ahrq annual meeting 2009: "research to reform: achieving health system change" september...
TRANSCRIPT

RATING THE EVIDENCE: USING GRADE TO DEVELOP CLINICAL PRACTICE GUIDELINES
AHRQ Annual Meeting 2009:"Research to Reform: Achieving Health System Change"
September 14, 2009
Yngve Falck-Ytter, M.D.Case Western Reserve University, Cleveland, Ohio
Holger Schünemann, M.D., Ph.D. Chair, Department of Clinical Epidemiology & Biostatistics
Michael Gent Chair in Healthcare ResearchMcMaster University, Hamilton, Canada

Disclosure
In the past 5 years, Dr. Falck-Ytter received no
personal payments for services from industry. His
research group received research grants from
Three Rivers, Valeant and Roche that were
deposited into non-profit research accounts. He is a
member of the GRADE working group which has
received funding from various governmental
entities in the US and Europe. Some of the GRADE
work he has done is supported in part by grant # 1
R13 HS016880-01 from the Agency for Healthcare
Research and Quality (AHRQ).

Content
Part 1 IntroductionPart 2 Why revisiting guideline
methodology?Part 3 The GRADE approach
Quality of evidence
Part 4 The GRADE approach
Strength of recommendations

Q to audience
Involved in giving recommendations? Using any form of grading system?
Familiarity with GRADE: Heard about GRADE before this
conference? Read a GRADE article published by the
GRADE working group? Attended a GRADE presentation? Attended a hands-on GRADE workshop?
Reassessment of clinical practice guidelines
Editorial by Shaneyfelt and Centor (JAMA 2009) “Too many current guidelines have
become marketing and opinion-based pieces…”
“AHA CPG: 48% of recommendations are based on level C = expert opinion…”
“…clinicians do not use CPG […] greater concern […] some CPG are turned into performance measures…”
“Time has come for CPG development to again be centralized, e.g., AHQR…”

Evidence-based clinical decisions
Research evidence
Patient values and preferences
Clinical state and circumstances
Expertise
Equal for allHaynes et al. 2002

Oxford Centre of Evidence Based Medicine; http://www.cebm.net 7
Before GRADE
Level of evidence
I
II
III
IV
V
Source of evidence
SR, RCTs
Cohort studies
Case-control studies
Case series
Expert opinion
A
Grades of recomend.
B
C
D
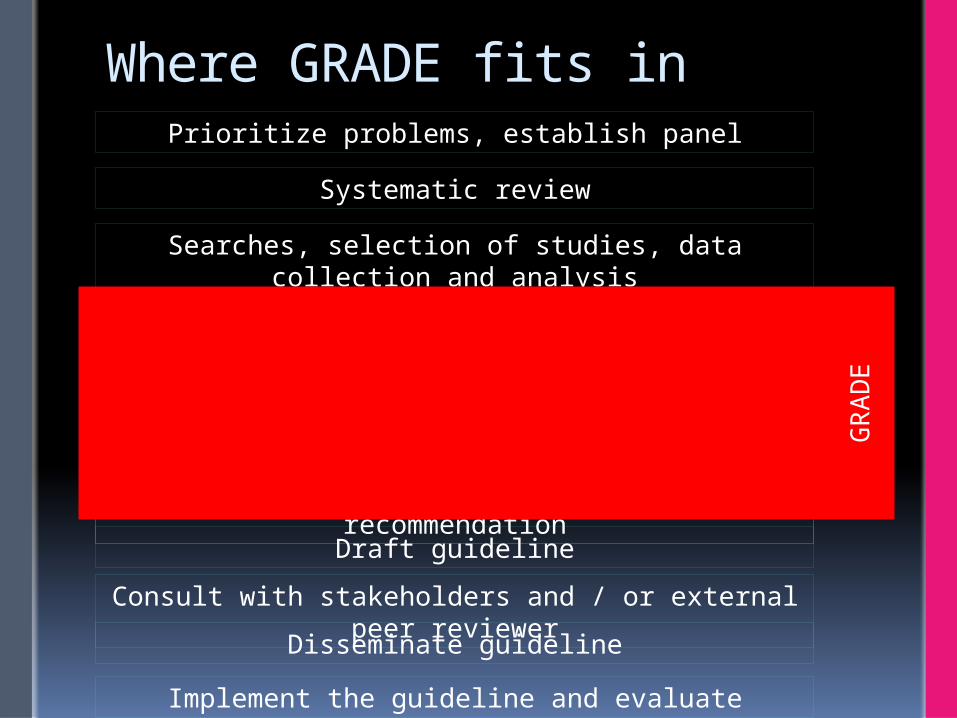
Where GRADE fits inPrioritize problems, establish panel
Systematic review
Searches, selection of studies, data collection and analysis
Assess the relative importance of outcomes
Prepare evidence profile: Quality of evidence for each outcome and summary
of findingsAssess overall quality of evidence
Decide direction and strength of recommendation
Draft guideline
Consult with stakeholders and / or external peer reviewer
Disseminate guideline
Implement the guideline and evaluate
GR
AD
E

GRADE uptake

GRADE – WHY REVISITING GUIDELINE METHODOLOGY?
10

Disclosure
Dr. Schünemann receives no personal payments for service from the pharmaceutical industry. The research group he belongs to received research grants from the industry that are deposited into research accounts. Institutions or organizations that he is affiliated with likely receive funding from for-profit sponsors that are supporting infrastructure and research that may serve his work. He is documents editor for the American Thoracic Society and co-chair of the GRADE Working Group.
Content
Why grading Confidence in information and
recommendationsIntro to: Quality of evidence Strength of recommendations

Please discuss the difference between consensus statements and guidelines?
Be prepared to discuss your answer
13
There are no RCTs! Do you think that users of
recommendations would like to be informed about the basis (explanation) for a recommendation or coverage decision if they were asked (by their patients)?
I suspect the answer is “yes” If we need to provide the basis for
recommendations, we need to say whether the evidence is good or not so good; in other words perhaps “no RCTs” 14

Hierarchy of evidence
STUDY DESIGN Randomized Controlled
Trials Cohort Studies and
Case Control Studies Case Reports and Case
Series, Non-systematic observations
BIAS
Expert Opinion

Confidence in evidence
There always is evidence “When there is a question there is
evidence” Better research greater confidence in
the evidence and decisions
Who can explain the following? Concealment of randomization Bias, confounding and effect
modification Blinding (who is blinded in a double
blinded trial?) Intention to treat analysis and its correct
application Why trials stopped early for benefit
overestimate treatment effects? P-values and confidence intervals

Hierarchy of evidence
STUDY DESIGN Randomized Controlled
Trials Cohort Studies and
Case Control Studies Case Reports and Case
Series, Non-systematic observations
BIAS
Expert Opinion
Exp
ert O
pin
ion
Expert Opinion

Reasons for grading evidence?
Appraisal of evidence has become complex and daunting
People draw conclusions about the quality of evidence and strength of
recommendations
Systematic and explicit approaches can help protect against errors, resolve disagreements communicate information and fulfil needs
Change practitioner behavior However, wide variation in approaches
GRADE working group. BMJ. 2004 & 2008
Which grading system?
Evidence Recommendation B Class I A 1 IV C
Organization AHA ACCP SIGN
Recommendation for use of oral anticoagulation in patients with atrial fibrillation and rheumatic mitral valve disease

What to do?

22
Recommendations vs statements!
Limitations of older systems & approaches
confuse quality of evidence with strength of recommendations

Levels of evidence

Recommendations
Limitations of older systems & approaches
confuse quality of evidence with strength of recommendations
lack well-articulated conceptual framework
criteria not comprehensive or transparent focus on single outcomes

GRADE Quality of Evidence
In the context of a systematic review The quality of evidence reflects the
extent to which we are confident that an estimate of effect is correct.
In the context of making recommendations The quality of evidence reflects the
extent to which our confidence in an estimate of the effect is adequate to support a particular recommendation.

What makes you confident in health care decisions
28
Confident in the evidence?A meta-analysis of observational studies showed that bicycle helmets reduce the risk of head injuries in cyclists. OR: 0.31, 95%CI: 0.26 to 0.37
A meta-analysis of observational studies showed that warfarin prophylaxis reduces the risk of thromboembolism in patients with cardiac valve replacement. RR: 0.17, 95%CI: 0.13 to 0.24
29

30
31
GRADE: Quality of evidenceThe extent to which our confidence in an estimate of the treatment effect is adequate to support a particular recommendation.
GRADE defines 4 categories of quality: High Moderate Low Very low

I B II V III
Quality of evidence across studies
Outcome #1Outcome #2Outcome #3
Quality: HighQuality: ModerateQuality: Low

Determinants of quality
RCTs start high
Observational studies start low
34
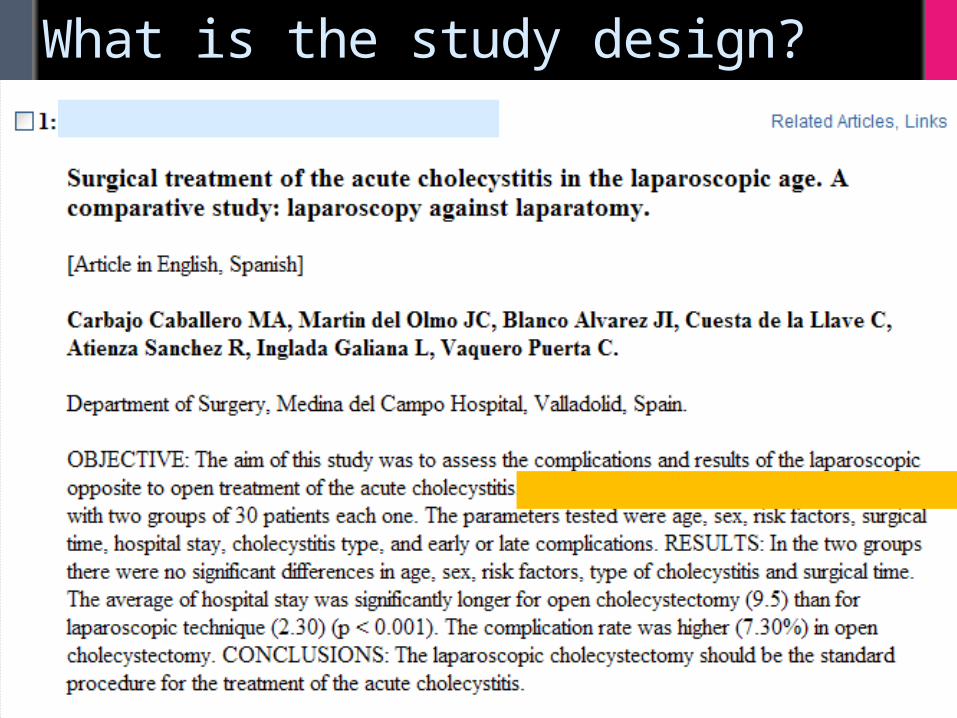
What is the study design?

Determinants of quality
What lowers quality of evidence? 5 factors:
Methodological limitations
Inconsistency of results
Indirectness
of evidence
Imprecision of results
Publication bias

Assessment of detailed design and execution (risk of bias)For RCTs: Lack of allocation concealment No true intention to treat principle Inadequate blinding Loss to follow-up Early stopping for benefit
Methodological limitations
Inconsistency of results
Indirectness
of evidence
Imprecision of results
Publication bias

Schulz KF et al. JAMA 1995 37
Allocation concealment
250 RCTs out of 33 meta-analysesAllocation concealment:Effect
(Ratio of OR)
adequate 1.00 (Ref.)unclear 0.67 [0.60
– 0.75]not adequate 0.59
[0.48 – 0.73]
*
* significant
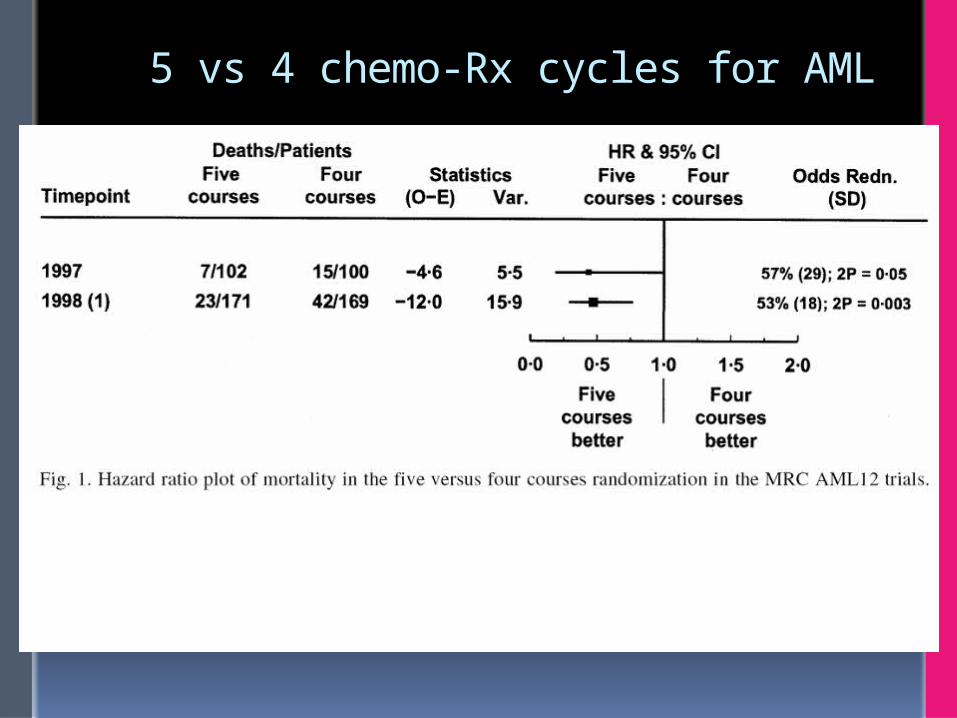
5 vs 4 chemo-Rx cycles for AML

Studies stopped early becasue of benefit

Jadad AR et al. Control Clin Trials 1996 40
What about scoring tools?
Example: Jadad score
Was the study described as randomized?1
Adequate description of randomization? 1Double blind? 1
Method of double blinding described? 1Description of withdrawals and dropouts?
1
Max 5 points for quality
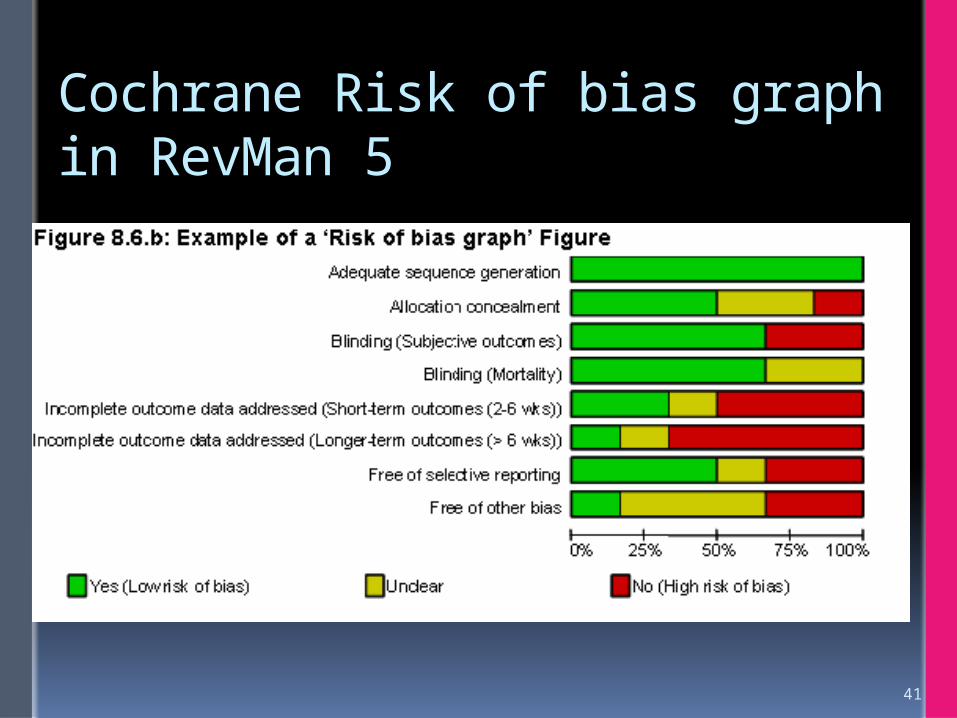
Cochrane Risk of bias graph in RevMan 5
41

Look for explanation for inconsistency patients, intervention, comparator, outcome,
methods
Judgment variation in size of effect overlap in confidence intervals statistical significance of heterogeneity I2
Methodological limitations
Inconsistency of results
Indirectness
of evidence
Imprecision of results
Publication bias

43
HeterogeneityNeurological or vascular complications or death within 30 days of endovascular treatment (stent, balloon angioplasty) vs. surgical carotid endarterectomy (CEA)
Indirect comparisons Interested in head-to-head comparison Drug A versus drug B Tenofovir versus entecavir in hepatitis B
treatment
Differences in patients (early cirrhosis vs end-stage cirrhosis) interventions (CRC screening: flex. sig. vs
colonoscopy) comparator (e.g., differences in dose) outcomes (non-steroidal safety: ulcer on
endoscopy vs symptomatic ulcer complications)
Methodological limitations
Inconsistency of results
Indirectness
of evidence
Imprecision of results
Publication bias

Small sample size small number of events wide confidence intervals uncertainty about magnitude of effect
Methodological limitations
Inconsistency of results
Indirectness
of evidence
Imprecision of results
Publication bias
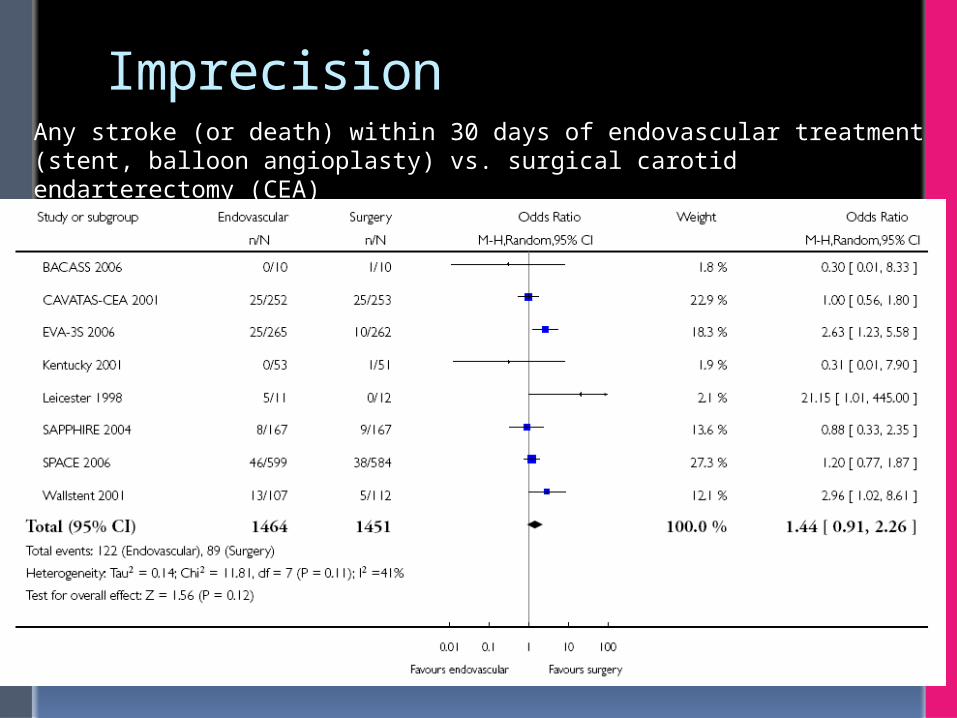
ImprecisionAny stroke (or death) within 30 days of endovascular treatment (stent, balloon angioplasty) vs. surgical carotid endarterectomy (CEA)

Reporting of studies publication bias
number of small studies
Methodological limitations
Inconsistency of results
Indirectness
of evidence
Imprecision of results
Publication bias

All phase II and III licensing trial for antidepressant drugs between 1987 and 2004 (74 trials – 23 were not published)
49
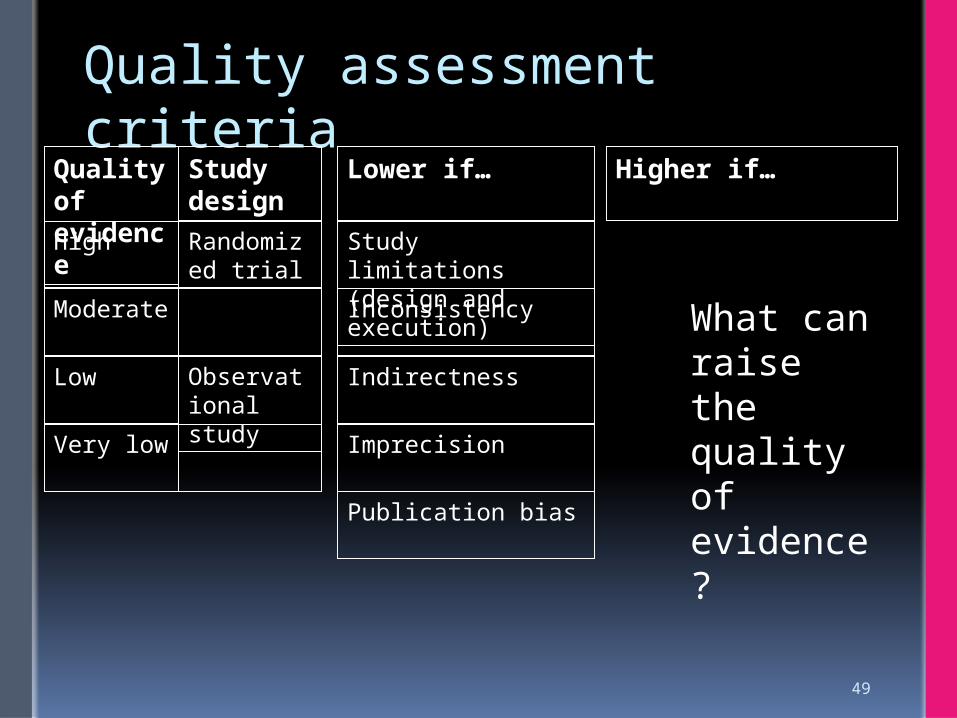
Quality assessment criteria
Lower if…Quality of evidence
High
Moderate
Low
Very low
Study limitations(design and execution)
Inconsistency
Indirectness
Imprecision
Publication bias
Observational study
Study design
Randomized trial
Higher if…
What can raise the quality of evidence?
50

51
Quality assessment criteria
Lower if… Higher if…Quality of evidence
High
Moderate
Low
Very low
Study design
Randomized trial
Observational study
Study limitations
Inconsistency
Indirectness
Imprecision
Publication bias
Large effect (e.g., RR 0.5)Very large effect (e.g., RR 0.2)
Evidence of dose-response gradient
All plausible confounding would reduce a demonstrated effect

52
Conceptualizing quality
Further research is very unlikely to change our confidence in the estimate of effectHigh
LowFurther research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate
ModerateFurther research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate
Very low Any estimate of effect is very uncertain
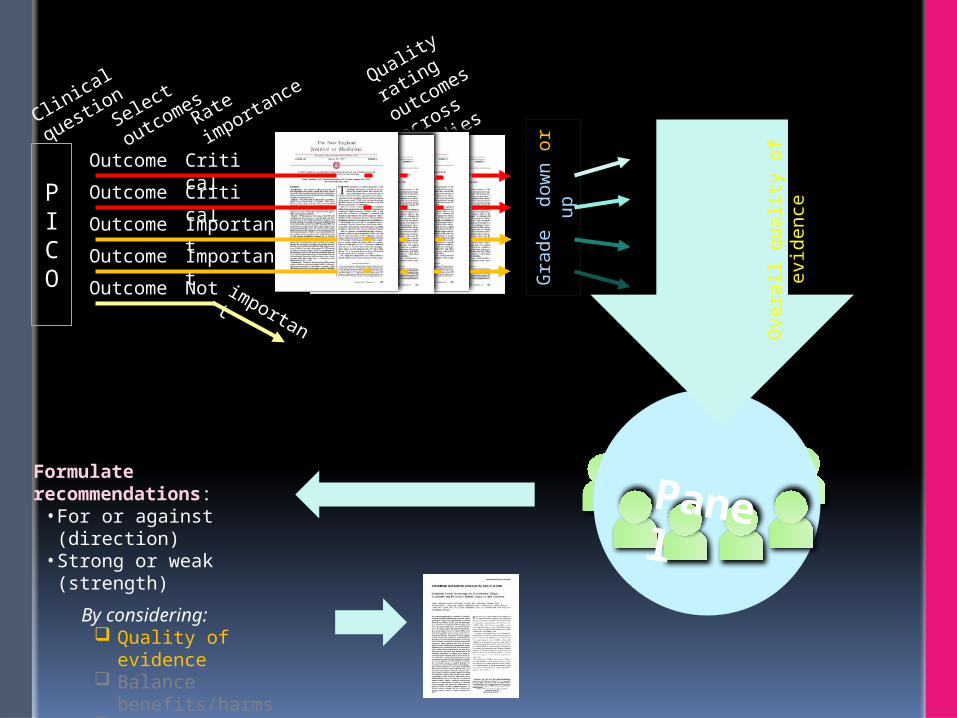
PICO
Clinica
l questi
on
Rate
importa
nce
Panel
Select
outcomes
Very low
Low
Modera
te
High
Formulate recommendations:
• For or against (direction)• Strong or weak (strength)
By considering: Quality of evidence Balance
benefits/harms Values and
preferences
Revise if necessary by considering:
Resource use (cost)
Quality
rating
outcomes
across
studies
OutcomeOutcomeOutcome
Outcome
Critical
Important
Critical
Not important
Gra
de
dow
n o
r up
Outcome
Important
Overa
ll q
ualit
y o
f evid
ence

GRADE evidence profile
GRADE - FROM EVIDENCE TO DECISONS
55

Strength of recommendations
Desirable effects• health benefits• less burden• savings
Undesirable effects• harms• more burden• costs

Developing recommendations
Strength of recommendation
“The strength of a recommendation reflects the extent to which we can, across the range of patients for whom the recommendations are intended, be confident that desirable effects of a management strategy outweigh undesirable effects.”
Strong or weak/conditional

Quality of evidence & strength of recommendation GRADE separates quality of evidence
from strength of recommendation Linked but no automatism Other factors beyond the quality of
evidence influence our confidence that adherence to a recommendation causes more benefit than harm
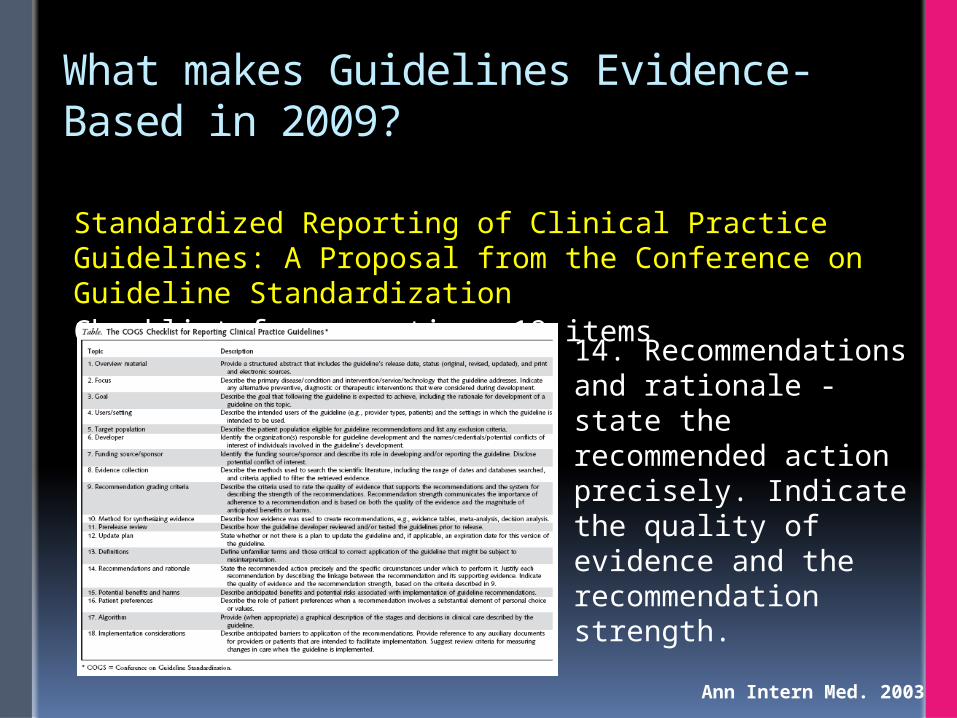
What makes Guidelines Evidence-Based in 2009?
Standardized Reporting of Clinical Practice Guidelines: A Proposal from the Conference on Guideline StandardizationChecklist for reporting: 18 items
Ann Intern Med. 2003
14. Recommendations and rationale - state the recommended action precisely. Indicate the quality of evidence and the recommendation strength.

What makes Guidelines Evidence-Based in 2009?
Standardized Reporting of Clinical Practice Guidelines: A Proposal from the Conference on Guideline StandardizationChecklist for reporting: 18 items
Ann Intern Med. 2003
16. Patient preferences - describe the role of patient preferences when a recommendation involves a substantial element of personal choice or values.

A COPD guideline – do you want your review used like this?

Another COPD guideline

And another COPD guideline

What to do?

Current state of recommendations
66

Current state of recommendations
Reviewed 7527 recommendations 1275 randomly selected
Inconsistency across/within 31.6% did not recommendations
clearly Most of them not written as executable
actions 52.7% did not indicated strength
67

Yale Guideline Corpus
1. Identify the critical recommendations in guideline text using semantic indicators
2. Use consistent semantic and formatting indicators throughout the publication
3. Group recommendations together in a summary section
4. Do not use assertions of fact as recommendations.
5. Clearly and consistently assign evidence quality and recommendation strength in proximity distinguish between the distinct concepts of
quality of evidence and strength of recommendation.
68
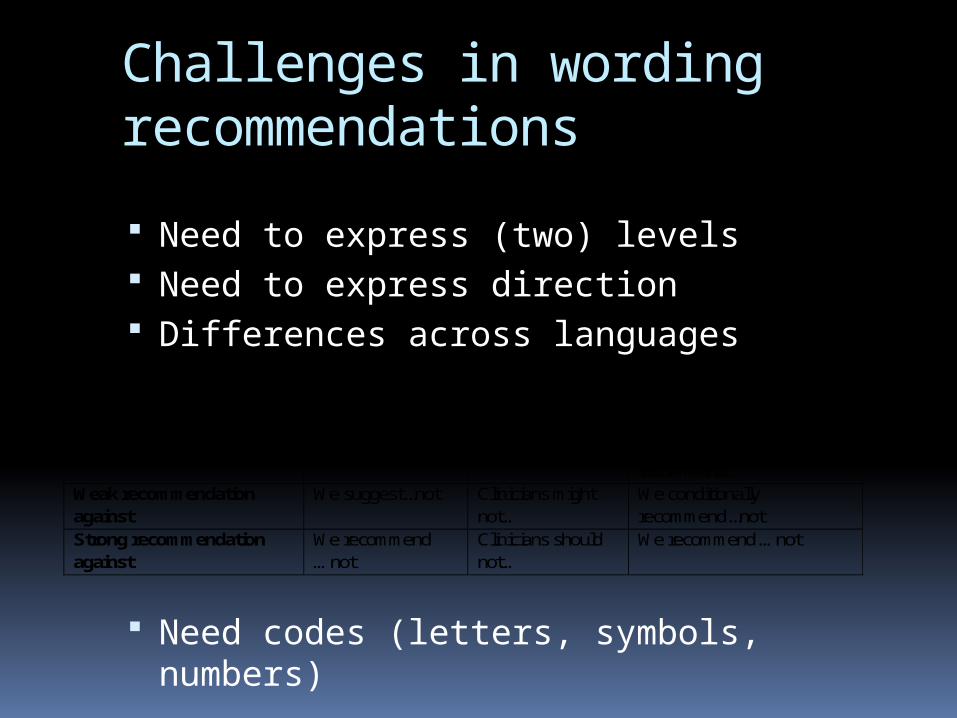
Challenges in wording recommendations
Need to express (two) levels Need to express direction Differences across languages
Need codes (letters, symbols, numbers)
Wording 1 Wording 2 Wording 3 Strong recommendation for We recommend… Clinicians should… We recommend…
Weak recommendation for We suggest Clinicians might… We conditionally
recommend… Weak recommendation against
We suggest...not Clinicians might not…
We conditionally recommend...not
Strong recommendation against
We recommend …not
Clinicians should not…
We recommend …not

70
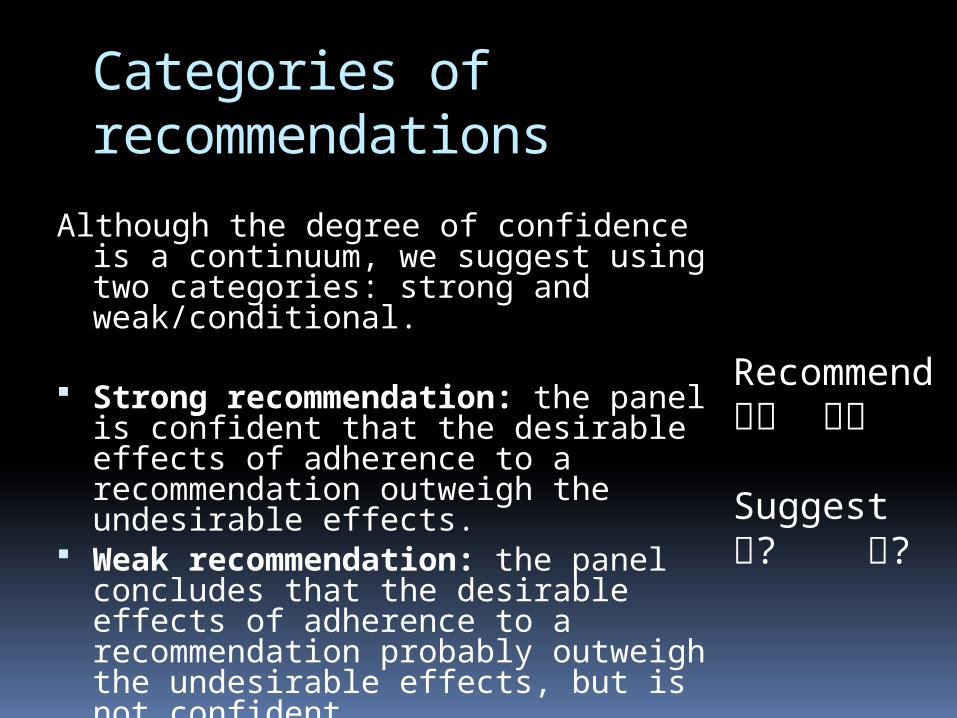
Categories of recommendations
Although the degree of confidence is a continuum, we suggest using two categories: strong and weak/conditional.
Strong recommendation: the panel is confident that the desirable effects of adherence to a recommendation outweigh the undesirable effects.
Weak recommendation: the panel concludes that the desirable effects of adherence to a recommendation probably outweigh the undesirable effects, but is not confident.
Recommend
Suggest? ?
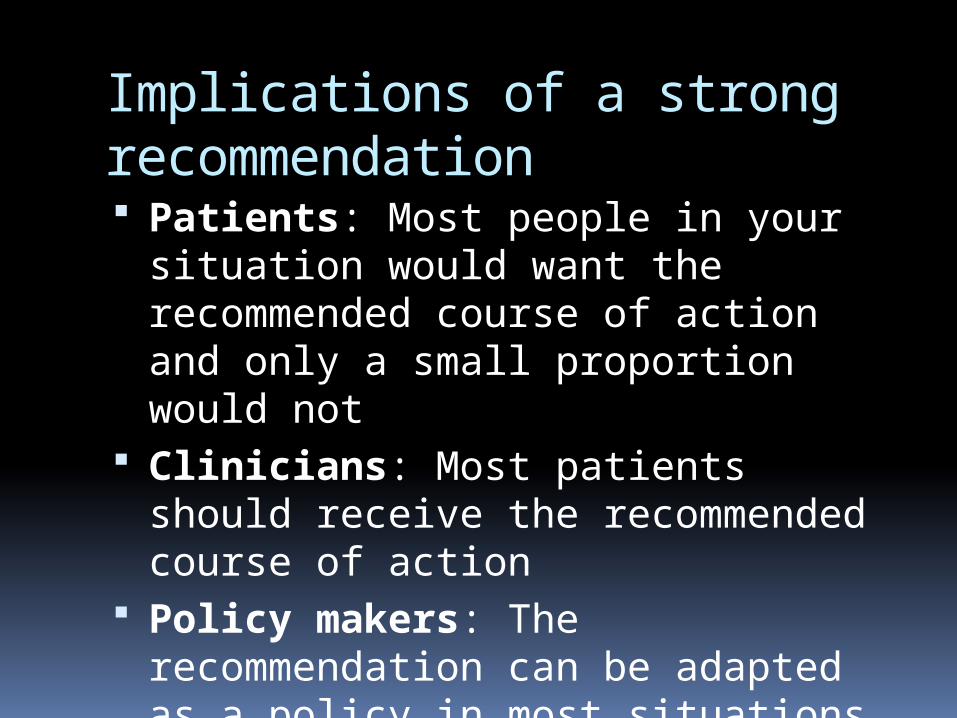
Implications of a strong recommendation Patients: Most people in your
situation would want the recommended course of action and only a small proportion would not
Clinicians: Most patients should receive the recommended course of action
Policy makers: The recommendation can be adapted as a policy in most situations

Implications of a weak/conditional recommendation Patients: The majority of people in
your situation would want the recommended course of action, but many would not
Clinicians: Be prepared to help patients to make a decision that is consistent with their own values
Policy makers: There is a need for substantial debate and involvement of stakeholders
Case scenario
A 13 year old girl who lives in rural Indonesia presented with flu symptoms and developed severe respiratory distress over the course of the last 2 days. She required intubation. The history reveals that she shares her living quarters with her parents and her three siblings. At night the family’s chicken stock shares this room too and several chicken had died unexpectedly a few days before the girl fell sick.
Interventions: antivirals, such as neuraminidase inhibitors oseltamivir and zanamivir

Relevant healthcare question?Clinical question:
Population: Avian Flu/influenza A (H5N1) patients
Intervention: Oseltamivir (or Zanamivir)
Comparison: No pharmacological intervention
Outcomes: Mortality, hospitalizations, resource use, adverse
outcomes, antimicrobial resistanceWHO Avian Influenza GL. Schunemann et al., The Lancet ID, 2007

How would you make decisions?
76

Judgements about the strength of a recommendation No precise threshold for going from a strong to a
weak recommendation The presence of important concerns about one or
more of these factors make a weak recommendation more likely.
Panels should consider all of these factors and make the reasons for their judgements explicit.
Recommendations should specify the perspective that is taken (e.g. individual patient, health system) and which outcomes were considered (including which, if any costs).

Evidence Profile
No of studies(Ref)
Design Limitations Consistency DirectnessOther
considerationsOseltamivir Placebo
Relative(95% CI )
Absolute(95% CI )
Mortality
0 - - - - - - - - - 9
5(TJ 06)
Randomised trial
No limitations One trial only Major uncertainty
(-2)1
Imprecise or sparse data (-1)
- - OR 0.22(0.02 to 2.16)
- Very low
6
0 - - - - - - - - - - 7
5(TJ 06)
Randomised trial
No limitations One trial only Major uncertainty
(-2)1
Imprecise or
sparse data (-1)2
2/982(0.2%)
9/662(1.4%)
RR 0.149(0.03 to 0.69)
- Very low
8
53
(TJ 06)(DT 03)
Randomised trials
No limitations4 Important inconsistency
(-1)5
Major uncertainty
(-2)1
- - - HR 1.303
(1.13 to 1.50)
- Very low
5
26
(TJ 06)
Randomised trials
No limitations -7 Major uncertainty
(-2)1
None - - - WMD -0.738
(-0.99 to -0.47)
Low
4
0 - - - - - - - - - - 4
0 - - - - - - - - - - 7
09 - - - - - - - - - - 7
311
(TJ 06)
Randomised trials
No limitations -12 Some uncertainty
(-1)13
Imprecise or
sparse data (-1)14
- - OR range15
(0.56 to 1.80)
- Low
0 - - - - - - - - - - 4
I mportance
Summary of findings
Cost of drugs
Outbreak control
Resistance
Serious adverse effects (Mention of significant or serious adverse effects)
Minor adverse effects 10 (number and seriousness of adverse effects)
Viral shedding (Mean nasal titre of excreted virus at 24h)
Duration of disease (Time to alleviation of symptoms/median time to resolution of symptoms – influenza cases only)
Duration of hospitalization
LRTI (Pneumonia - influenza cases only)
Healthy adults:
Hospitalisation (Hospitalisations from influenza – influenza cases only)
Quality assessmentNo of patients Effect
Quality
Oseltamivir for treatment of H5N1 infection:
-
-

Oseltamivir for Girl with Avian FluSummary of findings: No clinical trial of oseltamivir for treatment
of H5N1 patients. 4 systematic reviews and health technology
assessments (HTA) reporting on 5 studies of oseltamivir in seasonal influenza. Hospitalization: OR 0.22 (0.02 – 2.16) Pneumonia: OR 0.15 (0.03 - 0.69)
3 published case series. Many in vitro and animal studies. No alternative that is more promising at
present. Cost: ~ $45 per treatment course
What are the factors that determine your decisions?
80

GRADE: Factors influencing decisions and recommendations
Quality of Evidence Balance of desirable and undesirable
consequences Values and preferences Cost
81
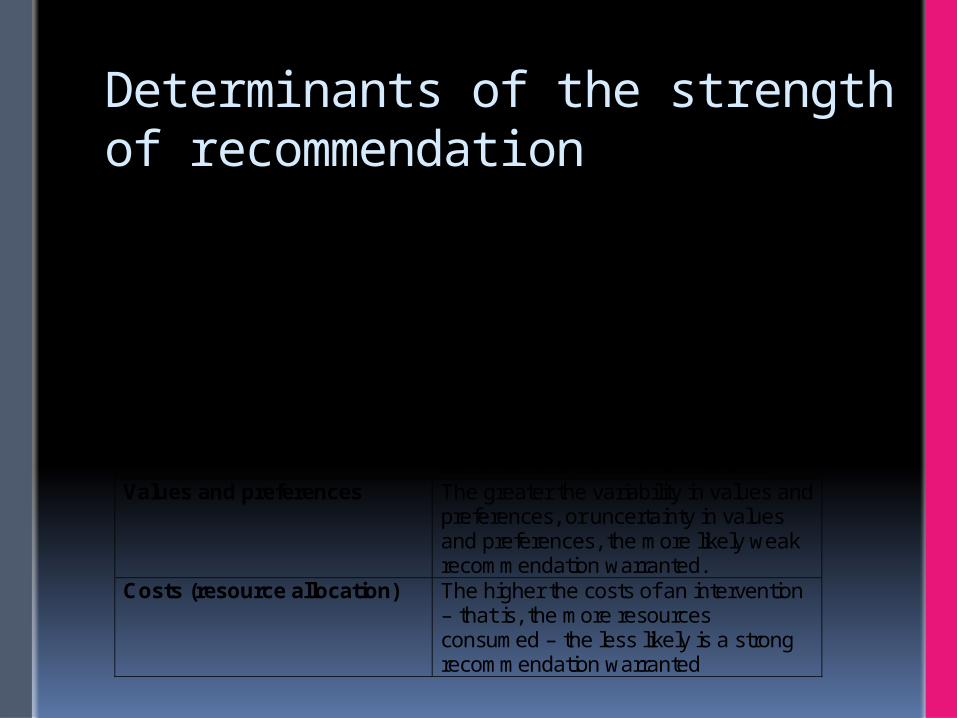
Determinants of the strength of recommendation
Factors that can strengthen a recommendation
Comment
Quality of the evidence The higher the quality of evidence, the more likely is a strong recommendation.
Balance between desirable and undesirable effects
The larger the difference between the desirable and undesirable consequences, the more likely a strong recommendation warranted. The smaller the net benefit and the lower certainty for that benefit, the more likely weak recommendation warranted.
Values and preferences The greater the variability in values and preferences, or uncertainty in values and preferences, the more likely weak recommendation warranted.
Costs (resource allocation) The higher the costs of an intervention – that is, the more resources consumed – the less likely is a strong recommendation warranted

Determinants of the strength of recommendation
Factors that can weaken the strength of a recommendation. Example:
Decision Explanation
Lower quality evidence □ Yes□ No
Uncertainty about the balance of benefits versus harms and burdens
□ Yes□ No
Uncertainty or differences in values □ Yes□ No
Uncertainty about whether the net benefits are worth the costs
□ Yes□ No
Table. Decisions about the strength of a recommendationFrequent “yes” answers will increase the likelihood of a weak recommendation

Oseltamivir – Avian Influenza
Factors that can weaken the strength of a recommendation. Example: treatment of H5N1 patients with oseltamivir
Decision Explanation
Lower quality evidence
Yes □ No
The quality of evidence is very low
Uncertainty about the balance of benefits versus harms and burdens
Yes □ No
The benefits are uncertain because several important or critical outcomes where not measured. However, the potential benefit is very large despite potentially small relative risk reductions.
Uncertainty or differences in values □ Yes No
All patients and care providers would accept treatment for H5N1 disease
Uncertainty about whether the net benefits are worth the costs
□ Yes No
For treatment of sporadic patients the price is not high ($45).
Frequent “yes” answers will increase the likelihood of a weak recommendation

Example: Oseltamivir for Avian Flu
Recommendation: In patients with confirmed or strongly suspected infection with avian influenza A (H5N1) virus, clinicians should administer oseltamivir treatment as soon as possible (????? recommendation, very low quality evidence).
Schunemann et al. The Lancet ID, 2007

Are values important?Should resources be considered?
86

Example: Oseltamivir for Avian Flu
Recommendation: In patients with confirmed or strongly suspected infection with avian influenza A (H5N1) virus, clinicians should administer oseltamivir treatment as soon as possible (strong recommendation, very low quality evidence). Values and PreferencesRemarks: This recommendation places a high value on the prevention of death in an illness with a high case fatality. It places relatively low values on adverse reactions, the development of resistance and costs of treatment. Schunemann et al. The Lancet ID, 2007

Other explanations
Remarks: Despite the lack of controlled treatment data for H5N1, this is a strong recommendation, in part, because there is a lack of known effective alternative pharmacological interventions at this time.
The panel voted on whether this recommendation should be strong or weak and there was one abstention and one dissenting vote.

Systematic review
Guideline development
PICO
OutcomeOutcomeOutcomeOutcome
Formulate
question
Rate
importa
nce
Critical
Important
Critical
Not important
Create
evidence
profile with
GRADEpro
Summary of findings & estimate of effect for each outcome
Rate overall quality of
evidence across outcomes based
on lowest quality of critical outcomes
Panel
RCT start high, obs. data start
low1. Risk of bias2. Inconsisten
cy3. Indirectnes
s4. Imprecision5. Publication
bias
Gra
de
dow
nG
rad
e
up
1. Large effect
2. Dose response
3. Confounders
Rate quality
of evidence
for each
outcomeSelect
outcomes
Very low
LowModerate
High
Formulate recommendations:
• For or against (direction)• Strong or weak (strength)
By considering: Quality of evidence Balance
benefits/harms Values and
preferences
Revise if necessary by considering:
Resource use (cost)
• “We recommend using…”• “We suggest using…”• “We recommend against using…”• “We suggest against using…”
Outcomes
across
studies

90