acute abdomen
TRANSCRIPT

The Acute AbdomenThe Acute Abdomen
ByBy
PROF/ GOUDA ELLABBANPROF/ GOUDA ELLABBAN
Department of General Department of General SurgerySurgery

IntroductionIntroduction
CommonCommon 5 – 10 admissions / 5 – 10 admissions / dayday
per 500,000 per 500,000 populationpopulation
VariableVariable Onset usually within 7 daysOnset usually within 7 days May require early surgeryMay require early surgery

Anatomy and Anatomy and PhysiologyPhysiology
Surface anatomySurface anatomy EmbryologyEmbryology
Somatic vs Visceral Somatic vs Visceral painpain
PathophysiologyPathophysiology

PathologyPathology
InflammatoryInflammatory
ObstructionObstruction HaemorrhageHaemorrhage IschaemiaIschaemia
(Trauma)(Trauma)

Making a diagnosisMaking a diagnosis
Not always absolutely necessaryNot always absolutely necessary
Careful historyCareful history
ExaminationExamination
InvestigationsInvestigations
History iHistory i
PainPain Site, radiationSite, radiation OnsetOnset Frequency, periodicityFrequency, periodicity Aggravating / relieving factorsAggravating / relieving factors Severity & type of painSeverity & type of pain

History iiHistory ii
Nausea + vomiting, appetiteNausea + vomiting, appetite Bowel habitBowel habit Gynaecological symptomsGynaecological symptoms Urinary symptomsUrinary symptoms Pat surgical / medical historyPat surgical / medical history Drug historyDrug history
Examination iExamination i
Begins as you first clap eyes on the Begins as you first clap eyes on the patient!patient!
AnalgesiaAnalgesia
Vital signs, Vital signs, general appearancegeneral appearance

Examination iiExamination iiAbdominal Abdominal
examinationexamination InspectionInspection movementmovement
scarsscars PalpationPalpation signs of peritonitissigns of peritonitis
swellings, massesswellings, massesdistensiondistension
PercussionPercussion AuscultationAuscultation bowel soundsbowel sounds

Signs of peritonitisSigns of peritonitis
TendernessTenderness GuardingGuarding RigidityRigidity Rebound tendernessRebound tenderness

Examination iiiExamination iii
Groins + external genitaliaGroins + external genitalia Rectal examinationRectal examination
UrinalysisUrinalysis

Investigations for Investigations for diagnosisdiagnosis
UrineUrine BloodBlood WCCWCC
AmylaseAmylase ImagingImaging
erect CXRerect CXRAXRAXRIVUIVUU/SU/SCTCT

Initial managementInitial management
Immediate operationImmediate operation
Resuscitation Resuscitation Emergency operationEmergency operation
ObservationObservationRepeated examinationRepeated examination

Common conditionsCommon conditions
AppendicitisAppendicitis CholecystitisCholecystitis DiverticulitisDiverticulitis PancreatitisPancreatitis Perforated peptic Perforated peptic
ulcerulcer
(Ischaemic gut)(Ischaemic gut)
Renal colic Renal colic
Intestinal Intestinal obstructionobstruction
GI bleedingGI bleeding Ruptured AAARuptured AAA
NSAPNSAP

Investigations for Investigations for managementmanagement
HaemoglobinHaemoglobin U+Es, CreatinineU+Es, Creatinine LFTsLFTs ABGsABGs Contrast x-raysContrast x-rays EndoscopyEndoscopy
(DPL)(DPL)

Central abdominal pain shifting to Central abdominal pain shifting to right iliac fossaright iliac fossa
Anorexia, constipationAnorexia, constipation Low grade feverLow grade fever RIF tendernessRIF tenderness
in ~50% of in ~50% of cases!cases!
Appendicitis!Appendicitis!
2 -3 day history2 -3 day history RUQ pain radiating to back / RUQ pain radiating to back /
shouldershoulder Vomiting, feverVomiting, fever
FebrileFebrile RUQ tenderness +/- Murphy’s signRUQ tenderness +/- Murphy’s sign


Elderly patientElderly patient Lower abdominal / LIF pain Lower abdominal / LIF pain FeverFever +/- altered bowel +/- altered bowel
habithabit
FeverFever LIF peritonitisLIF peritonitis

Severe upper abdominal painSevere upper abdominal painradiating to back and flanksradiating to back and flanks
Vomiting++Vomiting++
Dehydrated++Dehydrated++ Generalised peritonitisGeneralised peritonitis

PancreatitisPancreatitis

Severe upper abdominal painSevere upper abdominal pain Sudden onsetSudden onset History of indigestion, NSAID History of indigestion, NSAID
usageusage
Dehydrated, unwell, lying stillDehydrated, unwell, lying still Generalised peritonitisGeneralised peritonitis

Colicky abdominal painColicky abdominal pain VomitingVomiting ConstipationConstipation
absolute constipationabsolute constipation Dehydration, tachycardiaDehydration, tachycardia Abdominal distension, tendernessAbdominal distension, tenderness Scars, herniasScars, hernias


Younger patientYounger patient Colicky loin painColicky loin pain
radiation to groin, genitaliaradiation to groin, genitalia
Well, distressed by painWell, distressed by pain Unremarkable abdominal examUnremarkable abdominal exam Microscopic haematuriaMicroscopic haematuria

Sudden onsetSudden onset Severe back / left loin painSevere back / left loin pain History of hypertensionHistory of hypertension
ShockShock Absent femoral pulsesAbsent femoral pulses Pulsatile massPulsatile mass

Non-specific Abdominal Non-specific Abdominal PainPain
Very commonVery common Only a small proportion are Only a small proportion are
admittedadmitted
Pain is the predominant symptomPain is the predominant symptom Normal vital signs, investigationsNormal vital signs, investigations
Irritable Bowel SyndromeIrritable Bowel Syndrome

More unusual More unusual conditionsconditions
Rectus sheath haematomaRectus sheath haematoma Abdominal wall herniaAbdominal wall hernia
eg Spigelianeg Spigelian Medical causesMedical causes
PneumoniaPneumoniaMyocardial InfarctionMyocardial InfarctionPulmonary EmbolismPulmonary Embolism

The Acute AbdomenThe Acute Abdomen
BYBY
PROF/ GOUDA ELLABBANPROF/ GOUDA ELLABBAN

OutcomesOutcomes
1. Identify the organs and structures within the peritoneum
2. List four causes of abdominal dysfunction
3. Consider the causes and signs and symptoms of acute intestinal obstruction
4. Discuss vomiting and bowel movement in relation to abdominal dysfunction
5. Consider appendicitis, pancreatitis and peritonitis in relation to their effects upon the peritoneal cavity
.

Kidneys (retro-peritoneal)
Abdominal StructuresAbdominal Structures
Bladder, ureters, urethraCervix
Also:

Intestinal ObstructionIntestinal Obstruction• Partial or complete blockage of the small or large intestine.
The blockage may be mechanical or functional.
Mechanical causes include:
TumoursForeign BodiesImpacted FaecesIschaemia (Volvulus, Interssusception, Hernia, Clot)Inflammatory Bowel Disease
Adhesions
Functional cause:
Ileus – peristalsis stops

Tumour obstructionTumour obstruction

VolvulusVolvulus
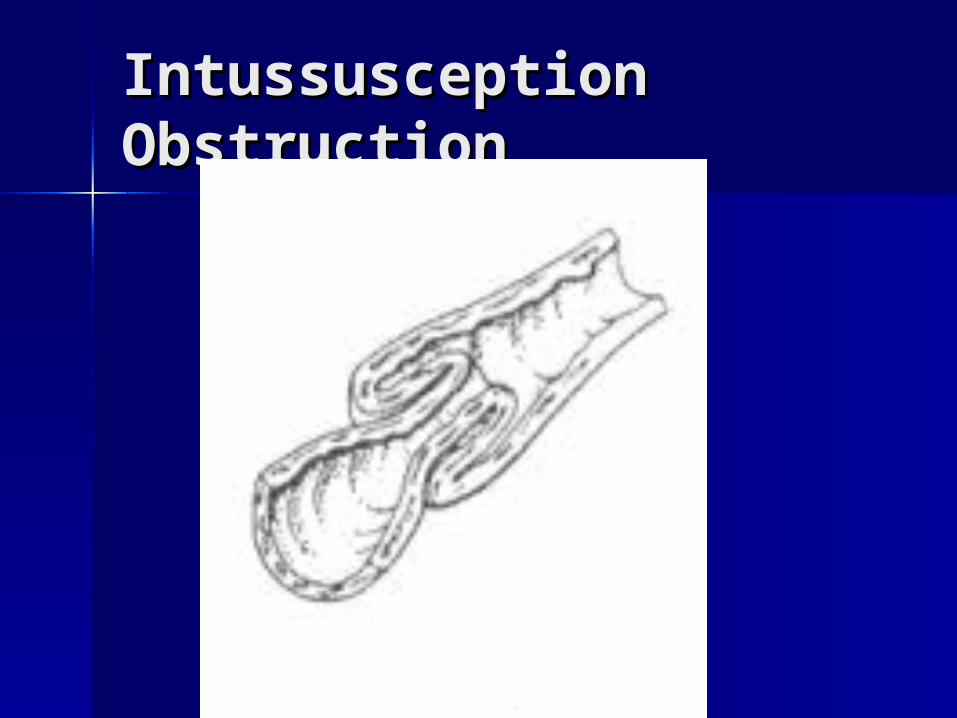
Intussusception Intussusception ObstructionObstruction

Ischaemic ObstructionIschaemic Obstruction
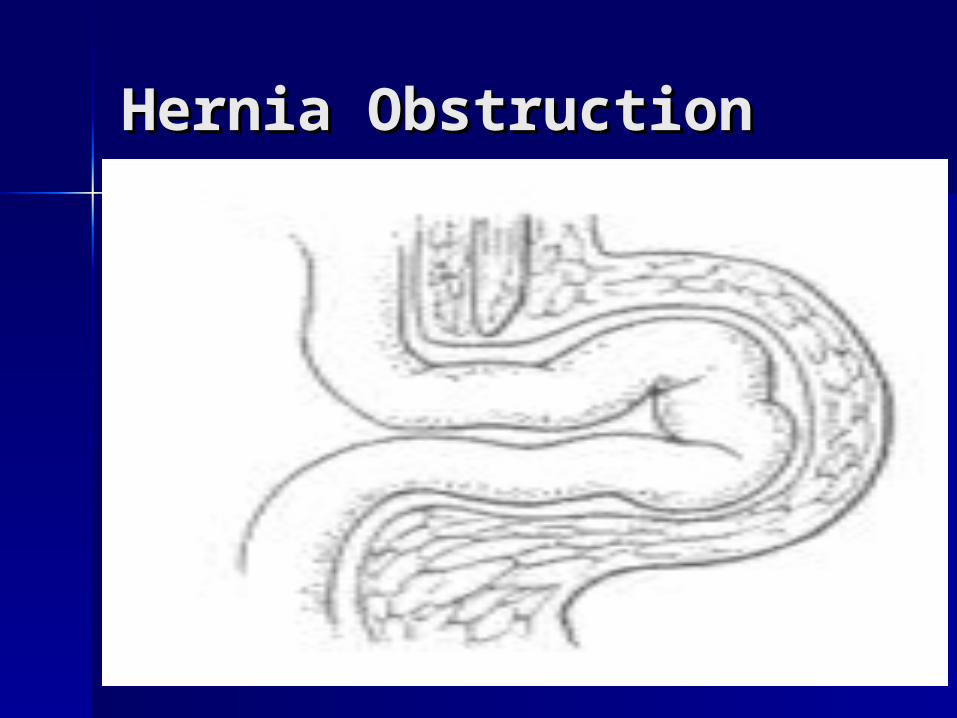
Hernia ObstructionHernia Obstruction
.
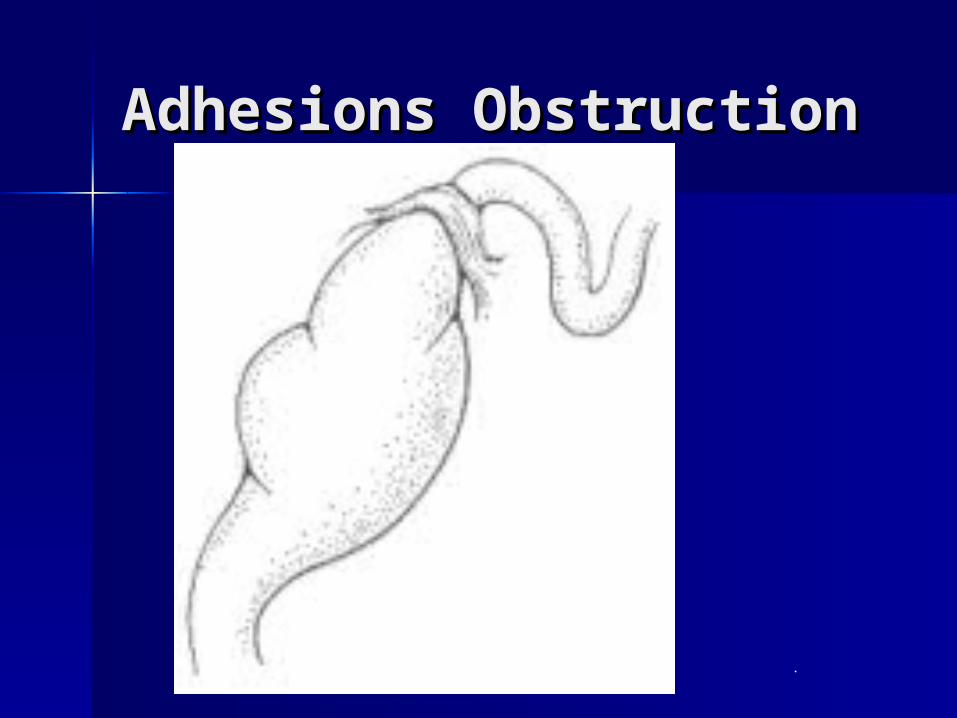
Adhesions ObstructionAdhesions Obstruction
.

Stages of obstructionStages of obstruction
Simple obstruction
Strangulated obstruction
Close-looped obstruction
©M.Bailey 2002

Problem ProgressionProblem Progression
• Depends upon site of problem
• Early – gas/fluid back-up behind obstruction
• Increased peristalsis / colicky pain/discomfort
• Abdominal distension increases
• Blood supply compromised (due to above), water drawn into bowel
• Sodium/Potassium pulled INTO intestines
• Bacteria activity increase
• Dehydration / Hypovolaemia signs appear

Clinical ManifestationsClinical Manifestations
• Pain / discomfort colicky in nature
• May have swollen abdomen
• May be abdominal guarding
• Nausea / vomiting may be evident
• May have slight fever
• Lack of bowel sounds / bowel movements as condition worsens

Principles of Principles of TreatmentTreatment
• Nil Orally (oral hygiene)
• Strict Input and Output Chart
• Drip and Suck
• Analgesia
• Antibiotics
• Surgical Investigation (Laparotomy then proceed)

VomitingVomiting
• Indicative of a problem developing
• Mucus and bile may be present – suggests upper GI tract obstruction
• Faecal matter/smell from vomit – suggests lower GI tract obstruction
• Risk of inhalation very real in the “ill patient”
• Keep Nil orally, Drip & Suck, Monitor
AppendicitisAppendicitis• General pain in abdomen – localises – RIF – rebound tenderness• May be vomiting and reduced/increased bowel sounds
• May have diarrhoea in the first instance – then nothing
• General Malaise, lethargy
• Low grade pyrexia
Management Principles:
• NBM
• Drip & Suck
• Monitor / Surgery

PancreatitisPancreatitis
Many causes
• Digestive enzymes (Amylase) from the pancreas start to eat away at the gland
• Can be life threatening
• Classic symptoms – Pain, nausea/vomiting and fever
• Blood results show High WCC and VERY high Amylase levels
• Management is NBM, Drip & Suck, Antibiotics, Analgesia, Monitor closely
PeritonitisPeritonitis
Two main causes:
Chemical cause:
Perforated GU, Pancreatitis, rupture of bladder, ovary or fallopians
Bacterial cause:
Inflammation of any sort (appendicitis, peptic ulcer, UC, Volvulus, strangulated obstruction, Neoplasm, Stab wound)
• Presentation varies – often weakness, pain, cold and shocked, nausea/vomiting
• Abdominal tenderness with direct/rebound tenderness
• Dehydration signs and high temperature are common features©M.Bailey 2002

Management of Management of PeritonitisPeritonitis
NBM
Drip & Suck
Analgesia
Antibiotics (IV usually)
Surgery – lavage with drainage and identify/treat cause
Acute AbdomenAcute Abdomen

Acute AbdomenAcute Abdomen
General name for presence of General name for presence of signs, symptoms of signs, symptoms of inflammation of peritoneum inflammation of peritoneum (abdominal lining)(abdominal lining)

Acute AbdomenAcute Abdomen
Determining exact cause Determining exact cause irrelevant in pre-hospital careirrelevant in pre-hospital care
Important factor is recognizing Important factor is recognizing acute abdomen is presentacute abdomen is present

HistoryHistory
Where do you hurt?Where do you hurt?– Know locations of major organsKnow locations of major organs– But realize abdominal pain locations But realize abdominal pain locations
do not correlate well with sourcedo not correlate well with source

HistoryHistory
What does pain feel like?What does pain feel like?– Steady pain - inflammatory processSteady pain - inflammatory process– Crampy pain - obstructive processCrampy pain - obstructive process

HistoryHistory
Was onset of pain gradual or Was onset of pain gradual or sudden?sudden?– Sudden = perforation, hemorrhage, Sudden = perforation, hemorrhage,
infarctinfarct– Gradual = peritoneal irrigation, Gradual = peritoneal irrigation,
hollow organ distensionhollow organ distension

HistoryHistory
Does pain radiate (travel) Does pain radiate (travel) anywhere?anywhere?– Right shoulder, angle of right Right shoulder, angle of right
scapula = gall bladderscapula = gall bladder– Around flank to groin = kidney, Around flank to groin = kidney,
ureterureter
HistoryHistory
Duration?Duration?– > 6 hour duration = ? surgical significance> 6 hour duration = ? surgical significance
Nausea, vomiting? Bloody? “Coffee Nausea, vomiting? Bloody? “Coffee Grounds”?Grounds”?
Any blood in GI tract = Emergency until proven otherwise

HistoryHistory
Change in urinary habits? Urine Change in urinary habits? Urine appearance?appearance?
Change in bowel habits? Change in bowel habits? Appearance of bowel movements? Appearance of bowel movements? Melena?Melena?

HistoryHistory
Regardless of underlying cause Regardless of underlying cause vomiting or diarrhea can be a vomiting or diarrhea can be a problem because of associated problem because of associated volume lossvolume loss

HistoryHistory
FemalesFemales– Last menstrual period? Last menstrual period? – Abnormal bleeding? Abnormal bleeding?
In females, abdominal pain = Gyn problem until proven otherwise

Physical ExamPhysical Exam
General AppearanceGeneral Appearance– Lies perfectly still Lies perfectly still inflammation, inflammation,
peritonitisperitonitis– Restless, writhing Restless, writhing obstruction obstruction
Abdominal distension?Abdominal distension? Ecchymosis around umbilicus, Ecchymosis around umbilicus,
flanks?flanks?

Physical ExamPhysical Exam
Vital signsVital signs– TachycardiaTachycardia ? Early shock (more ? Early shock (more
important than BP)important than BP)– Rapid shallow breathingRapid shallow breathing peritonitis peritonitis
Tilt test should be done with non-traumatic abdominal pain

Physical ExamPhysical Exam
Palpate each quadrantPalpate each quadrant– Work toward area of painWork toward area of pain– WarmWarm handshands– Patient on back, knee bent (if Patient on back, knee bent (if
possible)possible)– Note tenderness, rigidity, Note tenderness, rigidity,
involuntary guarding,voluntary involuntary guarding,voluntary guarding, massesguarding, masses

Physical ExamPhysical Exam
Bowel SoundsBowel Sounds– Listen 1 minute in each quadrantListen 1 minute in each quadrant– Listen Listen beforebefore feeling feeling– Absent bowel sounds Absent bowel sounds ileus, ileus,
peritonitis, shockperitonitis, shock
Auscultating bowel sounds has no pre-hospital value in trauma patients

ManagementManagement
AirwayAirway High concentration OHigh concentration O22
Anticipate vomitingAnticipate vomiting Anticipate hypovolemiaAnticipate hypovolemia Nothing by mouthNothing by mouth No analgesics, sedativesNo analgesics, sedatives

ManagementManagement
In In adults > 30adults > 30, consider possibility , consider possibility of referred of referred cardiac paincardiac pain..
In In femalesfemales, consider possible gyn , consider possible gyn problem, especially problem, especially tubal ectopictubal ectopic pregnancypregnancy

AppendicitisAppendicitis
Usually due to obstruction with Usually due to obstruction with fecalithfecalith
Appendix becomes swollen, Appendix becomes swollen, inflamed gangrene, possible inflamed gangrene, possible perforationperforation

AppendicitisAppendicitis
Pain begins periumbilical; moves to Pain begins periumbilical; moves to RLQRLQ
Nausea, vomiting, anorexiaNausea, vomiting, anorexia Patient lies on side; right hip, knee Patient lies on side; right hip, knee
flexedflexed Pain may Pain may notnot localize to RLQ if localize to RLQ if
appendix in odd locationappendix in odd location Sudden relief of pain = possible Sudden relief of pain = possible
perforationperforation

Duodenal Ulcer Duodenal Ulcer DiseaseDisease Steady, well-localized epigastric Steady, well-localized epigastric
painpain ““Burning”, “gnawing”, “aching”Burning”, “gnawing”, “aching” Increased by coffee, stress, spicy Increased by coffee, stress, spicy
food, smokingfood, smoking Decreased by alkaline food, Decreased by alkaline food,
antacidsantacids

Duodenal Ulcer Duodenal Ulcer DiseaseDisease May cause massive GI bleedMay cause massive GI bleed Perforation = intense, steady Perforation = intense, steady
pain, pt lies still, rigid abdomenpain, pt lies still, rigid abdomen
Kidney StoneKidney Stone
Mineral deposits form in kidney, move Mineral deposits form in kidney, move to ureterto ureter
Often associated with history of recent Often associated with history of recent UTIUTI
Severe flank pain radiates to groin, Severe flank pain radiates to groin, scrotumscrotum
Nausea, vomiting, hematuriaNausea, vomiting, hematuria Extreme restlessnessExtreme restlessness

Abdominal Aortic Abdominal Aortic AneurysmAneurysm Localized weakness of blood Localized weakness of blood
vessel wall with dilation (like vessel wall with dilation (like bubble on tire)bubble on tire)
Pulsating mass in abdomenPulsating mass in abdomen Can cause lower back painCan cause lower back pain Rupture shock, exsanguinationRupture shock, exsanguination

PancreatitisPancreatitis
Inflammation of pancreasInflammation of pancreas Triggered by ingestion of EtOH; large Triggered by ingestion of EtOH; large
amounts of fatty foodsamounts of fatty foods Nausea, vomiting; abdominal Nausea, vomiting; abdominal
tenderness; pain radiating from upper tenderness; pain radiating from upper abdomen straight through to backabdomen straight through to back
Signs, symptoms of hypovolemic Signs, symptoms of hypovolemic shockshock

CholecystitisCholecystitis
Inflammation of gall bladderInflammation of gall bladder Commonly associated with gall stonesCommonly associated with gall stones More common in 30 to 50 year old More common in 30 to 50 year old
femalesfemales Nausea, vomiting; RUQ pain, Nausea, vomiting; RUQ pain,
tenderness; fevertenderness; fever Attacks triggered by ingestion of fatty Attacks triggered by ingestion of fatty
foodsfoods

Bowel ObstructionBowel Obstruction
Blockage of inside of intestineBlockage of inside of intestine Interrupts normal flow of contentsInterrupts normal flow of contents Causes include adhesions, Causes include adhesions,
hernias, fecal impactions, tumorshernias, fecal impactions, tumors Crampy abdominal pain; nausea, Crampy abdominal pain; nausea,
vomiting (often of fecal matter); vomiting (often of fecal matter); abdominal distensionabdominal distension

Esophageal VaricesEsophageal Varices
Dilated veins in lower part of Dilated veins in lower part of esophagusesophagus
Common in EtOH abusers, Common in EtOH abusers, patients with liver diseasepatients with liver disease
Produce massive upper GI bleedsProduce massive upper GI bleeds

The Acute AbdomenThe Acute Abdomen
BYBY
PROF/ GOUDA ELLABBANPROF/ GOUDA ELLABBAN

Visceral PainVisceral Pain
To fully understand the patient’s To fully understand the patient’s complaint during a acute episode of complaint during a acute episode of abdominal pain the examiner must abdominal pain the examiner must possess a good understanding of the possess a good understanding of the neurophysiology and anatomy of painneurophysiology and anatomy of pain
Visceral pain reaches the central nervous Visceral pain reaches the central nervous system by three routes:system by three routes:– The parasympathetic nervesThe parasympathetic nerves– The sympathetic nervesThe sympathetic nerves– The somatic nervesThe somatic nerves

AnatoAnatomy and my and PhysiolPhysiology of ogy of VisceraVisceral Painl Pain

Multiple Faces of PainMultiple Faces of Pain
Pain can be characterized as:Pain can be characterized as:– SharpSharp– StabbingStabbing– BurningBurning– HeavyHeavy– DiffuseDiffuse– DullDull

Clinical ConsiderationsClinical Considerations
The patient with acute abdominal The patient with acute abdominal pain requires a thorough and pain requires a thorough and complete history and physical complete history and physical examination by an examination by an unhurriedunhurried examinerexaminer
It is important to assess the It is important to assess the clinical situation in detail including clinical situation in detail including pertinent laboratory studiespertinent laboratory studies

HistoryHistory
PainPain– The examiner should elicit the time of The examiner should elicit the time of
onset, its location and whether a change in onset, its location and whether a change in character occurs with various positionscharacter occurs with various positions
– The exact situation in which the onset of The exact situation in which the onset of pain occurs may be important in pain occurs may be important in establishing the diagnosisestablishing the diagnosis
– The original location of pain and its The original location of pain and its shifting or changing in position may shifting or changing in position may provide a clue to the diagnosisprovide a clue to the diagnosis

HistoryHistory
VomitingVomiting– May result from severe painMay result from severe pain– May be related to the GI tractMay be related to the GI tract– Almost always occurs with obstruction of the Almost always occurs with obstruction of the
small intestine (and provides temporary relief)small intestine (and provides temporary relief)– The timing of emesis to pain may provide The timing of emesis to pain may provide
important diagnostic cluesimportant diagnostic clues– The character of emesis, including the volume, The character of emesis, including the volume,
color and content is pertinent in regard to color and content is pertinent in regard to bowel obstructionbowel obstruction

HistoryHistory
AnorexiaAnorexia– Is uncommon for patients with acute Is uncommon for patients with acute
abdominal pain to desire foodabdominal pain to desire food– May precede the onset of painMay precede the onset of pain

HistoryHistory
BowelsBowels– Constipation, diarrhea and a recent Constipation, diarrhea and a recent
change in bowel habits are change in bowel habits are important in the diagnosis of important in the diagnosis of patients with abdominal painpatients with abdominal pain
– The failure to pass flatus associated The failure to pass flatus associated with cramping pain and vomiting with cramping pain and vomiting strongly supports mechanical strongly supports mechanical obstructionobstruction

HistoryHistory
MenstruationMenstruation– An accurate menstrual history is An accurate menstrual history is
especially valuable in the especially valuable in the assessment of abdominal pain in the assessment of abdominal pain in the femalefemale
– Any change in the volume of Any change in the volume of menstrual flow is also pertinentmenstrual flow is also pertinent

HistoryHistory
Past illnessesPast illnesses– Past illnesses especially previous Past illnesses especially previous
abdominal operations is importantabdominal operations is important– Any history of similar pain in the Any history of similar pain in the
pastpast

Physical ExamPhysical Exam
Should start with the patient’s Should start with the patient’s appearance, body posture and appearance, body posture and degree of obvious paindegree of obvious pain
Inspection, auscultation, Inspection, auscultation, palpation and percussionpalpation and percussion

Diagnostic ImagingDiagnostic Imaging
Flat and upright abdominal films (the most Flat and upright abdominal films (the most common first step)common first step)– AirAir– Calcific densities (stones, eggshell)Calcific densities (stones, eggshell)– Mechanical obstruction / ileusMechanical obstruction / ileus
UltrasonographyUltrasonography CT scanCT scan Specific organ studiesSpecific organ studies
– IVPIVP– HIDAHIDA
AngiographyAngiography

Laboratory StudiesLaboratory Studies
The results obtained from laboratory The results obtained from laboratory information may or may not play a information may or may not play a significant role in the decision for significant role in the decision for operationoperation– Complete blood countComplete blood count– UrinalysisUrinalysis– Serum amylase and lipaseSerum amylase and lipase– Liver function studiesLiver function studies– HCGHCG– Serum electrolytesSerum electrolytes
PeritonitisPeritonitis
Patients with abdominal pain may show Patients with abdominal pain may show tenderness to palpation of the abdomentenderness to palpation of the abdomen
If peritoneal irritation exist they have If peritoneal irritation exist they have rebound tendernessrebound tenderness
Localized inflammation of the anterior Localized inflammation of the anterior parietal peritoneum may lead to voluntary parietal peritoneum may lead to voluntary muscle guardingmuscle guarding
An inflammatory response may involve the An inflammatory response may involve the entire intra-abdominal cavity or only a entire intra-abdominal cavity or only a portion of either the visceral or parietal portion of either the visceral or parietal peritoneumperitoneum

Peritonitis (Continued)Peritonitis (Continued)
Primary or spontaneous peritonitisPrimary or spontaneous peritonitis– Caused by bacterial infection without an apparent Caused by bacterial infection without an apparent
intra-abdominal source of infectionintra-abdominal source of infection– There are different common bacteria for adults There are different common bacteria for adults
and childrenand children Secondary peritonitisSecondary peritonitis
– Caused as a result of bacterial contamination Caused as a result of bacterial contamination from a known source within the abdomen from a known source within the abdomen (perforation or trauma)(perforation or trauma)
Chemical peritonitisChemical peritonitis– Inflammation from substances other than bacteria Inflammation from substances other than bacteria
(gastric contents) bacterial infection soon follows(gastric contents) bacterial infection soon follows

Signs and Symptoms Signs and Symptoms of Peritonitisof Peritonitis
Usually associated with the abrupt onset of Usually associated with the abrupt onset of abdominal pain, often localized at first and then abdominal pain, often localized at first and then spreading throughout the abdomenspreading throughout the abdomen
The physical findings depend on etiology and The physical findings depend on etiology and duration and whether the process is diffuse or duration and whether the process is diffuse or localizedlocalized
Fever is usually present early and may disappearFever is usually present early and may disappear The abdomen is usually distended with hypoactive The abdomen is usually distended with hypoactive
bowel soundsbowel sounds Tenderness to percussion and palpation is present Tenderness to percussion and palpation is present
in all four quadrantsin all four quadrants
Signs and Symptoms Signs and Symptoms of Peritonitis of Peritonitis (Continued)(Continued) Early recognition of peritoneal Early recognition of peritoneal
irritation is importantirritation is important Management includesManagement includes
– NG tubeNG tube– Restoration of volumeRestoration of volume– Insertion of Foley catheterInsertion of Foley catheter– Intravenous antibiotics (broad Intravenous antibiotics (broad
spectrum)spectrum)– Hemodynamic monitoring (Swan)Hemodynamic monitoring (Swan)

Organ Subsystem Organ Subsystem AnalysisAnalysis
GastrointestinalGastrointestinal RenalRenal GynecologicGynecologic VascularVascular CardiacCardiac
NeurologicNeurologic HematologicHematologic MetabolicMetabolic PulmonaryPulmonary MusculoskeletalMusculoskeletal

Gastrointestinal Gastrointestinal SubsystemSubsystem The most common cause of acute The most common cause of acute
abdominal pain in the gastrointestinal abdominal pain in the gastrointestinal system is associated with an system is associated with an inflammatory or mechanical process of inflammatory or mechanical process of the:the:– StomachStomach– Small and large intestineSmall and large intestine– GallbladderGallbladder– Common bile ductCommon bile duct– LiverLiver– PancreasPancreas

Perforated Peptic Perforated Peptic UlcerUlcer More commonly results from a duodenal More commonly results from a duodenal
ulcer than a gastric ulcerulcer than a gastric ulcer Commonly seen in males between the Commonly seen in males between the
third and fourth decade of lifethird and fourth decade of life Manifest as sudden, sharp, severe pain Manifest as sudden, sharp, severe pain
located first in the epigastrium and later located first in the epigastrium and later over the entire abdomenover the entire abdomen
Nausea is frequent however vomiting is an Nausea is frequent however vomiting is an unusual occurrenceunusual occurrence
The patient usually lies in the supine The patient usually lies in the supine position avoiding any undue motionposition avoiding any undue motion

Perforated Peptic Perforated Peptic Ulcer (Continued)Ulcer (Continued)
Respirations are shallow (the patient avoids deep Respirations are shallow (the patient avoids deep breathing or coughing) breathing or coughing)
Palpation of the abdomen reveals a firm Palpation of the abdomen reveals a firm appearance (boardlike)appearance (boardlike)
Rebound tenderness is the rule in all four Rebound tenderness is the rule in all four quadrants and is worse in the epigastric region.quadrants and is worse in the epigastric region.
Rectal exam is unremarkableRectal exam is unremarkable White blood counts are usually elevated (12 to White blood counts are usually elevated (12 to
20,000)20,000) Abdominal films demonstrate free air in the Abdominal films demonstrate free air in the
abdomen (75 percent of cases)abdomen (75 percent of cases)

Acute CholecystitisAcute Cholecystitis
Most commonly occurs in females between Most commonly occurs in females between 30-60 years of age with a previous history of 30-60 years of age with a previous history of pregnancypregnancy
Younger patients have a family history of Younger patients have a family history of biliary tract disease biliary tract disease
The usual presentation is a constant dull The usual presentation is a constant dull right upper quadrant painright upper quadrant pain
Nausea and vomiting is common (emesis is Nausea and vomiting is common (emesis is green)green)
The blood pressure is usually not altered and The blood pressure is usually not altered and the heart rate is seldom greater than 100the heart rate is seldom greater than 100

Acute Cholecystitis Acute Cholecystitis (Continued)(Continued) Examination of the abdomen reveals Examination of the abdomen reveals
mild to moderate distention sometimes mild to moderate distention sometimes showing asymmetry(in RUQ)showing asymmetry(in RUQ)
Bowel sounds are hypoactiveBowel sounds are hypoactive Tenderness is maximal in the RUQ with Tenderness is maximal in the RUQ with
deep inspirationdeep inspiration Frequently a mass may be palpated Frequently a mass may be palpated
along the right costal marginalong the right costal margin The White blood count is elevated (10-The White blood count is elevated (10-
13,000)13,000)

Acute Cholecystitis Acute Cholecystitis (Continued)(Continued) Ultrasound can rapidly assess the Ultrasound can rapidly assess the
caliber of the biliary tree, stones or caliber of the biliary tree, stones or their absence, the contents of the their absence, the contents of the gallbladder and its appearancegallbladder and its appearance
HIDA (radioenuclide) studies may HIDA (radioenuclide) studies may assist in the diagnosis when not assist in the diagnosis when not confirmed by ultrasoundconfirmed by ultrasound
CT scan’s play limited role in its CT scan’s play limited role in its diagnosisdiagnosis

Acute PancreatitisAcute Pancreatitis
Presents with sudden onset of severe Presents with sudden onset of severe epigastric pain radiating directly to the back epigastric pain radiating directly to the back and around both costal marginsand around both costal margins
Can be confused with acute perforation of Can be confused with acute perforation of peptic ulcerpeptic ulcer
The disease is associated with biliary tract The disease is associated with biliary tract disease or chronic alcohol intakedisease or chronic alcohol intake
Is usually seen in patients between 30-50 Is usually seen in patients between 30-50 years of ageyears of age
Anorexia, nausea and vomiting are common Anorexia, nausea and vomiting are common (emesis rarely provides significant relief)(emesis rarely provides significant relief)

Acute Pancreatitis Acute Pancreatitis (Continued)(Continued)
Hypotension is rarely evident early in the Hypotension is rarely evident early in the disease but may develop 4-6 hours laterdisease but may develop 4-6 hours later
Abdominal tenderness is usually in the Abdominal tenderness is usually in the epigastric areaepigastric area
Bowel sounds are usually hypoactive or absentBowel sounds are usually hypoactive or absent Classic findings:Classic findings:
– Grey Turner’s signGrey Turner’s sign– Cullens signCullens sign
White blood count is elevated (12-22,000)White blood count is elevated (12-22,000) The key diagnostic test-serum amylaseThe key diagnostic test-serum amylase

Acute AppendicitisAcute Appendicitis
A common cause of abdominal painA common cause of abdominal pain Difficult to dx in patients <3 and >70Difficult to dx in patients <3 and >70 Abd pain usually starts in the epigastrium, Abd pain usually starts in the epigastrium,
gradually migrates to the periumbilical area gradually migrates to the periumbilical area and finally ends in the RLQ (after 6 hrs)and finally ends in the RLQ (after 6 hrs)
Anorexia, nausea and vomiting are all Anorexia, nausea and vomiting are all commoncommon
The abdomen is tender to palpation with The abdomen is tender to palpation with rebound tenderness rebound tenderness

Acute Appendicitis Acute Appendicitis (Continued)(Continued) Retrocecal appendix may cause Retrocecal appendix may cause
only mild abdominal tendernessonly mild abdominal tenderness Abdominal distention is rarely Abdominal distention is rarely
present in the early stagespresent in the early stages Rectal exam yields extreme pain to Rectal exam yields extreme pain to
palpation on the right palpation on the right WBC +/- elevationWBC +/- elevation Ultrasound and CT scan may be Ultrasound and CT scan may be
helpfulhelpful

Differential DiagnosisDifferential Diagnosis
Perforated ulcerPerforated ulcer Acute diverticulitisAcute diverticulitis Ruptured graafian follicleRuptured graafian follicle Ectopic pregnancyEctopic pregnancy PIDPID Renal or ureteral calculiRenal or ureteral calculi

Meckel’s DiverticulaMeckel’s Diverticula
May produce bleeding and May produce bleeding and intestinal obstructionintestinal obstruction
The disease is uncommon but The disease is uncommon but should be considered in patients should be considered in patients with appendicitiswith appendicitis
The diagnosis is made at time of The diagnosis is made at time of operationoperation

Acute DiverticulitisAcute Diverticulitis
Congenital or acquiredCongenital or acquired Results from an inflamed diverticulaResults from an inflamed diverticula Usually involves the left colon (sigmoid)Usually involves the left colon (sigmoid) Presents as LLQ pain, chills and fever Presents as LLQ pain, chills and fever
(101-104)(101-104) Presents with history of constipation but Presents with history of constipation but
anorexia and vomiting are uncommonanorexia and vomiting are uncommon The abdomen is usually slightly The abdomen is usually slightly
distended with LLQ tenderness distended with LLQ tenderness

Acute Diverticulitis Acute Diverticulitis (Continued)(Continued) Bowel sounds - hypoactiveBowel sounds - hypoactive WBC - increased (10-20,000)WBC - increased (10-20,000) Patients sometimes improve with Patients sometimes improve with
medical Tx if this is the case BE medical Tx if this is the case BE should be performed in 4-6 weeks should be performed in 4-6 weeks to R/O colon cancer to R/O colon cancer

Acute Obstruction of Acute Obstruction of the Small Intestinethe Small Intestine
Symptoms are usually sudden, sharp, colicky Symptoms are usually sudden, sharp, colicky abdominal pain that is often periumbilicalabdominal pain that is often periumbilical
Between episodes of pain the patient usually Between episodes of pain the patient usually feels quite wellfeels quite well
Nausea and vomiting occur soon after the onset Nausea and vomiting occur soon after the onset of pain and emesis may relieve the painof pain and emesis may relieve the pain
The color of emesis is green at first (contains bile) The color of emesis is green at first (contains bile) changing to a yellow brown with a feculent odorchanging to a yellow brown with a feculent odor
Inspection of the abdomen can provide important Inspection of the abdomen can provide important diagnostic clues (previous incisions, ventral or diagnostic clues (previous incisions, ventral or inguinal hernia or peristaltic waves)inguinal hernia or peristaltic waves)

Acute Obstruction of Acute Obstruction of the Small Intestine the Small Intestine (Continued)(Continued) Abdominal distention does not occur with Abdominal distention does not occur with
obstruction of the proximal jejunum but is obstruction of the proximal jejunum but is common with distal jejunum or ileal common with distal jejunum or ileal obstructionsobstructions
Auscultation of the abdomen reveals Auscultation of the abdomen reveals hyperactive bowel soundshyperactive bowel sounds
Visible peristaltic waves can be seen in Visible peristaltic waves can be seen in patients with distal obstructionpatients with distal obstruction
Laboratory data reveals an increase Laboratory data reveals an increase hematocrit due to dehydration. The white hematocrit due to dehydration. The white blood cell count is elevated (12-20K)blood cell count is elevated (12-20K)

Acute Obstruction of Acute Obstruction of the Small Intestine the Small Intestine (Continued)(Continued) Supine and erect abdominal films Supine and erect abdominal films
are most helpful in mid to distal SBOare most helpful in mid to distal SBO Barium contrast studies is valuable Barium contrast studies is valuable
in confirming the diagnosis and in confirming the diagnosis and upper obstructionsupper obstructions
Ultrasonography may also be of Ultrasonography may also be of benefitbenefit
Paralytic ileus vs. mechanical Paralytic ileus vs. mechanical obstructionobstruction
Most Common Causes Most Common Causes of Abdominal Pain of Abdominal Pain Secondary to Secondary to Obstructing Lesions of Obstructing Lesions of the Gastrointestinal the Gastrointestinal TractTract Jejunum and ileumJejunum and ileum
– MalignancyMalignancy– VolvolusVolvolus– AdhesionsAdhesions– IntussusceptionIntussusception
ColonColon– MalignancyMalignancy– Volvolus-cecal or sigmoidVolvolus-cecal or sigmoid– DiverticulitisDiverticulitis

Acute Obstruction of Acute Obstruction of the Large Intestinethe Large Intestine Occurs more often in patients older than 40Occurs more often in patients older than 40 Patients sometime complain of progressive Patients sometime complain of progressive
constipation (over several months) with or constipation (over several months) with or without thin pencil size stools streaked with without thin pencil size stools streaked with blood (distal colon)blood (distal colon)
Is gradual in onset and presents as Is gradual in onset and presents as constipation with abdominal distentionconstipation with abdominal distention
Pain is minimal or absent unless peritonitis Pain is minimal or absent unless peritonitis occursoccurs
Nausea and vomiting do not usually occur Nausea and vomiting do not usually occur until the later stages of diseaseuntil the later stages of disease

Acute Obstruction of Acute Obstruction of the Large Intestine the Large Intestine (Continued)(Continued) The abdomen appears distended The abdomen appears distended
and tympanic to percussionand tympanic to percussion Rectal exam is usually Rectal exam is usually
unremarkableunremarkable Laboratory studies-hematocrit and Laboratory studies-hematocrit and
WBC are usually normalWBC are usually normal Diagnosis can usually be made by Diagnosis can usually be made by
supine and erect abdominal filmssupine and erect abdominal films

Ruptured Abdominal Ruptured Abdominal Aortic AneurysmAortic Aneurysm Almost always presents as abdominal Almost always presents as abdominal
painpain With acutely expanding aneurysms With acutely expanding aneurysms
patients can present with a history of patients can present with a history of back pain for several daysback pain for several days
Physical exam demonstrates a Physical exam demonstrates a pulsatile midline abdominal masspulsatile midline abdominal mass
Abdominal films may demonstrate a Abdominal films may demonstrate a calcified “eggshell” aortacalcified “eggshell” aorta
Abdominal ultrasound can be helpfulAbdominal ultrasound can be helpful
Gynecologic DiseaseGynecologic Disease
Is a common cause of acute Is a common cause of acute abdominal painabdominal pain
A thorough history and complete A thorough history and complete pelvic and rectal exam is importantpelvic and rectal exam is important
Plain films of the abdomen usually Plain films of the abdomen usually are not helpfulare not helpful
Pelvic ultrasound is the diagnostic Pelvic ultrasound is the diagnostic examination of choiceexamination of choice

Acute SalpingitisAcute Salpingitis Most commonly due to gonococcal infectionMost commonly due to gonococcal infection Usually seen in the 15-35 year age groupUsually seen in the 15-35 year age group Pain is usually at the pubic symphysis (midline) Pain is usually at the pubic symphysis (midline)
and radiates to the right and left lower quadrantsand radiates to the right and left lower quadrants The pain usually does not have gastrointestinal The pain usually does not have gastrointestinal
complaintscomplaints Bowel sounds are hypoactiveBowel sounds are hypoactive Cervical tenderness is severeCervical tenderness is severe A vaginal discharge is frequent and diagnostic A vaginal discharge is frequent and diagnostic
when culturedwhen cultured

Ovarian TumorOvarian Tumor
Pain is usually sudden and Pain is usually sudden and located in either right or left lower located in either right or left lower abdomen depending on which abdomen depending on which ovary is involvedovary is involved
Pelvic examination is the key Pelvic examination is the key diagnostic maneuver, a palpable diagnostic maneuver, a palpable mass may confirm the suspicionmass may confirm the suspicion

Ectopic PregnancyEctopic Pregnancy May present as a sudden lower abdominal May present as a sudden lower abdominal
pain that is sharp persistent, with or without pain that is sharp persistent, with or without nausea and vomitingnausea and vomiting
Usually occurs during the first trimesterUsually occurs during the first trimester The patient’s history is the most important The patient’s history is the most important
factor in the diagnosisfactor in the diagnosis After rupture peritonitis insurersAfter rupture peritonitis insurers The pain worsens with timeThe pain worsens with time If blood loss is significant hypotension and If blood loss is significant hypotension and
tachycardia may developtachycardia may develop

Ectopic Pregnancy Ectopic Pregnancy (Continued)(Continued) Pelvic examination may demonstrate Pelvic examination may demonstrate
blood in the vagina or cervical osblood in the vagina or cervical os Motion to the cervix is painful and an Motion to the cervix is painful and an
adnexal mass is often palpableadnexal mass is often palpable The cervix is frequently blueThe cervix is frequently blue Laboratory data-hematocrit is low, Laboratory data-hematocrit is low,
WBC is slightly increased and HCG is WBC is slightly increased and HCG is positivepositive
The simplest and most accurate study The simplest and most accurate study is ultrasoundis ultrasound

Nonsurgical Causes of Nonsurgical Causes of the Acute Abdomenthe Acute Abdomen Bacterial peritonitisBacterial peritonitis Sickle cell anemiaSickle cell anemia GastroenteritisGastroenteritis Pseudomembranous colitisPseudomembranous colitis Lead poisoningLead poisoning Acute porphyriaAcute porphyria Right or left lower lobe pneumoniaRight or left lower lobe pneumonia Myocardial infarctionMyocardial infarction

The EndThe End