actra asm 2016 derivation of an occupational exposure limit...
TRANSCRIPT

ACTRA ASM 2016
1
Derivation of anOccupational Exposure Limit for Methoxyflurane

Standard Setting
2
Review dataset
Choose critical adverse effect
Define point of departure
Select uncertainty factors
Choose criticalstudy
Derive Occupationalexposure limit

Introduction and Overview
Presentation
Glass bottle containing liquid form of methoxyflurane
Dose limiting inhaler
Activated Charcoal (AC) Chamber (optional)
3

Introduction and Overview
INTERNAL FIBROUS PAD(to act as a wick)
ONE-WAY VALVE(to prevent blow-back into wick)
DILUTOR HOLE(enables two concentrations)
OXYGEN INLET
4

Introduction and Overview
Pharmacology
Dramatically reduces pain scores by 50 – 80%
Unique member of the volatile anaesthetics group which provides analgesia when inhaled in very low concentrations
Primary site of action is in the central nervous system where inhibition of nerve transmission occurs at synapses; the sites at which neurotransmitters are released and exert their initial action in the body
5

Introduction and Overview
Anaesthesia 40 – 60 mL dose
Greater than 2.5 MAC hours of exposure required to cause reversible toxicity1,2
Analgesia doses 3 – 6 mL dose
Approximately 0.3 - 0.6 MAC hours of exposure 3
Less than 25% of dose required to cause toxicity
0
10
20
30
40
50
60
70
Analgesia Anaesthesia
6

Introduction and Overview
Simple to give, safe, effective inhaled analgesia
Given intermittently; patient controlled
Initial 10-12 breaths, or until onset of pain relief
Rapid onset, effective for 7-10 minutes
Patient decides on need for a further 6 breath supplement intermittently as needed
Rapid recovery – feel normal after maximum of 20 minutes, often much less
7

Introduction and Overview
30+ years and circa 4,000,000 doses of safe effective analgesic use
Minimal minor side effects
No requirement to withhold food or drink
No need for premedication – facilitates scheduling procedures
Discharge at proceduralist discretion
Improves patient outcomes
8

Data set
Endpoints: Liver Kidney CNS Depression Developmental Toxicity (spontaneous abortion)
12 October 2012 9

Introduction and Overview
Properties(3, 4)
Methoxyflurane [CAS 76-38-0; MOF]
2,2-dichloro-1,1-difluoromethyl ether
Clear, colourless, volatile liquid with a sweet fruity odourStable, non-flammable and non-explosive in air or oxygen
10

Introduction and Overview
Kinetics
Complete and rapid absorption following inhalation
Primarily distributed to blood, brain, liver and lungs
Extensively metabolised20, 21, 22, 23
40 - 70% of MOF converted to metabolites
Approximately 20% excreted as MOF in exhaled air
11

Introduction and Overview
Kinetics (cont.)
Metabolites include; Methoxydifluoroacetic acid, oxalic acid, chloride, inorganic fluoride, dichloroacetic acid
Conclusion: At analgesic doses metabolites eliminated rapidly (within 24 hours)24,25
12

Penthrox Safety
Central Nervous System (CNS)
No adverse non expected central nervous system effects or symptoms24,26,27,29,30
Minor side effects not troublesome in most cases31
Conclusion for Patients : Other than analgesia, CNS effects are transient and minor
Conclusion for Operators : No adverse effects expected
13

Penthrox Toxicity
Kidney Toxicity Nephrotoxicity thoroughly investigated in animals and
humans21,22,23,32
MOF nephrotoxicity is dose related
MOF nephrotoxicity has a strong correlation with inorganic fluoride levels, no effects at 40 micromolar per litre1
Serum fluoride levels need to be substantially elevated before kidney damage occurs
14

Penthrox Toxicity
Kidney Toxicity (cont.)
Conclusion Kidney Toxicity only occurs at doses greater than those
achievable in current use4
No adverse effects for Patients when used for analgesia
No adverse effects for Operators when used for analgesia
15

Penthrox Toxicity
Liver Toxicity
Postulated immune system mediated mechanism of action5,32
Rare, even at anaesthetic concentrations5,32
Extremely rare in current uses16
Conclusion
Highly unlikely when used for analgesia
16
Penthrox Toxicity
Other Toxicity
Animals study in mice investigating exposure at anaesthetic concentrations concluded that halogenated general anaesthetics do not pose a significant risk of cancer to humans33
International Agency for Research on Cancer - no conclusive evidence for carcinogenicity (Group 3)36
17

Penthrox Toxicity
Other Toxicity (Cont.)
Animal studies investigating the reproductive and developmental toxicity of MOF consistently show that MOF is neither teratogenic nor causes reproductive effects at sub-anaesthetic exposures which are not toxic to the mother34,35
18

Key Study
November 8, 2016 19
Kidney Clinical studies provided do not provide suitable data. Issues with
historical studies … extrapolation of dose
Pivotal Study reference(s)
Cousins MJ and Mazze RI (1973), Methoxyflurane nephrotoxicity, a study of dose response in man, JAMA 225(13) 1611-1616.
Study Population 26 healthy men scheduled for elective surgery (no age related information disclosed)
Route of ExposureInhalation via inhaler connected to anaesthetic vaporiser; anaesthesia was maintained with methoxyflurane or halothane supplemented by 50% nitrous oxide and 50% oxygen at a total gas flow of 6 litres/min.

Critical Effect – Kidney Toxicity
20
Critical Effect(s)
Cousins & Mazze found the mean threshold for toxicity to be approximately 2.5 MAC-hours. Subclinical toxicity was found to occur at exposures 2.5 - 3.0 MAC-hours which resulted in:
Peak serum fluoride ion concentration from 50 - 80 µM Delayed return to preoperative urine osmolality Unresponsiveness to vasopressin administration
This is equivalent to the lowest observed adverse effect levelThe study also found that patients receiving 2.0 MAC-hours or less methoxyfluranehad peak serum fluoride ion concentrations <40 µM which was not associated with nephrotoxicity.
Dose response:

Dose Groups Cousins & Mazze
21
Converting MAC’s to ppm is inherently difficult
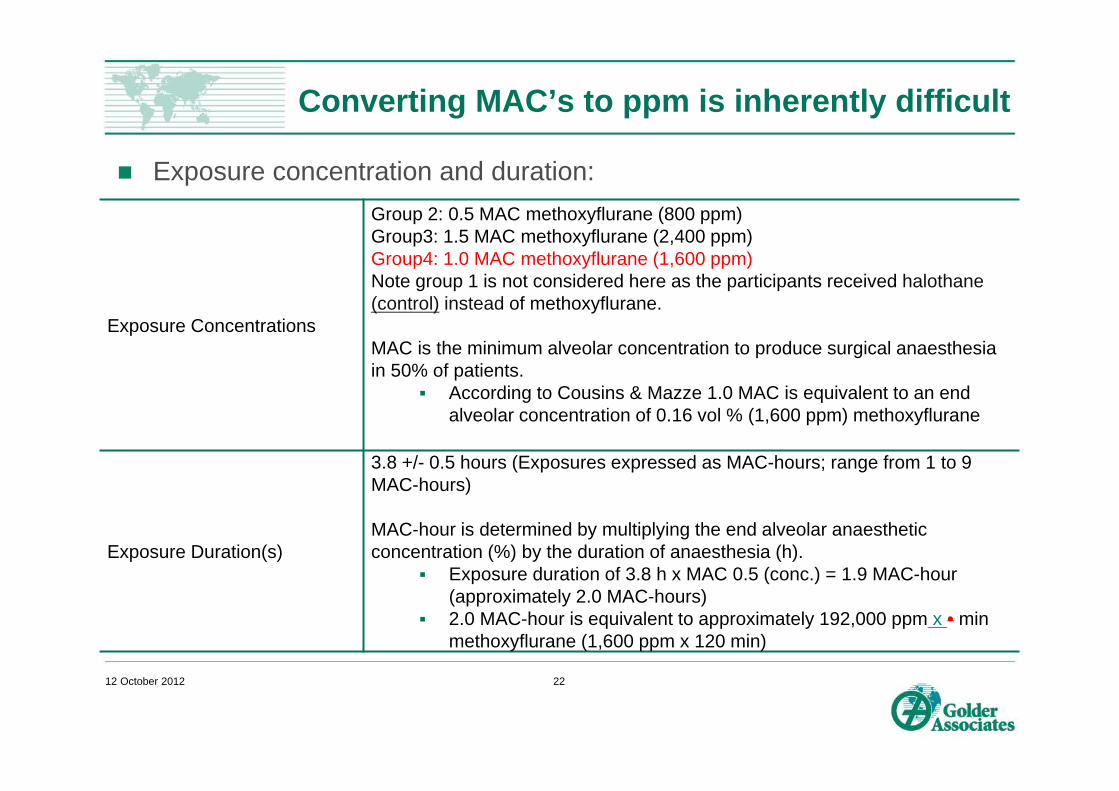
Exposure concentration and duration:
12 October 2012 22
Exposure Concentrations
Group 2: 0.5 MAC methoxyflurane (800 ppm)Group3: 1.5 MAC methoxyflurane (2,400 ppm)Group4: 1.0 MAC methoxyflurane (1,600 ppm)Note group 1 is not considered here as the participants received halothane(control) instead of methoxyflurane.
MAC is the minimum alveolar concentration to produce surgical anaesthesia in 50% of patients.
According to Cousins & Mazze 1.0 MAC is equivalent to an end alveolar concentration of 0.16 vol % (1,600 ppm) methoxyflurane
Exposure Duration(s)
3.8 +/- 0.5 hours (Exposures expressed as MAC-hours; range from 1 to 9 MAC-hours)
MAC-hour is determined by multiplying the end alveolar anaesthetic concentration (%) by the duration of anaesthesia (h).
Exposure duration of 3.8 h x MAC 0.5 (conc.) = 1.9 MAC-hour (approximately 2.0 MAC-hours)
2.0 MAC-hour is equivalent to approximately 192,000 ppm x • min methoxyflurane (1,600 ppm x 120 min)

Extrapolated Dose Data
23

Preparing Concentration v Response dataset
24

Fig. 2. Dose-response data grouping. 1 The maximum dose (192,000 ppm min MOF) selected for benchmarking as there were no incidences recorded for Dose group 1. 2 Conservatively the lowest dose concentration (240,000 ppm min MOF) used for benchmarking for Dose g...

Derivation of MEL
26
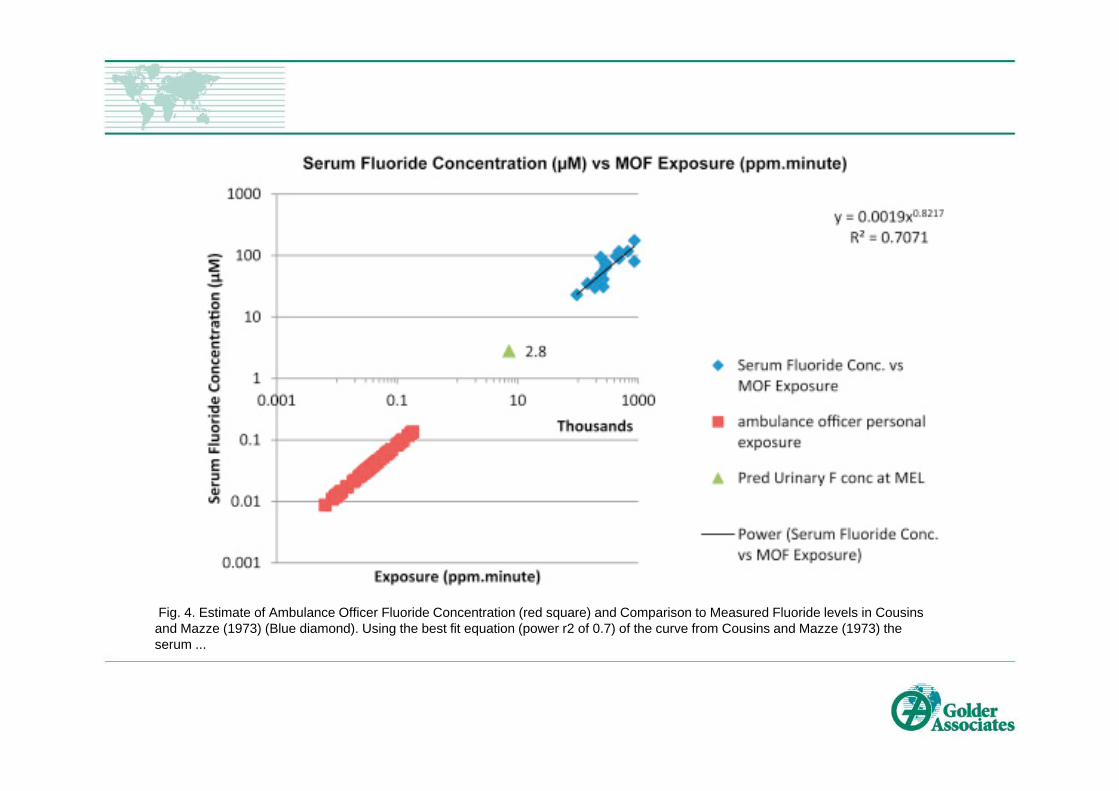
Fig. 4. Estimate of Ambulance Officer Fluoride Concentration (red square) and Comparison to Measured Fluoride levels in Cousinsand Mazze (1973) (Blue diamond). Using the best fit equation (power r2 of 0.7) of the curve from Cousins and Mazze (1973) the serum ...

Fig. 5. Modelled vapour concentrations in ambulance patient compartment at intensive usage rate of 1 vial/h (top) or 2 vial/h (bottom) with AC Chamber. A volume of 11.25 m3 and ACH of 46/h was assumed. Each peak represents a new vial being dispensed. The TWA (...

Fig. 6. Modelled MOF vapour concentrations in the TR, at intensive usage rates of 1(top) or 2 (bottom) vials/h with AC Chamber, assuming 32.4 m3 volume and 6 ACH. Each peak represents a new vial being dispensed. The TWA (0.74, 1.5 ppm) and peak concentrations ...

Uncertainties
Extrapolation from MAC to ppm Selection of dose groups Lack of d/r data on CNS effects Reliance on Cousins & Mazze - lack of d/r data on kidney toxicity in
human or animal studies
30

Acknowledgements
Antti Mikonnen Christin Down Sponsor Medical Developments International
31

References
1 Cousins, M. J. and Mazze, R. I. (1973). Methoxyflurane Toxicity A Study of Dose Response in Man. Journal of the American Medical Association. 225(13):1611-1616.
2 Mazze, R. I. (1984). Fluorinated anaesthesia nephrotoxicity: An Update. Canadian Anaesthetists’ Society Journal. 31(3):S16-22.
3 Medical Developments International. (2010). PENTHROX® (methoxyflurane) Inhalation. Product Information, Version 6. Melbourne, Australia.
4 National Library of Medicine. (n.d.). ChemIDplus Advanced Methoxyflurane Fact Sheet. United States of America. Available from: http://chem.sis.nlm.nih.gov/chemidplus/. (Accessed 12 April 2012).
5 Therapeutic Goods Administration. (2006). Safety of Methoxyflurane (Penthrox Inhalational Analgesic) – nephrotoxicity and hepatotoxicity. Resolution No 8945. Woden, Australian Capital Territory, Australia.
6 Frangos, J. (2001). Health Based Risk Assessment for Ambulance Officers Exposed to Methoxyflurane. Toxikos Toxicology Consultants. Victoria, Australia.
7 National Occupational Health and Safety Commission. (2005). Exposure Standard Documentation. Australia. Available from: http://hsis.safeworkaustralia.gov.au/DocumentationES.aspx?ID=303 (Accessed 20 Mar 2012).
32

References
8 The National Institute for Occupational Safety and Health (NIOSH). (1977). Criteria for a Recommended Standard: Occupational Exposure to Waste Anesthetic Gases and Vapors. DHEW (NIOSH) Publication No.77-140. Washington DC, United States of America.
9 Centre of Ambulance Services. (2009). COAS Clinical Practise Guidelines – Emergency Medical Technician as amended from PHECC CPG 3rd Edition. Dubai Corporation for Ambulance Services, Dubai, United Arab Emirates.
10 Chalgham, R. (24 October 2011). Abu Dhabi Police communication with Allan, G.
11 Hamad Medical Corporation. Ambulance Department Clinical Practise Guidelines.
12 Oxer, H. and Wilkes, G. J. (2007). Methoxyflurane is a safe, easy, effective analgesic for pre-hospital pain relief. St John Ambulance Western Australia, Australia.
13 Johnston, S., Wilkes, G., J., Thompson, J. A., Ziman, M. and Brightwell, R. (2011). Inhaled methoxyflurane and intranasal fentanyl for prehospital management of visceral pain in an Australian ambulance service. Emergency Medicine Journal. 28(1):57-63
14 Yakaitis, R. W. and Redding, J. S. (1970). Self-Administered Methoxyflurane. Anesthesia and Analgesia. 49(3):345-350.
33

References
15 Medical Developments International. (2012). Data on file.
16 Grindlay, J and Babl, F. E. (2009). Review article: Efficacy and safety of methoxyflurane analgesia in the emergency department and prehospital setting. Emergency Medicine Australasia. 21:4-11.
17 Gillis, M., Keirens, A., Steinkamm, C., Verbelen, J., Muysoms, W. and Reynders, N. (2008). The Use of Methoxyflurane (Penthrox) in the Emergency Department. Regional Anesthesia & Pain Medicine. 33(5):247
18 Buntine, P., Thom, O., Babl, F., Bailey, M. Bernard, S. (2007). Prehospital analgesia in adults using inhaled methoxyflurane. Emergency Medicine Australasia. 19:509–514.
19 Jacobs, I. G. (2010). Health Effects of Patients Given Methoxyflurane in the Pre-Hospital Setting: A Data Linkage Study. The Open Emergency Medicine Journal. 2010(3):7-13.
20 Yoshimura, N., Holaday, D.A. and Fiserova-Bergerova, V. (1976). Metabolism of methoxyflurane in man. Anesthesiology. 44(5) 372-379.
21 Mazze, R.I., Cousins, M.J. and Kosek, J.C. (1973). Strain differences in metabolism and susceptibility to the nephrotoxic effects of methoxyflurane in rats. Journal of Pharmacology and Experimental Therapeutics. 184(2):481-488.
34
References
22 Kharasch, E.D., Schroeder, J.L., Liggitt, H.D., Park, S.B., Whittington, D. and Sheffels, P. (2006). New insights into the mechanism of methoxyflurane nephrotoxicity and implications for anesthetic development (part 1): Identification of the nephrotoxic metabolic pathway. Anesthesiology. 105(4):726-736.
23 Kharasch, E.D., Schroeder, J.L., Liggitt, H.D., Ensign, D. and Whittington, D. (2006). New insights into the mechanism of methoxyflurane nephrotoxicity and implications for anestheticdevelopment (part 2): Identification of nephrotoxic metabolites. Anesthesiology. 105(4):737-745.
24 Corbett, T.H. and Ball, G.L. (1971). Chronic exposure to methoxyflurane a possible occupational hazard to anesthesiologists. Anesthesiology. 34(6):532-537.
25 Strum, D.P., Eger EI 2nd, Unadkat, J.D., Johnson, B.H. and Carpenter, R.L. (1991). Age affects the pharmacokinetics of inhaled anesthetics in humans. Anesthesia and Analgesia. 73(3):310-318.
26 Dahlgren, B.E. and Goodrich, B.H. (1976). Changes in kidney and liver function after methoxyflurane (penthrane) anaesthesia. British Journal of Anaesthesia. 48(2):145-149.
27 Dahlgren, B.E. (1977). Influence of methoxyflurane-nitrous oxide analgesia during childbirth on renal and hepatic function. British Journal of Anaesthesia. 49(12):1271-1276.
35

References
28 Abdullah, W. A., Sheta, S. A., and Nooh, N. S. (2011). Inhaled methoxyflurane (Penthrox) sedation for third molar extraction: a comparison to nitrous oxide sedation. Australian Dental Journal. 56(3):296-301
29 Dahlgren, B.E. (1979). Fluoride concentrations in urine of delivery ward personnel following exposure to low concentrations of methoxyflurane. Journal of Occupational Medicine. 21(9):624-626.
30 Mazze, R.I., Trudell, J.R. and Cousins, M.J. (1971). Methoxyflurane metabolism and renal dysfunction: Clinical correlations in man. Anesthesiology. 35(3):247-252.
31 Gilman, A.G., Goodman, L.S., Gilman, A., Meyer, S.E. and Melmon, K.L. (1980). Chapter 13 and Chapter 14. Goodman and Gilman’s The Pharmacological Basis of Therapeutics, 6th
edition. McGraw Hill, United States of America.
32 Kenna, J.G. and Jones, R.M. (1995). The organ toxicity of inhaled anesthetics. Anesthesia and Analgesia. 81(6 Suppl):S51-66.
33 Eger II, E.I. White, A.E, Brown, C.L, Biava, C.G, Corbett, T.H. and Stevens, W.C. (1978) A test of the carcinogenicity of enflurane, isoflurane, halothane, methoxyflurane and nitrous oxide in mice. Anesthesia and Analgesia. 57(6):678-694
36

References
34 Pope, W.D., Halsey, M.J., Lansdown, A.B., Simmonds, A. and Bateman, P.E. (1978). Fetotoxicity in rats following chronic exposure to halothane, nitrous oxide, or methoxyflurane, Anesthesiology. 48(1):11-16.
35 Wharton, R.S., Mazze, R.I., Baden, J.M., Hitt, B.A. and Dooley, J.R. (1978). Fertility, reproduction and postnatal survival in mice chronically exposed to halothane. Anesthesiology. 48(3):167-174.
36 International Agency for Research on Cancer. (1987). Overall evaluations of carcinogenicity, Anaesthetics, volatile. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans Overall Evaluations of Carcinogenicity: An Updating of IARC Monographs Volumes 1 to 42 Supplement 7. 93-95.
37 Pollard , T. (1990). Relative Addiction Potential of Major Centrally-Active Drugs and Drug Classes – Inhalants and Anaesthetics. Addiction Potential of Abused Drugs and Drug Classes. Editors; Erickson, I., Carlton K., Javors, M., A., Morgan, W, Stimmel, B. Haworth Press.
37

38

39

40

41

42

43

Fig. 1. Dose response data adapted from Cousins and Mazze (1973).

Fig. 3. Benchmark dose modelling results (using US EPA BMDS Wizard).