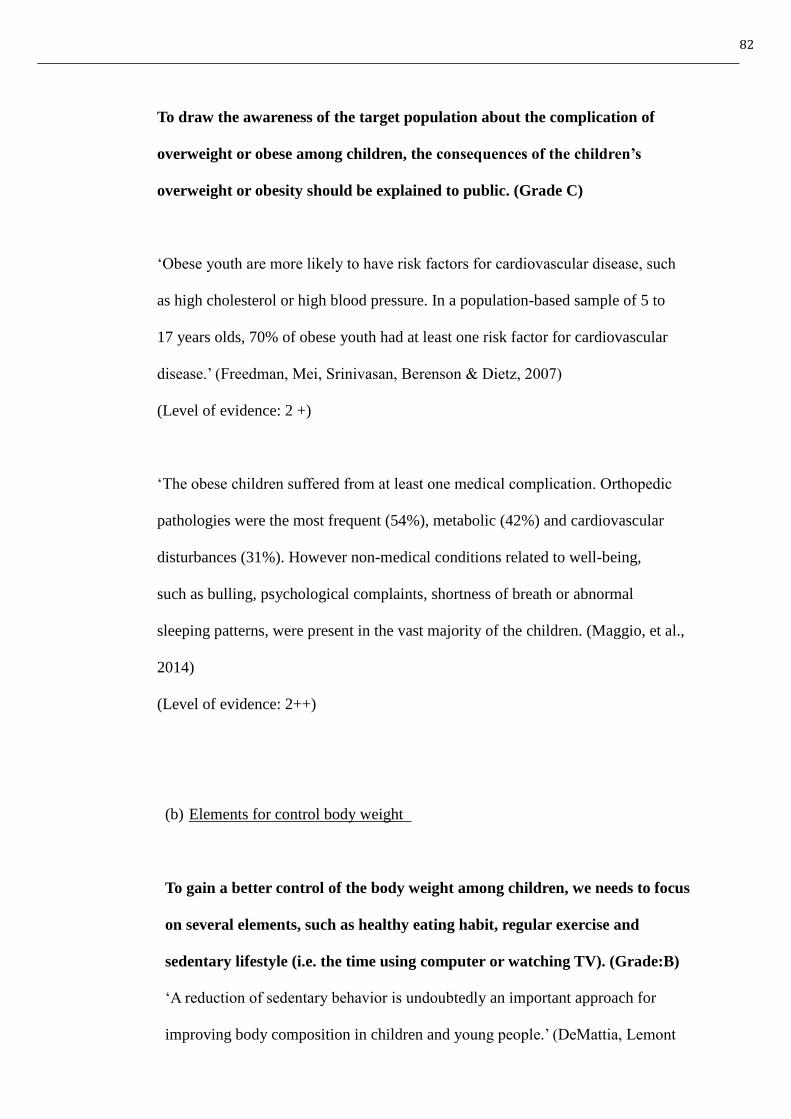
82
To draw the awareness of the target population about the complication of
overweight or obese among children, the consequences of the children’s
overweight or obesity should be explained to public. (Grade C)
‘Obese youth are more likely to have risk factors for cardiovascular disease, such
as high cholesterol or high blood pressure. In a population-based sample of 5 to
17 years olds, 70% of obese youth had at least one risk factor for cardiovascular
disease.’ (Freedman, Mei, Srinivasan, Berenson & Dietz, 2007)
(Level of evidence: 2 +)
‘The obese children suffered from at least one medical complication. Orthopedic
pathologies were the most frequent (54%), metabolic (42%) and cardiovascular
disturbances (31%). However non-medical conditions related to well-being,
such as bulling, psychological complaints, shortness of breath or abnormal
sleeping patterns, were present in the vast majority of the children. (Maggio, et al.,
2014)
(Level of evidence: 2++)
(b) Elements for control body weight
To gain a better control of the body weight among children, we needs to focus
on several elements, such as healthy eating habit, regular exercise and
sedentary lifestyle (i.e. the time using computer or watching TV). (Grade:B)
‘A reduction of sedentary behavior is undoubtedly an important approach for
improving body composition in children and young people.’ (DeMattia, Lemont
83
& Meure, 2007)
(Level of evidence: 2++)
‘Lifestyle changes, including reduced caloric intake, decreased sedentary behavior
and increase physical activity, are recommended for prevention and treatment of
child and adolescent obesity.’ (Martin, Saunders, Shenkin & Sproule, 2014)
(Level of evidence: 1+)
(c) Definition of overweight or obesity in children or adolescent
There are different definitions among each organization or countries, we
should find out what is meant by overweight or obesity among children or
adolescent to select potential participants for the programme. (Grade:D)
‘Overweight or obese can be defined as weight > 120% of the median weight for
height index by the 1993 Growth survey for students in Hong Kong.’ (Department
of Health, 2012)
(Level of evidence: 1+)
‘The definition of overweight by World Health Organization (WHO) is BMI ≥250
and the definition of obese by WHO is ≥ 30.’ (World Health Organization, 2014)
(Level of evidence: 4)
84
2. Programme Components & benefit to the target participants
(a) Including peer or parent in the praogramme
Despite active video game is an effective innovation to reduce weight among
overweight or obese children and adolescents, including peer or parent in the
weight reduction programme will foster the effect of weight reduction.
(Grade:B)
‘Treatment materials focused on the guardians’ roles in supporting the child’s
weight management efforts (reinforcement, modeling and changing the home
environment) rather than parental weight outcomes.’ (Trost, et al., 2014)
(Level of evidence: 1- )
‘Cooperative exergame players lost significantly more weight than the control
group. Cooperation may foster a team bond more so than competition, which may
help observe adolescents persist during physically demanding tasks such as
exergame play.’ (Staiano, et al., 2013)
(Level of evidence: 1- )
(b) Promoting physical activity as a habit among the overweight or obese
adolescents after implementing active video game
Although playing active video game can reduce weight among overweight or
obese adolescents, we also want to draw the awareness of the participant to
85
perform regular exercise persistently. (Grade:B)
‘Relative to baseline, MVPA from week 1 to 16 in the P+AG group was
significantly greater than that observed in the PO group (p=0.04).’ (Trost, et al.,
2014)
(Level of evidence: 1- )
‘Average time spent in all physical activities measured with an accelerometer was
higher in the active video game intervention group compared to the control group.’
(NiMhurchu, et al., 2008)
(Level of evidence: 1- )
(c) Modifying the eating habit of the target audience
Performing active video game to modify the eating habit of the participants
becoming healthier. (Grade:B)
‘Children in the intervention group played more active video games and fewer
non-active video games. This change in non-active video game play, which may
hand an effect on energy intake by minimizing cues to eat snack foods, was
reflected in the self-reported reductions in snack food data.’ (Maddison, et al., 2011)
(Level of evidence: 1+)
‘Active game play may have helped participants adhere to the program’s dietary
intake goals, resulting in greater reduction in energy intake.’ (Trost, et al., 2014)
(Level of evidence: 1- )

86
(d) Promote active video game in the home setting environment
To promote active video game as a long-term innovation for weight control
among overweight or obese students, because it is a convenient innovation
and easily to be adopted in home setting. (Grade:B)
‘Active gaming is convenient safe and popular among young people and it amy be
applied at home setting especially in countries were outdoor access is limited or
prolonged periods of winter’ (Trost, et al., 2014 & Maddison, et al., 2011)
(Level of evidence: 1- )

87
Appendix X. References of the Clinical Guidelines
1. Maddison, R., Foley, L., Ni MC., Jiang, Y., Jull, A., Prapavessis, H., Hohepa, M.
& Rodgers, A. (2012). Effect of active video games on body composition: a
randomized controlled trial. Am J Clin Nutr, 2011(94), 156-63.
2. Trost, S. G., Sundal, D., Foster, G. D., Lent, M. R. & Vojta, D. (2014). Effects of a
Pediatric Weight Management Program With and Without Active Video Games.
JAMA Pediatr, 168(5), 407-413.
3. Ni Mhurchu, C., Maddison, R., Jiang, Y., Jull, A., Prapavessie, H. & Rodgers, R.
(2008). Couch potatoes to jumping beans: A pilot study of the effect of active
video games on physical activity in children. International Journal of Behavioral
Nutrition and Physical Activity, 5(8), 1-5.
4. Staiano, A. E. Abraham, A. A. & Calvert, S. L. (2013). Adolescent Exergame Play
for Weight Loss and Psychosocial Improvement: A Controlled Physical Activity
Intervention. Obesity (Silver Spring), 21(3), 1-7.
5. Department of Health. (2012). Childhood overweight and obesity. Bridge Issue
No.57. Retrieved from December 8, 2014, from
http://www.studenthealth.gov.hk/english/newsletters/newsletter_57.html
88
6. Maggio, A. BR., Martin, X. E., Gasser, C. S., Gal-Dusing, C., Beghetti, M.,
Farpour-Lambert, N. J. & Chamay-Weber, C. (2014). Medical and non-medical
7. complications among children and adolescents with excessive body weight. BMC
Pediatrics, 14(232), 1-9.
8. Freedman, D. S., Srinivasan, S. R., Berenson, G. S. & Dietz, W. H. (2007).
Cardiovascular Risk Factors and Excess Adiposity Among Overweight Children
and Adolescents: The Bogalusa Heart Study. The Journal of Pediatrics, 150(12-
7), 12-17.
9. DeMattia, L., Lemont, L. & Meurer, L. (2007). Do interventions to limit sedentary
behaviours change behavior and reduce childhood obesity? A critical review of
the literature. Obesity Reviews, 8(1), 69-81.
10. Martin, A., Saunders, DH., Shenkin, SD. & Sproule, J. (2014). Lifestyle
intervention for improving school achievement in overweight or obese children
and adolescents. Cochrane Database of Systematic Review, 14(3), 1-93.
11. World Health Organization. (2014). Obesity and Overweight. Fact sheet N°311.
Retrieved from December 8, 2014 from
http://www.who.int/mediacentre/factsheets/fs311/en/
89
References
1. Ogden, C. L., Carroll, M. D., Kit, B. K. & Flegal, K. M. (2014). Prevalence of
childhood and adult obesity in the United States, 2011-2012. Journal of the
American Medical Association 311(8), 806-814.
2. National Institutes of Health, National Heart, Lung, and Blood Institute. (2010).
Disease and Conditions Index: What are overweight and obesity?. National
Institutes of Health. Retrieved from August 8, 2014, from
http://www.cdc.gov/healthyyouth/obesity/facts.htm
3. de Onis, M., Blössner, M. & Borghi, E. (2010). Global prevalence and trends of
overweight and obesirt among preschool children. The American Journal of
Clinical Nutrition, 92(5), 1257-64.
4. Department of Health. (2012). Childhood overweight and obesity. Bridge Issue
No.57. Retrieved from August 8, 2014, from
http://www.studenthealth.gov.hk/english/newsletters/newsletter_57.html
90
5. Education Bureau. (2002). Physical Education Key Learning Area Curriculum
Guide (2002). Physical Education – Curriculum Documents. Retrieved from
August 8, 2014 from http://www.edb.gov.hk/en/curriculum-
development/kla/pe/cirriculum-doc/index.html
6. Lu, X., Shi, P., Luo, CY., Zhou, YF., Yu, HT., Guo, CY. & Wu, F. (2013).
Prevalence of hypertension in overweight and obese children from a large school-
based population in Shanghai, China. BMC Public Health, 13(24), 1-7.
7. Leisure and Cultural Services Department & Community Sports Committee of the
Sports Commission. (2012). Healthy Exercise for All Campaign – Physical
Fitness Test for the Community. Final Summary Report. Retrieved from August 8,
2014 from
http://www.lcsd.gov.hk/healthy/physical_fitness_test/download/SummaryReport
en.pdf
8. Critical Appraisal Skills Programme. (2013). About us & History. Critical
Appraisal Skills Programme. Retrieved from August 8, 2014 from
http://www.casp-uk.net/#!history/cnxo
91
9. Scottish Intercollegiate Guidelines Network. (2012). Methodology Checklist 2:
Randomized Controlled Trials. Critical Appraisal: Notes and Checklists.
Retrieved from August 8, 2014 from
http://www.sign.ac.uk/methodology/checklists.html
10. Maddison, R., Foley, L., Ni MC., Jiang, Y., Jull, A., Prapavessis, H., Hohepa, M.
& Rodgers, A. (2012). Effect of active video games on body composition: a
randomized controlled trial. Am J Clin Nutr, 2011(94), 156-63.
11. Trost, S. G., Sundal, D., Foster, G. D., Lent, M. R. & Vojta, D. (2014). Effects of a
Pediatric Weight Management Program With and Without Active Video Games.
JAMA Pediatr, 168(5), 407-413.
12. Adamo, K. B., Rutherford, J. A. & Goldfield, G. S. (2010). Effects of interactive
video game cycling on overweight and obese adolescent health. Appl. Physiol.
Nutr. Metab, 2010(35), 805-815.
13. Staiano, A. E. Abraham, A. A. & Calvert, S. L. (2013). Adolescent Exergame Play
for Weight Loss and Psychosocial Improvement: A Controlled Physical Activity
Intervention. Obesity (Silver Spring), 21(3), 1-7.
92
14. Ni Mhurchu, C., Maddison, R., Jiang, Y., Jull, A., Prapavessie, H. & Rodgers, R.
(2008). Couch potatoes to jumping beans: A pilot study of the effect of active
video games on physical activity in children. International Journal of Behavioral
Nutrition and Physical Activity, 5(8), 1-5
15. Department of Health. (2014). About Student Health Service. Retrieved from
December 8, 2014 from
http://www.studenthealth.gov.hk/english/aboutus/aboutus_shs/aboutus_shs.html
16. Department of Health. (2013). Statistics on Student Health Service Centers for
School Year 2012/13. Department of Health: Hong Kong.
17. Department of Health. (2012). Background. ‘[email protected]’Campaign. Retrieved from
December 22, 2014 from
http://school.eatsmart.gov.hk/en/template/index.asp?pid=2005&id=3075
18. Maggio, A. BR., Martin, X. E., Gasser, C. S., Gal-Dusing, C., Beghetti, M.,
Farpour-Lambert, N. J. & Chamay-Weber, C. (2014). Medical and non-medical
complications among children and adolescents with excessive body weight. BMC
Pediatrics, 14(232), 1-9.

93
19. Civil Service Bureau. (2013). Master Pay Scale. Pay and Allowances. Retrieved
from December 8, 2014 from http://www.csb.gov.hk/english/admin/pay/42.html
20. Lenth, R. V. (2006-9). Java Applets for Power and Sample Size [Computer
Software]. Retrieved from April 18, 2015 from
http://www.stat.uiowa.edu/~rlenth/Power.