agenda - lpbcc.files.wordpress.com file12.10.2011 · lambeth clinical commissioning collaborative...
TRANSCRIPT

Adrian McLachlan, Lambeth Clinical Commissioning Collaborative Board Chair Andrew Eyres, Managing Director
Lambeth Clinical Commissioning Collaborative Board (LCCCB)
All Practice Event
Wednesday 12th October 2011 1.00 – 4.00pm
Planned outcomes of the day
Contribute to the development of clinically led commissioning in Lambeth
Increase awareness of the different clinical and non-clinical roles that contribute to successful clinical led commissioning
Develop ownership of the Strategic Plan and ensure local plans are robust
Share progress to date, good practice and learning
Agenda
1.00pm Welcome and Introductions Adrian McLachlan Chair of the LCCCB
1.10pm Overview Progress in Clinical Commissioning
– Improving Health, Improving Quality
Adrian McLachlan Chair of the LCCCB Andrew Eyres Managing Director, Lambeth, BSU
1.30pm Patient Perspectives – Diabetes
2.10pm Group Work: Delivering our Programmes – followed by coffee break
Andrew Eyres Managing Director, Lambeth, BSU
3.10pm Update on the Future Forum Ash Soni, Clinical Network Lead
3.15pm View from Practice Managers Marie Ah-Moye, Practice Manager, Tulse Hill Practice
Jenny Hoggins, Practice Manager – Stockwell Group Practice
3.30pm Question Time and Next Steps
LCCCB Panel
4.00pm Close
Copies of presentations will be available on the website
Age
nda


Lambeth Clinical Commissioning Collaborative Board (LCCCB)
All Practice Event
Wednesday 12th October 2011
Group One - Urgent Care
Lambeth continues to have high levels of A&E attendance and local audits reveal that between 40-60% of people attending A&E could have their care provided safely and appropriately in primary and community settings. Please join this group to find out more about Lambeth’s Unscheduled Care Strategy and how we proactively manage high A&E attendance rates across the borough. Lambeth has been working with St Thomas’ to identify the cohorts of patients that frequently re-attend A&E and we would like to discuss the findings with you. This session will be interactive and your feedback is essential in taking our Unscheduled Care Strategy forward.
Gro
up 1
- U
rgen
t Car
e


Unplanned Care Programme The aim of the Unplanned Care Programme to is to design and implement improved unplanned care services across Lambeth that support the shift to improved health outcomes through greater planned and co-ordinated care, and reflected in lower A&E attendances and subsequent emergency admissions, fewer readmissions, enhanced quality of care and the delivery of national standards. The Unplanned Care Programme operates across two main workstreams:
Frail Elderly, (includes admission avoidance and intermediate care)
Urgent Care, (including Urgent Care Centres, Out of Hours and the Single Point of Access / 111 Initiative)
This Group will be looking at Urgent Care. Urgent Care Lambeth continues to have high levels of A&E attendance and local audits reveal that between 40-60% of people attending A&E could have their care provided safely and appropriately in primary and community settings. Please join this group to find out more about Lambeth’s Unscheduled Care Strategy including an update on Front-end A&E at Guy’s and St Thomas’, King’s and St George’s. We will also update you on the Single Point of Access / 111 Project currently underway and welcome your feedback on current plans to support the Unscheduled Care Strategy. We will also be looking at A&E attendance data by borough (Lambeth, Southwark, Lewisham) over the last three years, which highlights some improvements, so it will be interesting to find out what works well. We would also like to share data that highlight’s the high usage of A&E during core hours. This gives us the opportunity to discuss what we might do differently to address this issue. Lambeth has also been working with St Thomas’ to identify the cohorts of patients that frequently re-attend A&E and we would like to discuss the findings with you. This session will be interactive and your feedback is essential in taking our Unscheduled Care Strategy forward. Data Attached
SEL Cluster trend over 3 years – A&E Attendance by Provider
SEL Cluster Bar Chart Comparison over 3 years – A&E Attendance Qtr 1
Lambeth trend over 2 years – A&E Attendance by Provider
A&E Attendance during core hours
Gro
up 1
- U
rgen
t Car
e


0
20
00
40
00
60
00
80
00
10
00
0
12
00
0
14
00
0
Apr. '08
May '08
Jun. '08
Jul. '08
Aug. '08
Sep. '08
Oct. '08
Nov. '08
Dec. '08
Jan. '09
Feb. '09
Mar. '09
Apr. '09
May '09
Jun. '09
Jul. '09
Aug. '09
Sep. '09
Oct. '09
Nov. '09
Dec. '09
Jan. '10
Feb. '10
Mar. '10
Apr. '10
May '10
Jun. '10
Jul. '10
Aug. '10
Sep. '10
Oct. '10
Nov. '10
Dec. '10
Jan. '11
Feb. '11
Mar. '11
Apr. '11
May '11
Jun. '11
Jul. '11
Axis Title
A&
E A
tte
nd
ance
s (N
.B.
Kin
g's
did
no
t su
bm
it t
o S
US
in '0
8/9
, so
me
Gre
en
wic
h d
ata
mis
sin
g in
'09
/10
)
Bex
ley
Bro
mle
y
Gre
enw
ich
Lam
bet
h
Lew
ish
am
Sou
thw
ark
Gro
up 1
- U
rgen
t Car
e

0
50
00
10
00
0
15
00
0
20
00
0
25
00
0
30
00
0
35
00
0
40
00
0
45
00
0
50
00
0
Bex
ley
Bro
mle
y G
reen
wic
h
Lam
bet
h
Lew
ish
am
Sou
thw
ark
A&
E A
tte
nd
ance
s
(N.B
. K
ing'
s d
id n
ot
sub
mit
in 2
00
8/9
)
Ap
r. -
Ju
l. '0
8
Ap
r. -
Ju
l. '0
9
Ap
r. -
Ju
l. '1
0
Ap
r. -
Ju
l. '1
1

0
20
00
40
00
60
00
80
00
10
00
0
12
00
0
14
00
0
Ap
r.
'09
May
'0
9
Jun
. '0
9
Jul.
'09
Au
g.
'09
Se
p.
'09
O
ct.
'09
No
v.
'09
Dec
. '0
9
Jan
. '1
0
Feb
. '1
0 M
ar.
'10
A
pr.
'1
0 M
ay
'10
Ju
n.
'10
Ju
l. '1
0 A
ug.
'1
0
Sep
. '1
0
Oct
. '1
0 N
ov.
'1
0 D
ec.
'10
Ja
n.
'11
Fe
b.
'11
Mar
. '1
1
Ap
r.
'11
May
'1
1
Jun
. '1
1
Jul.
'11
A&
E A
tte
nd
ance
s -
Lam
bet
h
Lam
bet
h
Lin
ear
(Lam
bet
h)
Gro
up 1
- U
rgen
t Car
e


Provider
GP Core
Hours
(8.00am -
6.30pm)
GP Out of
Hours
(6.30pm -
8.00am)
GUY'S AND ST THOMAS' NHS FOUNDATION TRUST 64% 36%
KING'S COLLEGE HOSPITAL NHS FOUNDATION TRUST 61% 39%
ST GEORGE'S HEALTHCARE NHS TRUST 60% 40%
Total 62% 38%
0%
10%
20%
30%
40%
50%
60%
70%
GUY'S AND ST THOMAS' NHS FOUNDATION TRUST
KING'S COLLEGE HOSPITAL NHS FOUNDATION TRUST
ST GEORGE'S HEALTHCARE NHS TRUST
%
AE Providers
Percentage busy times in Lambeth AE Providers
GP Core Hours (8.00am - 6.30pm)
GP Out of Hours (6.30pm - 8.00am)
Gro
up 1
- U
rgen
t Car
e


Lambeth Clinical Commissioning Collaborative Board (LCCCB)
All Practice Event
Wednesday 12th October 2011
Group Two – Hypertension/
Cardiovascular Risks
Although good progress has been made, reducing premature mortality and health inequalities from cardiovascular disease remains an important priority for Lambeth. The purpose of this workshop is to review how best to reduce this excess premature mortality from cardiovascular disease by a focus on primary and secondary prevention.
Gro
up 2
- H
yper
tens
ion/
Car
diov
ascu
lar
Ris
ks


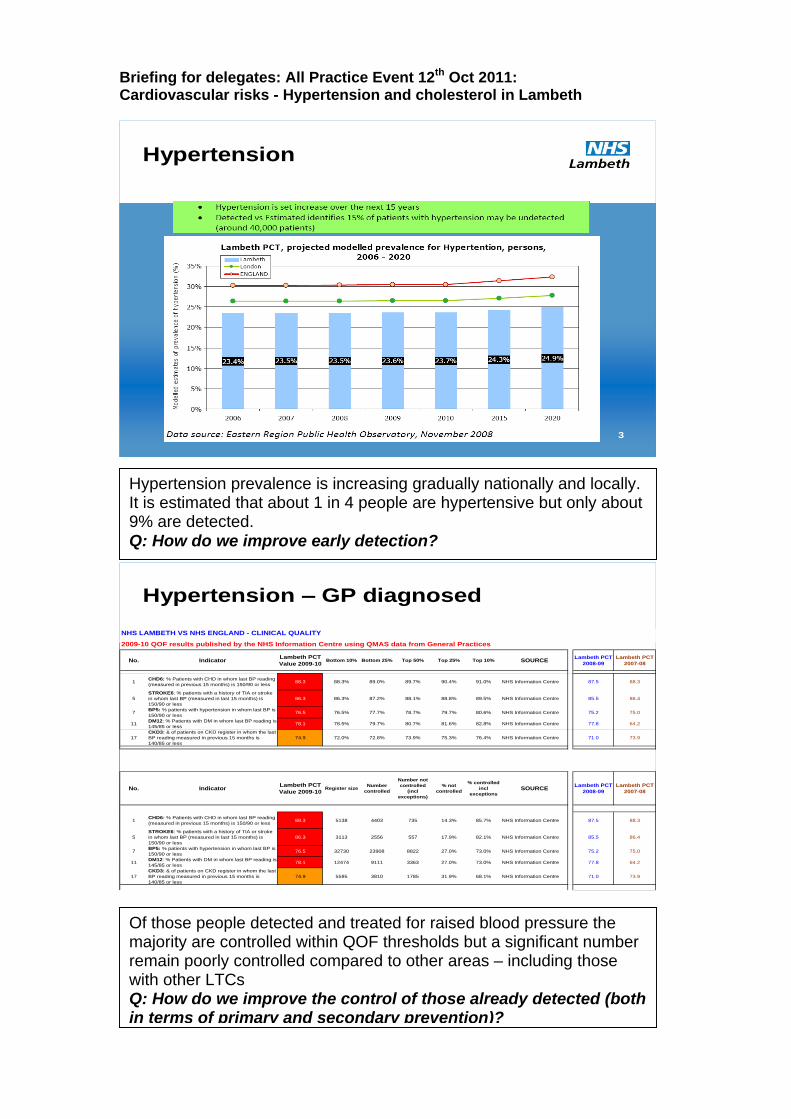
Briefing for delegates: All Practice Event 12th Oct 2011: Cardiovascular risks - Hypertension and cholesterol in Lambeth
16
Risk factors
Source: The World Health Report 2002
23
Met/unmet need
Hypertension and cholesterol (as well as smoking) are important reversible risk factors for cardiovascular disease.
Although there has been a decline in cardiovascular disease mortality in the last 10-15 years it remains an important problem with a relatively higher burden in Lambeth.
Gro
up 2
- H
yper
tens
ion/
Car
diov
ascu
lar
Ris
ks
Briefing for delegates: All Practice Event 12th Oct 2011: Cardiovascular risks - Hypertension and cholesterol in Lambeth
3
Hypertension
4
Hypertension – GP diagnosed
NHS LAMBETH VS NHS ENGLAND - CLINICAL QUALITY
2009-10 QOF results published by the NHS Information Centre using QMAS data from General Practices
No. IndicatorLambeth PCT
Value 2009-10Bottom 10% Bottom 25% Top 50% Top 25% Top 10% SOURCE
Lambeth PCT
2008-09
Lambeth PCT
2007-08
1CHD6: % Patients with CHD in whom last BP reading
(measured in previous 15 months) is 150/90 or less88.3 88.3% 89.0% 89.7% 90.4% 91.0% NHS Information Centre 87.5 88.3
5
STROKE6: % patients with a history of TIA or stroke
in whom last BP (measured in last 15 months) is
150/90 or less
86.3 86.3% 87.2% 88.1% 88.8% 89.5% NHS Information Centre 85.5 86.4
7BP5: % patients with hypertension in whom last BP is
150/90 or less76.5 76.5% 77.7% 78.7% 79.7% 80.6% NHS Information Centre 75.2 75.0
11DM12: % Patients with DM in whom last BP reading is
145/85 or less78.1 78.5% 79.7% 80.7% 81.6% 82.8% NHS Information Centre 77.8 64.2
17
CKD3: & of patients on CKD register in whom the last
BP reading measured in previous 15 months is
140/85 or less
74.9 72.0% 72.8% 73.9% 75.3% 76.4% NHS Information Centre 71.0 73.9
No. IndicatorLambeth PCT
Value 2009-10Register size
Number
controlled
Number not
controlled
(incl
exceptions)
% not
controlled
% controlled
incl
exceptions
SOURCELambeth PCT
2008-09
Lambeth PCT
2007-08
1CHD6: % Patients with CHD in whom last BP reading
(measured in previous 15 months) is 150/90 or less88.3 5138 4403 735 14.3% 85.7% NHS Information Centre 87.5 88.3
5
STROKE6: % patients with a history of TIA or stroke
in whom last BP (measured in last 15 months) is
150/90 or less
86.3 3113 2556 557 17.9% 82.1% NHS Information Centre 85.5 86.4
7BP5: % patients with hypertension in whom last BP is
150/90 or less76.5 32730 23908 8822 27.0% 73.0% NHS Information Centre 75.2 75.0
11DM12: % Patients with DM in whom last BP reading is
145/85 or less78.1 12474 9111 3363 27.0% 73.0% NHS Information Centre 77.8 64.2
17
CKD3: & of patients on CKD register in whom the last
BP reading measured in previous 15 months is
140/85 or less
74.9 5595 3810 1785 31.9% 68.1% NHS Information Centre 71.0 73.9
Hypertension prevalence is increasing gradually nationally and locally. It is estimated that about 1 in 4 people are hypertensive but only about 9% are detected. Q: How do we improve early detection?
Of those people detected and treated for raised blood pressure the majority are controlled within QOF thresholds but a significant number remain poorly controlled compared to other areas – including those with other LTCs Q: How do we improve the control of those already detected (both in terms of primary and secondary prevention)?

Briefing for delegates: All Practice Event 12th Oct 2011: Cardiovascular risks - Hypertension and cholesterol in Lambeth
5
Hypertension – GP variation
NHS LAMBETH GENERAL PRACTICES VARIATION - CLINICAL QUALITY
2009-10 QOF results published by the NHS Information Centre (QMAS) for Lambeth General Practices
No. IndicatorLambeth PCT
Value 2009-10
Lambeth GP
Lowest ValueBottom 10% Bottom 25% Top 50% Top 25% Top 10%
Lambeth GP
Best Value
1CHD6: % Patients with CHD in whom last BP reading
(measured in previous 15 months) is 150/90 or less88.3 73.3% 88.3% 89.0% 89.7% 90.4% 91.0% 100.0%
5
STROKE6: % patients with a history of TIA or stroke
in whom last BP (measured in last 15 months) is
150/90 or less
86.3 66.8% 86.3% 87.2% 88.1% 88.8% 89.5% 100.0%
7BP5: % patients with hypertension in whom last BP is
150/90 or less76.5 66.8% 76.5% 77.7% 78.7% 79.7% 80.6% 90.7%
11DM12: % Patients with DM in whom last BP reading is
145/85 or less78.1 66.7% 78.5% 79.7% 80.7% 81.6% 82.8% 91.9%
17
CKD3: & of patients on CKD register in whom the last
BP reading measured in previous 15 months is
140/85 or less
74.9 53.3% 72.0% 72.8% 73.9% 75.3% 76.4% 91.8%
England PCTs' performance
10
Cholesterol
Secondary prevention
NHS LAMBETH VS NHS ENGLAND - CLINICAL QUALITY
2009-10 QOF results published by the NHS Information Centre using QMAS data from General Practices
No. IndicatorLambeth PCT
Value 2009-10Top 10% Top 25% Top 50% Bottom 25% Bottom 10% SOURCE
Lambeth PCT
2008-09
Lambeth PCT
2007-08
2
CHD8: % Patients with CHD whose last measured
total cholesterol (measured in previous 15 months) is
5mmol/l or less.
79.5 84.2% 83.1% 82.0% 80.7% 79.5% NHS Information Centre 78.6 79.6
6STROKE8: % patients with TIA or stroke whose last
measured total cholesterol is 5 or less74.3 79.6% 78.6% 77.3% 75.6% 74.2% NHS Information Centre 73.0 73.8
12
DM17: % Patients with DM whose last measured total
cholesterol (measured in previous 15 months) is
5mmol/l or less.
79.9 85.4% 84.3% 83.1% 81.5% 79.9% NHS Information Centre 78.5 80.3
Total
Cholesterol
Grand
Totalmmol/l Yes No
</=2 17 7 24
2.1- 2.5 133 20 153
2.6.- 3.0 640 87 727
3.1 - 3.5 1437 229 1666
3.6 - 4.0 1834 486 2320
4.1 - 4.5 1690 743 2433
4.5 - 5.0 1241 704 1945
5.1 - 5.5 697 418 1115
5.6 - 6.0 452 239 691
6.1 - 6.5 308 127 435
6.6 - 7.0 176 63 239
>7 187 56 243
Total 8812 3179 11991
Prescribed Statin
1. A number of people don’t appear to have a
cholesterol level measured
2. A significant number of people are prescribed
a statin but remain poorly controlled.
3. A number of people who are uncontrolled are
not prescribed a statin
Source: Lambeth DataNet 2011
There is wide variation between practices within Lambeth in the control of people with raised blood pressure – some of this is likely to both avoidable and unjustifiable. Q: How do we reduce intra-practice variation in control of blood pressure?
Gro
up 2
- H
yper
tens
ion/
Car
diov
ascu
lar
Ris
ks

Briefing for delegates: All Practice Event 12th Oct 2011: Cardiovascular risks - Hypertension and cholesterol in Lambeth
8
CVD risk factors
Teenagers
/Adolescent
Young school agePre-schoolPre-natal
Older people (65+)Adults (18-65)CYP (0-18)Population
Group
Wider
determinants
Primary
prevention
Secondary
prevention
End of Life
Population strategies to reduce CVD risk
Early detection, effective diagnosis
& management including lifestyle
advice to reduce CVD risk
Effective management in
people with LTCs (secondary
prevention of CVD risk)
Of those people with LTCs (CHD, Diabetes and Stroke/TIA) and a measure of cholesterol in past 15 months one in four are not controlled (QOF threshold value). Data from Lambeth DataNet suggests that poor control of risk factors tends to cluster (i.e. poor control of one CVD risk factor is also associated with poor control of other risk factors). Q: How do systematise the control of all avoidable CVD risk factors into a coherent approach in Lambeth?
The current Strategic Plan (SP) target focuses on control of blood pressure in people with CHD only (735 patients with uncontrolled blood pressure – QOF threshold - in a register size of 5138). Q: What should be the focus for Lambeth in terms of setting a target for prevention of CVD? How should this be performance managed?

Lambeth Clinical Commissioning Collaborative Board (LCCCB)
All Practice Event
Wednesday 12th October 2011
Group Three – Staying Healthy
The greatest contributors to premature morality in Lambeth are vascular disease and cancer which can be prevented by addressing some common risk factors (tobacco & alcohol use, inactivity and poor diet). Discussion will be focused around smoking, alcohol and current programmes.
G
roup
3 -
Sta
ying
Hea
lthy


NHS Lambeth Staying Healthy Programme
Although life expectancy continues to improve for both males and females in Lambeth, it is still lower than the England average. The greatest contributors to premature morality in Lambeth are vascular disease and cancer which can be prevented by addressing some common risk factors (tobacco & alcohol use, inactivity and poor diet). Up to 80% of heart disease, stroke, and type 2 diabetes and over a third of cancers could be prevented by eliminating shared risk factors, mainly tobacco use, unhealthy diet, physical inactivity and the harmful use of alcohol. The Staying Healthy Programme seeks to improve health outcomes and reduce health inequalities through the commissioning of systematic health promotion and prevention services. The Programme covers the following areas: Smoking Cessation and Tobacco Control, NHS Health Checks (Vascular Checks), Adult Obesity and Physical Activity, Alcohol Prevention, Mental Wellbeing, Lambeth Early Intervention and Prevention Service and Sexual Health, and Infection Prevention.
Tobacco Control: Smoking is one of the largest causes of preventable premature death. The prevalence of smoking in Lambeth is estimated as 25.2% compared to the national average of 22.2%. Between 2007 and 2009 there were an estimated 272 smoking attributable deaths compared to the England average of approximately 216 deaths.. Smoking cessation as part of wider tobacco control measures is one of NHS Lambeth’s priorities and local targets have been set in addition to the Department of Health performance targets. In 2010/11 the PCT achieved 2482 4 week quitters which exceeded the DH target of 1908 but fell short of the PCT target of 2482. This year emphasis is being made to increase the quality of the service as well as more timely submission of stop smoking data. The DH 4 week quitter target is 1935 whilst the NHS Lambeth target is 2532. NHS Health Checks: The NHS Health Check is a national programme to assess people aged 40 -74 every five years for their risk of developing heart disease, stroke, diabetes and kidney disease within the next 10 years. Patients without CVD are offered lifestyle advice and support to help prevent them from developing it. Those patients identified with a CVD related condition are placed on the appropriate disease register for management of their condition. The service is delivered by GP practices and there is an outreach service provided by GSTT community services. In 2010/2011 4,810 people (17% of the eligible population) were offered a health check. The target for 2011/2012 is for at least 20% of the eligible population to be offered the check. The focus of the work this year has been to improve reporting mechanisms and to increase practice uptake. Referrals to appropriate support through a single referral system (Lambeth Early Intervention and Prevention Service) are being promoted. . Lambeth Early Intervention and Prevention Service (LEIPS): Implementation of the new LEIP service began in July 2011. The LEIPS is an integrated health
Gro
up 3
- S
tayi
ng H
ealth
y

improvement service offering support for clients around diet, exercise, smoking cessation, alcohol, in addition to the services provided by Health Trainers. Referral to this service is through a single referral system. The service will be engaging with practices to raise awareness of the services being offered. Childhood Obesity: Addressing childhood obesity is a priority for Lambeth. Results of the National Child Measurement Programme (NCMP) 2009/10 show
that nearly 14% of young children (5‐6 years) in Lambeth schools are obese; this
is higher than the national and London average. Amongst children aged 10‐11, 1
in 4 of all Lambeth school children are obese which is substantially higher than seen nationally. The PCT aims to reduce childhood obesity prevalence from a baseline of 25.1% to 23.2% by 2015 as measured by the NCMP (year 6). Prioritised evidence based interventions are being commissioned to help tackle the issue and form part of the Lambeth multi-agency healthy Weight care pathway for children (0 – 11years). Interventions include promoting breastfeeding through the accreditation of all children centres as UNICEF Baby Friendly, Level; Level 1 healthy weight training for health and non-health practitioners; healthy weight promoting schools and the commissioning of Levels 2 and 3 children’s weight management services. Level 1 training is currently being offered to all those working with children and families. The Level 3 service will start at the end of October, whilst the Level 2 service will commence in January 2012. Information will be provided to practices once the services are up and running. Alcohol: Alcohol misuse is a risk to health locally with about 20% of the adult population estimated to be binge drinkers, similar to the national average but higher than London (14.3%). Higher risk drinkers make up 5.9% (13,358 people) locally and London has a slightly lower estimate at 5%. Increasing risk drinkers comprise 17% (38,064 people), less than London (18.8%). Those at lower risk/abstinent make up the remaining 77.1%. Admissions to hospital for alcohol related conditions have declined in the last two years to 1470.3 per 100,000 admissions in 2008/9, slightly less than London and England, prior to that Lambeth had a high and increasing rate. The mortality rate related to alcohol in Lambeth (33.6 per 100,000) remains higher than that in London (23.2) and England (25.7) in 2007/8, but has declined slightly over recent years. A range of services are being offered across different agencies in Lambeth. In the health service, 85% of General Practices are delivering screening and brief interventions (SBI), with SBI’s also part of the NHS Health checks. Specialist services have been remodelled to improve access and capacity for primary care to a specialist team of drug and alcohol workers. An alcohol specialist nurse is also in post in the acute trust (GSTT); and the Homeless Team (Three Boroughs) works with particularly vulnerable people.

Questions Alcohol
How best to support practices so that screening and brief interventions are done to a high standard to maximise effectiveness?
What specialist service support in the community do you require to improve alcohol care?
Smoking
What is needed to improve success rates and timely submission of stop smoking data?
LEIPS
What are Practices experiences so far of the Lambeth Early Intervention and Prevention Service?
Childhood Obesity
What are the ways in which practices can best be engaged to support the Lambeth Children’s Healthy Weight Care Pathway and to provide referrals to the appropriate services?
Gro
up 3
- S
tayi
ng H
ealth
y


Lambeth Clinical Commissioning Collaborative Board (LCCCB)
All Practice Event
Wednesday 12th October 2011
Group Four – Reducing Variation
Lambeth has started to successfully reduce variation in GP referrals and other outpatient attendances. This workshop will engage participants in identifying what has worked well, what could be done to support further improvement and what are the potential barriers enablers such as to checklist and choose and book utilisation.
Gro
up 4
- R
educ
ing
Var
iatio
n


Reducing Variation in GP referrals
National research indicates that referral rates to a particular specialty within a single area vary by as much as 10-fold between GPs (Creed et al 1990; Ashworth et al 2002). There is strong evidence that a wide variety of factors account for this variation, clinical and non-clinical (Foot et al 2010). The available research suggests that not all referrals are necessary in clinical terms and a substantial proportion of activity is discretionary and avoidable. Local specialty specific audit work indicates an 8 fold variation in GP referral rates (unstandardised).
There are also patients who need a referral but fail to receive one. For example, lack of or late referral is thought to be a key driver of poor survival rates for cancer (Department of Health 2011b).
Over the last few months, there has been significant work to support practices in reducing local variation and as such we have been road-testing a programme of visits and an information pack. Priority actions and good practice identified from these visits will be shared following the first round and review meetings will take place in early 2012. Early indicators are that this combined effort has started to have an impact. For 2011/12 we have a target saving of £1.2m relating to GP referrals (informed by benchmarks), or £510k by August. As at August £410k (80%) of this saving had been achieved. Well done to all who have contributed to this achievement! Of course, not all outpatient activity is initiated by GPs. First outpatient attendances are also initiated by General Dental Practitioners, Consultants, A&E and for a limited number specialties there are self referrals/walk-ins. There are similar efforts to reduce variation from these sources. In particular, activity levels for consultant-to-consultant referrals and follow-ups have been capped at local Trusts and payment will not be made over these agreed activity levels. Policies regarding appropriateness of consultant-to-consultant referrals are also being reviewed. Attached some benchmarked information on outpatient activity levels.
Gro
up 4
- R
educ
ing
Var
iatio
n

Group work In the group work we’d like to capture participants’ input in to: What are the savings on GP referrals to date attributable to? What has made the biggest difference? How could we have more impact? Pre-referral checklists to support referrers in making decisions to refer are available in Lambeth. Are you aware of the checklists? How could we increase utilisation? Nationally choose and book, including use of the advice and guidance function, has been successfully used to reduce variation in referrals. What are the local barriers to rolling this out for Lambeth? What value could engaging patients more in this work add? How should we do it to best effect?

Firs
t
Spec
Lam
bet
h P
CT
Lon
do
n S
HA
% v
aria
nce
Car
dio
logy
6.5
13.7
7.13
5
Clin
ical
Hae
mat
olo
gy2.
42.
2-0
.224
Der
mat
olo
gy14
.113
.9-0
.341
Dia
bet
ic M
edic
ine
3.3
3-0
.333
End
ocr
ino
logy
21.
9-0
.12
ENT
9.5
13.8
4.20
5
Gas
tro
ente
rolo
gy5.
36.
30.
947
Gen
eral
Su
rger
y5.
711
.25.
443
Ger
iatr
ic M
edic
ine
21.
7-0
.32
Gyn
aeco
logy
16.5
16.6
-0.0
65
Hep
ato
logy
0.8
0.5
-0.3
08
Neu
rolo
gy3.
95.
51.
561
Op
hth
alm
olo
gy18
.617
.9-0
.886
Pae
dia
tric
Clin
ical
Hae
mat
olo
gy2.
10.
3-1
.821
Pai
n M
anag
emen
t0.
71.
70.
993
Reh
eum
ato
logy
4.6
5.6
0.95
4
Res
pir
ato
ry M
edic
ine
2.5
3.3
0.77
5
T&O
1118
6.89
Uro
logy
7.1
80.
829
Foll
ow
-Up
Spec
Lam
bet
h P
CT
Lon
do
n S
HA
% v
aria
nce
Car
dio
logy
1.8
1.3
-0.5
18
Clin
ical
Hae
mat
olo
gy4.
67.
52.
854
Der
mat
olo
gy2.
26.
34.
078
Dia
bet
ic M
edic
ine
0
End
ocr
ino
logy
0
ENT
1.3
1.3
-0.0
13
Gas
tro
ente
rolo
gy1.
92.
00.
081
Gen
eral
Su
rger
y1.
61.
6-0
.016
Ger
iatr
ic M
edic
ine
0
Gyn
aeco
logy
1.0
1.2
0.19
Hep
ato
logy
0
No
te
The
follo
win
g sp
ecia
litie
s h
ave
bee
n e
xclu
ded
fro
m t
he
rep
ort
as d
ata
in N
HS
com
par
ato
rs is
inco
mp
lete
Dia
bet
ic M
edic
ine
End
ocr
ino
logy
Ger
iatr
ic M
edic
ine
Hep
ato
logy
Pae
dia
tric
Clin
ical
Hae
mat
olo
gy
Pai
n M
anag
emen
t0 2 4 6 8 10
12
14
16
18
20
Cardiology
Clinical Haematology
Dermatology
Diabetic Medicine
Endocrinology
ENT
Gastroenterology
General Surgery
Geriatric Medicine
Gynaecology
Hepatology
Neurology
Ophthalmology
Paediatric Clinical …
Pain Management
Reheumatology
Respiratory Medicine
T&O
Urology
Rates Per 1000
Spe
cial
ity
10/1
1 G
P N
ew
Ra
tes
Per
10
00 f
or
Lam
bet
h A
gain
st L
on
do
n P
osi
tio
n
Lam
bet
h P
CT
Lon
do
n S
HA
0
5
10
15
20
25
30
35
40
Cardiology
Clinical Haematology
Dermatology
Diabetic Medicine
Endocrinology
ENT
Gastroenterology
General Surgery
Geriatric Medicine
Gynaecology
Hepatology
Neurology
Ophthalmology
Paediatric Clinical …
Pain Management
Reheumatology
Respiratory Medicine
T&O
Urology
Attendance Ratio
Spec
ialit
y
10/
11 O
utp
atie
nt
Follo
w-u
p T
o F
irst
Att
en
dan
ce R
ati
o
Lam
bet
h P
CT
Lon
do
n S
HA
Gro
up 4
- C
hart
s


Var
ian
ce a
nal
ysis
fo
r Fi
rst
atte
nd
ance
s in
lam
be
th f
or
Top
sp
eci
alit
ies
Sum
mar
y:
• Fo
r Fi
rst
atte
nd
ance
s, o
vera
ll co
st h
as g
on
e u
p b
y 4
77
k b
ut
acti
vity
has
red
uce
d
• A
ctiv
ity
and
co
st h
as r
edu
ced
fo
r: (
Der
mat
olo
gy, E
NT,
Gyn
ae, N
euro
logy
an
d T
&O
)
• Th
ere
is a
dec
reas
e in
co
st b
ut
an in
crea
se in
act
ivit
y in
: (G
eria
tric
Med
an
d P
ain
Mn
gt)
• Th
ere
is a
n in
crea
se in
co
st b
ut
a d
ecre
ase
in a
ctiv
ity
in: (
Clin
ical
Hae
mat
olo
gy, G
astr
o a
nd
Gen
eral
)
* In
tro
du
ctio
n o
f G
PSI
in S
E lo
calit
y an
d b
oro
ugh
wid
e G
P e
du
cati
on
pro
gram
me
has
red
uce
d d
erm
ato
logy
ref
erra
ls.
* T&
O a
ctiv
ity
and
co
st h
ave
red
uce
d d
ue
to M
CA
TTs,
ho
wev
er t
he
09
/10
dat
a in
clu
des
so
me
ph
ysio
ther
apy
act
ivit
y fo
r K
CH
wh
ich
is n
ot
incl
ud
ed in
th
e 1
0/1
1 a
ctiv
ity.
Th
eref
ore
th
e re
du
ctio
n in
act
ivit
y 3
00
att
end
s lo
wer
th
an r
epo
rted
.
* O
pth
alm
olo
gy r
efer
rals
hav
e si
gnif
ican
tly
incr
ease
d.
• A
ctiv
ity
and
co
st h
ave
incr
ease
d f
or:
(C
ard
io, D
iab
Med
, En
do
crin
olo
gy, H
epat
olo
gy, O
ph
thal
mo
logy
,
Pae
dia
tric
Clin
ical
Hae
mat
olo
gy, R
esp
irat
ory
Med
icin
e, R
heu
mat
olo
gy a
nd
Uro
logy
)
-5000
-4000
-3000
-2000
-1000
0
1000
2000
3000
Cardiology
Clinical Haematology
Dermatology
Diabetic Medicine
Endocrinology
Ent
Gastroenterology
General Surgery
Geriatric Medicine
Gynaecology
Hepatology
Neurology
Ophthalmology
Paediatric Clinical Haematology
Pain Management
Respiratory Medicine
Rheumatology
Trauma & Orthopaedics
Urology
Ou
tpa
tie
nt A
cti
vit
y, f
irs
t a
tte
nd
an
ce
, va
ria
nc
e 0
9/1
0 t
o 1
0/1
1
-800000
-600000
-400000
-200000
0
200000
400000
600000
Cardiology
Clinical Haematology
Dermatology
Diabetic Medicine
Endocrinology
Ent
Gastroenterology
General Surgery
Geriatric Medicine
Gynaecology
Hepatology
Neurology
Ophthalmology
Paediatric Clinical Haematology
Pain Management
Respiratory Medicine
Rheumatology
Trauma & Orthopaedics
Urology
Ou
tpati
en
t C
ost,
fir
st
att
en
dan
ce, vari
an
ce 0
9/1
0 -
10/1
1
Gro
up 4
- C
hart
s

Var
ian
ce a
nal
ysis
fo
r fo
llow
up
att
en
dan
ces
in la
mb
eth
fo
r To
p s
pec
ialit
ies
Sum
mar
y:
• Fo
r fo
llow
up
att
end
ance
s, o
vera
ll re
du
ctio
n in
Act
ivit
y an
d C
ost
fo
r A
ll La
mb
eth
To
p S
pec
ialt
ies
• ac
tivi
ty a
nd
co
st h
as r
edu
ced
fo
r: (
ENT,
Gas
tro
, Ger
iatr
ic m
edec
ine
and
Gyn
ae)
• th
ere
is a
dec
reas
e in
co
st b
ut
an in
crea
se in
act
ivit
y in
: (D
erm
ato
logy
, Hep
ato
logy
an
d U
rolo
gy)
• th
ere
is a
n in
crea
se in
co
st b
ut
a d
ecre
ase
in a
ctiv
ity
in: (
Pai
n M
ngt
an
d R
esp
irat
ory
Med
)
* T&
O a
ctiv
ity
follo
w u
p a
ctiv
ity
and
co
st h
ave
red
uce
d d
ue
to M
CA
TTs,
ho
we
ver
the
09
/10
dat
a in
clu
des
so
me
ph
ysio
ther
apy
ac
tivi
ty f
or
KC
H w
hic
h is
no
t in
clu
ded
in t
he
10
/11
act
ivit
y. T
her
efo
re t
he
red
uct
ion
in a
ctiv
ity
900
att
end
s lo
we
r th
an r
epo
rted
.
• ac
tivi
ty a
nd
co
st a
nd
incr
ease
d f
or:
(C
ard
io, C
linic
al H
aem
ato
logy
, Gen
eral
Su
rger
y, N
euro
logy
, Op
hth
alm
olo
gy,
Pae
dia
tric
Clin
ical
Hae
mat
olo
gy, R
heu
mat
olo
gy a
nd
T&
O )
-12
,00
0
-10
,00
0
-8,0
00
-6,0
00
-4,0
00
-2,0
00
0
2,0
00
Cardiology
Clinical Haematology
Dermatology
Diabetic Medicine
Endocrinology
Ent
Gastroenterology
General Surgery
Geriatric Medicine
Gynaecology
Hepatology
Neurology
Ophthalmology
Paediatric Clinical Haematology
Pain Management
Respiratory Medicine
Rheumatology
Trauma & Orthopaedics
Urology
Ou
tpati
en
t A
cti
vit
y,
follo
w u
p a
tten
dan
ce, vari
an
ce 0
9/1
0 t
o 1
0/1
1
-£1
,00
0,0
00
-£8
00
,00
0
-£6
00
,00
0
-£4
00
,00
0
-£2
00
,00
0
£0
£2
00
,00
0
£4
00
,00
0
Cardiology
Clinical Haematology
Dermatology
Diabetic Medicine
Endocrinology
Ent
Gastroenterology
General Surgery
Geriatric Medicine
Gynaecology
Hepatology
Neurology
Ophthalmology
Paediatric Clinical Haematology
Pain Management
Respiratory Medicine
Rheumatology
Trauma & Orthopaedics
Urology
Ou
tpati
en
t C
ost,
fo
llo
w u
p a
tten
dan
ce,
vari
an
ce 0
9/1
0 -
10/1
1

Lambeth Clinical Commissioning Collaborative Board (LCCCB)
All Practice Event
Wednesday 12th October 2011
Group Five – Long Term Conditions
Life expectancy in Lambeth has continued to improve over the last ten years, with mortality rate continually reducing across all causes. However, the gap in life expectancy and largest cause of death in Lambeth continue to be attributable to circulatory diseases, respiratory diseases, digestive diseases and cancer. This workshop will engage participants in identifying what areas of Long Term Conditions should future redesign work focus on, both in terms of stage of pathway and disease progression as well as specific conditions.
Gro
up 5
- L
ong
Ter
m C
ondi
tions


Long Term Conditions Life expectancy in Lambeth has continued to improve over the last ten years, with mortality rate continually reducing across all causes. However, the gap in life expectancy and largest cause of death in Lambeth continue to be attributable to circulatory diseases, respiratory diseases, digestive diseases and cancer. Lambeth has focused on Long Term Conditions as part of it’s core priorities for a number of years, specifically:
Cardiovascular disease (including coronary heart disease, stroke and hypertension)
Diabetes
COPD
Renal disease
Sickle cell anemia
Lambeth has delivered significant progress in terms of development of community heart
failure, respiratory and diabetes services. Collaboration of key stakeholders including
Acute and Primary Care Clinicians has lead to robust redesign of new care pathways
that will deliver a reduction in emergency admissions.
However, on a day to day basis there is still work to be done to help people bring blood
pressure, cholesterol and HbA1C under control, in the face of increasing prevalence of
these key risk factors.
Lambeth’s recent JSNA report highlighted the need to review emphasis and intervention in our provision of services for people with, or at risk of developing long term conditions. This workshop will engage participants in identifying what areas of Long Term Conditions should future redesign work focus on, both in terms of stage of pathway and disease progression as well as specific conditions.
Gro
up 5
- L
ong
Ter
m C
ondi
tions

Group work In the group work we’d like to capture participants’ input in to: High numbers of emergency attendances and admissions are people with one or more
long term condition. Focus to date has been on higher risk patients, should we continue
the focus on the high risk group, or should we revisit programmes of early care pathway
intervention?
What would have the biggest effect that we are not currently doing?
Based on your experience of your patient population what care pathways are not working as well as they could? What would it take to make these pathways good? What value could engaging patients more in this work add? How should we do it to best effect? How do the existing programmes, e.g. DMI, Virtual Hospital, Integrated Care Pilot, PHMCC etc. add value to this work. What can we do to ensure practices get the most out of these programmes?

Firs
t
Spec
Lam
bet
h P
CT
Lon
do
n S
HA
% v
aria
nce
Car
dio
logy
6.5
13.7
7.13
5
Clin
ical
Hae
mat
olo
gy2.
42.
2-0
.224
Der
mat
olo
gy14
.113
.9-0
.341
Dia
bet
ic M
edic
ine
3.3
3-0
.333
End
ocr
ino
logy
21.
9-0
.12
ENT
9.5
13.8
4.20
5
Gas
tro
ente
rolo
gy5.
36.
30.
947
Gen
eral
Su
rger
y5.
711
.25.
443
Ger
iatr
ic M
edic
ine
21.
7-0
.32
Gyn
aeco
logy
16.5
16.6
-0.0
65
Hep
ato
logy
0.8
0.5
-0.3
08
Neu
rolo
gy3.
95.
51.
561
Op
hth
alm
olo
gy18
.617
.9-0
.886
Pae
dia
tric
Clin
ical
Hae
mat
olo
gy2.
10.
3-1
.821
Pai
n M
anag
emen
t0.
71.
70.
993
Reh
eum
ato
logy
4.6
5.6
0.95
4
Res
pir
ato
ry M
edic
ine
2.5
3.3
0.77
5
T&O
1118
6.89
Uro
logy
7.1
80.
829
Foll
ow
-Up
Spec
Lam
bet
h P
CT
Lon
do
n S
HA
% v
aria
nce
Car
dio
logy
1.8
1.3
-0.5
18
Clin
ical
Hae
mat
olo
gy4.
67.
52.
854
Der
mat
olo
gy2.
26.
34.
078
Dia
bet
ic M
edic
ine
0
End
ocr
ino
logy
0
ENT
1.3
1.3
-0.0
13
Gas
tro
ente
rolo
gy1.
92.
00.
081
Gen
eral
Su
rger
y1.
61.
6-0
.016
Ger
iatr
ic M
edic
ine
0
Gyn
aeco
logy
1.0
1.2
0.19
Hep
ato
logy
0
No
te
The
follo
win
g sp
ecia
litie
s h
ave
bee
n e
xclu
ded
fro
m t
he
rep
ort
as d
ata
in N
HS
com
par
ato
rs is
inco
mp
lete
Dia
bet
ic M
edic
ine
End
ocr
ino
logy
Ger
iatr
ic M
edic
ine
Hep
ato
logy
Pae
dia
tric
Clin
ical
Hae
mat
olo
gy
Pai
n M
anag
emen
t0 2 4 6 8 10
12
14
16
18
20
Cardiology
Clinical Haematology
Dermatology
Diabetic Medicine
Endocrinology
ENT
Gastroenterology
General Surgery
Geriatric Medicine
Gynaecology
Hepatology
Neurology
Ophthalmology
Paediatric Clinical …
Pain Management
Reheumatology
Respiratory Medicine
T&O
Urology
Rates Per 1000
Spe
cial
ity
10/1
1 G
P N
ew
Ra
tes
Per
10
00 f
or
Lam
bet
h A
gain
st L
on
do
n P
osi
tio
n
Lam
bet
h P
CT
Lon
do
n S
HA
0
5
10
15
20
25
30
35
40
Cardiology
Clinical Haematology
Dermatology
Diabetic Medicine
Endocrinology
ENT
Gastroenterology
General Surgery
Geriatric Medicine
Gynaecology
Hepatology
Neurology
Ophthalmology
Paediatric Clinical …
Pain Management
Reheumatology
Respiratory Medicine
T&O
Urology
Attendance Ratio
Spec
ialit
y
10/
11 O
utp
atie
nt
Follo
w-u
p T
o F
irst
Att
en
dan
ce R
ati
o
Lam
bet
h P
CT
Lon
do
n S
HA
Gro
up 5
- C
hart
s


Var
ian
ce a
nal
ysis
fo
r Fi
rst
atte
nd
ance
s in
lam
be
th f
or
Top
sp
eci
alit
ies
Sum
mar
y:
• Fo
r Fi
rst
atte
nd
ance
s, o
vera
ll co
st h
as g
on
e u
p b
y 4
77
k b
ut
acti
vity
has
red
uce
d
• A
ctiv
ity
and
co
st h
as r
edu
ced
fo
r: (
Der
mat
olo
gy, E
NT,
Gyn
ae, N
euro
logy
an
d T
&O
)
• Th
ere
is a
dec
reas
e in
co
st b
ut
an in
crea
se in
act
ivit
y in
: (G
eria
tric
Med
an
d P
ain
Mn
gt)
• Th
ere
is a
n in
crea
se in
co
st b
ut
a d
ecre
ase
in a
ctiv
ity
in: (
Clin
ical
Hae
mat
olo
gy, G
astr
o a
nd
Gen
eral
)
* In
tro
du
ctio
n o
f G
PSI
in S
E lo
calit
y an
d b
oro
ugh
wid
e G
P e
du
cati
on
pro
gram
me
has
red
uce
d d
erm
ato
logy
ref
erra
ls.
* T&
O a
ctiv
ity
and
co
st h
ave
red
uce
d d
ue
to M
CA
TTs,
ho
wev
er t
he
09
/10
dat
a in
clu
des
so
me
ph
ysio
ther
apy
act
ivit
y fo
r K
CH
wh
ich
is n
ot
incl
ud
ed in
th
e 1
0/1
1 a
ctiv
ity.
Th
eref
ore
th
e re
du
ctio
n in
act
ivit
y 3
00
att
end
s lo
wer
th
an r
epo
rted
.
* O
pth
alm
olo
gy r
efer
rals
hav
e si
gnif
ican
tly
incr
ease
d.
• A
ctiv
ity
and
co
st h
ave
incr
ease
d f
or:
(C
ard
io, D
iab
Med
, En
do
crin
olo
gy, H
epat
olo
gy, O
ph
thal
mo
logy
,
Pae
dia
tric
Clin
ical
Hae
mat
olo
gy, R
esp
irat
ory
Med
icin
e, R
heu
mat
olo
gy a
nd
Uro
logy
)
-5000
-4000
-3000
-2000
-1000
0
1000
2000
3000
Cardiology
Clinical Haematology
Dermatology
Diabetic Medicine
Endocrinology
Ent
Gastroenterology
General Surgery
Geriatric Medicine
Gynaecology
Hepatology
Neurology
Ophthalmology
Paediatric Clinical Haematology
Pain Management
Respiratory Medicine
Rheumatology
Trauma & Orthopaedics
Urology
Ou
tpa
tie
nt A
cti
vit
y, f
irs
t a
tte
nd
an
ce
, va
ria
nc
e 0
9/1
0 t
o 1
0/1
1
-800000
-600000
-400000
-200000
0
200000
400000
600000
Cardiology
Clinical Haematology
Dermatology
Diabetic Medicine
Endocrinology
Ent
Gastroenterology
General Surgery
Geriatric Medicine
Gynaecology
Hepatology
Neurology
Ophthalmology
Paediatric Clinical Haematology
Pain Management
Respiratory Medicine
Rheumatology
Trauma & Orthopaedics
Urology
Ou
tpati
en
t C
ost,
fir
st
att
en
dan
ce, vari
an
ce 0
9/1
0 -
10/1
1 G
roup
5 -
Cha
rts

Var
ian
ce a
nal
ysis
fo
r fo
llow
up
att
en
dan
ces
in la
mb
eth
fo
r To
p s
pec
ialit
ies
Sum
mar
y:
• Fo
r fo
llow
up
att
end
ance
s, o
vera
ll re
du
ctio
n in
Act
ivit
y an
d C
ost
fo
r A
ll La
mb
eth
To
p S
pec
ialt
ies
• ac
tivi
ty a
nd
co
st h
as r
edu
ced
fo
r: (
ENT,
Gas
tro
, Ger
iatr
ic m
edec
ine
and
Gyn
ae)
• th
ere
is a
dec
reas
e in
co
st b
ut
an in
crea
se in
act
ivit
y in
: (D
erm
ato
logy
, Hep
ato
logy
an
d U
rolo
gy)
• th
ere
is a
n in
crea
se in
co
st b
ut
a d
ecre
ase
in a
ctiv
ity
in: (
Pai
n M
ngt
an
d R
esp
irat
ory
Med
)
* T&
O a
ctiv
ity
follo
w u
p a
ctiv
ity
and
co
st h
ave
red
uce
d d
ue
to M
CA
TTs,
ho
we
ver
the
09
/10
dat
a in
clu
des
so
me
ph
ysio
ther
apy
ac
tivi
ty f
or
KC
H w
hic
h is
no
t in
clu
ded
in t
he
10
/11
act
ivit
y. T
her
efo
re t
he
red
uct
ion
in a
ctiv
ity
900
att
end
s lo
we
r th
an r
epo
rted
.
• ac
tivi
ty a
nd
co
st a
nd
incr
ease
d f
or:
(C
ard
io, C
linic
al H
aem
ato
logy
, Gen
eral
Su
rger
y, N
euro
logy
, Op
hth
alm
olo
gy,
Pae
dia
tric
Clin
ical
Hae
mat
olo
gy, R
heu
mat
olo
gy a
nd
T&
O )
-12
,00
0
-10
,00
0
-8,0
00
-6,0
00
-4,0
00
-2,0
00
0
2,0
00
Cardiology
Clinical Haematology
Dermatology
Diabetic Medicine
Endocrinology
Ent
Gastroenterology
General Surgery
Geriatric Medicine
Gynaecology
Hepatology
Neurology
Ophthalmology
Paediatric Clinical Haematology
Pain Management
Respiratory Medicine
Rheumatology
Trauma & Orthopaedics
Urology
Ou
tpati
en
t A
cti
vit
y,
follo
w u
p a
tten
dan
ce, vari
an
ce 0
9/1
0 t
o 1
0/1
1
-£1
,00
0,0
00
-£8
00
,00
0
-£6
00
,00
0
-£4
00
,00
0
-£2
00
,00
0
£0
£2
00
,00
0
£4
00
,00
0
Cardiology
Clinical Haematology
Dermatology
Diabetic Medicine
Endocrinology
Ent
Gastroenterology
General Surgery
Geriatric Medicine
Gynaecology
Hepatology
Neurology
Ophthalmology
Paediatric Clinical Haematology
Pain Management
Respiratory Medicine
Rheumatology
Trauma & Orthopaedics
Urology
Ou
tpati
en
t C
ost,
fo
llo
w u
p a
tten
dan
ce,
vari
an
ce 0
9/1
0 -
10/1
1

Lambeth Clinical Commissioning Collaborative Board (LCCCB)
All Practice Event
Wednesday 12th October 2011
Group Six – Mental Health –
Integrated Primary Care
Talking Therapies
Competitive tender now for a service offering a single point of access and self referral for all talking therapies, including counselling and IAPT, in primary care in Lambeth. Consultation event on 1st November 12.30 - 3.00. The purpose of this workshop is to identify outcomes an integrated Lambeth wide talking therapy service should deliver, considering key aspects such as a single point of access, employment support activities and learning from the past.
Gro
up 6
- M
enta
l Hea
lth, T
alki
ngT
hera
pies


6th October 2011 Dear Stakeholder,
Consultation Paper: A proposed service specification for an integrated talking therapy service in Lambeth
You are invited to be involved in a consultation on an integrated primary care talking therapy service in Lambeth. Please find attached a consultation paper giving the background, purpose and time frames of this consultation. The consultation paper and timeframe was approved by the Lambeth Talking Therapy Board in September 2011. The purpose of the consultation exercise is to provide a period of community engagement in order to enable further development of the ideas and proposals for the service. Included in the attached consultation paper is a table of questions to which the Board would be grateful for your responses. There is also space to include comments on areas that you consider have not been addressed elsewhere. The questions have been attached as an optional framework for response. Please send your responses to Joiss Soumahoro at:
Tel: 0207 049 4381
NHS Lambeth, 1 Lower Marsh, London, SE1 7NT Alternatively, you are welcome to use your own written response format or, if you prefer to provide your comments via telephone or email, please contact Joiss. I should be most grateful if you would let me have any comments you wish to make by 11/11/2011 at the latest. The consultation document is being widely distributed, and members of the Board will be pleased to make every effort to attend any Provider/Commissioning network to discuss and debate further if requested. A workshop is also taking place on 1st November, 12.30 to 3.00 to allow for face to face discussion and input into this piece of work. To register a place at the event, contact Joiss on the contact details above. All responses will be collated and reported to the Talking Therapy Board in November. You may respond individually, as an organisation, and as part of a provider network or other stakeholder forum. The intention is to finalise the service specification and include it in an Invitation to Tender Pack which will be released on 21/11/2011. The new service will be in place from 1st August 2011.
Gro
up 6
- M
enta
l Hea
lth, T
alki
ngT
hera
pies

Please do contact me via NHS Lambeth if you require any clarification on the content of the consultation document. I do hope you can find the time to respond. Yours sincerely, Dr Mark Smith, Talking Therapy Board Chair

This is a summary of documentation out for consultation on the integrated primary care talking therapies service.
EXECUTIVE SUMMARY
1.1 As a result of the various drivers (4.1 below) influencing the future of
primary care talking therapy services in the London Borough of Lambeth, the Talking Therapy Board has reviewed current provision. The outcome of the review has concluded that the service should be developed and enhanced. It is proposed this could be realised by reconfiguring the services into one integrated service, with a single point of entry into talking therapy provision. Under the proposals, people referred into the service will be assessed and directed to the most appropriate service to meet their needs. The purpose of any talking therapy service intervention arranged and the outcomes that the service will aim to achieve will be explicit and agreed with the service user.
1.2 In future, one integrated talking therapy service will work more
collaboratively with other mental health and social care services, as well as relevant community based services, to aid people’s recovery and the maintenance of their physical and psychological health; to help them to retain and to return to employment, and to remove dependency on welfare benefits; and to aid optimum social functioning.
1.3 The consultation paper describes the approach that the Talking Therapy
Board is proposing to take in order to introduce the changes. The Board is seeking views and comments from stakeholders as widely as possible. Attached to this paper is a questionnaire, which people may wish to use to submit their comments. Alternatively the Board will be pleased to receive views in whatever format stakeholders prefer.
Gro
up 6
- M
enta
l Hea
lth, T
alki
ngT
hera
pies


Lambeth Clinical Commissioning Collaborative Board (LCCCB)
All Practice Event
Wednesday 12th October 2011
Group Seven – Mental Health – Lambeth Living
Well Collaborative
Developing an asset based approach to mental health through collaboration. A philosophy of easy in and easy out of services is part of the Lambeth Living Well developments. The purpose of this workshop is to further explore this aspect of easy in/easy out and the role of the newly formed Primary Care Mental Health Support Service.
Gro
up 7
- M
enta
l Hea
lth, L
ivin
g W
ell
Col
labo
rativ
e


Our future in practice
People who use services, carers, front-line staff, care coordinators,
clinicians, GPs, service commissioners and service managers
making it real & delivering change together
Wednesday 19th October at The Oval
1. Morning session: 9.30am -12.30pm Lunch social: 12.30pm -1.30pm2. Afternoon session: 1.30pm -3.30pm
Bringing people from North Lambeth together for a hands-on session to experience, connect, build and plan for the future of mental health services in Lambeth.
Hosted by the
Lambeth Living Well Collaborative
Gro
up 7
- M
enta
l Hea
lth, L
ivin
g W
ell
Col
labo
rativ
e

For the past year, the Lambeth Living Well Collaborative have been hosting events and sessions to bring people to work together in a new way. We believe that in order to make real change happen, we need to co-design our services with the people who will use them and do all we can to enable people to flourish, contribute to society and lead the life they want to lead.
Our last event was in July and brought together over 100 participants - from people who use services to GPs - for two days of rolling-up sleeves and thinking about and planning how support needs to change.
Visit lambethlivingwell.wordpress.com to read about what happend
About the sessionExperience some of the new services being developed through interactive sessions where you can give us your suggestions and feedback
Connect with people from across North Lambeth. Listen to and share your experiences, opinions and ideas through practical sessions
Build new services for the future of Lambeth with us through hands-on sessions
Plan how we will work together to deliver this radical transformation
Book a place and more informationIf you would like to book a place for this free event please reply to Natalie Sutherland
020 3049 4268 [email protected]
Who are the Lambeth Living Well Collaborative?We are a group of service users, carers, GPs, public service
commissioners and providers from the public and third sector. We are dedicated to working together to tackle the big
challenges we all face and to radically improve wellbeing by enabling people to better recover, choose and participate.
WhereWhenIndia RoomThe OvalKenningtonSE11 5SS
Choose a session:1. Morning session: 9.30am -12.30pm Lunch social: 12.30pm -1.30pm 2. Afternoon session: 1.30pm -3.30pm
Oval station 36, 185, 436

Lambeth Clinical Commissioning Collaborative Board (LCCCB)
All Practice Event
Wednesday 12th October 2011
Group Eight – Community
Services
Community health services for Lambeth and Southwark is now provided by Guy’s and St Thomas’ Foundation trust Community Health Services. There is a 3 year contract (with the option to extend for a further 2 years) running from 1st April 2011 to 31st March 2014. As part of the new contract negotiations all service specifications were reviewed and new CQUIN targets were set. Please join us to discuss how we can work together to review annual CQUINs and key areas of development in the Community contract for 2012/13.
Gro
up 8
- C
omm
unity
Ser
vice
s


1
Community Health Services In Lambeth Community health services for Lambeth and Southwark is now provided by Guy’s and St Thomas’ Foundation trust Community Health Services. There is a 3 year contract (with the option to extend for a further 2 years) running from 1st April 2011 to 31st March 2014. The annual contract value for the contract is over £83 million per annum providing a range of generic and specialist services across Lambeth, Southwark, Lewisham and Wandsworth. As part of the new contract negotiations all service specifications were reviewed and new CQUIN targets were set. These are:-
CQUIN Indicator
1. Pressure Ulcers: Productive community services metric
1-A. Reduction in grade 2 and 3 pressure ulcers
1-B. No grade 4 pressure ulcers
2. Falls: Productive community services metric
2-A. Update the Lambeth and Southwark falls pathway
2-B. Reduction in the number of falls resulting in fracture
3. End of Life Care 3-A. EOLC planning discussions
3-B. Gold patient register
3-C. Advanced care plans
3-D. Liverpool care pathway
4. To Encourage Effective Communication between Community and Primary Care.
4-A. Confirming electronic referral receipt
4-B Part A DN caseloads list for GP practices
4-B Part B Care plans shared with the GP practices
4-B Part C DN discharge summaries sent to GP practices
4-C. Monthly HV and GP meetings
5. Children's Immunisations 5-A.Increase the proportion of 1st DTaP/IPV/Hib immunisations
5-B.ncrease the proportion of Hib/Men C immunizations
5-C.Increase the proportion of PCV immunizations
5-D.Increase the proportion of 1st MMR immunisations
5-E. Increase the proportion of 2nd MMR immunisations
5-F. Increase the proportion of DTaP/IPV or dTaP/IPV immunisations
6. To improve the responsiveness to personal needs of patients receiving community based and community based hospital healthcare
6-A. Patient questionnaire response, Involvement in decisions
6-B. Patient questionnaire response, time for discussion
6-C. Patient questionnaire response, information provided
6-D. Patient questionnaire response, confidence in health professional
6-E. Patient questionnaire response, overall experience
Gro
up 8
- C
omm
unity
Ser
vice
s

2
Areas of work that we want to review in 2012/13 include:-
District nurses & community matrons
Health visitors
Diabetes (Southwark only)
Stop smoking (Southwark only)
Sexual health
Intermediate care
School Nurses
Early interventions (Lambeth only)
Breastfeeding (Lambeth only)
Child Immunisations
Admissions Avoidance Schemes
Use of Telemedicine
How can we work together on this?
Involvement from primary care on the contract monitoring – this can be done via the LCCCB lead Ruth Jeffrey
Reviewing the impact on 2011/12 CQUIN measures especially CQUIN measure 4 on communications
Input into service reviews and setting CQUIN target for 2012/13 Lead commissioners
Name Position Contact
Moira McGrath Director of Care Pathways [email protected]
Therese Fletcher
Assistant Director of Primary and Community Care
Mahroof Kazi Commissioning Manager of Primary and Community Care
Ruth Jeffrey LCCCB lead for community contract