anaesthetic managent of turp
TRANSCRIPT
ANAESTHETIC MANAGENT OF TURP Presentor : Ritika Gupta
Moderator : Dr Trishala Jain
TURP - INTRODUCTION
The current gold standard surgical treatment for benign prostatic hyperplasia (BPH).
TURP is the 2nd most common procedure in men over 65 yrs of age.
BPH affects 50% of males at 60 years and 90% of 85-year-olds, so TURP is most commonly performed on elderly patients, a population group with a high incidence of cardiac, respiratory and renal disease.
TURP carries unique complications because of the need to use large volumes of irrigating fluid for the endoscopic resection.
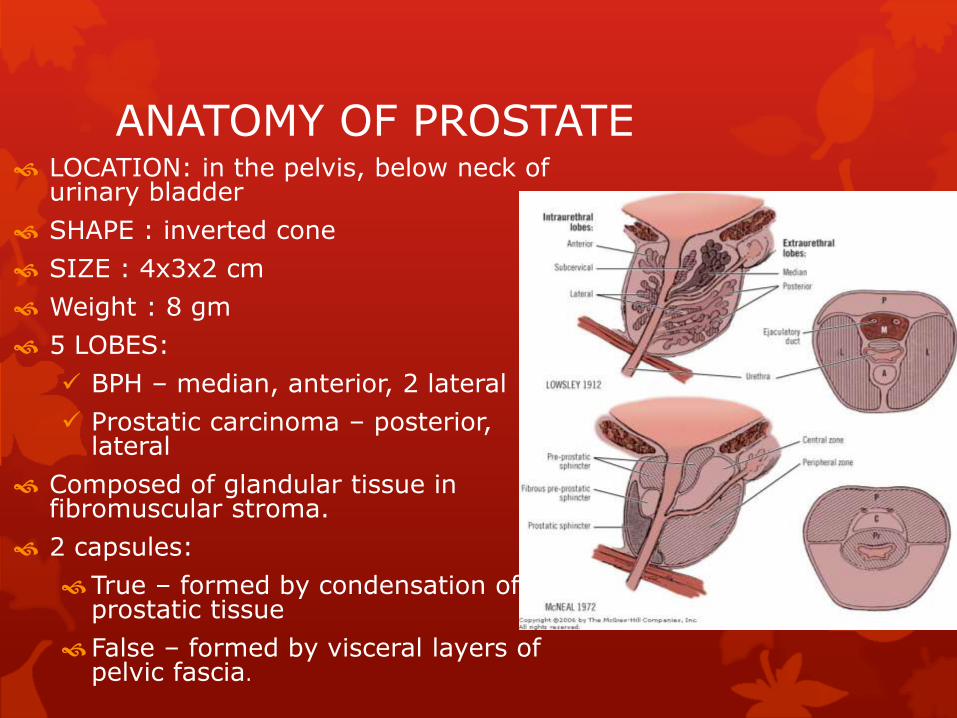
ANATOMY OF PROSTATE LOCATION: in the pelvis, below neck of
urinary bladder
SHAPE : inverted cone
SIZE : 4x3x2 cm
Weight : 8 gm
5 LOBES:
BPH – median, anterior, 2 lateral
Prostatic carcinoma – posterior, lateral
Composed of glandular tissue in fibromuscular stroma.
2 capsules:
True – formed by condensation of prostatic tissue
False – formed by visceral layers of pelvic fascia.
ANATOMY OF PROSTATE
NERVE SUPPLY
Sympathetic supply
T11-L2
Inferior hypogastricplexus
Parasympathetic supply
S2,3,4
Pelvic splanchnic nerve
BLOOD SUPPLY
Arterial supply
Inferior vesical artery
Middle rectal artery
Internal pudendal artery
Venous supply
Vesical plexus
Internal pudendal veins
Vertebral venous plexus
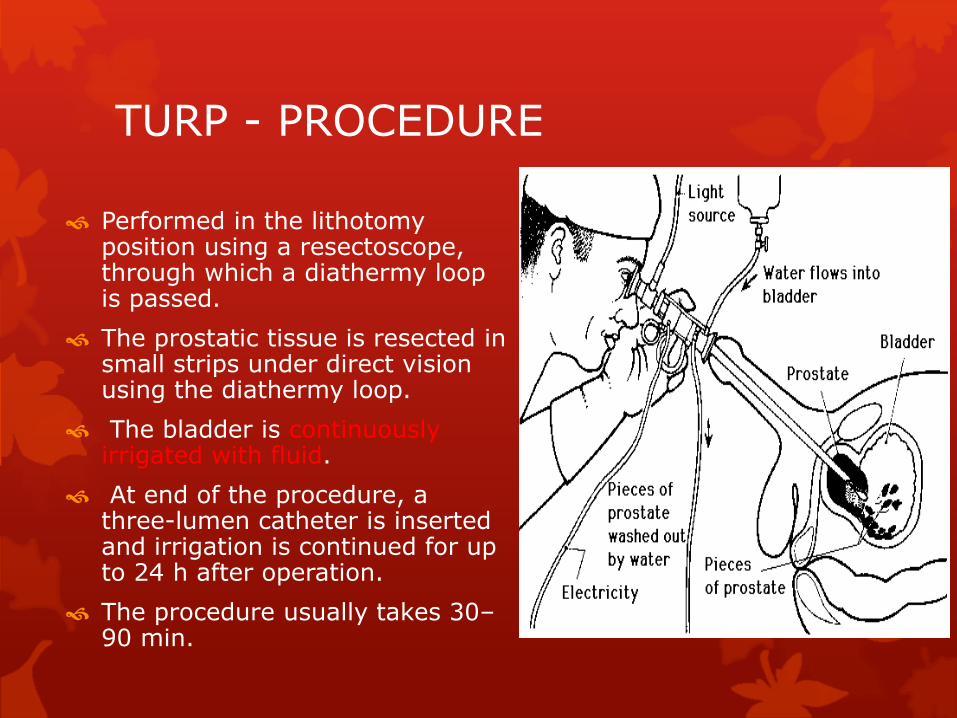
Performed in the lithotomy position using a resectoscope, through which a diathermy loop is passed.
The prostatic tissue is resected in small strips under direct vision using the diathermy loop.
The bladder is continuously irrigated with fluid.
At end of the procedure, a three-lumen catheter is inserted and irrigation is continued for up to 24 h after operation.
The procedure usually takes 30–90 min.
TURP - PROCEDURE
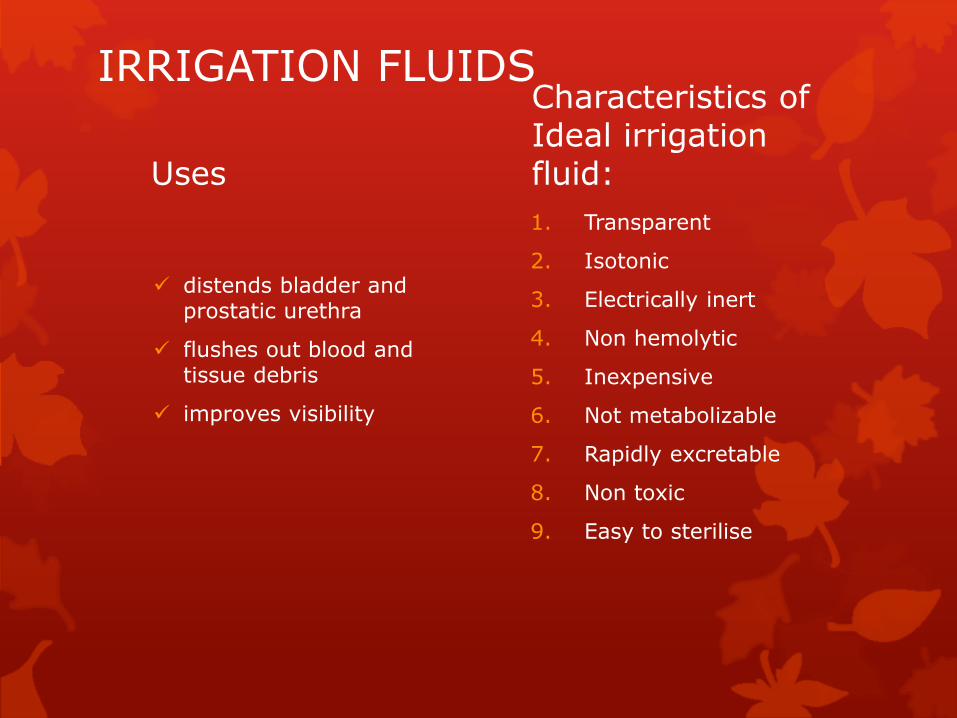
IRRIGATION FLUIDS
Uses
distends bladder and prostatic urethra
flushes out blood and tissue debris
improves visibility
Characteristics of Ideal irrigation fluid:
1. Transparent
2. Isotonic
3. Electrically inert
4. Non hemolytic
5. Inexpensive
6. Not metabolizable
7. Rapidly excretable
8. Non toxic
9. Easy to sterilise
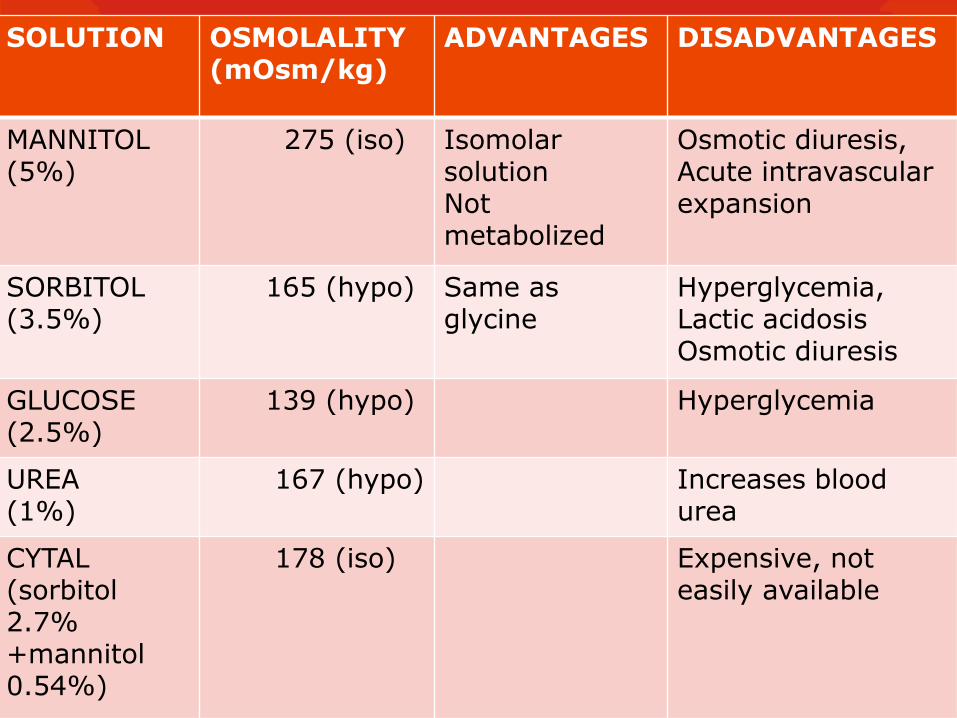
SOLUTION OSMOLALITY (mOsm/kg)
ADVANTAGES DISADVANTAGES
MANNITOL(5%)
275 (iso) IsomolarsolutionNotmetabolized
Osmotic diuresis, Acute intravascular expansion
SORBITOL(3.5%)
165 (hypo) Same as glycine
Hyperglycemia,Lactic acidosisOsmotic diuresis
GLUCOSE(2.5%)
139 (hypo) Hyperglycemia
UREA(1%)
167 (hypo) Increases blood urea
CYTAL(sorbitol2.7% +mannitol0.54%)
178 (iso) Expensive, not easily available
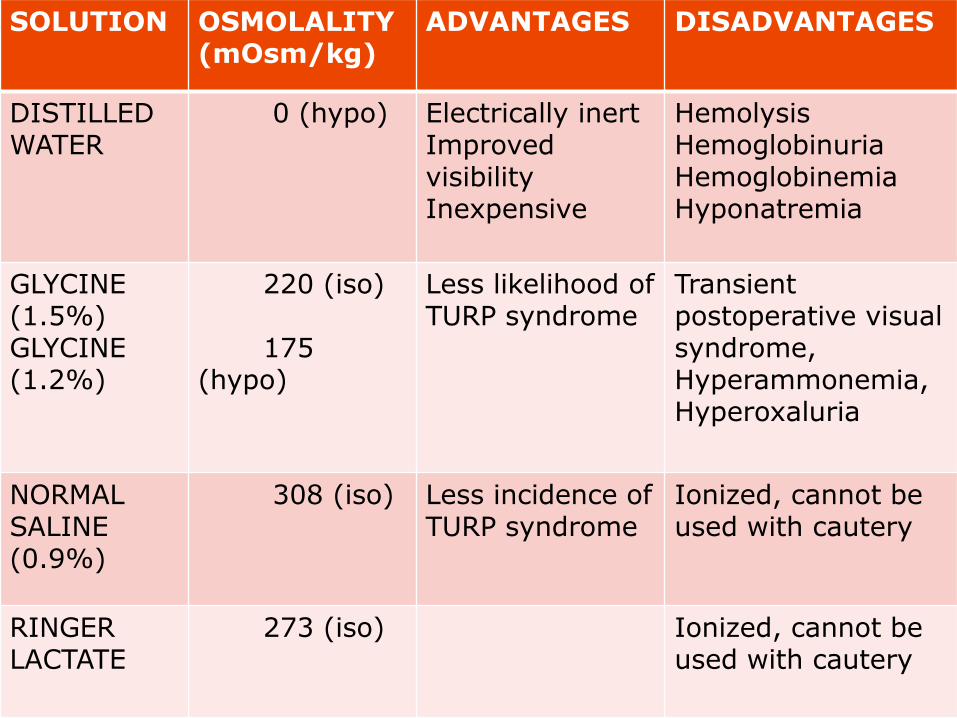
SOLUTION OSMOLALITY (mOsm/kg)
ADVANTAGES DISADVANTAGES
DISTILLED WATER
0 (hypo) Electrically inertImprovedvisibilityInexpensive
HemolysisHemoglobinuriaHemoglobinemiaHyponatremia
GLYCINE (1.5%) GLYCINE(1.2%)
220 (iso)
175 (hypo)
Less likelihood of TURP syndrome
Transientpostoperative visual syndrome,Hyperammonemia,Hyperoxaluria
NORMAL SALINE (0.9%)
308 (iso) Less incidence of TURP syndrome
Ionized, cannot be used with cautery
RINGER LACTATE
273 (iso) Ionized, cannot be used with cautery
Factors affecting amount and rate of fluid absorption
Size of gland (25ml/gm of prostate)
Number and size of open sinuses
Hydrostatic pressure of irrigating fluid
Duration of procedure (@ 20-30 ml/min)
Integrity of capsule
Venous pressure at irrigant-blood interface
Vascularity of diseased prostate
PREOPERATIVE CONSIDERATIONS Patients for TURP are frequently elderly with coexistent diseases.
- cardiac disease 67%
- cardiovascular disease 50%
- abnormal electrocardiogram (ECG) 77%
- chronic obstructive pulmonary disease 29%
- diabetes mellitus 8%
Occasionally, patients are dehydrated and depleted of essential electrolytes (long-term diuretic therapy and restricted fluid intake).
Long standing urinary obstruction can lead to impaired renal function and chronic urinary infection.
About 30% of TURP patients have infected urine preoperatively
PREOPERATIVE EVALUATION
History and examination of all organ systems
INVESTIGATIONS
Hb, TLC, DLC, platelet count
Blood sugar
Blood urea, S. Creatinine, S. Electrolytes
Urine R/M
ECG
Chest X-ray
Blood grouping and cross matching
PREOPERATIVE PREPARATION
Optimization of pre-existing co-morbid conditions
Consideration of ongoing drug therapy
Antibiotic prophylaxis (in case of urinary tract infection or urinary obstruction)
Arrangement of blood
CHOICE OF ANAESTHESIA Regional anaesthesia is the technique of choice for TURP.
Advantages of regional over general anaesthesia
1. Allows monitoring of mentation and early signs of TURP syndrome and bladder perforation
2. Promotes peripheral vasodilation , reducing circulatory overload
3. Reduces blood loss, requiring fewer transfusions
4. Avoids effects of general anaesthesia on pulmonary pathology
5. Good early post-operative analgesia
6. Reduced incidence of post-operative DVT/PE
7. Neuroendocrine and immune response are better preserved
8. Lower cost
General anaesthesia preferred when regional is contraindicated.
REGIONAL ANAESTHESIA
TECHNIQUES:
Subarachnoid block
Epidural block
Caudal block
Saddle block
Level of sensory block
T10 dermatome level – to eliminate discomfort caused by bladder distention
T9 dermatome level – enable to elicit capsular sign (pain on perforation of prostatic capsule)
REGIONAL ANAESTHESIA
Subarachnoid block is preferred.
Advantages of SAB over epidural anaesthesia:
Technically easier to perform
Dense motor blockade
No sacral sparing
Lower incidence of PDPH
MONITORING
ECG
Blood pressure
Pulse oximetry
Temperature
Mentation
Blood loss
S. electrolytes (serial)
EtCO2 if GA is used

INTRAOPERATIVE CONSIDERATIONS
Lithotomy position
TURP syndrome
Bladder perforation
Hypothermia
Transient bacterial septicemia
Hemorrhage and coagulopathy
LITHOTOMY POSITIONING
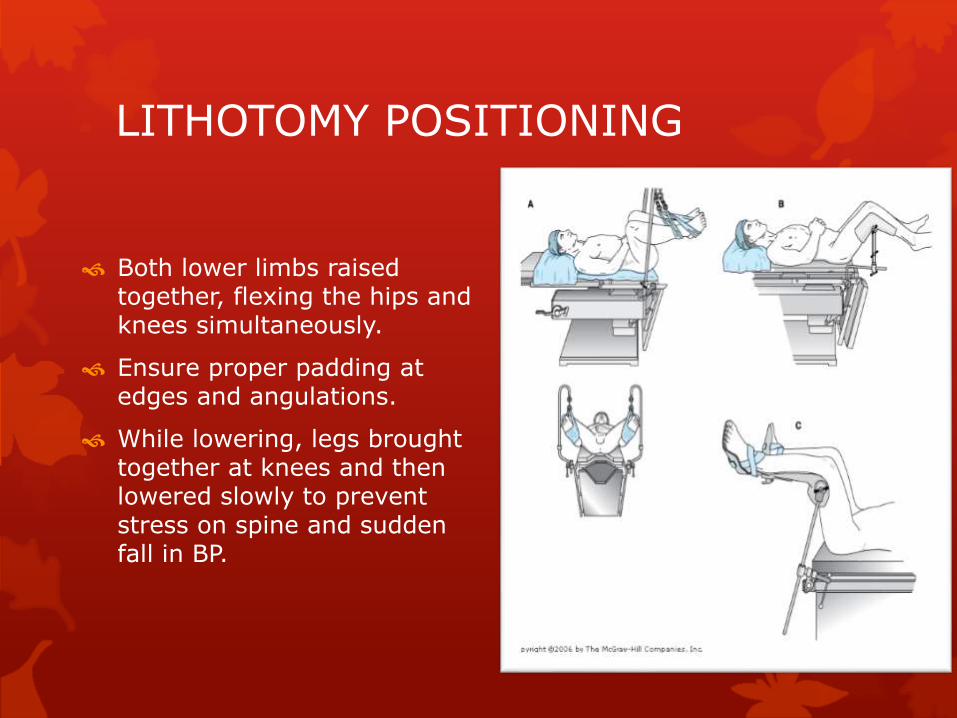
Both lower limbs raised together, flexing the hips and knees simultaneously.
Ensure proper padding at edges and angulations.
While lowering, legs brought together at knees and then lowered slowly to prevent stress on spine and sudden fall in BP.
LITHOTOMY POSITIONING
Physiologic changes with lithotomy
Decreased FRC
Increased venous return on elevation of legs
Decreased venous return following lowering of legs
Exaggeration of hypotension with SAB
Problems with lithotomy position
Injury to nerves
Injury to fingers
Compression of major vessels at joints
Lower extremity Compartment syndrome
Aggravation of preexisting lower back pain
TURP SYNDROME Rapid absorption of a large-volume irrigation solution.
Can occur 15 min after resection or upto 24 hrs postop.
Incidence : 1 – 8%
Characterized by intravascular volume shifts and plasma-solute (osmolarity) effects:
Circulatory overload
Water intoxication
Hyponatremia
Hypoosmolality
Hyperglycinemia
Hyperammonemia
Hemolysis
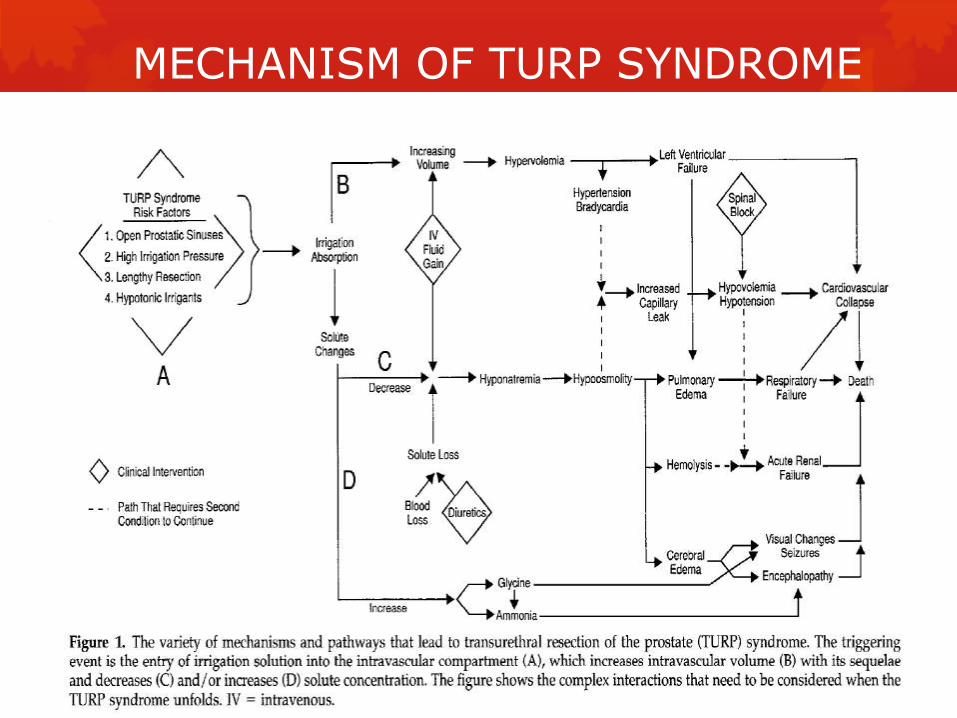
MECHANISM OF TURP SYNDROME
TURP SYNDROME – WATER INTOXICATION Cause : cerebral edema
Signs and symp:
Somnolence, restlessness, seizures, coma
CNS – decerebrate posture, clonus, +vebabinski’s reflex
Eyes – papilloedema, dilated and non reactive pupils
EEG – low voltage b/l.
TURP SYNDROME -HYPONATREMIA Cause : excessive absorption of Na free irrigation
fluid
During TURP, S.Na falls by 3 to 10 meq/l.
SIGNS AND SYMPTOMS OF Acute Hyponatremia
Nausea
Vomiting
Irritability
Mental confusion
Cardiovascular collapse
Pulmonay edema
Seizures
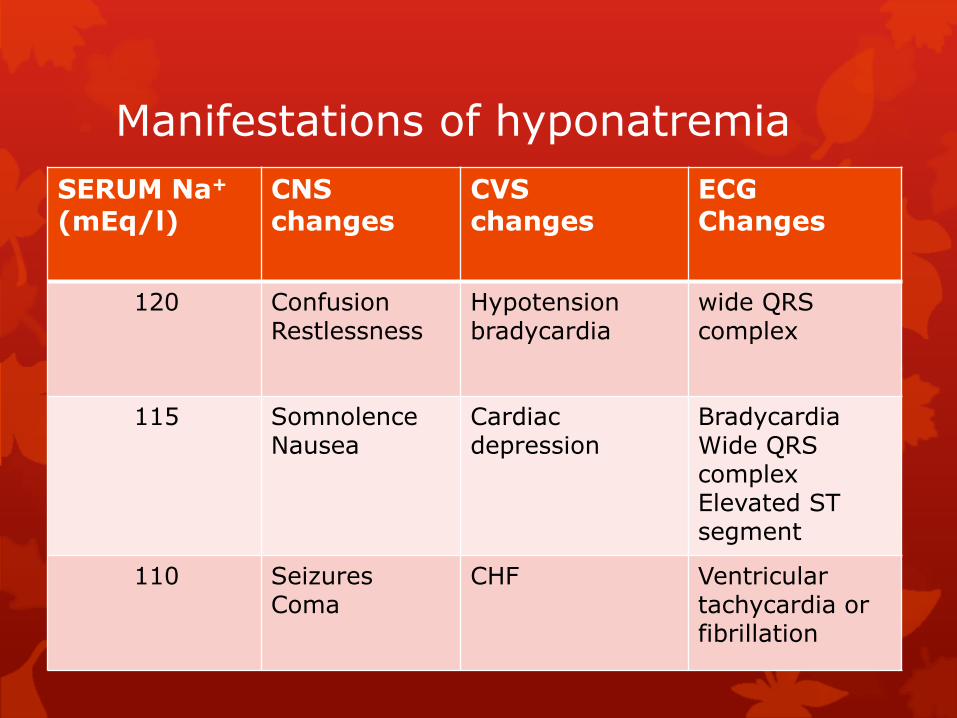
Manifestations of hyponatremia
SERUM Na+
(mEq/l)CNS changes
CVS changes
ECG Changes
120 ConfusionRestlessness
Hypotension bradycardia
wide QRS complex
115 SomnolenceNausea
Cardiacdepression
BradycardiaWide QRS complexElevated ST segment
110 Seizures Coma
CHF Ventriculartachycardia or fibrillation
TURP SYNDROME -HYPERGLYCINEMIA
Glycine, a non essential amino acid, is an inhibitory neurotransmitter in spinal cord and retina.
Metabolized in liver by oxidative deamination to ammonia and glyoxylic and oxalic acid.
When absorbed in large amounts, has direct toxic effects on heart and retina.
Manifestations of glycine toxcity: nausea, headache, malaise, weakness, visual distubances ( transient blindness), seizures, encephalopathy.
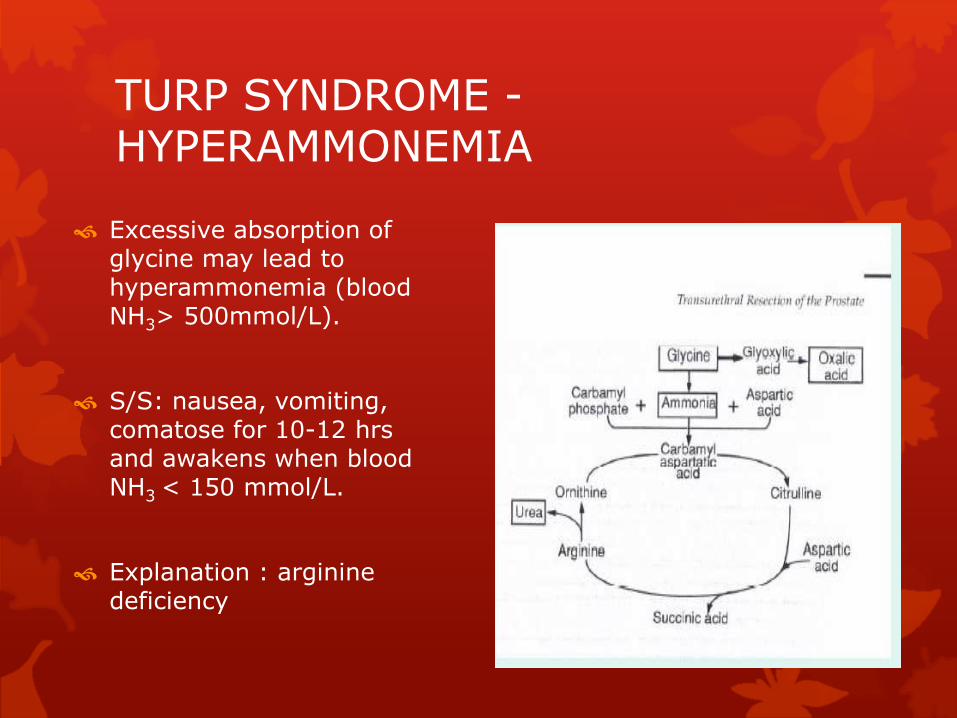
TURP SYNDROME -HYPERAMMONEMIA
Excessive absorption of glycine may lead to hyperammonemia (blood NH3> 500mmol/L).
S/S: nausea, vomiting, comatose for 10-12 hrsand awakens when blood NH3 < 150 mmol/L.
Explanation : arginine deficiency
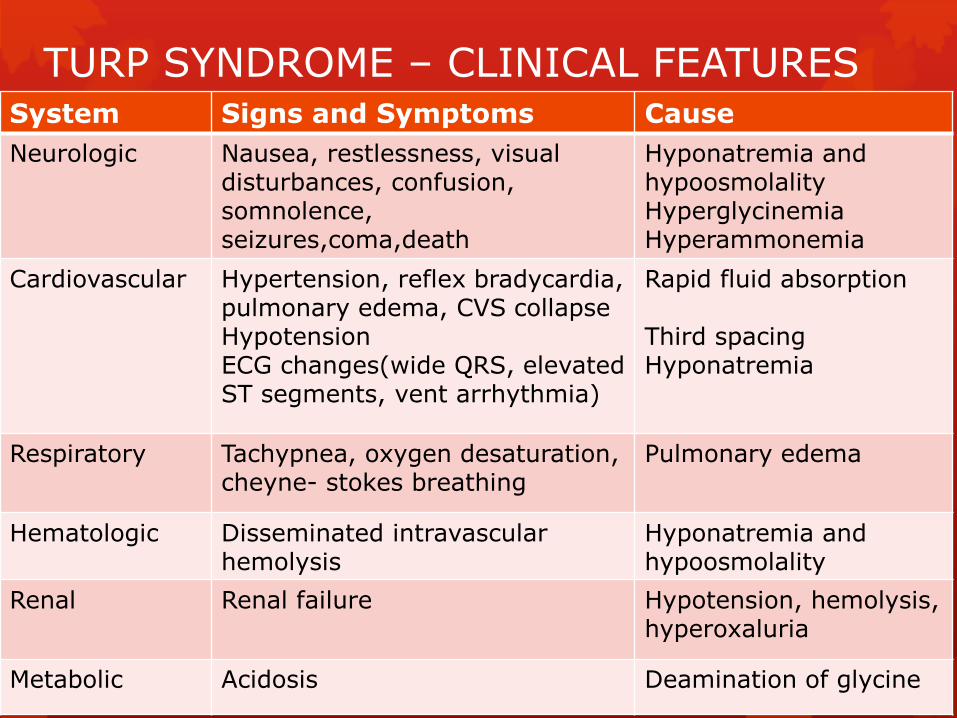
TURP SYNDROME – CLINICAL FEATURES System Signs and Symptoms Cause
Neurologic Nausea, restlessness, visual disturbances, confusion, somnolence, seizures,coma,death
Hyponatremia and hypoosmolalityHyperglycinemiaHyperammonemia
Cardiovascular Hypertension, reflex bradycardia, pulmonary edema, CVS collapseHypotension ECG changes(wide QRS, elevated ST segments, vent arrhythmia)
Rapid fluid absorption
Third spacingHyponatremia
Respiratory Tachypnea, oxygen desaturation, cheyne- stokes breathing
Pulmonary edema
Hematologic Disseminated intravascular hemolysis
Hyponatremia and hypoosmolality
Renal Renal failure Hypotension, hemolysis,hyperoxaluria
Metabolic Acidosis Deamination of glycine
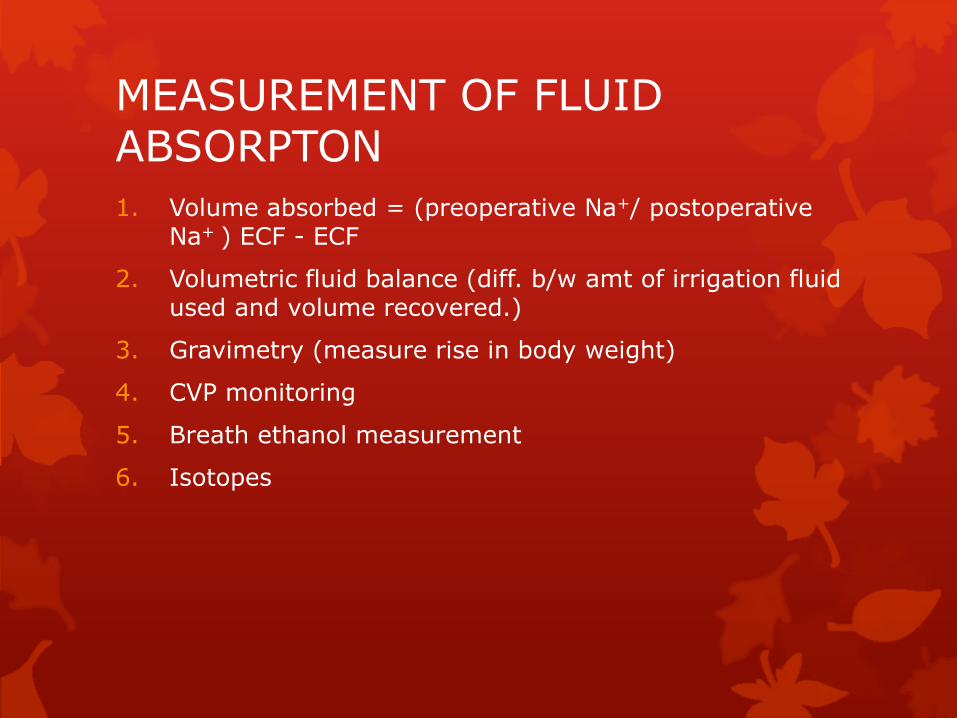
MEASUREMENT OF FLUID ABSORPTON
1. Volume absorbed = (preoperative Na+/ postoperative Na+ ) ECF - ECF
2. Volumetric fluid balance (diff. b/w amt of irrigation fluid used and volume recovered.)
3. Gravimetry (measure rise in body weight)
4. CVP monitoring
5. Breath ethanol measurement
6. Isotopes
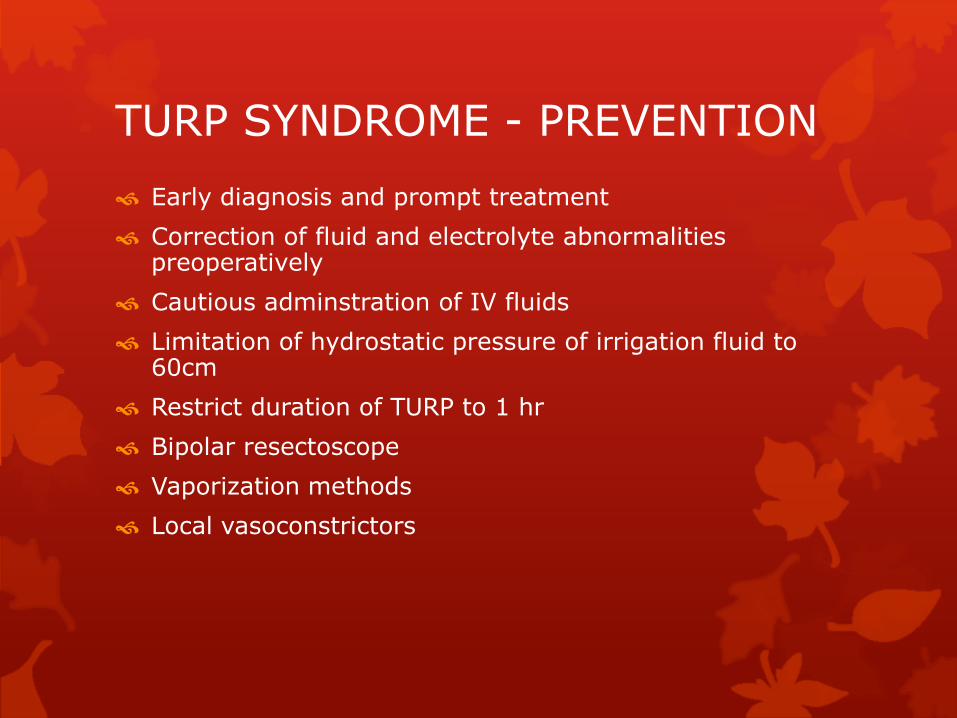
TURP SYNDROME - PREVENTION
Early diagnosis and prompt treatment
Correction of fluid and electrolyte abnormalities preoperatively
Cautious adminstration of IV fluids
Limitation of hydrostatic pressure of irrigation fluid to 60cm
Restrict duration of TURP to 1 hr
Bipolar resectoscope
Vaporization methods
Local vasoconstrictors
TURP SYNDROME -MANAGEMENT
Notify surgeon and terminate surgery.
Ensure oxygenation
Restrict fluids
Pulmonary edema : intubate and IPPV
Bradycardia, hypotension: atropine, adrenergic agents
Seizures : BZD, thiopentone, phenytoin, i.v.Mg2+
Invasive monitoring of arterial and CVP
Send blood sample for electrolytes, arterial blood gas analysis.
TURP SYNDROME -MANAGEMENT
Treat mild symptoms (if S. Na+ > 120 mEq/L) with fluid restriction and loop diuretic (furosemide)
Treat severe symptoms (if S. Na+ <120 mEq/L) with 3% NaCl IV at rate < 100 ml/ hr.
BLADDER PERFORATION
Incidence – 1%
Causes
Trauma by surgical instrument
Overdistention of bladder with irrigation fluid
Manifestation
Early sign : sudden decrease in return of irrigation solution from bladder
Extraperitoneal perforations : pain in periumbilical, inguinal or suprapubic region
Intraperitoneal : generalised abdominal pain, shoulder tip pain, abdo rigidity
BLOOD LOSS
Difficult to quantify blood loss.
Visual estimation of haemorrhage may be difficult due to dilution with irrigation fluid.
Usual warning signs (tachycardia, hypotension) masked by overhydration and effects of regional anaesthesia.
Blood loss can be estimated on the basis of
Resection time (2-5ml/min)
Size of prostate (7-20ml/g)
No. of open venous sinuses
Intraoperative BT should be based on preop Hb, duration and difficulty of resection and clinical assessment of ptcondition.
COAGULOPATHY
Causes of excessive bleeding
Dilutional thrombocytopenia
DIC as a result of release of prostatic particles rich in thromboplastin into blood
Local release of fibrinolytic agents (plasminogen and urokinase)
Treatment – administration of FFP, platelets blood transfusion
HYPOTHERMIA
Continuous fluid irrigation causes loss of temp @1oC/hr.
Elderly patients have reduced thermoregulatory capacity.
Unintentional hypothermia is asso. with a significantly higher incidence of postoperative MI.
Postoperative shivering asso. with hypothermia may dislodge clots and promote postoperative bleeding.
Monitor body temp of patient to maintain normothermia.
Appropriate measures to reduce heat loss are: warming blankets, heated irrigation solution and warm I/V fluids.
BACTEREMIA AND SEPTICEMIA
INCIDENCE – 6-7%
Causes
Release of bacteria from prostatic tissue
Preoperative indwelling urinary catheter
Preoperative UTI
C/F – chills, fever, tachycardia
T/T – antibiotic, supportive care
POSTOPERATIVE COMPLICATIONS
Hypothermia
Hypotension
Haemorrhage
Septicaemia
TURP syndrome
Bladder spasm
Clot retention
Deep vein thrombosis
Postoperative cognitive impairment
REFERENCES
Miller’s Anesthesia 7th Editon. Anesthesia and renal and genitourinary system.
Barasch’s Clinical Anesthesia 5th Edition. The renal system and anesthesia for urologic surgery.
Yao and Artusio’s Anesthesiology problem oriented patient management. 6th Edition.
Clinical anesthesiology by Morgan and Mikhail. 4th
Edition. Anesthesia for genitourinary surgery.
Dietrich Gravenstein. Transurethral resection of prostate (TURP) syndrome: a review of pathophysiology and management. Anesth Analg 1997;84:438-46.
