advances in heart care - amazon web services · 2016-11-21 · percutaneous coronary intervention...
TRANSCRIPT

The past year has been an exciting one at the Vanderbilt Heart and Vascular Institute (VHVI). Our clinical and academic programs continue to grow, through the recruitment of leading physicians and researchers, the launch of several new research centers, and the expansion of our renowned clinical programs.
Advances in Heart Care
With more than 120 faculty members, we have one of the largest academic cardiology programs in the country. We recruited several new physician leaders in the past year. Dr. JoAnn Lindenfeld, current president of the Heart Failure Society of America (HFSA), joined Vanderbilt as the Section Head for Advanced Heart Failure and Transplantation. Dr. Thomas Force, immediate past president of the HFSA, assumed the role of Director of Cardiovascular Research. Dr. Matthew Freiberg moved from the University of Pittsburgh to start a new center at Vanderbilt in cardiovascular outcomes research. Dr. Javid Moslehi moved from the Brigham and Women’s Hospital to direct our recently expanded program in Cardio-Oncology. Dr. George Crossley joined our electrophysiology group and assumed the role of Associate Director of the Clinical Research Enterprise.
We have had substantial growth in our research programs. Federal funding for research at VHVI increased by 55% compared with the prior fiscal year. We were named one of the four national centers in the American Heart Association’s Strategically Focused Prevention Research Network, an effort led by Dr. David Harrison. Investigators at VHVI also played key roles in a large award from the Patient Centered Outcomes Research Institute to form the Mid-South Clinical Data Research Network. Over the winter, we opened the new Vanderbilt Translational and Clinical Cardiovascular Research Center (VTRACC), which includes 12 full-time faculty members. Finally, Vanderbilt’s DNA biobank (BioVU, led by Dr. Dan Roden) moved past 190,000 samples. It remains the largest biobank at a single academic institution worldwide.
Our clinical programs have never been stronger. Vanderbilt cardiologists conducted more than 130,000 clinic visits in the past year, a five-fold growth since 2008. Our ventricular assist device (VAD) and transplant programs remain among the largest in the country, with approximately 90 left ventricular assist devices (LVADs) and 40 heart transplants performed annually. In early 2014, we moved into the new cardiac catheterization and electrophysiology laboratories at VHVI. Our procedural volume in both areas continues to grow.
This issue of Advances in Heart Care highlights several new clinical programs for patients with advanced coronary disease or heart failure. Dr. Elias Haddad, an interventional cardiologist and part of the VHVI Complex Coronary Revascularization and Coronary Chronic Total Occlusion (CTO) program, discusses the clinical significance of CTO and emerging percutaneous approaches for revascularization. Drs. Jayant Bagai and Robert Piana review recent data regarding percutaneous ventricular restoration (PVR), a novel treatment for severe chronic heart failure after myocardial infarction.
VHVI also continues to expand the range of therapeutic options for patients and referring physicians. Dr. Meredith Pugh and colleagues in the Pulmonary Vascular Center review chronic thromboembolic pulmonary hypertension, an important sequela of pulmonary embolism, and describe medical and surgical treatment options. Dr. Arvindh Kanagasundrum and colleagues provide a series of case-based vignettes that highlight a range of catheter-based ablation options available for patients with ventricular arrhythmias.
Robert N. Piana, M.D.
Quinn Wells, M.D.
Thomas Wang, M.D.
V A N D E R B I L T H E A R T A N D V A S C U L A R I N S T I T U T E
WINTER 2015

Coronary chronic total occlusions (CTO) are common in contemporary practice with a prevalence of 1 in 5 cases at the time of diagnostic coronary angiography.1 A higher prevalence of 52% has been previously reported in a veteran population without prior coronary artery bypass undergoing coronary angiography.2 A CTO is defined as a 100% occlusion in a coronary artery with TIMI 0 flow (no antegrade flow beyond point of occlusion) of at least 3 months duration. Chronic coronary occlusions have generally been managed by medical therapy or surgical revascularization. Percutaneous coronary intervention (PCI) for CTO remains controversial as no randomized trial of CTO PCI versus medical therapy or coronary bypass has been performed to determine long-term survival after attempted CTO PCI. Due to the need for additional data for CTO PCI, appropriate use criteria (AUC) for percutaneous coronary intervention (PCI) downgrade the indications for PCI of CTO relative to non-CTO vessels. Critics of CTO revascularization generally perceive that symptoms are easily controlled with medications and CTO vessels have no impact on quality of life or survival. However, it is becoming increasingly evident that there are patients who continue to experience lifestyle limiting symptoms, despite optimal medical therapy for angina. In addition, observational data repeatedly suggest that a mortality benefit is provided by full revascularization.3-6 Greater recognition of the benefits of comprehensive revascularization for complex coronary artery disease (CAD) in conjunction with increasing success rates of CTO recanalization have together transformed CTO management into a vibrant new frontier in coronary artery disease therapies (Figure 1).
Consideration for CTO revascularization occurs in light of two important factors: 1) whether revascularization will provide the patient with quality of life benefit, improved survival, or both; and 2) which modality will provide the most durable result at the lowest up-front risk. The following review will attempt to provide a brief synopsis of data relevant to these factors and will highlight advances in technology that have made the emphasis on CTO PCI possible. We will review the data in the context of three broad questions: 1) Do CTOs contribute to ischemia despite
Chronic Total Occlusion of the Coronary Artery —Evolving Therapeutic OptionsElias Haddad, M.D.
collaterals filling the distal vessel? 2) Do CTOs cause symptoms? 3) Can CTOs be opened with high success and at an acceptable level of risk using percutaneous technology? Do CTOs contribute to ischemia despite collaterals filling the distal vessel?An elegant study to answer this question was performed by Sachdeva et al in which Fractional Flow Reserve (FFR) was performed of CTO vessels. FFR is a modality which measures pressure differences across a coronary stenosis to determine the likelihood that the stenosis impedes oxygen delivery to the myocardium. In this study, it was found that resting ischemia was present in 78% of CTO patients, and nearly every CTO crossed was hemodynamically significant despite collateral filling of the distal vessel.7 This is important as the field of CTO recanalization matures and becomes recognized by bodies formulating AUC criteria. The AUC criteria emphasize ischemic burden in selecting patients for whom benefit would be expected from revascularization. Data using nuclear imaging studies to quantify ischemia or at-risk myocardium suggest survival benefit from revascularization in patients with ≥10% ischemic myocardium.8 This has influenced contemporary CTO practice when selecting candidates for CTO recanalization.
Elias Haddad, M.D.
Potential Benefits of CTO Recanalization
•Improvesymptomsofanginaanddyspnea
•Decreaseneedforcoronaryarterybypasssurgery
•Decreasetheneedforanti-anginalmedications
•Improvesurvivalcomparedtothatofpatientswithincompleterevascularization
•Improveleftventricularfunction
•Decreasesubstrateforarrhythmias
•Improvetoleranceoffutureacutecoronarysyndromeevents
Critics of CTO revascularizationgenerallyperceivethatsymptomsareeasilycontrolledwithmedications and CTO vesselshavenoimpactonqualityoflifeorsurvival.However,itis becoming increasinglyevidentthattherearepatientswhocontinuetoexperiencelifestylelimitingsymptoms,despiteoptimalmedicaltherapyforangina.
@
Figure 1

Do CTOs cause symptoms? Observational studies suggest that classic anginal chest pain may be less prominent with CTOs than exertional shortness of breath. Physicians may underestimate symptoms in CTO patients and may underestimate the effect of those symptoms on quality of life (QOL). Several studies have reported significant improvement in QOL metrics following successful CTO recanalization.9-11 A recent multi-center prospective cohort study evaluated QOL at 1 year after one of four treatment options: medical therapy only, PCI to non-CTO, PCI to CTO, and coronary artery bypass graft (CABG). The medical therapy group had no improvement in QOL. The CTO revascularization groups (either PCI or CABG) had significant improvement in QOL metrics including angina frequency and disease perception scores.12 Can CTOs be opened with high success and at an acceptable level of risk using percutaneous technology? The answer to the question whether CTOs can be opened reliably by percutaneous techniques has evolved rapidly since January 2011. At that time, several high-volume North American CTO operators convened in Bellingham, Washington, to develop a consensus approach to CTO crossing. The “Hybrid CTO PCI algorithm” developed out of that meeting, and has placed a focus on teaching effective and efficient opening of CTO vessels. The hybrid algorithm emphasizes that anatomy dictates strategy in order to achieve CTO crossing with the least radiation and contrast exposure to the patient, and the least lab equipment utilization possible. In addition, the algorithm has emphasized comfort working in the sub-intimal space which was once considered a reason to abort a procedure. A CTO-specific system developed by BridgePoint Medical has embraced the sub-intimal space as a means to quickly and safely cross CTOs. This system includes a blunt tip catheter (CrossBoss™) and a specialized re-entry balloon (StingRay™) to perform antegrade dissection and re-entry of the CTO (Figure 2). In conjunction with an
emphasis on efficiency, the hybrid algorithm for CTO recanalization has resulted in success rates for recanalization of approximately 90% compared to previous success rates of 70 to 75%.13, 14 CTO operators are also performing the procedures safely. In a European registry of highly-experienced operators, the risk of major adverse events including death, stroke, and need for urgent CABG was less than 1%. The risk of a peri-procedural MI was 3.1%.15
SummaryIn counseling patients, consideration should be given to the potential for improved quality of life by decreasing angina class, decreasing the need for CABG, and decreasing the need for anti-anginal medications. There are also data to support improved left ventricular function with CTO recanalization, provided the territory is viable.16-19 As mentioned, recent data suggest a mortality benefit with complete revascularization, including percutaneous management of CTO.3 Also, CTO recanalization may decrease the substrate for arrhythmic events and protect against future ACS events. Prospective and randomized data will be available to better define the value of CTO PCI in the next few years. EURO-CTO (European Study on the Utilization of Revascularization vs Optimal Medical Therapy for the Treatment of Chronic Total Coronary Occlusions) is a multicenter trial to evaluate 1- and 3-year outcomes in patients randomized to revascularization or medical therapy. In addition, OPEN CTO (Outcomes, Patient health status, and Efficiency iN Chronic Total Occlusion hybrid procedures) is a North American registry at 10 sites enrolling 1,000 patients to evaluate the safety and impact on patient health status of CTO PCI.(Continued on page 4)
Figure 2 CrossBoss™ and StingRay™ system for crossing CTO using antegrade dissection re-entry technique. Boston Scientific. Used with Permission.
Incounselingpatients,consideration should begiventothepotentialforimprovedqualityoflifebydecreasing angina class, decreasing the need for CABG, and decreasing the needforanti-anginalmedications. There are also data to supportimprovedleftventricularfunctionwithCTOrecanalization, providedtheterritoryisviable.
#

The VHVI Complex Coronary Revascularization and CTO program has been built to maximize success and value for patients and referring physicians. Our success rates for CTO recanalization are on par with national centers of excellence in complex CTO work (Figures 3A-D). A collaborative environment and a true “heart team approach” have been fostered to bring the best of PCI and coronary bypass for the benefit of patient outcomes.
References:1. Fefer P, Knudtson ML, Cheema AN, et al. Current perspectives on coronary chronic total occlusions: the Canadian Multicenter Chronic Total Occlusions Registry. J Am Coll Cardiol. 2012;59:991-7.
2. Christofferson RD, Lehmann KG, Martin GV, et al. Effect of chronic total coronary occlusion on treatment strategy. Am J Cardiol. 2005;95:1088-91.
3. George S, Cockburn J, Clayton TC, et al. Long-term follow-up of elective chronic total coronary occlusion angioplasty: analysis from the U.K. Central Cardiac Audit Database. J Am Coll Cardiol. 2014;64: 235-43.
4. Muramatsu T, Hirano K, Tsukahara R, et al. Long-term outcome of percutaneous transluminal coronary intervention for chronic total occlusion in the BMS era in Japan. Cardiovasc Interv Ther. 2010;25:78-84.
5. Khan MF, Wendel CS, Thai HM, et al. Effects of percutaneous revascularization of chronic total occlusions on clinical outcomes: a meta-analysis comparing successful versus failed percutaneous intervention for chronic total occlusion. Catheter Cardiovasc Interv. 2013;82:95-107.
6. Joyal D, Afilalo J, Rinfret S. Effectiveness of recanalization of chronic total occlusions: a systematic review and meta-analysis. Am Heart J. 2010;160:179-87.
7. Sachdeva R, Agrawal M, Flynn SE, et al. The myocardium supplied by a chronic total occlusion is a persistently ischemic zone. Catheter Cardiovasc Interv. 2014;83:9-16.
8. Hachamovitch R, Hayes SW, Friedman JD, et al. Comparison of the short-term survival benefit associated with revascularization compared with medical therapy in patients with no prior coronary artery disease undergoing stress myocardial perfusion single photon emission computed tomography. Circulation. 2003;107:2900-7.
9. Grantham JA, Jones PG, Cannon L, et al. Quantifying the early health status benefits of successful chronic total occlusion recanalization: Results from the FlowCardia’s approach to chronic total occlusion recanalization (FACTOR) Trial. Circ Cardiovasc Qual Outcomes. 2010;3:284-90.
10. Safley DM, Grantham JA, Hatch J, et al. Quality of life benefits of percutaneous coronary intervention for chronic occlusions. Catheter Cardiovasc Interv. 2014;84:629-34.
11. Borgia F, Viceconte N, Ali O, et al. Improved cardiac survival, freedom from MACE and angina-related quality of life after successful percutaneous recanalization of coronary artery chronic total occlusions. Int J Cardiol. 2012;161:31-8.
12. Wijeysundera HC, Norris C, Fefer P, et al. Relationship between initial treatment strategy and quality of life in patients with coronary chronic total occlusions. EuroIntervention. 2014;9:1165-72.
13. Olivari Z, Rubartelli P, Piscione F, et al. Immediate results and one-year clinical outcome after percutaneous coronary interventions in chronic total occlusions: data from a multicenter, prospective, observational study (TOAST-GISE). J Am Coll Cardiol. 2003;41:1672-8.
14. Christopoulos G, Menon RV, Karmpaliotis D, et al. The efficacy and safety of the “hybrid” approach to coronary chronic total occlusions: Insights from a contemporary multicenter US registry and comparison with prior studies. J Invasive Cardiol. 2014;26:427-32.
15. Galassi AR, Tomasello SD, Reifart N, et al. In-hospital outcomes of percutaneous coronary intervention in patients with chronic total occlusion: insights from the ERCTO (European Registry of Chronic Total Occlusion) registry. EuroIntervention. 2011;7:472-9.
16. Kirschbaum SW, Baks T, van den Ent M, et al. Evaluation of left ventricular function three years after percutaneous recanalization of chronic total coronary occlusions. Am J Cardiol. 2008;101:179-85.
17. Werner GS, Surber R, Kuethe F, et al. Collaterals and the recovery of left ventricular function after recanalization of a chronic total coronary occlusion. Am Heart J. 2005;149:129-37.
18. Piscione F, Galasso G, De Luca G, et al. Late reopening of an occluded infarct related artery improves left ventricular function and long term clinical outcome. Heart. 2005;91:646-51.
19. Cheng AS, Selvanayagam JB, Jerosch-Herold M, et al. Percutaneous treatment of chronic total coronary occlusions improves regional hyperemic myocardial blood flow and contractility: insights from quantitative cardiovascular magnetic resonance imaging. JACC Cardiovasc Interv. 2008;1:44-53.
Chronic Total Occlusion of the Coronary Artery — Evolving Therapeutic Options(Continued from page 3)
Figure 3A Occluded right coronary artery (RCA) in a patient with lifestyle limiting angina on three anti-anginal medications at maximal doses.
Figure 3B Dual injection of the right and left coronary arteries in the same patient. Note the collateral filling of the RCA from septal collaterals from the left anterior descending artery (LAD) (red arrow). Black arrow indicates the proximal occlusion of the RCA.
Figure 3C Retrograde approach to the occluded RCA with a wire and micro-catheter traversing LAD collaterals and entering the RCA to cross the distal cap of the occlusion (arrow).
Figure 3D Final angiogram after successful crossing of CTO and stenting.
$

Percutaneous Ventricular Restoration for Heart Failure After Anterior Myocardial InfarctionJayant Bagai, M.D., Robert N. Piana, M.D.
Despite aggressive emergent revascularization strategies, large myocardial infarction (MI) involving the left anterior descending coronary artery can result in akinesis or aneurysmal dilatation of the anterior wall and left ventricular apex. This in turn can cause progressive, deleterious remodeling of the left ventricle in up to 33% of post MI patients and increased wall stress on the non-infarcted regions of the heart.1 The management of such patients who consequently develop severe chronic heart failure (HF) can be challenging. Patients in NYHA class III and ambulatory class IV (heart failure symptoms with minimal exertion or at rest) have a poor quality of life, low intermediate and long-term survival (32% 1-year mortality), and frequent admissions to the hospital with decompensated heart failure.2 Therapeutic options for such patients include:a. Intensive therapy with vasodilators, beta-
blockers, aldosterone antagonists, and loop diuretics
b. Cardiac resynchronization therapy (CRT) with biventricular pacemakers/ Implantable Cardioverter Defibrillators (ICDs)
c. Ventricular assist devices (VAD), either as a permanent treatment modality in patients who are not candidates for heart transplant, or as a “bridge” to eventual heart transplant
d. Cardiac transplant
VAD and transplant are typically reserved for patients with ACC/AHA stage D heart failure (refractory to conventional medical therapy), whereas CRT is useful only in patients with a wide QRS duration on EKG. Drug therapy is also limited in some patients due to low blood pressure and poor kidney function.
Finally, some patients continue to have NYHA class III-IV symptoms despite maximally tolerated drug therapy and/or CRT, and are not candidates for VAD or transplant.
A novel mode of treatment for such patients is to percutaneously implant a device in the left ventricular cavity with the intention of reshaping and improving the compliance of the left ventricle (LV). Since the device partitions the LV and excludes the akinetic or aneurysmal segment, it is referred to as a ventricular partitioning device (VPD). The term “percutaneous ventricular restoration” or PVR has been proposed to differentiate the technique from surgical approaches to ventricular volume reduction.
Parachute DeviceThe Parachute device (Cardiokinetix, Menlo Park, CA) is a catheter-based VPD. The device in its current form consists of a conical nitinol frame covered with ePTFE. A soft radio-opaque “foot” is attached to the apex of this cone, and 2 mm projections at the base of the cone assist in anchoring the device to the LV endocardium (Figure 1). The entire device is constrained in a loader and delivered to the LV cavity via a dedicated and specially shaped guide catheter. The guide is advanced over a wire via 16F sheath in the femoral artery. The device is de-sheathed from the guide in the LV cavity and advanced to the apex until the “foot” abuts the LV apex. Left ventriculography and simultaneous transthoracic echocardiography guide this process. A 20 ml balloon is inflated within the cone of the device to assist in opening the device to its full extent, and then deflated. The device is then released from the delivery cable after ensuring satisfactory position by repeat (Continued on page 6)
Robert N. Piana, M.D.
JayantBagai,M.D.
%
Figure 1The Parachute device with nitinol frame and anchors, ePTFE covering, and foot composed of polymer material. Courtesy of CardioKinetix
Figure 2 – Angiographic sequence of a Parachute implantation in the left ventricle (LV). Pigtail in the LV cavity to perform LV angiography (A); device placement with foot exposed and in contact with the antero-apical wall (B); balloon inflation to facilitate self-expansion of the device (C); device fully expanded but still attached to the delivery system (D); final positioning after release of the device (E).With permission from Wolter Kluwer 8

angiography and echocardiography (Figure 2). The procedure is typically performed under conscious sedation and local anesthesia with a completely percutaneous approach. Patients are discharged on warfarin for 1 year, followed by aspirin indefinitely. Histopathological studies on devices removed during transplant or autopsy have shown platelet and fibrin-thrombus on both luminal and abluminal aspects of the device.3 Over time, granulation tissue and neo-endocardium form and incorporate the device surfaces and contact points with the LV wall (Figure 3).
Mechanism of Action The goal of PVR is to lower LV end-diastolic and systolic volumes, which are surrogates for severity of adverse LV remodeling. There are several potential mechanisms of action:
1. Substitution of the rigid apical scar with the more compliant device, coupled with the outward force exerted by the device’s anchors in diastole, improves LV filling by exerting a “trampoline effect.”
2. Improved LV compliance also reduces LV end diastolic pressure.
3. Favorable changes in LV geometry lower wall stress in the unaffected portion of the LV.
Clinical StudiesInitial animal studies found that implantation of the device 6 weeks following experimental MI was associated with attenuation of LV remodeling. The device was then successfully implanted in 2 patients in Belgrade, Serbia, with reductions in LV volumes and improvement in LV ejection fraction (LVEF).4 Since then the device has been evaluated in single-arm clinical trials with prospective follow-up, and more recently in randomized controlled trials. The European, first-in-human cohort A
consisted of 18 patients while cohort B had 59 patients. The US Feasibility trial enrolled 20 patients, and 18 had the device implanted.
In one recent series involving 91 patients, successful implantation was achieved in 90%.5 Five implantations were unsuccessful including one case of device infection, which required removal. One procedural death occurred and 1 patient suffered a stroke. Overall, 89% of patients improved or maintained their functional class.
The PARACHUTE trial (N=15) reported a significant reduction in LV end diastolic and systolic volumes at one year, coupled with an improvement in LVEF from 28% to 33%. Functional capacity and 6-minute walk test improved, with a significant reduction in NYHA class.6 The device had to be surgically removed in 2 patients and 1 patient died from non-device related infection.
Additional 1-year data from 111 patients from the European cohort A and B, U.S. feasibility, and Parachute III trials have been reported.7 Baseline LVEF was 27.9%. The device was successfully implanted in 96% of cases. Average length of hospital stay was 2.9 days. At 12 months, a highly significant 14% decline in LV volume was noted despite a modest 2% absolute increase in LVEF. Improvement or maintenance of NYHA class was noted in 54% and 32% of patients, respectively. Major complications were noted in 7.2% and minor complications in 8.2%. One-year stroke, all-cause mortality, and combined mortality and heart failure re-hospitalization rates were 2.9%, 5.7%, and 21.7%, respectively.
Three-year data in 23 patients, with post MI LVEF of 15-40% and NYHA class II-IV symptoms, were recently published.8 These patients underwent device implantation as part of the
^
Percutaneous Ventricular Restoration for Heart Failure After Anterior Myocardial Infarction(Continued from page 5)
Figure 3 (A) Gross photograph of LV apex showing Parachute device in contact with the LV endocardial surface; white area represents healing tissue, and brown area represents a layer of thrombus. (B) Whole section mount of LV showing Parachute device and its foot in contact with the apex and covered by neo-endocardium. With permission from John Wiley and Sons3
Figure 4Change in NYHA functional class from baseline (B) through 6, 12, 24, and 36 months.With permission from Wolter Kluwer 8
100%
80%
60%
40%
20%
0%B 6 M 12 M 24 M
Death
Transplant/VAD
IV
III
II
I36 M
A B

Parachute first-in-human study, which was a prospective, single-arm study conducted at 10 centers in the U.S. and Europe. In this study, NYHA class was improved or maintained in 85% of patients (Figure 4). Further, a statistically significant reduction occurred in LV end diastolic volume index by 10% and LV end-systolic volume index by 7% (Figure 5). This was paralleled by significant improvements in quality of life and functional capacity, as assessed by the Minnesota Living with Heart Failure questionnaire and 6-minute walk test. The incidence of heart failure hospitalization or death at 1 year was 16.1%, 32.3% at 2 years, and 38.7% at 3 years. Only 2 out of 31 patients died of cardiac causes over 3-year follow up and no cardiac death occurred after 6 months. No strokes were noted at 1-year follow up. Four strokes were noted by 3 years.
Percutaneous Versus Surgical Ventricular RestorationSurgical ventricular restoration (SVR) as studied in the STICH and RESTORE trials has provided mixed results and differs significantly from PVR.9, 10 In some studies, the degree of LV end systolic volume reduction appears to be greater with PVR compared with SVR. The Parachute device partitions the LV with a flexible device and results in a conical apex, whereas SVR results in a rigid flat apex due to an inflexible surgical patch. Also, the risk of PVR is considerably lower than SVR.
Pivotal TrialPARACHUTE IV is the pivotal FDA investigational device exemption trial, which is enrolling 560 post-left anterior descending artery territory MI heart failure patients in the U.S. who have NYHA class III or ambulatory class IV symptoms. Other inclusion criteria include LVEF between 15-35% by echocardiogram, appropriate left ventricular wall motion abnormality (akinesis, dyskinesis, or aneurysm), and anatomy
&
as assessed by cardiac CT and echocardiogram to allow device placement. Individuals with untreated significant coronary artery disease requiring revascularization, cardiogenic shock within 72 hours, stroke or transient ischemic attack within 6 months, pacemaker or ICD within 2 months, creatinine > 2.5 mg/dl, or moderate or severe valvular stenosis or regurgitation will be excluded. The primary endpoint of Parachute IV is all-cause mortality and hospitalization for worsening heart failure. Vanderbilt University Medical Center is one of the U.S. sites participating in Parachute IV. The first implant was performed successfully and without complications in August 2014, with a favorable clinical course post procedure.
ConclusionsPercutaneous ventricular restoration is a novel and potentially effective technique to counteract harmful LV remodeling after an extensive MI. Short and intermediate term data suggest that the procedure reduces LV volume, maintains or improves NYHA functional class in 85% of patients, and lowers heart failure hospitalization, with an acceptable safety profile in experienced centers. Long-term data and data from randomized controlled trials comparing the device to optimal medical therapy are awaited.
References:1. de Kam PJ, Nicolosi GL, Voors AA, et al. Prediction of 6 months left ventricular dilatation after myocardial infarction in relation to cardiac morbidity and mortality. Eur. Heart J. 2002;23:536–542.2. Chen J, Normand SL, Wang Y. National and regional trends in heart failure hospitalization and mortality rates for Medicare beneficiaries, 1998-2008. JAMA. 2011;306:1669-1678.3. Ladich E, Otsuka F, Virmani R. A pathologic study of explanted parachute devices from seven heart failure patients following percutaneous ventricular restoration. Catheter Cardiovasc Interv. 2014;83:619-30.4. Sharkey H, Nikolic S, Khairkhahan A, et al. Left ventricular apex occluder; Description of a ventricular partitioning device. EuroInterv. 2006;2:125-127.5. Thomas M. Presentation at EuroPCR 2013.6. Sagic D, Otasevic P, Sievert H, et al. Percutaneous implantation of the left ventricular partitioning device for chronic heart failure: a pilot study with 1-year follow-up. Eur J Heart Fail. 2010;12:600-606.7. Adamson P. Presentation at ACC 2014.8. Costa M, Mazzaferri E, Sievert H, et al. Percutaneous ventricular restoration using the Parachute device in patients with ischemic heart failure: three-year outcomes of the PARACHUTE first-in-human study. Circ Heart Fail. 2014;7:752-7589. Athanasuleas CL, Buckberg GD, Stanley AWH, et al. Surgical ventricular restoration: The RESTORE group experience. Heart Fail Rev. 2004;9:287–297.10. Jones RH, Velazquez EJ, Michler RE, et al. Coronary bypass surgery with or without surgical ventricular reconstruction. N Engl J Med. 2009;360:1705–1717.
Figure 5LV volume reduction by ECHO. Baseline ECHO compared with ECHO 2 years after device implantation.With permission from Wolter Kluwer 8

Chronic thromboembolic pulmonary hypertension (CTEPH) is increasingly recognized as a possible sequela of acute pulmonary emboli (PE). Histological findings in the pulmonary arteries of patients with CTEPH are different from those with acute PE: while acute clot may be present, classically, the vessels are filled with a white, fibrous material (Figure 1). Without treatment, CTEPH can lead to progressive pulmonary vascular obstruction, right heart failure, and death. CTEPH is a cause of pre-capillary pulmonary hypertension (PH), Group 4 in the most recent classification of PH,1 and distinguishing CTEPH from other causes of PH is important as it is potentially curable with surgical treatment. In CTEPH patients in whom surgery is not an option, medical therapies and interventional procedures may offer some benefit.
CTEPH develops in 0.6 – 3.8% of patients following acute PE.2 While most patients with CTEPH have a prior history of acute PE, 25% of patients with CTEPH have no history of thromboembolic disease.3 Risk factors for CTEPH include hypercoagulable states,4 indwelling catheters and leads, ventriculoatrial shunts, splenectomy, history of malignancy, inflammatory bowel disease, and thyroid replacement therapy.5, 6
Patients with CTEPH present with signs and symptoms of PH, and as disease progresses, of right heart failure: progressive dyspnea, exercise intolerance, lower extremity edema,
Chronic Thromboembolic Pulmonary Hypertension — Medical and Surgical Treatment OptionsMeredith Pugh, M.D., Anna Hemnes, M.D., Michael Petracek, M.D., Ivan Robbins, M.D.
fatigue, palpitations, lightheadedness, and exertional syncope. Findings on physical examination frequently include an accentuated P2, right ventricular heave, murmur of tricuspid regurgitation, and occasionally a bruit over the lungs indicative of focal pulmonary artery stenosis. Initial evaluation of the patient with CTEPH is similar to evaluation of other causes of PH and includes a chest X-ray, pulmonary function tests, EKG (may be unremarkable but often shows right ventricular hypertrophy, right atrial enlargement, and/or right axis deviation), and echocardiogram. Because prior history of thromboembolic disease is not universal, a ventilation/perfusion lung scan should be performed to assess for CTEPH in any patient with significant PH.
The pivotal goals of invasive testing to confirm CTEPH are to: 1) establish the extent and location of vascular obstruction, 2) determine the severity of hemodynamic impairment and, 3) determine surgical suitability based on anatomic and physiologic features. CTEPH is defined as a mean pulmonary artery pressure ≥ 25mmHg and pulmonary artery wedge pressure < 15mmHg in the presence of chronic PE.1, 7 Ventilation/perfusion (VQ) scanning remains the test of the choice for screening and initial assessment of CTEPH due to high sensitivity (> 95%).7 VQ scans in CTEPH show multiple segmental or lobar perfusion defects (Figure 2). CT angiogram is an excellent test to diagnose acute PE and can frequently be a
Meredith Pugh, M.D.
Anna Hemnes, M.D.
Michael Petracek, M.D.
Figure 1Chronic PE material removed from the right lung during pulmonary thromboendarterectomy.
IvanRobbins,M.D.
*
Figure 2Ventilation perfusion (VQ) scan in a patient with CTEPH. Panels A and C show normal ventilation pattern, while panels B and D show multiple perfusion defects.
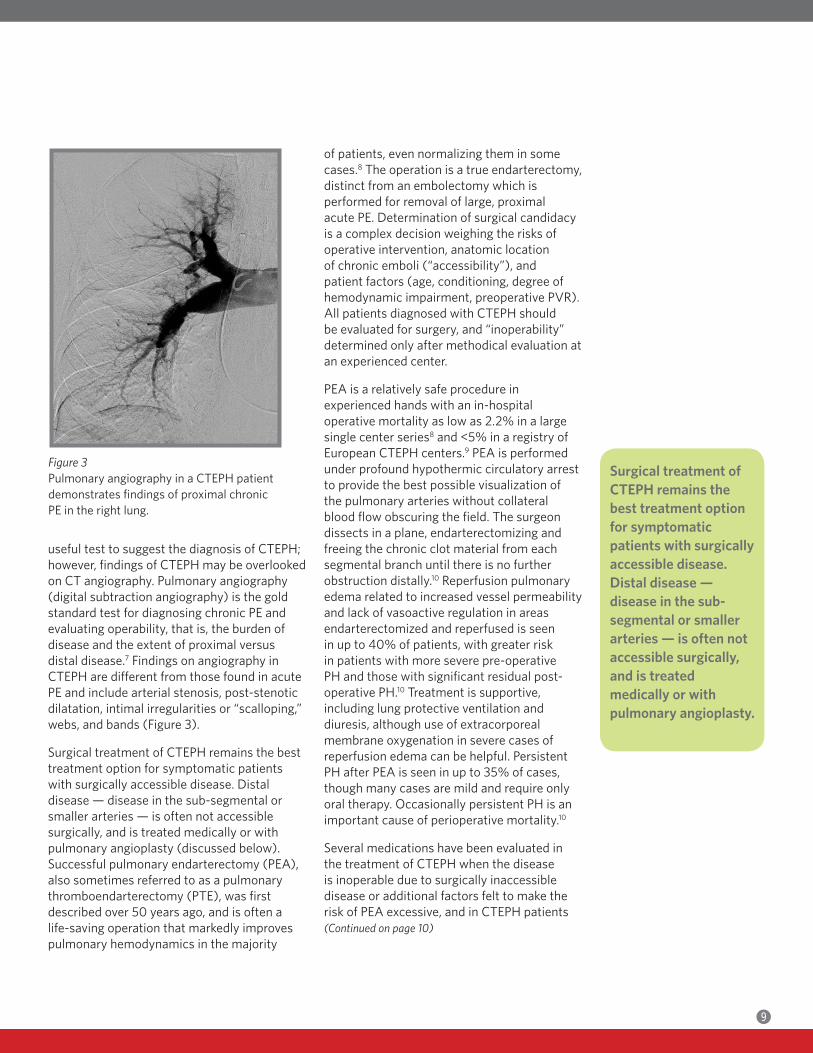
useful test to suggest the diagnosis of CTEPH; however, findings of CTEPH may be overlooked on CT angiography. Pulmonary angiography (digital subtraction angiography) is the gold standard test for diagnosing chronic PE and evaluating operability, that is, the burden of disease and the extent of proximal versus distal disease.7 Findings on angiography in CTEPH are different from those found in acute PE and include arterial stenosis, post-stenotic dilatation, intimal irregularities or “scalloping,” webs, and bands (Figure 3).
Surgical treatment of CTEPH remains the best treatment option for symptomatic patients with surgically accessible disease. Distal disease — disease in the sub-segmental or smaller arteries — is often not accessible surgically, and is treated medically or with pulmonary angioplasty (discussed below). Successful pulmonary endarterectomy (PEA), also sometimes referred to as a pulmonary thromboendarterectomy (PTE), was first described over 50 years ago, and is often a life-saving operation that markedly improves pulmonary hemodynamics in the majority
of patients, even normalizing them in some cases.8 The operation is a true endarterectomy, distinct from an embolectomy which is performed for removal of large, proximal acute PE. Determination of surgical candidacy is a complex decision weighing the risks of operative intervention, anatomic location of chronic emboli (“accessibility”), and patient factors (age, conditioning, degree of hemodynamic impairment, preoperative PVR). All patients diagnosed with CTEPH should be evaluated for surgery, and “inoperability” determined only after methodical evaluation at an experienced center. PEA is a relatively safe procedure in experienced hands with an in-hospital operative mortality as low as 2.2% in a large single center series8 and <5% in a registry of European CTEPH centers.9 PEA is performed under profound hypothermic circulatory arrest to provide the best possible visualization of the pulmonary arteries without collateral blood flow obscuring the field. The surgeon dissects in a plane, endarterectomizing and freeing the chronic clot material from each segmental branch until there is no further obstruction distally.10 Reperfusion pulmonary edema related to increased vessel permeability and lack of vasoactive regulation in areas endarterectomized and reperfused is seen in up to 40% of patients, with greater risk in patients with more severe pre-operative PH and those with significant residual post-operative PH.10 Treatment is supportive, including lung protective ventilation and diuresis, although use of extracorporeal membrane oxygenation in severe cases of reperfusion edema can be helpful. Persistent PH after PEA is seen in up to 35% of cases, though many cases are mild and require only oral therapy. Occasionally persistent PH is an important cause of perioperative mortality.10
Several medications have been evaluated in the treatment of CTEPH when the disease is inoperable due to surgically inaccessible disease or additional factors felt to make the risk of PEA excessive, and in CTEPH patients(Continued on page 10)
(
Figure 3Pulmonary angiography in a CTEPH patient demonstrates findings of proximal chronic PE in the right lung.
Surgical treatment of CTEPH remains the besttreatmentoptionforsymptomaticpatientswithsurgicallyaccessible disease. Distal disease — diseaseinthesub-segmental or smaller arteries — is often not accessiblesurgically,and is treated medicallyorwithpulmonaryangioplasty.

BL
with persistent PH following PEA. The endothelin receptor antagonist bosentan showed improvement in PVR but failed to demonstrate improvement in 6 minute walk distance.12 Recently, the guanylate cyclase stimulator riociguat demonstrated significant improvement in exercise capacity,13 and this agent is FDA-approved for the treatment of inoperable CTEPH or persistent PH following PEA. Balloon pulmonary angioplasty has also been evaluated in the treatment of inoperable CTEPH, mainly with distal disease. Several case series have been published with sustained hemodynamic improvement reported for up to 2 years.14, 15
Evaluation and treatment of CTEPH at Vanderbilt is a collaborative effort between the divisions of Cardiovascular Medicine, Pulmonary and Critical Care, Interventional Radiology, Cardiac Anesthesiology, and Cardiac Surgery. Pulmonologists in the Pulmonary Vascular Center coordinate the preoperative CTEPH evaluation and provide longitudinal follow-up and medical management of CTEPH patients. Invasive hemodynamic assessment and pulmonary angiography are performed by interventional cardiologists and radiologists with extensive expertise with these procedures. Over the last 5 years, more than 40 PEAs have been performed at Vanderbilt with an in-hospital mortality of 2.5%, and significant functional and hemodynamic improvement in the majority of patients.
References:1. Simonneau G, Gatzoulis MA, Adatia I, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2013;62:D34-41.2. Fedullo P, Kerr KM, Kim NH, et al. Chronic thromboembolic pulmonary hypertension. Am J Respir Crit Care Med. 2011;183:1605-13.3. Pepke-Zaba J, Delcroix M, Lang I, et al. Chronic thromboembolic pulmonary hypertension (CTEPH): results from an international prospective registry. Circulation. 2011;124:1973-81. 4. Wolf M, Boyer-Neumann C, Parent F, et al. Thrombotic risk factors in pulmonary hypertension. Eur Respir J. 2000;15:395-99.5. Bonderman D, Wilkens H, Wakounig S, et al. Risk factors for chronic thromboembolic pulmonary hypertension. Eur Respir J. 2009;33:325-31.6. Bonderman D, Jakowitsch J, Adlbrecht, et al. Medical conditions increasing the risk of chronic thromboembolic pulmonary hypertension. Thromb Haemost. 2005;93:512-16.7. Kim NH, Delcroix M, Jenkins DP, et al. E. Chronic thromboembolic pulmonary hypertension. J Am Coll Cardiol. 2013;62:D92-99.8. Madani MM, Auger WR, Pretorius V, et al. Pulmonary endarterectomy: recent changes in a single institution’s experience of more than 2,700 patients. Ann Thorac Surg. 2012;94:97-103.9. Mayer E, Jenkins D, Lindner J, et al. Surgical management and outcome of patients with chronic thromboembolic pulmonary hypertension: results from an international prospective registry. J Thorac Cardiovasc Surg. 2011;141:702-10.10. Poch D and Pretorius V. Pulmonary endarterectomy: assessment of operability, surgical description and post-op care. Adv Pulm Hypertension. 2014;12:86-192.11. Jenkins DP, Madani M, Mayer E, et al. Surgical treatment of chronic thromboembolic pulmonary hypertension. Eur Respir J. 2013;41: 735-42.12. Jais, X, D’Armini AM, Jansa P, et al, for the BENEFiT Study Group. Bosentan for treatment of inoperable chronic thromboembolic pulmonary hypertension. J Am Coll Cardiol. 2008;52:2127-34.13. Ghofrani HA, D’Armini AM, Grimminger F, et al, for the CHEST-1 Study Group. N Engl J Med. 2013;369:319-329.14. Mizoguchi H, Ogawa A, Munemasa M, et al. Refined balloon pulmonary angioplasty for inoperable patients with chronic thromboembolic pulmonary hypertension. Circ Cardiovasc Interv. 2012;6:748-55.15. Kataoka M, Inami T, Hayashida K, et al. Percutaneous transluminal pulmonary angioplasty for the treatment of chronic thromboembolic pulmonary hypertension. Circ Cardiovasc Interv. 2012;5:756-62.
Chronic Thromboembolic Pulmonary Hypertension — Medical and Surgical Treatment Options(Continued from page 9)
Evaluationandtreatment of CTEPH at Vanderbilt is a collaborativeeffortbetweenthedivisionsofCardiovascularMedicine,Pulmonaryand Critical Care, InterventionalRadiology,CardiacAnesthesiology,andCardiacSurgery.

Catheter Ablation of Ventricular Arrhythmias: Clinical VignettesArvindh N. Kanagasundram, M.D., Sharon Shen, M.D., Juan C. Estrada, M.D., Pablo Saavedra, M.D., Christopher R. Ellis, M.D.
Ventricular arrhythmias (VA) can develop in patients with structural heart disease (SHD) including prior myocardial infarction and non-ischemic cardiomyopathy. When VAs manifest in structurally normal hearts, they are usually a result of intra-cellular calcium overload (triggered activity) or an abnormal response to adrenergic stimulation (automaticity).1 Re-entry within the Purkinje fibers and specialized conduction system causes ~ 5% of all VAs in patients undergoing catheter ablation.2 This may occur in patients with severe dilated cardiomyopathy due to idiopathic or valvular heart disease etiologies, or in ischemic heart disease in which damaged His-Purkinje fibers can facilitate macro-reentrant bundle-branch reentry VT. In patients without structural heart disease, intra-fascicular reentry involving a portion of the LV Purkinje fibers can lead to VT. This most commonly is associated with the left posterior fascicle giving rise to a characteristic narrow complex right bundle branch block (RBBB) superior axis QRS configuration (Belhassen’s VT).
Although implantable cardioverter-defibrillators (ICDS) are the mainstay of therapy to prevent sudden death, they do not prevent VAs, and can lead to painful shocks.
Medical therapy has limited efficacy and may introduce adverse side effects. Catheter ablation of VAs is a rapidly evolving field and an important alternative in the management of patients with this disease. VT ablation is often a preferred front line therapy in patients with structurally normal hearts. In this series of clinical vignettes, we highlight the range of substrate-specific strategies used in our electrophysiology laboratory for catheter ablation of VAs.
Case 1: Premature Ventricular ContractionsMs. AF is a 34 year-old woman with frequent palpitations, shortness of breath, and fatigue, with a known history of ventricular premature depolarizations (VPDs). She had previously been on metoprolol without improvement of symptoms. An electrocardiogram (Figure 1) revealed frequent premature ventricular contractions in a bigeminal pattern. An echocardiogram revealed a reduced ejection fraction of 45%. A 24-hour Holter monitor was performed which revealed ~ 30% burden of VPDs.
An EP study was performed with activation mapping of the right and left ventricular outflow tracts. Intra-cardiac echocardiography(Continued on page 12)
ArvindhN.Kanagasundram,M.D.
Sharon Shen, M.D.
Juan C. Estrada, M.D.
PabloSaavedra,M.D.
ChristopherR.Ellis,M.D.
BM
Figure 1Twelve-lead ECG of ventricular bigeminy

was used to create an anatomic shell of the outflow tracts and aortic sinuses, and mark the ostial locations of the left main and right coronary arteries. The earliest site of activation was mapped to the left ventricular outflow tract in the commissure between the right and left coronary cusps. Ablation was performed with immediate termination of the VPDs (Figure 2).
At the 3-month follow-up, the patient had improvement in her symptoms of palpitations and exertional intolerance. A repeat Holter monitor was performed which revealed rare VPDs (< 1%) with an echocardiogram showing normalization of her left ventricular size and function.
In the absence of structural heart disease, VPDs most commonly arise from the right or left ventricular outflow tracts, or the epicardial tissue immediately adjacent to the sinuses of Valsalva.3 The presentation can be quite variable, ranging from an incidental finding on electrocardiogram to left ventricular dysfunction and heart failure. Dyssynchrony4 resulting from abnormal ventricular activation is felt to be an important causal mechanism of cardiomyopathy with VPD burden in most cases being greater than 20% (but may occur at levels as low as 10%).5 The decision to suppress ectopy is largely based on symptoms, interference with effective cardiac resynchronization therapy, or suspicion
of VPD-induced cardiomyopathy. Catheter ablation can result in elimination of VPDs in greater than 80% of cases.6, 7
Case 2: Recurrent Ventricular TachycardiaMr. HM is a 67 year-old man with medical history significant for coronary artery disease status post 3-vessel bypass grafting, ischemic cardiomyopathy (ejection fraction ~ 30%), and biventricular ICD, who experienced recurrent ventricular tachycardia despite amiodarone and mexiletine, with frequent ICD shocks. He had failed two prior attempts at VT ablation.
This patient met the criteria for VT storm, which is defined as > 3 episodes of VT within a 24- hour period. Intravenous anti-arrhythmic medications, sympathetic modulation, and intra-aortic balloon pump are often first-line therapies in the management of patients in VT storm (Table 1). After transfer and initial measures to stabilize the patient, the decision was made to attempt repeat ablation.
Electroanatomic mapping was performed with confirmation of inferior wall scar extending up the septum. Ventricular extra-stimuli resulted in induction of 2 VT morphologies which matched the characteristics of the clinical tachycardias. Since these tachycardias were hemodynamically tolerated, limited entrainment mapping demonstrated a common isthmus in the basal infero-septum critical to both circuits. Ablation in this
BN
Catheter Ablation of Ventricular Arrhythmias: Clinical Vignettes(Continued from page 11)
Figure 2Electroanatomic map of the aortic cusps revealing the successful ablation site at commissure between the right and left coronary cusps. RCC: right coronary cusp, LCC: left coronary cusp
In the absence of structural heart disease, VPDs most commonly arise from the right or left ventricular outflow tracts, or the epicardial tissue immediately adjacent to the sinuses of Valsalva.
Management of VT Storm
Beta blockade
Anti-arrhythmicdrugtherapy
Intubation, general anesthesia
Neuraxialmodulation(thoracicepidural)
Mechanicalhemodynamicsupport
Catheter ablation
Table 1

region resulted in prompt termination of the VT (Figure 3) and inability to induce further VAs with aggressive stimulation. The patient has done well during a 12-month follow-up period without recurrent VA or ICD therapies.
Scars that support VT circuits are comprised of both dense fibrosis and viable myocytes which create a substrate for slow conduction required to sustain re-entrant circuits.8, 9 There are multiple strategies for mapping VT with the optimal strategy often using a combination of techniques. In hemodynamically unstable VT, pace mapping with substrate mapping can localize a critical region, and in selected cases percutaneous left ventricular assist device placement can support end-organ perfusion while effectively mapping the VT. The use of such devices may add potential risk and as such requires center expertise.10
Case 3: Successful Epicardial Cryoablation of Ventricular Tachycardia Not Amenable to Radiofrequency AblationMs. BB, a 70 year-old woman with a history atrial fibrillation, was found to have wide complex tachycardia. She underwent evaluation that included echocardiogram, cardiac MRI, and cardiac catheterization, which revealed normal cardiac structure and function and no evidence of coronary artery disease.
The tachycardia morphology was consistent with an exit site in the basal infero-septum. The slurred QRS onset with maximal deflection index (MDI) greater than 0.55 was consistent with an epicardial location (Figure 4). Percutaneous epicardial access was obtained and VT mapping was performed. The earliest site of activation was found on the right ventricular epicardium near the origin of the posterior descending artery (Figure 5). (Continued on page 14)
BO
Figure 3Endocardial electroanatomic map of the left ventricle showing a large inferior scar in red extending into the septum. Successful ablation was performed at the border zone of scar along the basal infero-septum.
Figure 4Twelve-lead ECG of VT. Morphology is consistent with an exit site close to the basal infero-septum. The slurred QRS onset with maximal deflection index (MD) > 0.55 is consistent with an epicardial origin.

BP
Radiofrequency (RF) ablation was then performed at this site with slowing and termination of the tachycardia. Spontaneous re-initiation was observed despite high power lesions (Figure 6). Cryoablation was performed using a 6mm cryoablation catheter to deliver three 4-minute lesions to -75C. VT terminated without re-initiation or ectopy from that region (Figure 7). The patient has done well during a 16-month follow-up period without recurrent VT.
RF energy remains the primary ablative modality in the epicardium. However, there are several challenges to effective RF delivery in this space including the absence of convective cooling from blood flow (which is required for adequate energy delivery), poor catheter stability, and potential damage to collateral structures (coronary arteries, phrenic nerve, esophagus, great vessels).11 Cryothermal energy may have several potential benefits including better stability (due to “cryoadherance” to tissue) and improved cooling in the absence of blood flow.12
Case 4: Hybrid Ventricular Tachycardia Ablation using a Novel CatheterMr. GV is a 66 year-old man with coronary artery disease with prior inferior myocardial infarction (4-vessel CABG in 1993), who was transferred in the setting of VT storm. He had undergone a previous endocardial study with
Figure 6Slowing and termination of VT with ablation in the epicardial surface of the basal infero-septum.
Catheter Ablation of Ventricular Arrhythmias: Clinical Vignettes(Continued from page 13)
Figure 5The successful site of ablation is mapped to the epicardial RV site as marked by the ablation catheter in these RAO and LAO fluoroscopic images. Right coronary angiography was performed to assess proximity to the posterior descending artery prior to ablation. *Tip of the ablation catheter
RAO LAO
Figure 7Successful ablation with a cryocatheter reaching a max negative temperature of -76C.
BQ
identification of an epicardial VT originating from the inferior wall of the left ventricle (LV). The decision was made to perform repeat endocardial and epicardial mapping with surgical access.
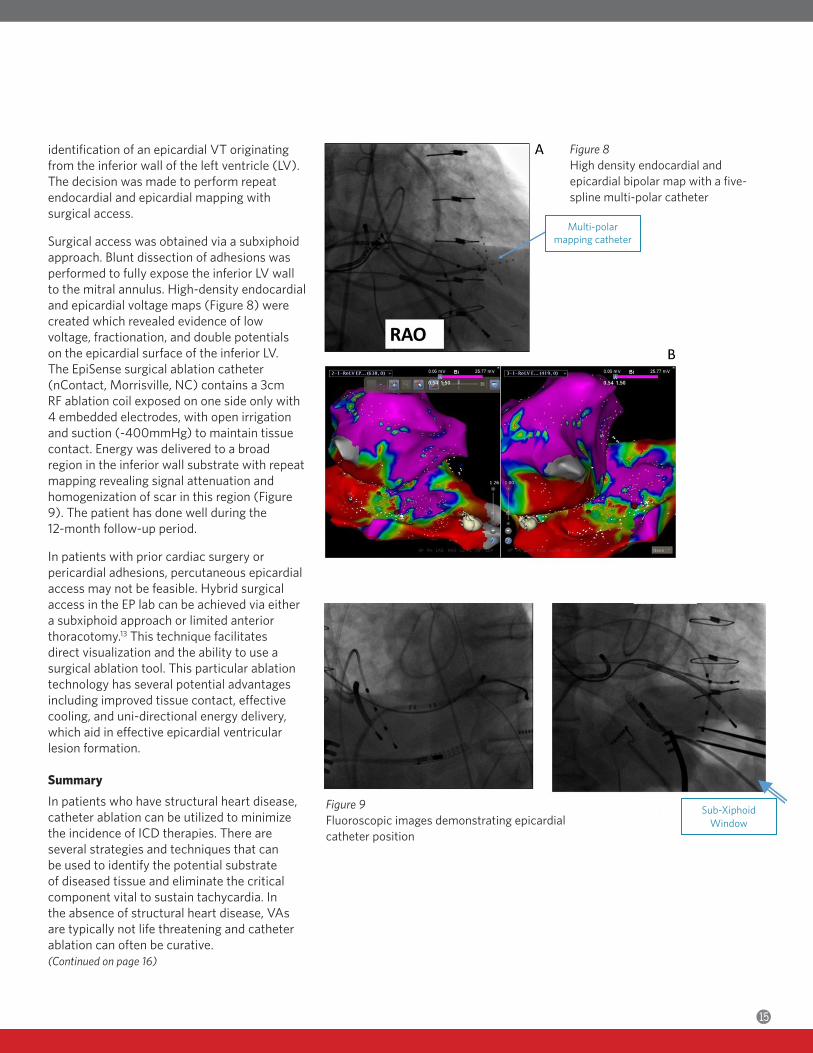
Surgical access was obtained via a subxiphoid approach. Blunt dissection of adhesions was performed to fully expose the inferior LV wall to the mitral annulus. High-density endocardial and epicardial voltage maps (Figure 8) were created which revealed evidence of low voltage, fractionation, and double potentials on the epicardial surface of the inferior LV. The EpiSense surgical ablation catheter (nContact, Morrisville, NC) contains a 3cm RF ablation coil exposed on one side only with 4 embedded electrodes, with open irrigation and suction (-400mmHg) to maintain tissue contact. Energy was delivered to a broad region in the inferior wall substrate with repeat mapping revealing signal attenuation and homogenization of scar in this region (Figure 9). The patient has done well during the 12-month follow-up period.
In patients with prior cardiac surgery or pericardial adhesions, percutaneous epicardial access may not be feasible. Hybrid surgical access in the EP lab can be achieved via either a subxiphoid approach or limited anterior thoracotomy.13 This technique facilitates direct visualization and the ability to use a surgical ablation tool. This particular ablation technology has several potential advantages including improved tissue contact, effective cooling, and uni-directional energy delivery, which aid in effective epicardial ventricular lesion formation.
SummaryIn patients who have structural heart disease, catheter ablation can be utilized to minimize the incidence of ICD therapies. There are several strategies and techniques that can be used to identify the potential substrate of diseased tissue and eliminate the critical component vital to sustain tachycardia. In the absence of structural heart disease, VAs are typically not life threatening and catheter ablation can often be curative. (Continued on page 16)
Figure 8High density endocardial and epicardial bipolar map with a five-spline multi-polar catheter
Figure 9Fluoroscopic images demonstrating epicardial catheter position
Multi-polarmapping catheter
Sub-XiphoidWindow
References:1. Lerman BB. Mechanism of outflow tract tachycardia. Heart Rhythm. 2007;4: 973-6.2. Lopera G, Stevenson WG, Soejima K, et al. Identification and ablation of three types of ventricular tachycardia involving the his-purkinje system in patients with heart disease. J Cardiovasc Electrophysiol. 2004;15:52-8.3. Kim RJ, Iwai S, Markowitz SM, et al. Clinical and electrophysiological spectrum of idiopathic ventricular outflow tract arrhythmias. J Am Coll Cardiol. 2007;49:2035-43.4. Del Carpio Munoz F, Syed FF, Noheria A, et al. Characteristics of premature ventricular complexes as correlates of reduced left ventricular systolic function: study of the burden, duration, coupling interval, morphology and site of origin of PVCs. J Cardiovasc Electrophysiol. 2011;22:791-8.5. Baman TS, Lange DC, Ilg KJ, et al. Relationship between burden of premature ventricular complexes and left ventricular function. Heart Rhythm. 2010;7:865-9.6. Yarlagadda RK, Iwai S, Stein KM, et al. Reversal of cardiomyopathy in patients with repetitive monomorphic ventricular ectopy originating from the right ventricular outflow tract. Circulation. 2005;112:1092-7.7. Bogun F, Crawford T, Reich S, et al. Radiofrequency ablation of frequent, idiopathic premature ventricular complexes: comparison with a control group without intervention. Heart Rhythm. 2007;4:863-7.
8. de Bakker JM, Coronel R, Tasseron S, et al. Ventricular tachycardia in the infarcted, Langendorff-perfused human heart: role of the arrangement of surviving cardiac fibers. J Am Coll Cardiol. 1990;15:1594-607.9. de Bakker JM, van Capelle FJ, Janse MJ, et al. Slow conduction in the infarcted human heart. ‘Zigzag’ course of activation. Circulation. 1993;88:915-26.10. Miller MA, Dukkipati SR, Koruth JS, et al. How to perform ventricular tachycardia ablation with a percutaneous left ventricular assist device. Heart Rhythm. 2012;9:1168-76.11. Tedrow U, Stevenson WG. Strategies for epicardial mapping and ablation of ventricular tachycardia. J Cardiovasc Electrophysiol. 2009;20:710-3.12. Jauregui-Abularach ME, Campos B, Betensky BP, et al. Comparison of epicardial cryoablation and irrigated radiofrequency ablation in a Swine infarct model. J Cardiovasc Electrophysiol. 2012;23:1016-23.13. Michowitz Y, Mathuria N, Tung R, et al. Hybrid procedures for epicardial catheter ablation of ventricular tachycardia: value of surgical access. Heart Rhythm. 2010;7:1635-43.
Catheter Ablation of Ventricular Arrhythmias: Clinical Vignettes(Continued from page 15)
VA N D E R B I LT U N I V E R S I T YVanderbilt Heart CommunicationsMCE, 5th floor, Ste. 51401215 21st Ave. S.Nashville, TN 37232-8802
NONPROFIT ORG.U.S. POSTAGE
PAIDNASHVILLE, TN
PERMIT NO. 3432
ToreferapatienttotheVanderbiltHeart&VascularInstitute,call(615)343-9188.