acute infection with microbes and their · pdf fileacute infection with microbes and their...
TRANSCRIPT

Acute Infection with Microbes and
Their Consequences
Mark Riddle, MD, DrPH
Associate Professor
Dept. of Preventive Medicine & Biostatistics
Uniformed Services University of the Health Sciences
Bethesda, Maryland
Gastrointestinal Tract in Health and Disease
Detoxification
Digestive tract
Immunity
Food allergies
Autoimmune diseases
Mix-ups
Post-infectious sequelae

Acute enteric infection risk: 50M in US each year
(Centers for Disease Control & Prevention, 2015)

…and their consequences
Irritable Bowel Syndrome Guilliane Barre Syndrome
Functional constipation
Reactive arthritis
Hemolytic Uremic Syndrome
Reflux/Dyspepsia Celiac disease
Inflammatory Bowel Disease
Tropical sprue

Case Study: Campylobacter in the Netherlands
In the Netherlands, with
approximately 80,000
cases of gastroenteritis
per year, the costs of
illness caused by
campylobacteriosis are
about 21 million Euros
per year (Silva, 2011).

Sudden, permanent sequelae
Progressive disease
Immune process
Persistent infection
Infe
cti
on
Symptomatic disease
Symptomatic disease
Dysbiotic process Symptomatic disease
Infectious Causes of Chronic Disease Association Causation Mechanism
EXAMPLES
•polio, malaria, meningitis
•histoplasmosis,
lyme disease
•rheumatic arthritis,
systemic lupus, GBS
•Hepatitis B virus, H. pylori,
HPV, HIV
•IBS, obesity, ? mood
disorders…
Adapted from O’Conner, et al, EID, Vol. 12, No. 7, July 2006.

Important non-GI Post-infectious
Complications of Enteric Infections
• Leading cause of paralysis worldwide
• Rare: 1–2 per 100,000 per year
• 1 per 1,058 Campy infections
• Occurs 1-3 weeks following Shigella , Salmonella , and Campy infections (1-4%)
• Persists in 15 – 30% of patients
• HLA-B27 genetic predisposition for more severe disease
Guerry P and Szymanski C, Trends Microbiol 2008;16:428
Campylobacter & Guillain-Barré Syndrome Post-dysenteric Reactive Arthritis
Hannu T. Ann Rheum Dis 2005;64:594-598

Post-dysenteric colitis (a.k.a. post-infectious Irritable Bowel Syndrome [PI-IBS])
8

Study
Viral Porter (‘12) Norovirus
Unspecified
Diarrhea Porter (‘10)
Marshall (‘06)
Cumberland (‘03)
ICD-9 code (infect. diarrhea)
Self-reported diarrhea
Medical care for acute GE
Exposure specifics
1 10 20
Jung (‘09)
Parry (‘02)
Porter (‘10)
Rodriguez (‘99)
Porter (‘13)
Wang (‘04)
Marshall (‘06)
Ji (‘05)
Mearin (‘05)
Thabane (‘10)
Bacterial
Shigella
Campylobacter, Salmonella
Campy, Shigella, Salmonella
Bacterial gastroenteritis
Shigella, Salm, Yers, Campy
Shigella
Campylobacter, EHEC
Shigella
Salmonella
Campylobacter, EHEC
Risk Risk
Odds Ratio (95% CI)
Exposure
Okhuysen (‘04) Travelers’
Diarrhea
Ilnyckyi (‘03)
Riddle (‘11)
Porter (‘11)
Stermer (‘06)
Pitzurra (‘11)
Mexico
55 different countries
Middle East Iraq / Afghanistan
Asia, Africa, S America SE Asia, S Asia, E Africa
Zanini (‘12) Norovirus
Consistency of Acute Infectious Gastroenteritis and IBS Association Is Strong

PI-IBS can be a chronic (? life-long) problem
• In US military active duty, visits
persist in 20-30% of cases
• Likely underestimates persistence
of symptoms
• 42% persistence at 8 years
after Campy/STEC infection (Marshall et al.Gut 2010)
• 57% persistence at 6 years
follow-up (Neal et al. Gut 2002)
• 63% persistence at 5 years
after Shigella infection (Jung et al. J Clin Gastro 2009)
Years after initial medical encounter
0 1 2 3 4 5 6 7
% w
ith
IB
S v
isit
20
40
60
80
100 All cases
Any IGE
Bacterial IGE
Viral IGE
0
Porter et al. Am J Gastro 2010

Overall
Mearin et al. 2005
Parry et al. 2003
Ford et al. 2010
2.18 (1.70, 2.81)
5.55 (2.62, 11.74)
2.91 (0.48, 17.71)
OR (95% CI)
2.45 (1.74, 3.44)
Porter et al. 2011 1.65 (0.68, 4.02)
Porter et al. 2013 1.51 (1.09, 2.08)
Porter et al. 2011 2.45 (2.15, 2.80)
Porter et al. 2012 1.42 (0.83, 2.43)
1 .1 1 10
Tuteja et al. 2008 3.09 (0.61, 15.72) Trivedi et al. 2011 2.79 (0.34, 23.03)
Self-Report
Record Review
Subtotal 2.83 (2.10, 3.81)
Subtotal 1.81 (1.26, 2.58)
Post-infectious Dyspepsia (? GERD)
Risk Risk
Pike et al. Amer J Gastro. 2013

Evidence for Post-C. difficile FGD Is Also Emerging
Among active duty personnel, C. difficile
infection was independently associated
with gastrointestinal sequelae
“New-onset IBS is common (25%)
after CDI. Longer CDI duration,
current anxiety and higher BMI are
associated with the diagnosis of
C. difficile PI-IBS.”
September 2016
Gutierrez RL, et.al. Gastroenterology 2015;149:1406-14.

Something Is Going on with the Microbiome in PI-IBS

• Invasive organisms and intestinal
barrier mucosal disruption
Putative Pathogen Specific Trigger Mechanisms
A. Epithelial tight junctions disruption
B. Δ cellular polarity/receptor relocation
C. internalization of non-invasive E. coli
D. Defective NOD2 interaction/regulation
Kalischuk. 2009; Glenn. 2009.
• Enterotoxigenic E. coli
heat-labile toxin-
mediated effects on
barrier disruption via lipid
raft sloughing
• tight junction disruption
• ? “adjuvanted” response
to commensals

Acute Gastrointestinal Infection Can Induce Long-Lived Microbiota-Specific T Cell Responses
• Each infection at barrier
surfaces represents an
additional opportunity for the
reactivation of commensal-
specific T cells
• May be beneficial through
promoting innate and adaptive
effect mechanisms
• May be harmful if results in
dysregulation of microbiome
and/or altered barrier function
Belkaid Y. Trends Immunol. 2013; Hand TW. Science. 2012.

Digestive Disease Sciences, 2014
❶
❷
❸
❹
❺
CdtB
ICCs
❻
Vinculin - human membrane
cystoskeletal protein
CdtB - cytolethal
distending toxin,
B subunit

Immunological Biomarkers of Postinfectious Irritable Bowel Syndrome
• Serum at time of initial ICD-9-CM diagnosis for IBS onset
(or matched time of censure for healthy controls)
• Biomarkers: cytokines, microbiome antigens (C. Elson) & vinculin
• DoD Serum Repository:
pilot study
• Groups:
– ❶ & ❸ PI-IBS
– ❷ healthy (GI infx)
– ❹ idiopathic-IBS
1 3
4
2
4
3
2
3
1 1
4

Geometric Mean and Std. Deviation by Group; Fold-Changes (FC) <1 are presented as x = -1/FC.
Antibodies Directed against Antigens of Gut Commensals
Differed between PI-IBS Cases and Those IBS Cases
Lacking a Prior IGE Episode
“idiopathic” IBS
[Mean (SD)] n = 30
PI-IBS (all cause)
[Mean (SD)] n = 60
FC p-Value
MDR254 (IgG) 193.56 (18.93) 898.84 (7.35) 4.64 0.0134
CBir8 (IgA) 3.07 (10.80) 9.33 (28.52) 3.04 0.0444
EF20 (IgG) 819.83 (8.19) 2245.54 (6.05) 2.74 0.0291
rIB16 (IgG) 287.15 (8.89) 753.18 (3.62) 2.62 0.0314
P3 (IgG) 268.14 (5.43) 615.91 (2.32) 2.30 0.0156
rIB19 (IgG) 5686.21(2.79) 9149.92 (1.73) 1.61 0.0227

Anti-Vinculin Antibody Higher in Campylobacter
Specific PI-IBS vs Other PI-IBS
Post-”Other”
IBS – [Mean (SD)]
n = 20
Post-Campy IBS [Mean (SD)]
n = 10
FC p-Value
Vinculin (IgG) 337.65 (5.51) 1251.38 (3.27) 3.71 0.0217 <<

Emerging concern about ESBL (Extended-Spectrum
β-Lactamase) producing Enterobacteriacea carriage
• 10-80% of travelers may be
colonized with ESBL-PE
• Risk Factors: region, TD; abx
use; diet, hospital exposure
• Growing argument to avoid
antibiotics in TD treatment
• May be a transient
phenomenon? (Ruppe, 2015) Kantele, 2015
• Colonization by less virulent strains/ pathovars (Vading, 2016)
• Nonetheless, dissemination from healthy travelers to vulnerable
individuals, and bacterial conjugation to more virulent strains must still
be considered
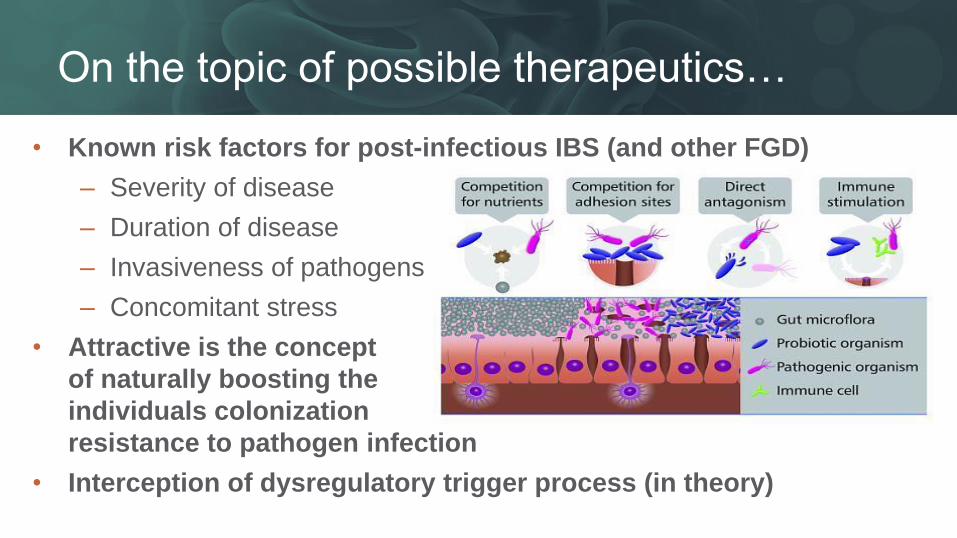
On the topic of possible therapeutics…
• Known risk factors for post-infectious IBS (and other FGD)
– Severity of disease
– Duration of disease
– Invasiveness of pathogens
– Concomitant stress
• Attractive is the concept
of naturally boosting the
individuals colonization
resistance to pathogen infection
• Interception of dysregulatory trigger process (in theory)

• Probiotics: Four meta-analyses have been published, only one
showed a significant pooled effect – Ritchie ML, Romanuk TN. PLoS ONE. 2012
– McFarland LV. Travel Medicine and Infectious Disease. 2007
– Takahashi O et al. J Clin Gastroenterol. 2007
– Sazawal S et al. Lancet Infectious Diseases. 2006.
“Difficult to interpret the findings given differing probiotic species,
formulations and dosages, and methodological problems within the
studies themselves (i.e. poor compliance, recall bias).”
• Prebiotics/synbiotics: preventive effects in TD is limited and mixed – Cummings J et al. Aliment Pharmacol Ther. 2001
– Drakoularakou A et al. Eur J Clin Nutr. 2010
– Virk A et al. Journal of Travel Medicine. 2013
Am J Gastro, April 2016

Practical Advice for the Clinician (Part 1)
Diagnosis
• Work-up cases of dysentery, moderate–severe disease, and symptoms lasting >7 days to clarify the etiology and enable specific directed therapy.
Treatment
• Don’t use antibiotics routinely for community acquired diarrhea (mostly viral)
• Do encourage use of single dose antibiotic therapy (with loperamide) for treatment of travelers’ diarrhea
Counseling
• Prevention counseling of acute enteric infection is not routinely recommended but may be considered in the individual or close contacts of the individual who is at high risk for complications.

Practical Advice for the Clinician (Part 2)
Prophylaxis
• Bismuth subsalicylates have moderate effectiveness and may be considered for travelers who do not have any contraindications to use and can adhere to the frequent dosing requirements
• Probiotics, prebiotics, and synbiotics for prevention of TD are not recommended.
• Antibiotic chemoprophylaxis has moderate to good effectiveness and may be considered in high-risk groups for short-term use.
Gaps
• No current guidelines on work-up of post-infectious FGD
• No unique studies evaluating therapeutic effectiveness in PI-FGD
• No studies evaluating effect of TD prevention on reduction of PI-FGD risk
• Studies evaluating TD prevention in IBS patients are needed

• Naval Medical Research Center
– Chad Porter, Brian Pike, Ramiro Gutierrez
• Armed Forces Health Surveillance Center
– Angie Eick-Cost and entire staff AFHSC/DoDSR staff
• University of Alabama
– Chuck Elson, Ben Christmann
• Uniformed Services University
– David Tribble
• The study protocols of presenter’s data were approved by institutional review boards in compliance with
all applicable Federal regulations governing the protection of human subjects.
• Funding: Department of Defense, International Society of Travel Medicine
Acknowledgements/Disclaimers

Photograph courtesy of J. Besser, MN Dept Health
If only our next meal came with a warning…
Questions?