achondroplasia · diego vélasquez, don sebastian de morra achondroplasia geert mortier, md, phd...
TRANSCRIPT

Diego Vélasquez, don Sebastian de Morra
ACHONDROPLASIA
Geert Mortier, MD, PhD Department of Medical Genetics
Antwerp University Hospital University of Antwerp
GENOMED Centre of Excellence
• autosomal dominant condition • recurrent mutation (p.G380R) in FGFR3 gene • most common form of short limb dwarfism (1/10.000-1/30.000)
• major clinical features: - prenatal onset of disproportionate short stature - macrocephaly, low nasal bridge, frontal bossing - short limbs with redundant skin folds, trident hand - ligamentous laxity in knees, genua vara - normal intelligence - adult height: males 131 ± 5,6 cm females 124 ± 5,9 cm
• major radiographic features:
- shortening of tubular bones (all segments involved) - platyspondyly, bullet-shaped vertebrae, posterior scalloping - interpedicular narrowing - abnormal pelvis with small iliac wings, flat acetabular roofs (trident) - lumbar hyperlordosis
Achondroplasia
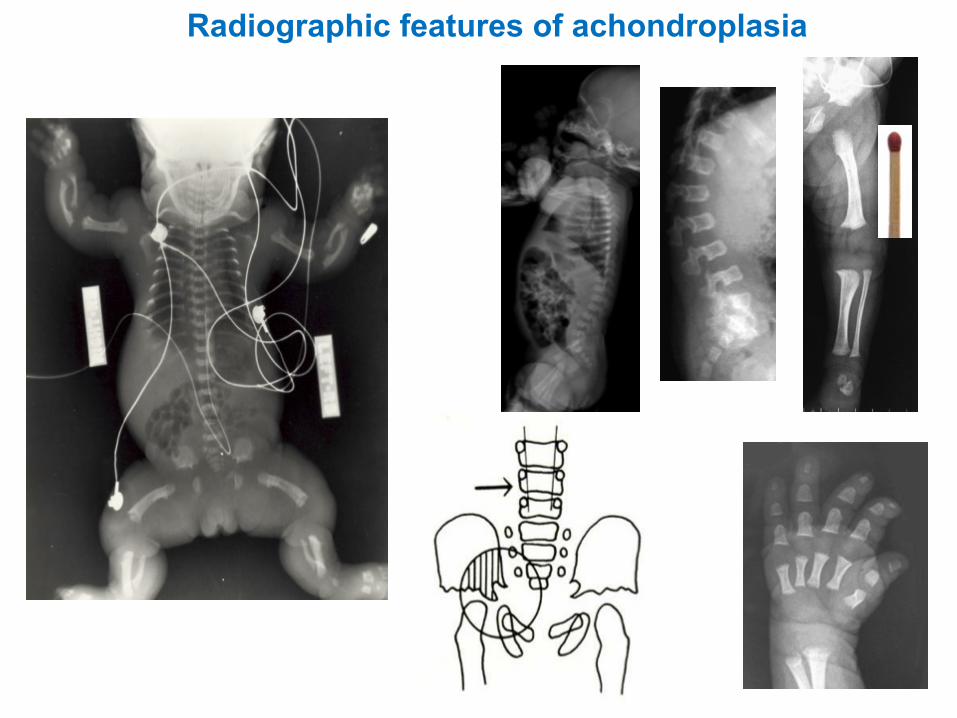
Radiographic features of achondroplasia
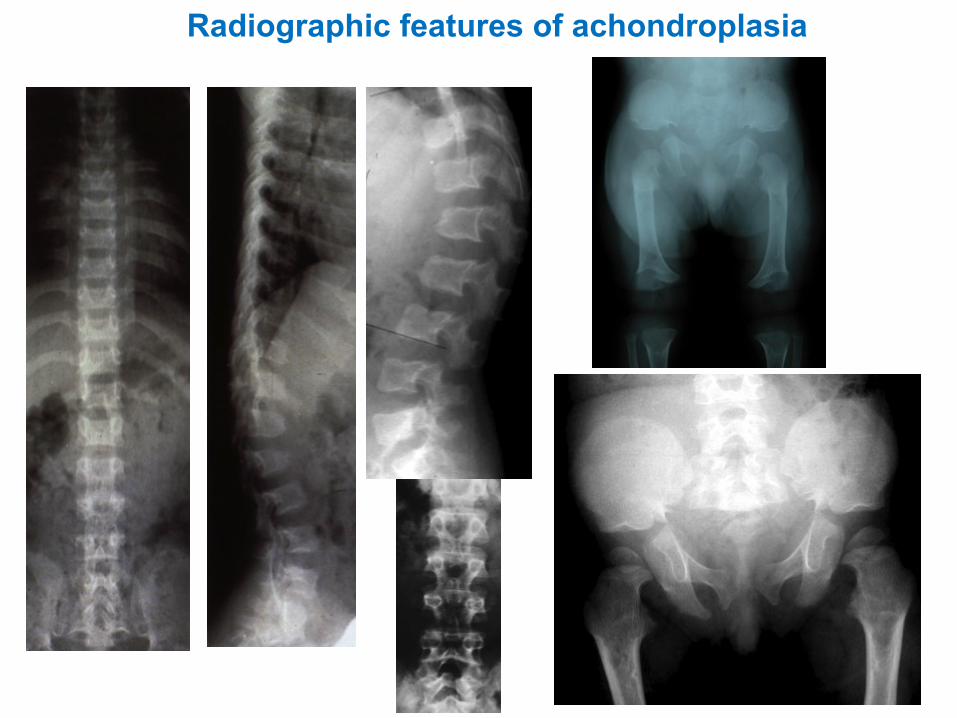
Radiographic features of achondroplasia

Short-limbdwarfism
Short-trunkdwarfism
Differential diagnosis

Hypochondroplasia
clinical photos deleted

thanatophoric dysplasia
achondroplasia hypochondroplasia
FamilyofFGFR3disorders

FGFR3
cell
mem
bran
e
intracellular extracellular
SP: signal peptide Ig: immunoglobuline-like domain TM: transmembrane domain
Structure of the FGFR3 protein
p.G380R mutation in achondroplasia

Activation of the fibroblast growth factor receptors
cell membrane

(Fibroblast growth factors)
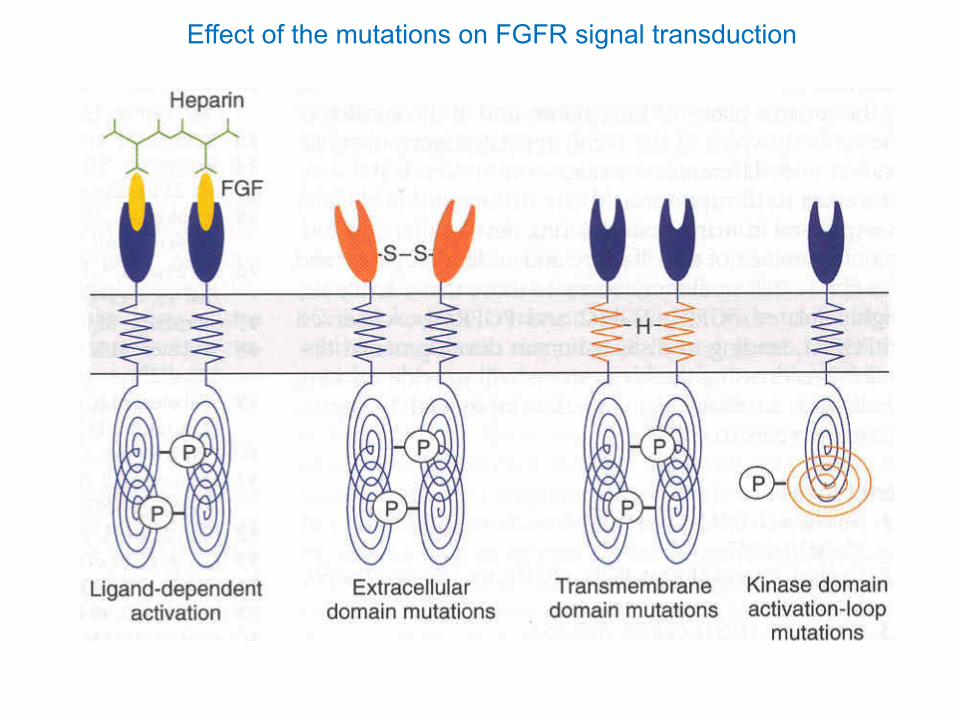
Effect of the mutations on FGFR signal transduction

Current care and management
• no cure • genetic counseling • growth hormone treatment: effect on adult height?1 • limb lengthening: final height up to + 20 cm • new drugs in the pipeline • now mainly prevention and treatment of complications • lack of evidence-based guidelines • need for multidisciplinary approach!
1 Miccoli M et al. Horm Res Paediatr 2016;86:27-34

Growth and development should be monitored according to norms for achondroplasia

Pediatrics 2005;116:771-783

males

Monitor neuromotor development


• key concerns in the infant and toddler: - ventriculomegaly/true hydrocephaly (very rare) - spinal cord compression at cervicomedullary junction (small foramen magnum)
- sudden infant death (rare) - thoracolumbar kyphosis - middle ear effusions and infections - sleep apnea (obstructive and/or central)
• key concerns in the older child:
- upper airway and ENT infections - sleep apnea - obesity - angular deformities of the lower limb (genua vara)
• key concerns in the adolescent and adult
- lumbar spinal stenosis - back pain - peripheral nerve compression
Areas of concern in achondroplasia
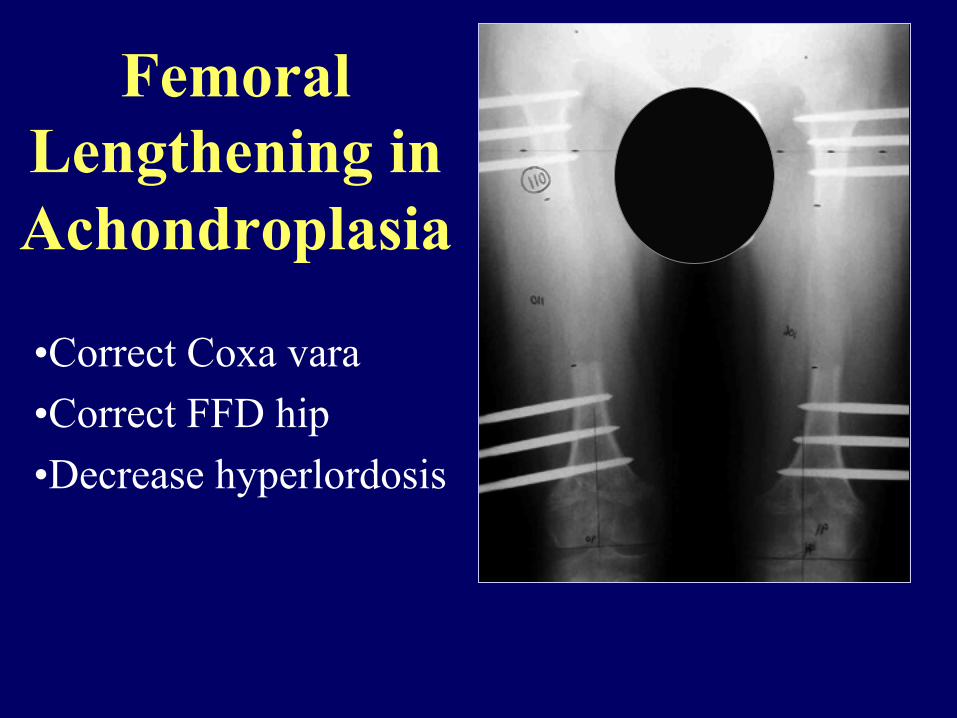
Femoral Lengthening in Achondroplasia
• Correct Coxa vara • Correct FFD hip • Decrease hyperlordosis
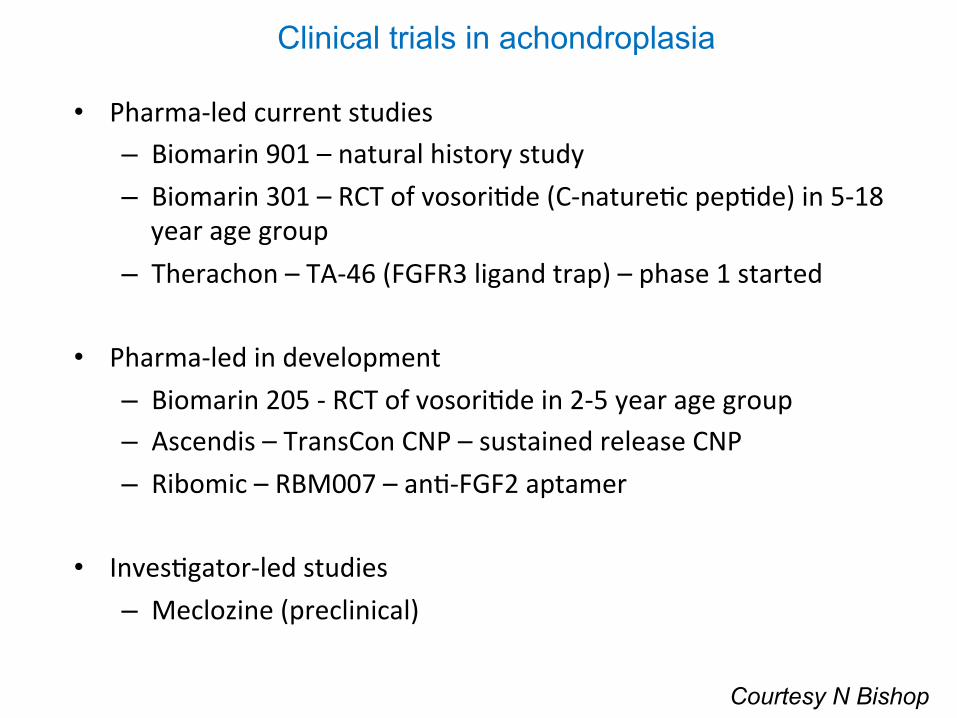
• Pharma-ledcurrentstudies– Biomarin901–naturalhistorystudy– Biomarin301–RCTofvosori@de(C-nature@cpep@de)in5-18yearagegroup
– Therachon–TA-46(FGFR3ligandtrap)–phase1started• Pharma-ledindevelopment
– Biomarin205-RCTofvosori@dein2-5yearagegroup– Ascendis–TransConCNP–sustainedreleaseCNP– Ribomic–RBM007–an@-FGF2aptamer
• Inves@gator-ledstudies
– Meclozine(preclinical)
Clinical trials in achondroplasia
Courtesy N Bishop

From: Klag KA & Horton WA. Hum Mol Genet 2015
Interaction between FGF and CNP signaling

Natriure@cpep@desystem
cGKII (cGMP dependent kinase II) � Acts downstream of cGMP � cGKII-/- mice
� Dwarfism
� Inhibits the MAPK pathway � Overactivation in achondroplasia
� Caused by gain-of-function mutations in FGFR3 � Short-limb dwarfism
è CNP possible therapeutic target
BMN-111

Yasoda A et al. Endocrinology 2009;150:3138-3144
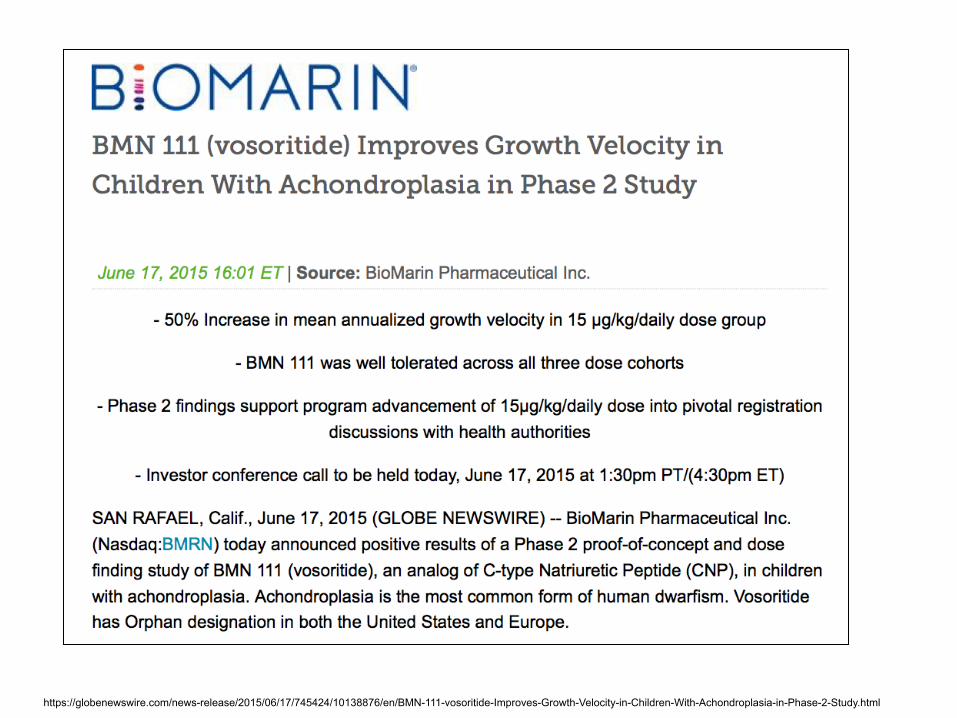
https://globenewswire.com/news-release/2015/06/17/745424/10138876/en/BMN-111-vosoritide-Improves-Growth-Velocity-in-Children-With-Achondroplasia-in-Phase-2-Study.html

https://globenewswire.com/news-release/2015/06/17/745424/10138876/en/BMN-111-vosoritide-Improves-Growth-Velocity-in-Children-With-Achondroplasia-in-Phase-2-Study.html
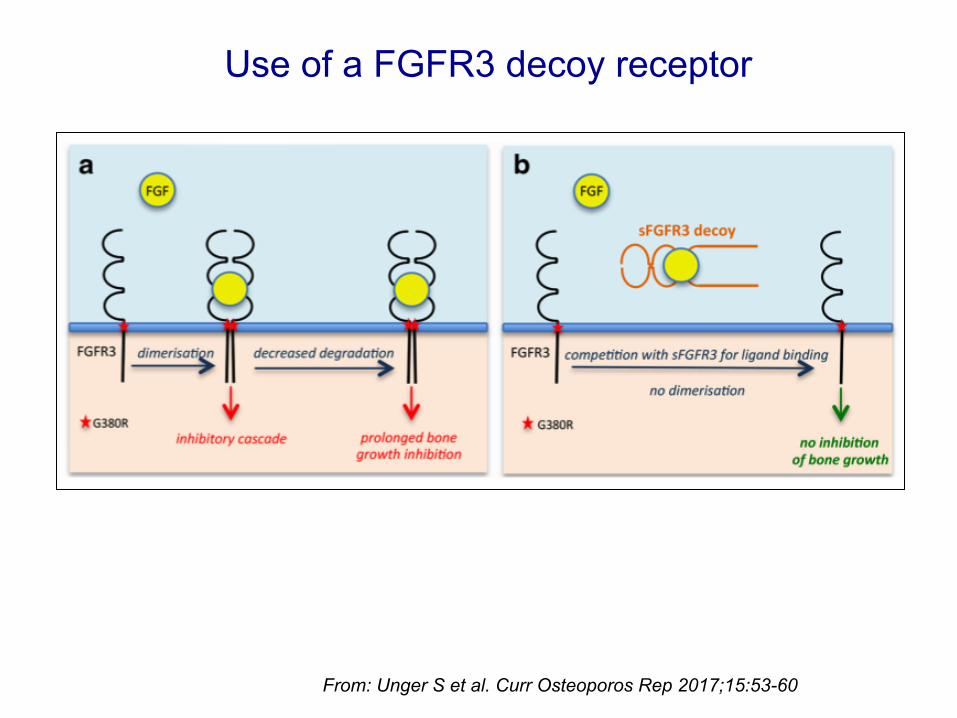
From: Unger S et al. Curr Osteoporos Rep 2017;15:53-60
Use of a FGFR3 decoy receptor

Garcia S et al. Sci Transl Med 2013;5:203ra124


Take home messages
• frequent skeletal dysplasia • significant morbidity (more than being short…) • need for close follow-up early on in life • multidisciplinary approach • use of achondroplasia-specific charts (growth and development) • need for good (evidence-based) clinical guidelines • new drugs maybe promising (not only for stature?)