adenomatous polyp in the gallbladder - isciiiscielo.isciii.es/pdf/diges/v96n8/imagenes.pdfel manejo...
TRANSCRIPT
Adenomatous polyp in the gallbladder
M. Menduiña Guillén, P. Alaminos García and M. Valenzuela Barranco
Departament of Medicine. University of Granada. Spain
1130-0108/2004/96/8/584-585REVISTA ESPAÑOLA DE ENFERMEDADES DIGESTIVASCopyright © 2004 ARÁN EDICIONES, S. L.
REV ESP ENFERM DIG (Madrid)Vol. 96. N.° 8, pp. 584-585, 2004
PICTURES IN DIGESTIVE PATHOLOGY
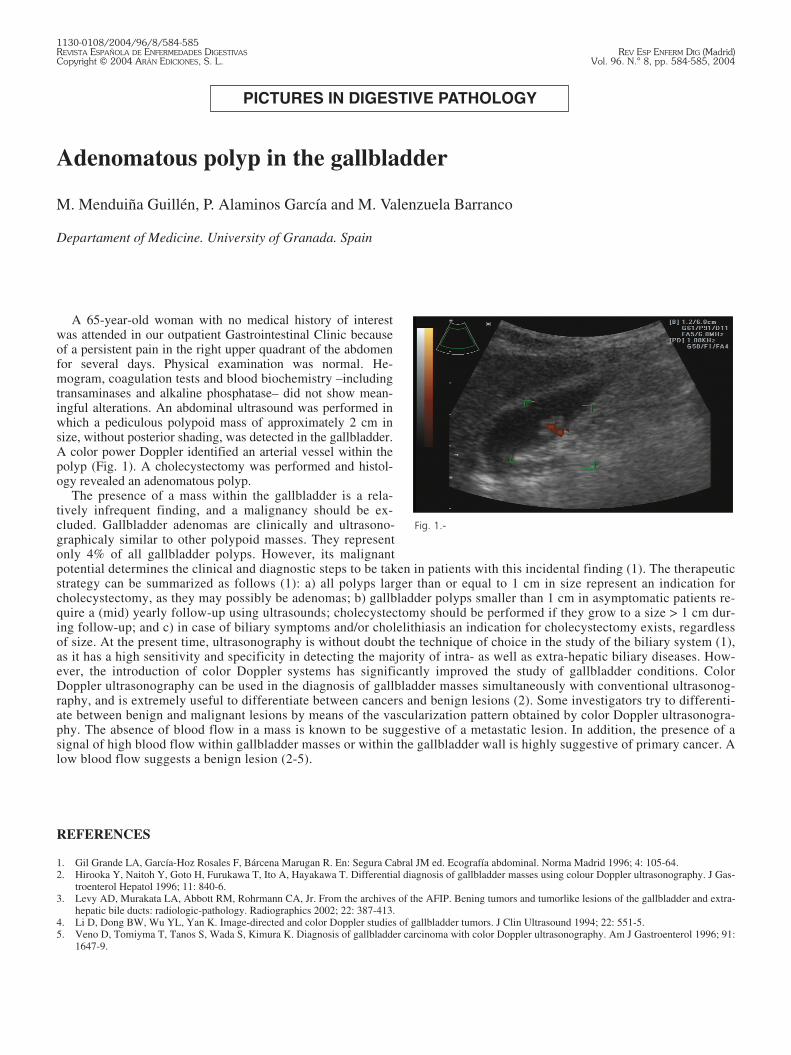
A 65-year-old woman with no medical history of interestwas attended in our outpatient Gastrointestinal Clinic becauseof a persistent pain in the right upper quadrant of the abdomenfor several days. Physical examination was normal. He-mogram, coagulation tests and blood biochemistry –includingtransaminases and alkaline phosphatase– did not show mean-ingful alterations. An abdominal ultrasound was performed inwhich a pediculous polypoid mass of approximately 2 cm insize, without posterior shading, was detected in the gallbladder.A color power Doppler identified an arterial vessel within thepolyp (Fig. 1). A cholecystectomy was performed and histol-ogy revealed an adenomatous polyp.
The presence of a mass within the gallbladder is a rela-tively infrequent finding, and a malignancy should be ex-cluded. Gallbladder adenomas are clinically and ultrasono-graphicaly similar to other polypoid masses. They representonly 4% of all gallbladder polyps. However, its malignantpotential determines the clinical and diagnostic steps to be taken in patients with this incidental finding (1). The therapeuticstrategy can be summarized as follows (1): a) all polyps larger than or equal to 1 cm in size represent an indication forcholecystectomy, as they may possibly be adenomas; b) gallbladder polyps smaller than 1 cm in asymptomatic patients re-quire a (mid) yearly follow-up using ultrasounds; cholecystectomy should be performed if they grow to a size > 1 cm dur-ing follow-up; and c) in case of biliary symptoms and/or cholelithiasis an indication for cholecystectomy exists, regardlessof size. At the present time, ultrasonography is without doubt the technique of choice in the study of the biliary system (1),as it has a high sensitivity and specificity in detecting the majority of intra- as well as extra-hepatic biliary diseases. How-ever, the introduction of color Doppler systems has significantly improved the study of gallbladder conditions. ColorDoppler ultrasonography can be used in the diagnosis of gallbladder masses simultaneously with conventional ultrasonog-raphy, and is extremely useful to differentiate between cancers and benign lesions (2). Some investigators try to differenti-ate between benign and malignant lesions by means of the vascularization pattern obtained by color Doppler ultrasonogra-phy. The absence of blood flow in a mass is known to be suggestive of a metastatic lesion. In addition, the presence of asignal of high blood flow within gallbladder masses or within the gallbladder wall is highly suggestive of primary cancer. Alow blood flow suggests a benign lesion (2-5).
REFERENCES
1. Gil Grande LA, García-Hoz Rosales F, Bárcena Marugan R. En: Segura Cabral JM ed. Ecografía abdominal. Norma Madrid 1996; 4: 105-64.2. Hirooka Y, Naitoh Y, Goto H, Furukawa T, Ito A, Hayakawa T. Differential diagnosis of gallbladder masses using colour Doppler ultrasonography. J Gas-
troenterol Hepatol 1996; 11: 840-6.3. Levy AD, Murakata LA, Abbott RM, Rohrmann CA, Jr. From the archives of the AFIP. Bening tumors and tumorlike lesions of the gallbladder and extra-
hepatic bile ducts: radiologic-pathology. Radiographics 2002; 22: 387-413.4. Li D, Dong BW, Wu YL, Yan K. Image-directed and color Doppler studies of gallbladder tumors. J Clin Ultrasound 1994; 22: 551-5.5. Veno D, Tomiyma T, Tanos S, Wada S, Kimura K. Diagnosis of gallbladder carcinoma with color Doppler ultrasonography. Am J Gastroenterol 1996; 91:
1647-9.
Fig. 1.-

Pólipo adenomatoso en vesícula biliar
M. Menduiña Guillén, P. Alaminos García y M. Valenzuela Barranco
Departamento de Medicina. Universidad de Granada
Mujer de 65 años de edad, sin antecedentes de interés, acude a consulta de enfermedades digestivas por dolor persistente enhipocondrio derecho de varios días de evolución. Exploración física anodina. El hemograma, la coagulación y la bioquímicasanguínea, incluyendo las transaminasas y la fosfatasa alcalina, no presentan alteraciones significativas. Se realiza una ecogra-fía abdominal en la que se observa en la vesícula la presencia de una formación polipoidea, pediculada, que no provoca sombraacústica posterior, y de unos 2 cm de diámetro. El estudio Power Doppler color identifica la existencia de un vaso sanguíneo ar-terial en el interior del pólipo (Fig. 1). Se practica una colecistectomía y el examen anatomopatológico informa esta lesión comoun pólipo de carácter adenomatoso.
La presencia de una masa en la vesícula biliar es relativamente infrecuente. Su importancia radica en su habilidad por imitarlesiones malignas en estas localizaciones. Los adenomas vesiculares son clínica y ecográficamente indistinguibles de otras for-maciones polipoideas; representan sólo el 4% de los pólipos vesiculares, pero su potencial maligno matiza de forma importanteel manejo clínico de los pacientes en quienes se ha producido el hallazgo casual ecográfico del pólipo vesicular (1). La conduc-ta terapéutica se podría resumir de la siguiente manera (1): a) todo pólipo mayor o igual a 1 cm es indicación de colecistectomíadebido a la posibilidad de que se trate de un adenoma; b) los pólipos vesiculares menores de 1 cm hallados en pacientes asinto-máticos requieren su seguimiento ecográfico semestral o anual y son indicación de colecistectomía cuando su tamaño alcance elcentímetro de diámetro; y c) en los casos en que existan síntomas biliares claros y/o colelitiasis asociada está indicada la cole-cistectomía con independencia del tamaño del pólipo.
En la actualidad, la ecografía es sin duda la técnica de elección en el estudio del sistema biliar (1), ya que tiene un alto índicede sensibilidad y de especificidad para detectar la mayoría de las patologías del sistema biliar tanto intra- como extrahepático.La introducción del Doppler color ha representado un gran avance en el estudio de la patología biliar. La ultrasonografía deDoppler color puede ser usada en el diagnóstico de masas en la vesícula biliar en combinación con la ultrasonografía conven-cional; es especialmente útil en la diferenciación entre cánceres y lesiones benignas (2). Algunos autores pretenden establecerun diagnóstico diferencial entre lesiones benignas y malignas basados en el patrón de vascularización que se obtiene con elDoppler color. Así, sabemos que la ausencia de flujo sanguíneo en una masa indica que se trata de una lesión metastásica. Por elcontrario, la presencia de una señal de flujo sanguíneo de alta velocidad en el interior de masas vesiculares o en el espesor de lapared es un rasgo significativo de cáncer primario. Por último, una señal de flujo de baja velocidad es sugerente de benignidad(2-5).
Vol. 96. N.° 8, 2004 PÓLIPO ADENOMATOSO EN VESÍCULA BILIAR 585
REV ESP ENFERM DIG 2004; 96(8): 584-585