advanced airway management · 1 advanced airway & respiratory assessment & management...
TRANSCRIPT

1
Advanced Airway & Respiratory
Assessment & Management
Michael D. Gooch, DNP, AC/F/ENPAssistant Professor of Nursing – Vanderbilt
Emergency NP – TeamHealth
Objectives
1. Exam a patient’s airway to develop the proper course for airway management.
2. Identify common intubation and airways options.
3. Recall the indications and considerations when using medications to facilitate an advanced airway placement.
Assessment of the Airway
• Is it patent?
• Any abnormal sounds?
• Is the patient vocalizing?
• Is there an obstruction or potential obstruction?– Tongue
– Dentures/Teeth
– Vomit, Blood
– Edema
– Foreign bodies
Assessment of Breathing
• Rate• Quality• Depth • Accessory Muscle Use• Breath Sounds• Chest Wall Integrity• Pulse Oximetry• Capnography• Mental Status
Oropharyngeal Airways
• Size – measure from the corner of the mouth to the angle of the mandible
• Insertion – depress the tongue with a tongue blade or a yankauer and insert over the tongue
• Risk of vomiting if the patient still has a gag reflex
• May occlude the airway if too large
Nasopharyngeal Airways
• Size – measure from the nose to the angle of the mandible
• Insertion – lubricate, then insert beveled edge against the nasal septum
• May stimulate a gag reflex if too large
• Contraindications
2
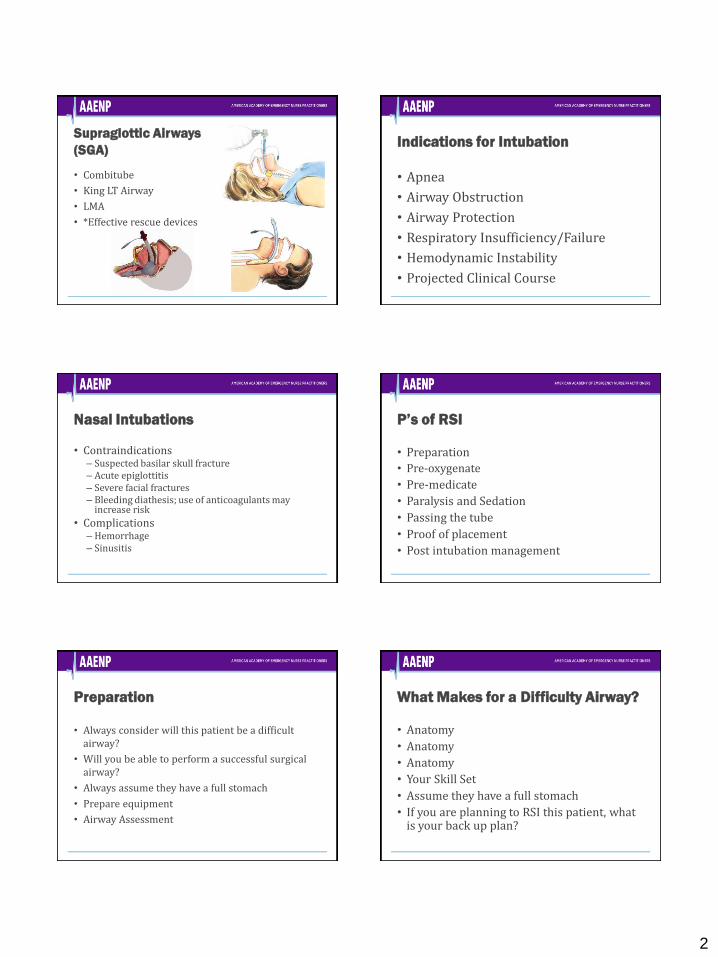
Supraglottic Airways
(SGA)
• Combitube
• King LT Airway
• LMA
• *Effective rescue devices
Indications for Intubation
• Apnea
• Airway Obstruction
• Airway Protection
• Respiratory Insufficiency/Failure
• Hemodynamic Instability
• Projected Clinical Course
Nasal Intubations
• Contraindications– Suspected basilar skull fracture– Acute epiglottitis– Severe facial fractures– Bleeding diathesis; use of anticoagulants may
increase risk
• Complications– Hemorrhage– Sinusitis
P’s of RSI
• Preparation
• Pre-oxygenate
• Pre-medicate
• Paralysis and Sedation
• Passing the tube
• Proof of placement
• Post intubation management
Preparation
• Always consider will this patient be a difficult airway?
• Will you be able to perform a successful surgical airway?
• Always assume they have a full stomach
• Prepare equipment
• Airway Assessment
What Makes for a Difficulty Airway?
• Anatomy
• Anatomy
• Anatomy
• Your Skill Set
• Assume they have a full stomach
• If you are planning to RSI this patient, what is your back up plan?
3
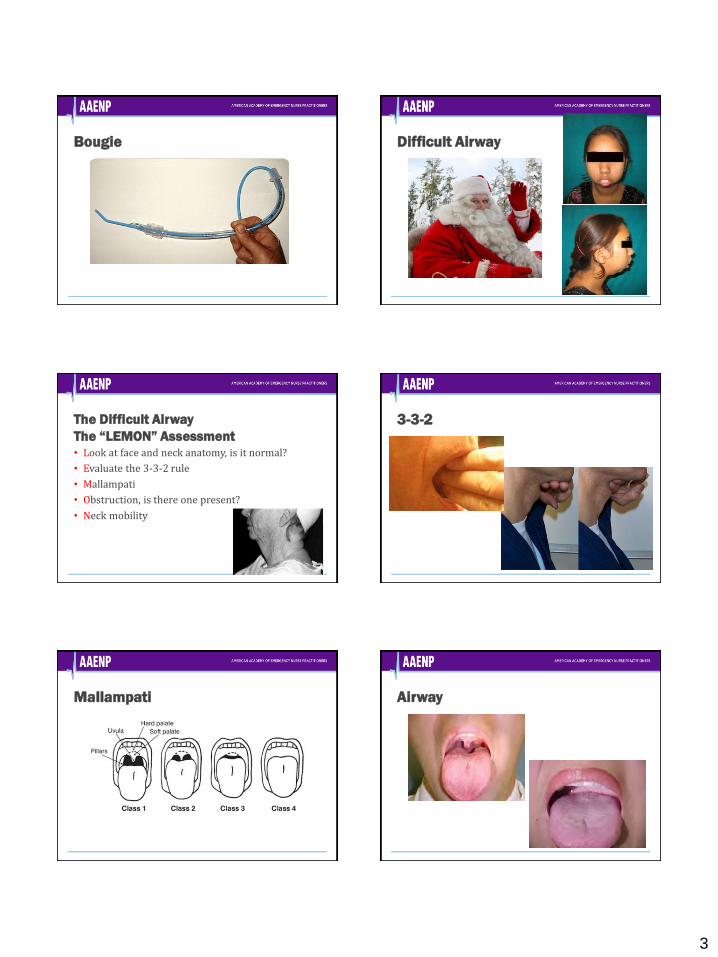
Bougie Difficult Airway
The Difficult Airway
The “LEMON” Assessment• Look at face and neck anatomy, is it normal?
• Evaluate the 3-3-2 rule
• Mallampati
• Obstruction, is there one present?
• Neck mobility
3-3-2
Mallampati Airway

4
Pre-Oxygenate
• 100% O2 NRB for 3-5 minutes will provide a Nitrogen washout of the lungs
• Avoid positive pressure ventilation if possible
• O2 15L via N/C – No DESAT Method
• Elevate the HOB
Annals of Emergency
Medicine 2012; 59(3)
Preparation
• Equipment
– Laryngoscope blade and handle
– ETT, Stylet
– BVM w/ OPA
– Suction
– ETCO2 Detector
– Securing device
– Back up device
• Position the patient
– C-Spine control if needed
– Towel roll under the shoulders of pediatric patients or obese patients
• Monitoring equipment
– ECG
– SaO2
– ETCO2
Medications
• Premedication
–Lidocaine
–Opioids
–Atropine
• Induction
–Etomidate
–Ketamine
–Midazolam
Medications
• Neuromuscular Blockade (NMB)
–Succinylcholine
• Avoid in patients with known or suspected hyperkalemia or h/o malignant hyperthermia
–Rocuronium
Laryngoscopic View and Anatomy

5
The ViewCormack-Lehane Scale –
Laryngoscopic View
Airway Manipulation
– Cric Pressure (Sellick Maneuver)
ELM (External Laryngeal Manipulation)
Video Nuances
Proof of Placement
• Visualize the tube passing through the cords
• Bilateral Lung Sounds
• No epigastric sounds
• Chest wall excursion
• ETCO2
• EDD
Capnography - ETCO2
• Pulse oximetry reflects oxygenation, End Tidal CO2 reflects ventilation.
• ETCO2 closely mirrors PaCO2 as long as there is no shunting or increase in dead space

6
Post Intubation Management
• Secure the ETT• ~3 x tube size - estimates proper depth
• Long term sedation– Lorazepam– Midazolam– Ketamine– Propofol
• Long term NMB– Vecuronium
• Gastric Decompression
Ongoing Assessment
• Patency and Proper Placement of the Airway
• Continued need for an artificial airway
• Risk of intubation and mechanical ventilation
• Assessment of breath sounds
• Evaluation of SaO2 and ETCO2
• Evaluation of blood gases and chest x-ray
Evaluation of the Chest X-RAY ETT Placement
Ultrasound Troubleshooting the Artificial Airway
• Displacement
• Obstructed
• Pneumothorax
• Equipment

7
Pediatrics
• Anatomical Differences
– Larynx is more anterior and cephalad
– The epiglottis is U shaped and protrudes more
– The narrowest portion of the airway is at the cricoid cartilage
• Sizing ET tubes
– Weight based resuscitation tape
– 16 + age in years / 4
– The patient’s little finger or nare
Ventilator Settings
• Tidal Volume (TV)– 4 – 8 ml/kg of Ideal Body Weight (IBW)
• FiO2
– Avoid hyperoxia and manage hypoxia• Positive End Expiratory Pressure (PEEP)
– Increases functional reserve capacity (FRC), by recruiting alveoli– 5- 20 cm H20
• Rate• Inspiratory - Expiratory Time (I:E Time)
– Normal is 1:2 or 1:3– Patients with reactive airway disease benefit from a longer
expiratory times
Pneumothorax Tension Pneumothorax
• Presentation
– Signs of Hypoxia
– Signs of Shock: Hypotension
–Decreased or Absent breath
sounds on the affected side
– JVD
– Tracheal deviation is a very late sign
Ultrasound Ultrasound Findings
8
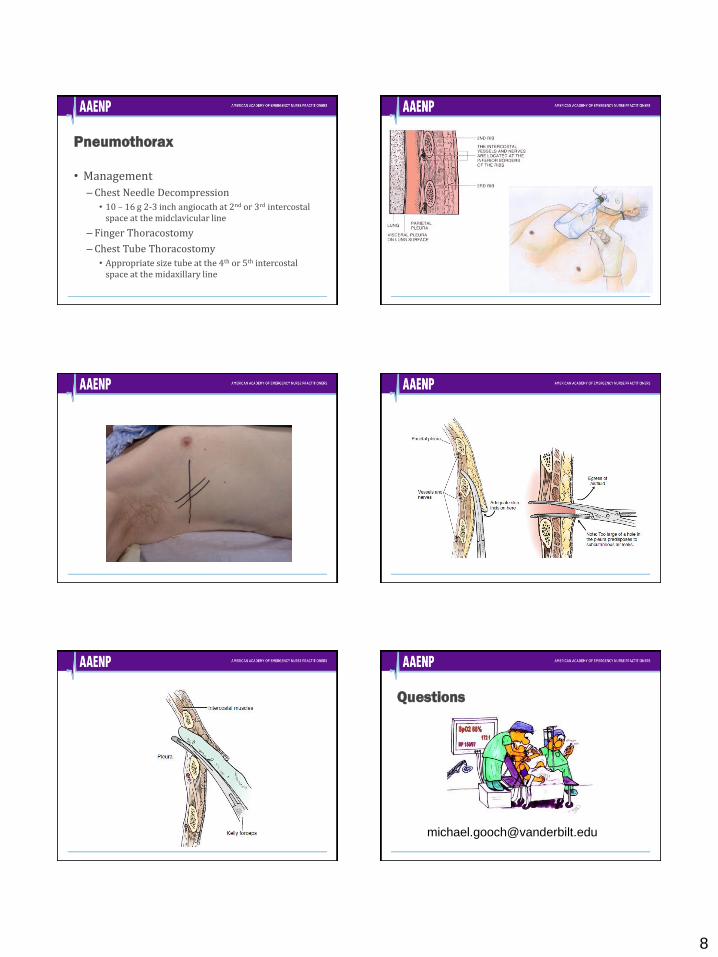
Pneumothorax
• Management
– Chest Needle Decompression
• 10 – 16 g 2-3 inch angiocath at 2nd or 3rd intercostal space at the midclavicular line
– Finger Thoracostomy
– Chest Tube Thoracostomy
• Appropriate size tube at the 4th or 5th intercostal space at the midaxillary line
Questions
9
References
• Dalley, C. B., Tola, D. H., & Kesten, K. S. (2012). Providing safe passage: Rapid sequence intubation for advanced practice nursing. Advanced Critical Care, 23(3), 270-283. doi:10.1111/aas.12032
• Gooch, M. D. & Roberts, E. (2017). Changing the emergency department’s practice of rapid sequence intubation to reduce the incidence of hypoxia. Advanced Emergency Nursing Journal, 39(4), 266-279. doi:10.1097/TME.0000000000000164
• Holleran, R. S., Wolf, A. C., & Frakes, M. A. (2017). Patient transport: Principles and practice (5th ed). St. Louis, MO: Elsevier.
• Walls, R.M. & Murphy, M.F. (2012). Manual of Emergency Airway Management (4th ed.) Philadelphia: Lippincott Williams and Wilkins.
References
• Weingart, S. D. (2011). Preoxygenation, reoxygenation, and delayed sequence intubation in the emergency department. The Journal of Emergency Medicine, 40(6), 661-67. doi:10.1016/j.jemermed.2010.02.014
• Weingart, S. D. & Levitan, R. M. (2012). Preoxygenation and prevention of desaturation during emergency airway management. Annals of Emergency Medicine, 59(3), 165-175. doi:10.1016/j.annemergmed.2011.10.002
• Weingart, S. D., Trueger, N. S., Wong, N., Scofi, J., Singh, N., & Rudolph, S. S. (2015). Delayed sequence intubation: A prospective observational study. Annals of Emergency Medicine, 65(4), 350-355. doi:10.1016/j.annemergmed.2014.09.025