american academy of pediatrics practice ......american academy of pediatrics 559 both the data and...
TRANSCRIPT

558 PEDIATRICS Vol. 94 No. 4 October 1994
AMERICAN ACADEMY OF PEDIATRICS
Practice Parameter: Management of Hyperbilirubinemia in the HealthyTerm Newborn
Provisional Committee for Quality Improvement and Subcommittee on Hyperbilirubinemia
Each year approximately 60% of the 4 million new-borns in the United States become clinically jaun-diced. Many receive various forms of evaluation andtreatment. Few issues in neonatal medicine havegenerated such long-standing controversy as thepossible adverse consequences of neonatal jaundiceand when to begin treatment. Questions regardingpotentially detrimental neurologic effects from ele-vated serum bilirubin levels prompt continuing con-cern and debate, particularly with regard to the man-agement of the otherwise healthy term newbornwithout risk factors for hemolysis.’’6 Although mostdata are based on infants with birth weights �2500 g,“term” is hereafter defined as 37 completed weeks ofgestation.
Under certain circumstances, bilirubin may betoxic to the central nervous system and may causeneurologic impairment even in healthy term new-borns. Most studies, however, have failed to substan-tiate significant associations between a specific levelof total serum bilirubin (TSB) during nonhemolytichyperbilirubinemia in term newborns and subse-quent IQ or serious neurologic abnormality (includ-ing hearing impairment).�5 Other studies have de-tected subtle differences in outcomes associated withTSB levels, particularly when used in conjunctionwith albumin binding tests and/or duration of expo-sure.5’15”7”8 In almost all published studies, the TSBconcentration has been used as a predictor variablefor outcome determinations.
Factors influencing bilirubin toxicity to the braincells of newborn infants are complex and incom-
The practice parameter, “Management of Hyperbilirubinemia in the
Healthy Term Newborn,” was reviewed by the appropriate committees andsections of the American Academy of Pediatrics (AAP), including the
Chapter Review Group, a focus group of office-based pediatricians repro-
senting each AAP DistriCt Gene R. Adams, MD; Robert M. Corwin, MD;Lawrence C. Pakula, MD; Barbara M. Harley, MD; Howard B. Weinblatt,
MD; Thomas J. Herr, MD; Kenneth E. Matthews, MD; Diane Fuguay, MD;
Robert D. Mines, MD; and Delosa A. Youn& MD. The dinicalalgorithm wasdeveloped by Carmie Margolis, MD; Agnatha Golan, MD; ProfessorMichael Karplus, Ben Gurion University of Negev, Beer Sheva, Israel; and
James R. Cooley, MD, Harvard Community Health Plan.The American Medical Association (AMA) Specialty Society Practice
Parameter Partnership reviewed the neonatal hyperbilirubinemia practice
parameter and found it to be in conformance with AMA attributes for
practice parameter development.The recommendations in this statement do not indicate an exdusive course
of treatment or procedure to be followed. Variations, taking into accountindividual circumstances, may be appropriate.PEDIATRICS (ISSN 0031 4008). Copyright © 1994 by the American Acad-emy of Pediatrics.
pletely understood; they include those that affect theserum albumin concentration and those that affectthe binding of bilirubin to albumin, the penetrationof bilirubin into the brain, and the vulnerability ofbrain cells to the toxic effects of bilirubin. It is notknown at what bilirubin concentration or underwhat circumstances significant risk of brain damageoccurs or when the risk of damage exceeds the risk oftreatment. Concentrations considered harmful mayvary in different ethnic groups or geographic loca-tions and may be lower outside North America ornorthern Europe. Reasons for apparent geographicdifferences in risk for kernicterus are not clear;the following practice parameter may not applyworldwide.
There are no simple solutions to the managementof jaundiced neonates. Continuing uncertaintiesabout the relationship between serum bilirubin 1ev-els and brain damage as well as differences in patientpopulations and practice settings contribute to van-ations in the management of hyperbilirubinemia.Early postpartum discharge from the hospital furthercomplicates the management ofjaundiced newborns,because it places additional responsibilities on par-ents or guardians to recognize and respond to devel-oping jaundice or clinical symptoms.
Some conditions significantly increase the risk ofhyperbilirubinemia, including history of a previoussibling with hyperbilirubinemia, decreasing gesta-tional age, breast-feeding, and large weight loss afterbirth. Although newborns of 37 weeks’ gestation andabove are considered “term,” infants 37 to 38 weeksof gestation may not nurse as well as more matureinfants, and there is a strong correlation betweendecreasing gestational age and risk for hyperbiliru-binemia. Infants born at 37 weeks’ gestation aremuch more likely to develop a serum bilirubin levelof 13 mg/dL or higher than are those born at 40weeks’ gestation.19�
METHODOLOGY
The Task Force on Quality Assurance (now de-signated the Provisional Committee on QualityImprovement) selected the management of hyperbi-lirubinemia as a topic for practice parameter devel-opment and appointed a subcommittee that per-formed a comprehensive literature review. Twoindependent MEDLINE searches identified primar-ily retrospective epidemiologic data derived almost
exclusively from North American and European lit-erature. The subcommittee also relied heavily on
by guest on July 29, 2020www.aappublications.org/newsDownloaded from

AMERICAN ACADEMY OF PEDIATRICS 559
both the data and analyses contained in a 1990 reportby Newman and Maisels.3 Moreover, the total expe-rience analyzed involved a relatively limited numberof healthy term infants with bilirubin levels in excessof 25 mg/dL (428 pmol/L) making it difficult todraw firm conclusions from the published data. Therecommendations that follow stem from careful con-sideration of currently available information, as an-alyzed and interpreted by subcommittee membersand consultants, and are based on evidence whenappropriate data exist and derived from consensuswhen data are lacking. The subcommittee’s recom-mendations are supported by a technical report con-taming a world literature search and analysis, andupdated literature review. The technical report isavailable from the Publications Department of theAmerican Academy of Pediatrics (AAP).
RECOMMENDATIONS
The following recommendations were developedby the AAP to aid in the evaluation and treatment ofthe healthy term infant with hyperbiirubinemia. Im-portant in the development of these guidelines is thegeneral belief that therapeutic interventions for hy-perbilirubinemia in the healthy term infant maycarry significant risk relative to the uncertain risk ofhyperbiirubinemia in this population. In theseguidelines, the AAP has attempted to describe arange of acceptable practices, recognizing that ade-quate data are not available from the scientific liter-ature to provide more precise recommendations.
Evaluation
I . Maternal prenatal testing should include ABOand Rh(D) typing and a serum screen for unusualisoimmune antibodies.Z�
2. A direct Coombs’ test, a blood type, and an Rh(D)type on the infant’s (cord) blood are recom-mended when the mother has not had prenatalblood grouping or is Rh-negative.
3. Institutions are encouraged to save cord blood forfuture testing, particularly when the mother’sblood type is group 0. Appropriate testing maythen be performed as needed.
4. When family history, ethnic or geographic origin,or the timing of the appearance of jaundice sug-gests the possibility of glucose-6-phosphate dehy-drogenase deficiency or some other cause of he-molytic disease, appropriate laboratoryassessment of the infant should be performed.
5. A TSB level needs to be determined in infantsnoted to be jaundiced in the first 24 hours of life.
6. In newborn infants, jaundice can be detected byblanching the skin with digital pressure, revealingthe underlying color of the skin and subcutaneoustissue. The clinical assessment of jaundice must bedone in a well-lighted room. Dermal icterus isseen first in the face and progresses caudally tothe trunk and extremities. As the TSB level rises,the extent of cephalocaudad progression may behelpful in quantifying the degree of jaundice; useof an icterometer or transcutaneous jaundicemeter may also be he1pful.24�
7. Evaluation of newborn infants who develop ab-
normal signs such as feeding difficulty, behaviorchanges, apnea, or temperature instability is rec-ommended-regardless of whether jaundice hasbeen detected-to rule out underlying ifiness(Table 1).
8. Follow-up should be provided to all neonates dis-charged less than 48 hours after birth by a healthcare professional in an office, clinic, or at homewithin 2 to 3 days of discharge.�
9. Approximately one third of healthy breast-fed in-
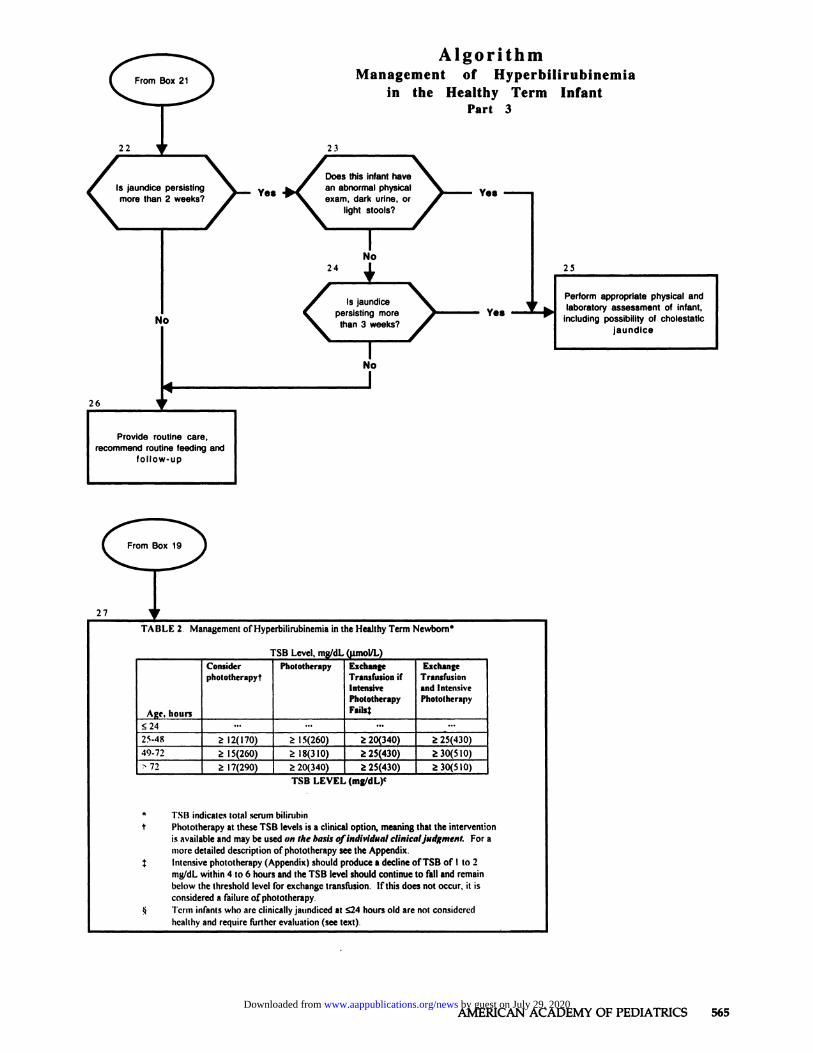
fants have persistent jaundice after 2 weeks ofage.27 A report of dark urine or light stools shouldprompt a measurement of direct serum bilirubin.If the history (particularly the appearance of theurine and stool) and physical examination resultsare normal, continued observation is appropriate.If jaundice persists beyond 3 weeks, a urine sam-ple should be tested for bilirubin, and a measure-ment of total and direct serum bilirubin obtained.
Treatment
Decisions about therapeutic intervention are tem-pered by clinical judgment based on the infant’shistory, course, and physical findings and are bal-anced by comparing the potential benefits with therisks. As appropriate, physicians are encouraged todiscuss management options and their recommenda-tions with parents or other guardians. The guidelines
in Table 2 are recommended for infants initially seenwith elevated TSB levels, as well as for infants whohave been followed up for clinical jaundice. Similarguidelines have been used in Great Britain.28’�Direct bilirubin measurements vary substantially asa function of individual laboratories and theirinstrumentation. For the purposes of the otherwise
Table 1. Factors To Be Considered When Assessing a Jaun-diced Infant”
Factors that suggest the possibility of hemolytic diseaseFamily history of significant hemolytic diseaseOnset of jaundice before age 24 hA rise in serum bilirubin levels of more than 0.5 mg/dL/hPallor, hepatosplenomegalyRapid increase in the TSB level after 24-48 h (consider G6PD
deficiency)
Ethnicity suggestive of inherited disease (G6PD deficiency,etc)
Failure of phototherapy to lower the TSB levelClinical signs suggesting the possibility of other diseases such
as sepsis or galactosemia in which jaundice may be onemanifestation of the disease
VomitingLethargyPoor feeding
HepatosplenomegalyExcessive weight loss
ApneaTemperature instabilityTachypnea
Signs of cholestatic jaundice suggesting the need to rule out
biliary atresia or other causes of cholestasisDark urine or urine positive for bilirubinLight-colored stoolsPersistent jaundice for >3 wk
* TSB indicates total serum biirubin; G6PD, glucose-6-phosphate
dehydrogenase.
by guest on July 29, 2020www.aappublications.org/newsDownloaded from

560 HYPERBILIRUBINEMIA IN THE NEWBORN
Table 2. ManagTerm Newborn”
ement of Hyperbilirubinemia in the Healthy
Age, TSB Level, mg/dL (pmol/L)hours .
ConsiderPhoto-
therapyt
Phototherapy ExchangeTransfusionif Intensive
PhototherapyFail$
ExchangeTransfusion
and Intensive
Phototherapy
s24� . . . . . . . . . ...
25-48 �12(170) �15(260) �20(340) �25 (430)49-72 �15 (260) �18 (310) �25 (430) �30 (510)>72 �17 (290) �20 (340) �25 (430) �30 (510)
* TSB indicates total serum bilirubin.t Phototherapy at these TSB levels is a clinical option, meaningthat the intervention is available and may be used on the basis of
individual clinical judgment. For a more detailed description ofphototherapy, see the Appendix.� Intensive phototherapy (Appendix) should produce a decline ofTSB of 1 to 2 mg/dL within 4 to 6 hours and the TSB level shouldcontinue to fall and remain below the threshold level for exchangetransfusion. If this does not occur, it is considered a failure ofphototherapy.§ Term infants who are dinically jaundiced at �24 hours old arenot considered healthy and require further evaluation (see text).
healthy appearing jaundiced newborn, it is recom-mended that the direct biirubin measurement not besubtracted from the TSB level and that the TSB levelbe relied on as the relevant criterion.
Determination of the rate of rise of TSB and theinfant’s age may help determine how often to mon-itor bilirubin levels and whether to begin photo-therapy. Continued observation may be an app-ropriate alternative to repeated TSB testing andphototherapy.
There is continuing uncertainty about what spe-cific TSB levels warrant exchange transfusion. Inten-sive phototherapy (Appendix) is recommended ininfants initially seen with a TSB concentration in the
exchange transfusion range (Table 2) while prepara-tions are being made for exchange transfusion. In-tensive phototherapy should produce a decline in theTSB level of I to 2 mg/dL within 4 to 6 hours, and thedecline should continue thereafter. If the TSB leveldoes not decline but persists above the level recom-mended for exchange transfusion, most experts rec-ommend exchange transfusion (Table 2). Exchangetransfusion is also indicated in infants whose TSBlevels rise to exchange transfusion levels in spite ofintensive phototherapy. In any of the above situa-tions, failure of intensive phototherapy to lower theTSB level strongly suggests the presence of hemolyticdisease or some other pathologic process and war-rants further investigation.
These guidelines apply to infants without signs ofillness or apparent hemolytic disease. It may be dif-ficult to rule out ABO hemolytic disease as well asrarer causes of hemolysis.
The evaluation and treatment of hyperbiiru-binemia in the healthy term infant is presented in thedinical Algorithm.�#{176}
Management of Hyperbilirubinemia in the HealthyTerm Newborn by Age (in Hours)
1. Infants �24 hours old are excluded from Table 2,because jaundice occurring before age 24 hours is
generally considered “pathologic” and requiresfurther evaluation. Although some healthy infantsappear slightly jaundiced by 24 hours, the pres-ence of jaundice before 24 hours requires (at least)a serum bilirubin measurement and, if indicated,further evaluation for possible hemolytic diseaseor other diagnoses. Phototherapy and/or ex-change transfusion may be indicated for rapidlyrising TSB levels in the first 24 hours of life.
2. For the treatment of the 25- to 48-hour-old infant,
phototherapy may be considered (see Table 2 fordefinition) when the TSB level is �12 mg/dL (170pmol/L). Phototherapy should be implementedwhen the TSB level is �I5 mg/dL (260 pmol/L). Ifintensive phototherapy fails to lower a TSB levelof �20 mg/dL (340 pmol/L), exchange transfu-sion is recommended. If the TSB level is �25mg/dL (430 pmol/L) when the infant is first seen,intensive phototherapy is recommended while
preparations are made for an exchange transfu-sion. If intensive phototherapy fails to lower theTSB level, exchange transfusion is recommended.The higher TSB levels in a 25- to 48-hour-old infant
suggest that the infant may not be healthy and indicate
the need for investigation into the cause of hyperbiliru-
binemia, such as hemolytic disease.
3. Phototherapy may be considered for the 49- to72-hour-old jaundiced infant when the TSB levelis �15 mg/dL (260 pmol/L). Phototherapy is rec-ommended when the TSB level reaches 18 mg/dL(310 pmol/L). If intensive phototherapy fails to
lower the TSB level when it reaches or is predictedto reach 25 mg/dL (430 pmol/L), an exchangetransfusion is recommended. If the TSB level is�30 mg/dL (510 pmol/L) when the infant is first
seen, intensive phototherapy is recommendedwhile preparations are made for exchange trans-fusion. If intensive phototherapy fails to lower theTSB level, an exchange transfusion is recom-mended.
4. For the infant >72 hours old, phototherapy may beconsidered if the TSB level reaches 17 mg/dL (290pmol/L). Phototherapy needs to be implementedat a TSB level of �20 mg/dL (340 pmol/L). Ifintensive phototherapy fails to lower a TSB levelof �25 mg/dL (430 pmol/L), exchange transfu-sion is recommended. If the TSB level is �30mg/dL (510 pmol/L) when the infant is first seen,intensive phototherapy is recommended whilepreparations are made for an exchange transfu-
sion. If intensive phototherapy fails to lower theTSB level, an exchange transfusion is recom-mended.
In all of the above situiitions, intensive phototherapy
(Appendix) should be used if the TSB level does not
decline under conventional phototherapy. Intensive
phototherapy should produce a steady decline in the
concentration of TSB. If this does not occur, the pres-
ence of hemolytic disease or some other pathologic pro-
cess is suggested and warrants further investigation.
by guest on July 29, 2020www.aappublications.org/newsDownloaded from

AMERICAN ACADEMY OF PEDIATRICS 561
Table 3. Treatment Options for Jaundiced Breast-fed Infants
ObserveContinue breast-feeding; administer phototherapySupplement breast-feeding with formula with or without
phototherapyInterrupt breast-feeding; substitute formula
Interrupt breast-feeding substitute formula; administerphototherapy
Treatment of Jaundice Associated With Breast-feedingin the Healthy Term Newborn
The AAP discourages the interruption of breast-feeding in healthy term newborns and encouragescontinued and frequent breast-feeding (at least eightto ten times every 24 hours). Supplementing nursingwith water or dextrose water does not lower thebilirubin level in jaundiced, healthy, breast-feedinginfants.3’ Depending on the mother’s preference andthe physician’s judgment, however, a variety of op-lions are presented in Table 3 for possible implemen-tation beyond observation, including supplementa-tion of breast-feeding with formula or the temporaryinterruption of breast-feeding and substitution withformula, either of which can be accompanied byphototherapy.
DOCUMENTATION
This practice parameter is designed to assist thepediatrician and other health care providers by pro-viding a framework for the management of hyperbi-lirubinemia in the healthy term newborn. It is notintended to replace the physician’s clinical judgmentor to establish a single protocol applicable to all suchnewborns with hyperbilirubinemia. It is understoodthat some clinical problems may not be adequatelyaddressed by the practice parameter, which cannotbe considered to represent an exclusive standard ofcare. Physicians are urged to document their man-agement strategies, including any significant devia-tion from these or other guidelines and the rationalefor the course of action taken.
Finally, all physicians and other health care pro-viders caring for jaundiced newborns are encour-aged to continue appraising and incorporating intotheir practices new scientific and technical advancesas clinical evidence of their effectiveness becomesestablished.
PROVISIONAL COMMi-I-I-EE ON QUALITY IMPROVEMENT,
1993 io 1994David A. Bergman, MD, ChairmanJames R. Cooley, MDJohn B. Coombs, MDMichael J. Goldberg, MD, Sections LiaisonCharles J. Homer, MD, Section on Epidemiology
LiaisonLawrence F. Nazarian, MDThomas A. Riemenschneider, MDKenneth B. Roberts, MDDame! W. Shea, MDThomas F. Tonniges, MD, AAP Board of Directors
Liaison
SUBCOMMrI-rEE ON HYPERBIURUBINEMIA, 1992 �ro 1994William 0. Robertson, MD, ChairmanJon R. Almquist, MD
Irwin J. Light, MDM. Jeffrey Maisels, MDThomas B. Newman, MD, MPH, ConsultantRonald W. Poland, MD
IN CONSULTATION Wim:Gerald B. Merenstein, MDJames A. Lemons, MDLawrence M. Gartner, MDLois Johnson, MDAudrey K. Brown, MDDavid K. Stevenson, MDAvroy Fanaroff, MDJames Cooley, MD, Clinical Algorithm
REFERENCES
1. Behrman RE, ed. Nelson’s Textbook of Pediatrics. 14th ed Philadelphia:
WB Saunders; 1992, pp 476-4812. Watchko JF, Oski FA. Bilirubin 20 mg/dL vigintiphobia. Pediatrics.
1983;71:660-.6633. Newman TB, Maisels MJ. Does hyperbilirubinemia damage the brain of
healthy newborn infants? Clin Perinatol. 1990;17:331-358
4. Newman TB, Maisels MJ. Evaluation and treatment of jaundice in the
term infant-i a kinder, gentler approach. Pediatrics. 199289:809-818
5. Newman TB, Kiebanoff M. Peak serum bilirubin in normal-sized infants
and neurodevelopmental outcome at age 7: a doser look at the collab-
orative perinatal study. Pediatrics. 199392:651-6576. Valaes T. Bilirubin toxicity: the problem was solved a generation ago.
Pediatrics. 199289:819-820
7. Wennberg RP. Bilirubin recommendations present problems: newguidelines simplistic and untested. Pediatrics. 199289:821-822
8. Merenstein GB. “NeW’ bilirubin recommendations questioned. Pediat-
rica. 199289:822-823
9. Poland RL In search of a “gold standard” for bilirubin toxicity. Pediat-
rics. 199289:823-824
10. Cashore WJ. Hyperbilirubinemia: should we adopt a new standard of
care? Pediatrics. 199Z89:824-826
11. Gartner LM. Management of jaundice in the well baby. Pediatrics. 1992;
89:826-82712. Brown AK, Seidman DS, Stevenson DK. Jaundice in healthy term
neonates: do we need new action levels or new approaches? Pediatrics.
199289:827-828
13. Johnson L Yet another expert opinion on bilirubin toxicity! Pediatrics.
199289:829-830
14. Newman TB, Maisels MJ. Response to commentaries re: evaluation and
treatment of jaundice in the term newborn: a kinder, gentler approach.
Pediatrics. 199289:831-833
15. Seidman DS, Paz I, Stevenson DK, et al. Neonatal hyperbifirubinemiaand physical and cognitive performances at 17 years of age. Pediatrics.
199188:828-833
16. Martinez JC, Maisels MJ, Otheguy L, ci al. Hyperbilirubinemia in the
breast-fed newborn: controlled trial of four interventions. Pediatrics.
199391:470-47317. Johnson LH, Boggs TR. Bilirubin-dependent brain damage: incidence
indications for treatment. In: O’Dell GB, Schaffer R, Simopoulous AP,eds. Phototherapy in the Newborn: An Overview. Washington, DC:National Academy of Sciences; 1974;122-149
18. Johnson LH. Hyperbilirubinemia in the term infant: when to worry,when to treat. NY State J Med. 199191:483-489
19. Gale R, Seidman DS, Dollberg 5, Stevenson DK. Epidemiology of neo-
natal jaundice in the Jerusalem population. I Pediatr Gastrcenterol Nutr.
1990;10:82-86
20. Friedman L, Lewis PJ, Clifton P, et aL Factors influencing the incidenceof neonatal jaundice. Br Med 1. 1978;1:1235-.1237
21. Linn 5, Schoenbaum SC, Monson RR, et al. Epidemiology of neonatal
hyperbilirubinemia. Pediatrics. 1985;75:770-774
22. MaiseIs MJ, Gifford KL, Antle CE, Lieb GR. Jaundice in the healthy
newborn infant: a new approach to an old problem. Pediatrics. 198881:
505-51123. American Academy of Pediatrics, American College of Obstetricians
and Gynecologists. Guidelines for Perinatal Care. 3rd ed. Elk Grove Vil-lage, IL: American Academy of Pediatrics; 1992
24. Kramer U. Advancement of dermal icterus in the jaundiced newborn.AJDC. 1969;118:454
25. Ebbesen F. The relationship between the cephalopedal progress of
clinical icterus and the serum bilirubin concentration in newborn in-
by guest on July 29, 2020www.aappublications.org/newsDownloaded from

562 HYPERBILIRUBINEMIA IN THE NEWBORN
fants without blood type sensitization. Obstet Gynecol Scand. 197554:
329-332
26. Schumacher RE. Nomnvasive measurements of bilirubin in the new-
born. Clin Perinatol. 1990;17:417-435
27. Alonso EM, Whitington PF, Whitington SH, Rivard WA, Given G.
Enterohepatic circulation of non-conjugated biirubin in rats fed with
human milk. I Pediatr. 1991;118:425-430
28. Dodd KL. Neonatal jaundice-a lighter touch. Arch Dis Child. 1993;68:529-533
29. Finlay 1-1’/L, Tucker SM. Neonatal plasma bilirubin chart. Arch Dis
Child. 1978;53:90-91
30. Pearson SD, Margolis CZ, Davis 5, Schreier LK, Gottlieb LK. The clinical
algorithm nosology: a method for comparing algorithmic guidelines.
Med Decision Making. 1992;12:123-131
31. Nicoll A, Ginsburg R, TrippJH. Supplementary feeding and jaundice in
newborns. Acta Pediatr Scand. 1982;71 :759-761
Phototherapy
APPENDIX
There is no standardized method for delivering phototherapy.Phototherapy units vary widely, as do the types of lamps used inthese units. The following factors strongly influence the efficacy ofphototherapy:
The energy output (or irradiance) of the phototherapy light in theblue spectrum, measured in pW/cm2;
The spectrum of light delivered by the phototherapy unit, deter-
mined by the type of light source.
The surface area of the infant exposed to phototherapy.
Commonly used phototherapy units contain a number of day-light, cool white, blue, or “special blue” fluorescent tubes. Other
units use tungsten-halogen lamps in different configurations, ei-
ther free-standing or as part of a radiant warming device. Mostrecently, fiberoptic systems have been developed that deliver lightfrom a high-intensity lamp to a fiberoptic blanket. Most of thesedevices deliver enough output in the blue-green region of thevisible spectrum to be effective for standard phototherapy use.When bilirubin levels approach the range at which exchange
transfusion might be indicated, maximal efficacy should be
sought. This can be achieved in the following manner.
The use of special blue tubes in standard fluorescent phototherapyunits. Note that special blue (narrow spectrum) tubes cany thedesignation P20 T12/BB are not the same as blue tubes (P20T12/B)) Special blue lights have the disadvantage of making theinfant look blue, but in healthy newborns this is generally not a
concern during the relatively brief period that phototherapy isnecessary. To mitigate this effect, four special blue tubes may beused in the central portion of a standard phototherapy unit andtwo daylight fluorescent tubes may be used on either side.2
Regardless of the type of light used, its maximum irradianceshould be employed. Standard fluorescent lamps accomplish this
by bringing the light as close to the baby as possible. In thefull-term nursery, this is most easily achieved by placing the infantin a bassinet (not an incubator) and lowering the lamps to within15 to 20 cm of the infant. If this treatment causes slight warming
of the infant, the lamps need to be elevated slightly. With halogenphototherapy lamps, however, there are no data to indicate howclose to the baby the lamp can be positioned without incurring therisk of a burn. When halogen lamps are used, manufacturers’recommendations should be followed. The reflectors, light source,and transparent light ifiters (if any) should be kept clean.
The third way to improve phototherapy efficiency is to increasethe surface area of the infant exposed to the lights. This is done,
most simply, by placing the infant on a fiberoptic blanket whileusing a standard phototherapy system described above.3 If fibe-roptic units are not available, several phototherapy lamps can beplaced around the infant. When a single phototherapy unit isused, the area of exposure can be increased by placing a whitereflecting surface (such as a sheet) around the bassinet so that lightis reflected onto the baby’s skin. Removing diapers will also
increase the exposed surface area.
Intermittent Versus Continuous Phototherapy
Clinical studies comparing intermittent with continuous pho-totherapy have produced conflicting results.46 Because all lightexposure increases bilirubin excretion (compared with darkness),no plausible scientific rationale exists for using intermittent pho-totherapy. In the majority of circumstances, however, photother-
apy does not need to be continuous. Phototherapy may be inter-rupted during feeding or brief parental visits. Individualjudgment should be exercised. If the infant is admitted to thehospital with a biirubin level �25 mg/dL(428 pmol/L), intensive
phototherapy should be administered continuously until a satis-
factory decline in the serum bilirubin level occurs or exchangetransfusion is initiated.
Intensity of Phototherapy
The intensity of the phototherapy (number of lights, distancefrom infant, and use of double phototherapy, use of special lights)
should also be tailored to the infant’s needs. In many circum-
stances intensive phototherapy is not necessary. However, if theserum bilirubin level is rising in spite of conventional photother-apy or the infant is admitted with a serum bilirubin concentration
within the exchange transfusion range, the necessary steps should
be taken to increase the intensity of phototherapy during prepa-ration for exchange transfusion. With the light sources commonlyused, it is impossible to overdose the patient.
Hydration
To our knowledge, no evidence exists that excess fluid admin-istration affects the serum bilirubin concentration. Some infants
who are admitted with high bilirubin levels are also mildly dehy-drated, however, may need supplemental fluid intake to correcttheir dehydration. As these infants are almost always breast-fed,
the best fluid to use in these circumstances is a milk-based for-
mula, because it inhibits the enterohepatic circulation of biirubinand helps lower the serum bilirubin level. Because the photoprod-ucts responsible for the decline in serum bilirubin are excreted inboth urine and bile, maintaining adequate hydration and goodurine output should help improve the efficacy of phototherapy.7
Routine supplementation (with dextrose water) of infants receiv-
ing phototherapy is not indicated.
When Should Phototherapy Be Stopped?
A recent study found that, in infants who do not have hemo-lyric disease, the average bilirubin rebound after phototherapy is
less than I mg/dL (17 pmol/L).8 Phototherapy may be discontin-ued when the serum biirubin level falls below 14 to 15 mg/dL.Discharge from the hospital need not be delayed in order to
observe the infant for rebound and, in most cases, no furthermeasurement of bilirubin is necessary. If phototherapy is initiatedearly and discontinued before the infant is 3 to 4 days old, addi-
tional outpatient follow-up may be necessary.
APPENDIX REFERENCES
1. Ennever JF. Blue light, green light, white light, more light: treatment of
neonatal jaundice. Clin Perinatol. 1990;17:407-478
2. Hammerman C, Eidelman A, Lee K-S. et al. Comparative measurements
of phototherapy: a practical guide. Pediatrics. 1981;67:368-372
3. Holtrop PC, Ruedisueli K, Maisels MJ. Double versus single photother-
apy in low birthweight infants. Pediatrics. 199290:674-677
4. Maurer HM, Shumway C, Draper DA, et al. Controlled trial comparing
agar, intermittent phototherapy, and continuous phototherapy for re-ducing neonatal hyperbilirubinemia. I Pediatr. 1973;82:73-76
5. Rubaltelli FF, Zanardo V. Granati B. Effect of various phototherapy
regimens on bilirubin decrement. Pediatrics. 1978;61 :838-841
6. Lau SP, Fung KP. Serum bilirubin kinetics in intermittent phototherapy
of physiological jaundice. Arch Dis Child. 198459:892-894
7. Wu PYK, Hodgman JE, Kirkpatrick By, et al. Metabolic aspects of
phototherapy. Pediatrics. 1985;75:427-433
8. Lazar L, Litwin A, Nerlob P. Phototherapy for neonatal nonhemolytic
hyperbilirubinemia. Analysis of rebound and indications for discon-
tinuing phototherapy. Clin Pediatr. 199332:2M-267
by guest on July 29, 2020www.aappublications.org/newsDownloaded from

IPediatric clinician
evaluates term newbornwith jaundice J
2
Exit this algorithm to Individualizedclinical evaluation, includingassessment of jaundice and
underlying disease
Ye.
:::::::i�#-___.__ Yes
Exit this algorithm to indMdualizedclinical evaluation, including
assessment of jaundice in light ofprematurity
9
)
8
� No PDoes the mother’sYes blood have any
Yes
Consider holding theinfant’s cord blood in a
blood bank In case futuretesting is necessary
V
10
Perform blood typing (ABO andRh) and direct Coombs’ testing
on the infant’s cord (preferably)or venous blood
Il�
Is the infantsblooddirect Coombs’ Yes
positive?
No
�x13
AMERICAN ACADEMY OF PEDIATRICS 563
AlgorithmManagement of Hyperbilirubinemia
in the Healthy Term Infant
K Does the infant have signs ofunderlying serious illness
(lethargy, apnea. tachypnea.temperature Instability, behavior
changes. hepatosplenomegaly,persistent vomiting,
or persistent feeding difficulty)?
No
4
Is the infant <37 weeks,gestatlonal age?
No6
Is the mother’s ABOand Rh blood typing
and isoimmunestatus
Li
Ye.
12
Exit this algorithm to individualizedclinical evaluation, includingassessment of jaundice and
Isoimmune hemolytic disease
by guest on July 29, 2020www.aappublications.org/newsDownloaded from

14
Perform appropriate laboratoryassessment of infant including(but not limited to consideration of):
(1) Complete blood count. differential,
smear, reticulocyte count;(2) G6PD screen;(3) Hemoglobin electrophoresis
‘I )
15
Does the evaluationsuggest hernolytic
NoI V
17
V
�lnfan:uE�_______________________� Yes
and � 24 hours of age?
No
::aundice clinicaily 19�ific�gment�_____ �(1) Measure infant’s total
(2)GotoBox27Yes serum bilirubin.t_ by medical
No
20 � -
Exit this algorithm to individualizedclinical evaluation, includingassessment of jaundice and
non-isoimmunehemoiytic disease
21
�x22
564 HYPERBILIRUBINEMIA IN THE NEWBORN
AlgorithmKI�I::� Management of Hyperbilirubinemia
in the Healthy Term Infant
From Box 12 Part 2
13
Are any of the following risk factorspresent to suggest that nonisoimmunehemolytic disease is possible in thisinfant?
(1) Family history of hemolyticanemia;
OR Yes�(2) Family history of early or
severe jaundice;OR
(3) Ethnicity or geographic originassociated with hemolytic anemia;
OR(4) Early or severe jaundice.
Healthy term infant with
I jaundice not clinically significant
L� by medical judgment J
Follow infant in routine
clinical supervision
by guest on July 29, 2020www.aappublications.org/newsDownloaded from
Yes -
Yes -
25
TABLE 2. Management ofHyperbilirubinemia in the Healthy Term Newborn*
TSB Level, mg/dL (�tmol/L)
TSB LEVEL (mg/dL)t
* TSB indicales total serum bilirubin
t Phototherapy at these TSB levels is a clinical option, meaning that the interventionis available and may be Used Oft the ba.cis ofindividsial clinicalJudgnient. For amore detailed description of phototherapy see the Appendix.
� Intensive phototherapy (Appendix) should produce a decline ofTSB of I to 2mg/dL within 4 to 6 hours and the TSB level should continue to fall and remainbelow the threshold level for exchange transfusion. lfthis does not occur, it is
considered a failure of phototherapy.§ Term infants who are clinically jaundiced at �24 hours old are not considered
healthy and require fI.srther evaluation (see text).
AMERICAN ACADEMY OF PEDIATRICS 565
AlgorithmManagement of Hyperbilirubinemia
in the Healthy Term InfantPart 3
Perform appropriate physical and
:.aJ laboratory assessment of infant,-� including possibility of cholestaticjaundice
Age, hours
Considerphototherapyt
Phototherspy ExchangeTransfusion ifIntensivePhototherapyFaiI4
Exchange
Transfusionand IntensivePhototherapy
�24 ‘.‘ ... � ... -...
2S-48 � 12(170) � 15(260) �20(340) �25(430)
49-72 � 15(260) � 38(310) �25(430) �30(510)> 72 � 17(290) � 20(340) � 25(430) � 30(510)
by guest on July 29, 2020www.aappublications.org/newsDownloaded from

1994;94;558Pediatrics Newborn
Practice Parameter: Management of Hyperbilirubinemia in the Healthy Term
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/94/4/558including high resolution figures, can be found at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlentirety can be found online at: Information about reproducing this article in parts (figures, tables) or in its
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on July 29, 2020www.aappublications.org/newsDownloaded from

1994;94;558Pediatrics Newborn
Practice Parameter: Management of Hyperbilirubinemia in the Healthy Term
http://pediatrics.aappublications.org/content/94/4/558the World Wide Web at:
The online version of this article, along with updated information and services, is located on
American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397. American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 1994 by thebeen published continuously since 1948. Pediatrics is owned, published, and trademarked by the Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it has
by guest on July 29, 2020www.aappublications.org/newsDownloaded from