acute abdomen.pptx
TRANSCRIPT

ACUTE ABDOMEN
Definition: Acute abdomen is a term applied to acute abdominal pain.
That is spontaneous, non-traumatic for which urgent interference may be necessary
The items of this lecture are discussed in details in their corresponding
chapters. The intention is to discuss in brief the important points in clinical
presentation and investigations.
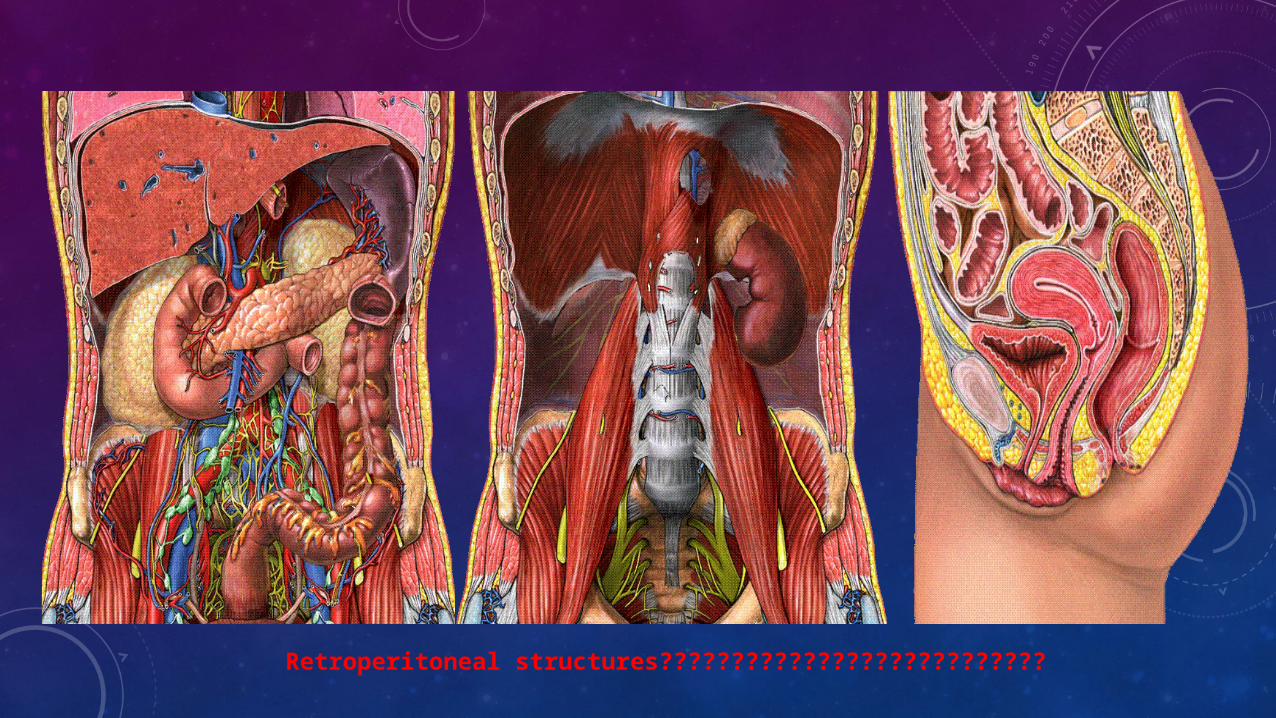
Retroperitoneal structures???????????????????????????

TYPES OF PAINVISCERAL ,SOMATIC , REFERRED PAIN AND SHIFTING PAIN
Visceral pain: is usually due to distension or spasm of a hollow viscus, ischemic
pain and inflammation. It is felt in the segment of the abdominal wall having the
same nerve supply of the affected organ and it is vague ill defined pain so;
Mediated by autonomic nerve fibers
FOREGUT PAIN (stomach and duodenum) is felt in the epigastrum.
MID-GUT PAIN (jejunum to transverase colon) is felt in the peri-umbilical region.
HIND-GUT PAIN (transverse colon to anal canal) is felt in the lower abdomen.

The abdominal organs are sensitive to
Spasm or distension
inflammation
strangulation
Somatic pain is due to irritation of the parietal peritoneum and so it is well
localized over the affected organ.
Mediated by afferent somatic nerve fibers.
The presence of these two types of pain explains why the initial pain of acute appendicitis is vague and is felt in the umbilical
region, but later it becomes localized to the right iliac fossa.
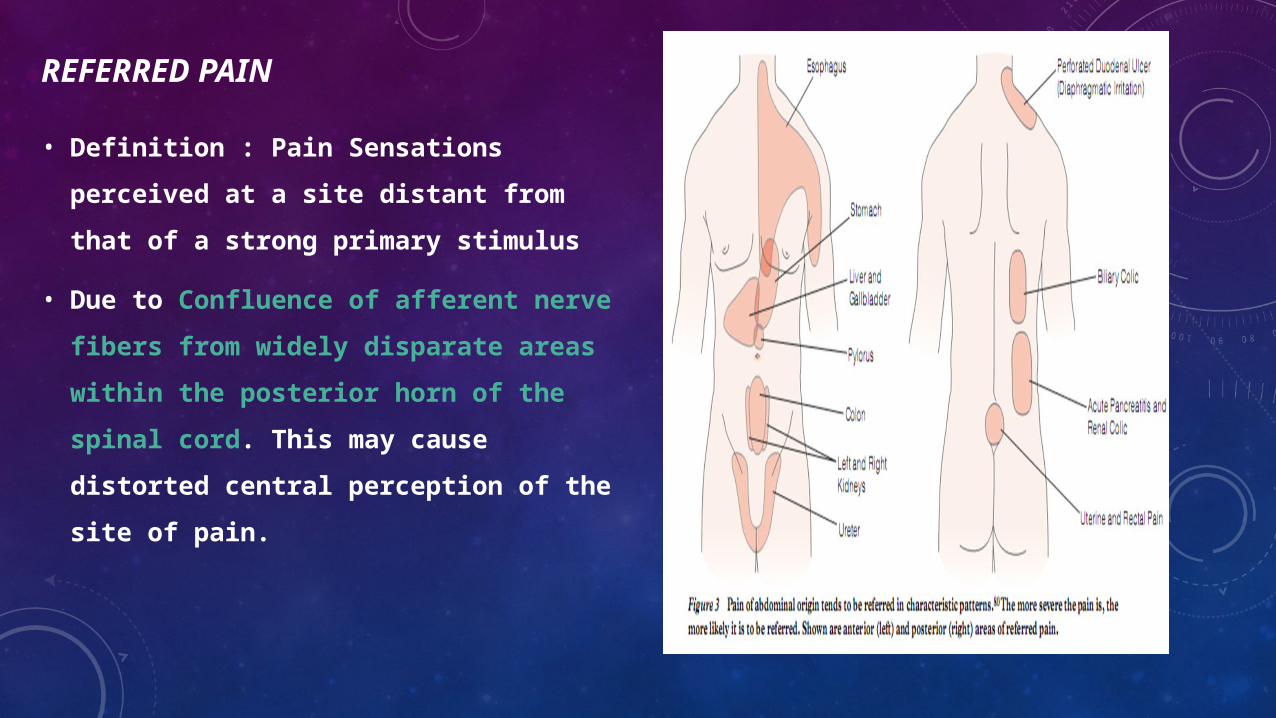
REFERRED PAIN
• Definition : Pain Sensations
perceived at a site distant from that
of a strong primary stimulus
• Due to Confluence of afferent nerve
fibers from widely disparate areas
within the posterior horn of the
spinal cord. This may cause
distorted central perception of the
site of pain.

Usually ipsilateral to the involved organureteric obstruction - ipsilateral testicular pain
supra/subdiaphragmatic irritation- ipsilateral supraclavicular

Classification of causes of acute abdomen:
According to the mode of presentation: abdominal pain may be due to:oColics ; Intestinal and Biliary.
o inflammation: Appendicitis, Cholecystitis, Pancreatitis, Diverticulitis, as Meckel’s diverticulitis.
oPerforations : Perforated appendix, Peptic ulcer, gall bladder, Diverticulum, and typhoid ulcer of the small bowel.
o Intestinal obstruction: Simple, Strangulation
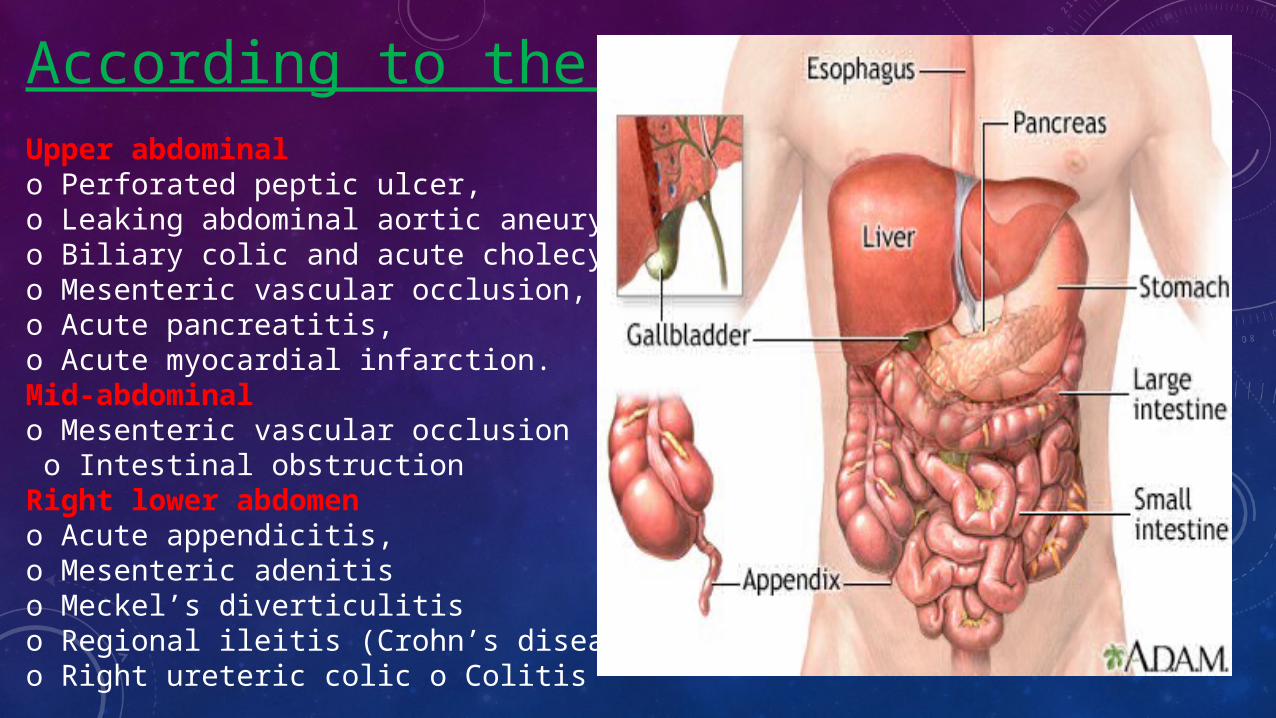
According to the siteUpper abdominalo Perforated peptic ulcer, o Leaking abdominal aortic aneurysm, o Biliary colic and acute cholecystitis, o Mesenteric vascular occlusion, o Acute pancreatitis, o Acute myocardial infarction.Mid-abdominalo Mesenteric vascular occlusion o Intestinal obstructionRight lower abdomeno Acute appendicitis, o Mesenteric adenitis o Meckel’s diverticulitiso Regional ileitis (Crohn’s disease) o Right ureteric colic o Colitis
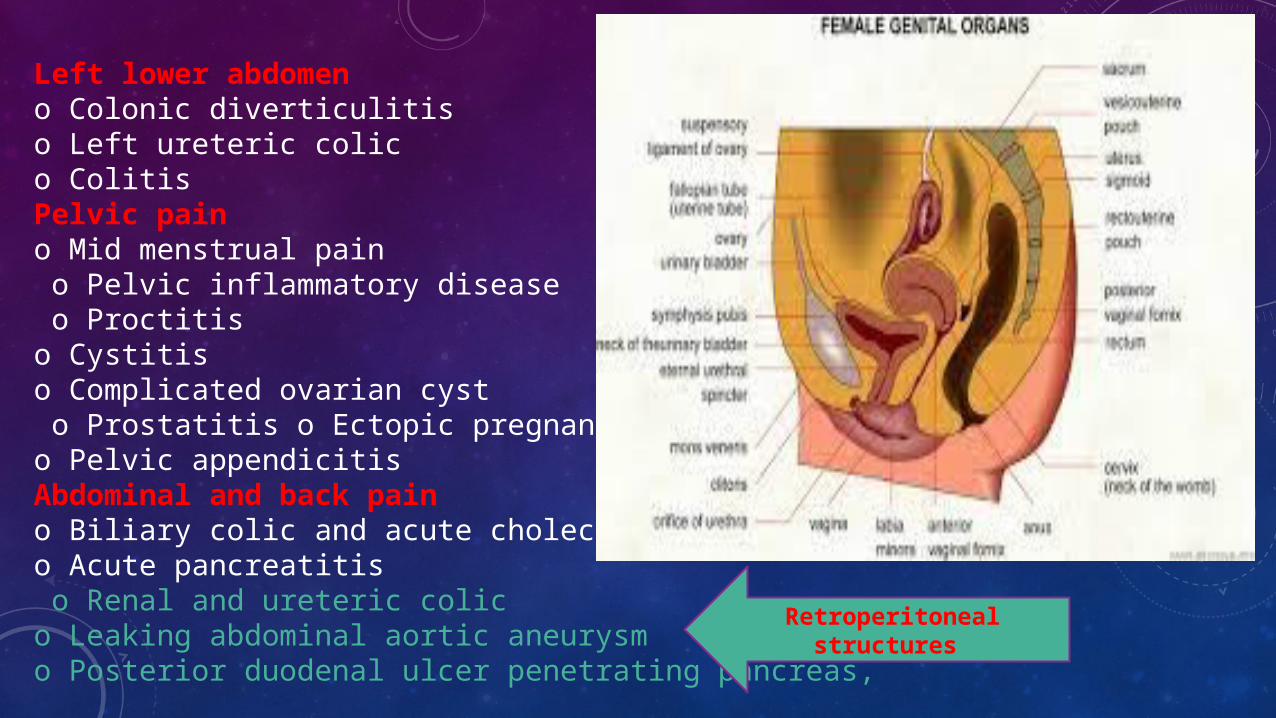
Left lower abdomeno Colonic diverticulitis o Left ureteric colic o ColitisPelvic paino Mid menstrual pain o Pelvic inflammatory disease o Proctitis o Cystitiso Complicated ovarian cyst o Prostatitis o Ectopic pregnancy o Pelvic appendicitisAbdominal and back paino Biliary colic and acute cholecystitis o Acute pancreatitis o Renal and ureteric colic o Leaking abdominal aortic aneurysm o Posterior duodenal ulcer penetrating pancreas,
Retroperitoneal structures

ACUTE ABDOMINAL PAINCAN PRESENT TO(which spatiality)
surgeon
medicine
urologist
gynecologist

SOME DETAILS ON COMMON CAUSES
• Acute appendicitis • Acute cholecystitis • Acute pancreatitis • Perforated peptic ulcer • Acute intestinal obstruction

•Gynecological Pathologies• Ruptured ectopic pregnancy
• Twisted ovarian cyst
• Salphingitis
• Ruptured ovarian cyst
• Tubo-ovarion abscess
•Mid cyclic pain

EXTRA ABDOMINAL CAUSES
• Myocardial infarction • Pneumonia• Diaphragmatic pleurisy • Herpeszoster • Medical causes • Malaria • Porphyria • Sickle cell anemia

COMMON INFLAMMATORY CONDITIONS

ACUTE APPENDICITISIt can affect any age, but is commonest in the second and third decades. There is usually a
characteristic shifting pattern of pain from the center to the right lower abdomen.
o Pain always occurs before vomiting.
o Diarrhoea is usually against the diagnosis.
Anorexia and nausea are almost always present.
INVESTIGATIONS ARE DONE IN DIFFICULT CASES:o Leucocytic count: Polymorphnuclear leucocytosis
• Abdominal and pelvic ultrasonography: if in doubt
o If a ureteric calculus or UTI is suspected, urine examination, plain X-ray PUT, IVU and
ultrasound are diagnostic,
o In females, if a tubo-ovarian or uterine problem is suspected, a pelvic ultrasound and
laparoscopy are helpful.

ACUTE CHOLECYSTITIS• The initial pain is diffuse and colicky in the upper abdomen. Later it
localizes in the right hypochondrium.
• It is difficult to palpate the gall bladder (20%), due to the overlying
tenderness and rigidity.
ULTRASOUND IS DIAGNOSTIC:
o Gall stones are detected in 95% of cases,
o Distension of the gall bladder,
o Thickened walls,
o Pericholecystic fluid collection,
ACUTE PANCREATITIS• Severe epigastric pain that increases in intensity
• Pain is referred to the back.
• Profuse vomiting is a prominent feature.
• The patient may be shocked.
• Tenderness and guarding are slight.
• Serum amylase rises. Many other conditions raise the serum amylase.
• CT may reveal enlargement of the pancreas, peripancreatic fluid collection, or pancreatic
necrosis.

ACUTE DIVERTICULITIS• Rare before the age of 40.
• Sigmoid colon is the commonest site.
• Diagnosis relies mainly on the clinical picture.
• Gastrografin enema may be helpful.
• Barium enema should be postponed till after resolution of the acute attack.
• CT may reveal localized thickening of the colonic wall, density in the pericolic
fat or a pericolic abscess.

INTESTINAL OBSTRUCTION

SIMPLE BOWEL OBSTRUCTION• Colicky abdominal pains
• Vomiting
• Abdominal distension
• Absolute constipation.
• Plain X-ray will reveal distended loops or fluid
levels.

STRANGULATION INTESTINAL OBSTRUCTION• Severe pain which is persistent and is not relieved by nasogastric suction.
• Localized tenderness and guarding.
• Fever and tachycardia.
• Leucocytosis.
MESENTERIC ISCHAEMIA• This is actually a type of strangulation intestinal obstruction.
• Suspect the diagnosis in patients over 50 years with valvular or atherosclerotic heart disease,
arrhythmias, hypotension, hypovolaemia, myocardial infarction, or polycythaemia.
• The pain is out of proportion to abdominal findings.
• Plain X-ray may reveal ground glass appearance.
• Ultrasound and CT scans may show the occluding thrombus, bowel wall oedema or abnormal
gas patterns.

GYNAECOLOGICAL CAUSES

Ruptured ovarian cyst• There is lower abdominal pain, tenderness and guarding.
• No toxemia.
• Abdominal and pelvic ultrasound examinations are diagnostic.
Torsion of an ovarian cyst• Severe lower lateral abdominal pain.
• Adnexal mass may be palpable.
• Ultrasound is diagnostic.
• Laparoscopy is diagnostic and therapeutic.
Pelvic inflammatory disease (PID)• Suspect the disease in females in the reproductive period.
• UD increases the possibility.
• Inflammation is usually bilateral, but may be severer on one side.
• There is lower abdominal tenderness and guarding with high pyrexia.
• Per vaginal examination and movement of the cervix are tender.

Ruptured ectopic pregnancy• History of menstrual abnormalities may be present.
• Severe lower abdominal pain.
• Pallor is usually a striking feature.
• Abdominal examination reveals tenderness and guarding.
• Per vaginal examination reveals tender cervix.
• Chorionic gonadotropin testing is positive.
• Ultrasound. The presence of a gestational sac in the
uterus is against the diagnosis. Free blood is present in
the pelvis.
• Laparoscopy is very helpful.
MANAGEMENT PLAN
• Resuscitation and monitoring• History: personal history menstrual history, analysis of
pain, past history of (surgery –medical diseases –drugs)• Examination• Investigation• Treatment
ABDOMINAL PAIN(HISTORY) Onset; course (Progression of pain)
Duration.
Site of pain: at onset, at present.
Radiation of Pain
Severity.
• Type: intermittent colicky, sharp persistent
Aggravating factors: movement, coughing, food
Relieving factors: position, drug, food

OTHER GIT SYMPTONS• VOMITING • ABDOMINAL DISTENTION• CONSTIPATION/DIARRHOEA
OTHER SYSTEMS • Urinary Symptoms• Gynecological Symptoms
GENERAL EXAMINATION:
• Pulse• Temperature • Respiratory rate • Blood pressure• Dehydration

INSPECTION:
Mobility : limited mobility on inspiration
Contour: may show abdominal distension
• Don’t forget to examine Hernial orifices , DRE
PALPATION:
Guarding• Voluntary abdominal wall spasm elicited by palpation, make the
examination difficult specially in children.
• Over come by distracting the patient with simple conversation.
• It is mediated consciously by the patient
RIGIDITY:-This is involuntary spasm of abdominal wall muscle in the
presence of peritonitis.
REBOUND TENDERNESS:- Characteristic feature of peritonitis Elicited by sudden release of hand over the tender area, patient
experiences severe pain as inflamed peritoneum hit the abdominal musculature.

• PERCUSSION• Tympanitic air /dull fluid or pus in the peritoneum
• Auscultation• Listen bowel sounds for at least two minutes• Exaggerated in mechanical intestinal obstruction• Absent (ileus) due to toxic effect of the pus on the abdominal
motility
• Rectal and vaginal examination

AFTER COMPLETE HISTORY AND EXAMINATION WE PUT
Provisional diagnosis
• Special signs of some causes of acute abdomen (discussed in the clinical part)• Appendicitis
• Cholecystitis

INVESTIGATIONS
LABORATORY IMAGING LAPAROSCOPY

In the majority of cases accurate clinical examination supplemented by few tests can confirm the diagnosis.
The following are some useful investigations.
Laboratory investigations• Full blood picture.• Urea and electrolytes.• Blood sugar.• Serum amylase.• Urine analysis.
Radiological investigationsPlain x rayPlain X-ray of the chest in the erect position may show free gas under the cupola of the diagram in perforation of a viscus. A basal pneumonia will be detected.
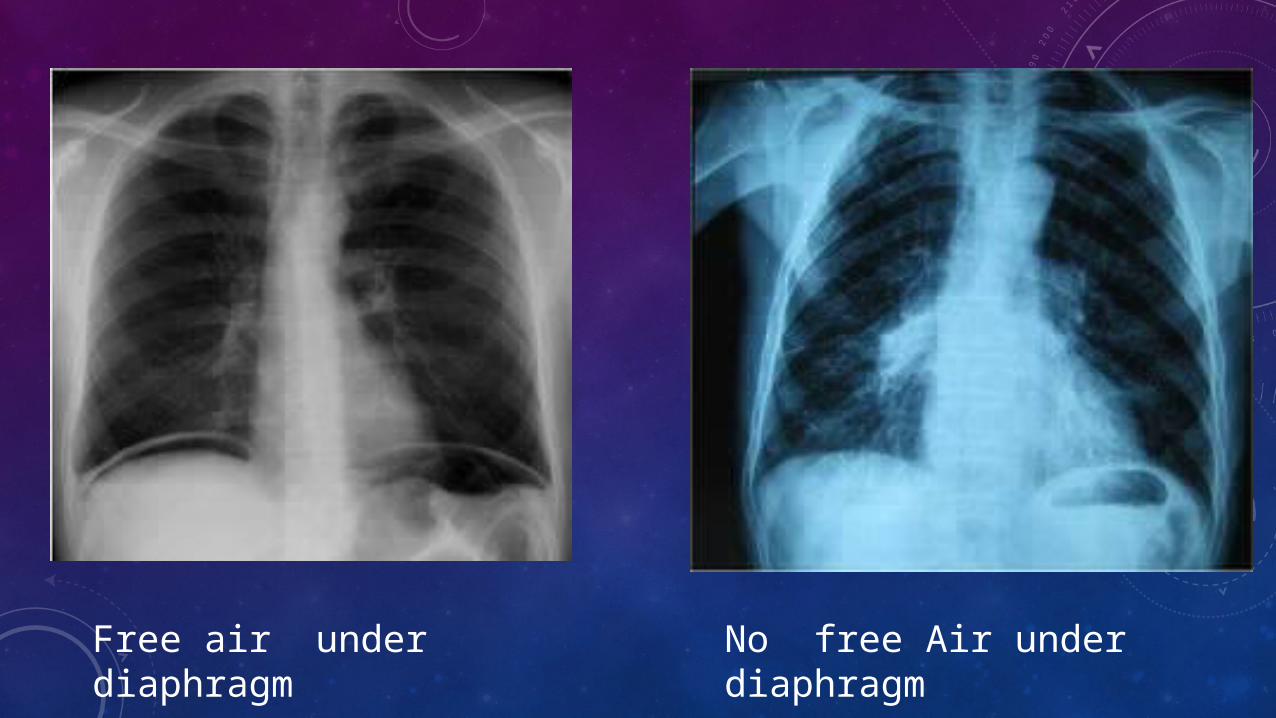
Free air under diaphragm No free Air under diaphragm

Distended loops of bowel or fluid levels in intestinal obstruction.
Plain X-ray of the abdomen may reveal: Calculi of the urinary tract

Abdominal ultrasound can diagnose the following:
Acute calcular cholecystitis. Stones are detected in 95% of cases. The gall bladder is distended, its wall is thickened
and subserosal oedema may be visualized.Acute pancreatitis. Enlargement of the pancreas, pancreatic pseudocyst or abscessLeaking aortic aneurysm.Distended pelvicalyceal system in cases where ureteric stones cause colic.Gynaecological disorders. Ruptured ovarian cyst, twisted ovarian cyst, ectopic pregnancy and pelvic inflammatory disease are easily detected by pelvic ultrasound.

CT scan of the abdomen: The main advantage of CT scan is that its picture is neither affected by obesity nor by the presence of gases. It is very helpful for the diagnosis of the following conditions:
• Acute pancreatitis. • Retroperitoneal haemorrhage.• Bowel infarction. • Splenic infarction.• Diverticulitis. bowel wall thickness is detected And abscess can be visualized.• Localized fluid collection or free fluid in the peritoneal cavity.
Diagnostic laparoscopy:
Diagnostic laparoscopy is valuable especially for
gynecological problems

TREATMANT OF EACH CAUSE

THANK YOU