anaesthetics prof. kršiak department of pharmacology, third faculty of medicine, charles university...
TRANSCRIPT

Anaesthetics
Prof. Kršiak
Department of Pharmacology, Third Faculty of Medicine, Charles University in Prague
Cycle II, Modul OTA („ Orthopedic-Tramatologic-Anesthetic“)
Charles University in Prague, Third Faculty of Medicine
Academic year 2012-2013
GENERAL MEDICINE 6-YEAR MASTER‘S STUDY PROGRAMME

General anaesthetics• Intravenous anaesthetics• Inhalation anaesthetics
Local anaesthetics
Rang & Dale's Pharmacology 7E,
OUTLINE
Rang & Dale's Pharmacology 7E,

THEORIES OF GENERAL ANAESTHESIA
•Earlier theories of anaesthesia postulated interaction with the lipid membrane bilayer General anaesthetic potency is closely correlated with lipid solubility.
•Recent work favours interaction with membrane ion channels and receptors.
Most anaesthetics enhance the activity of inhibitory GABAA receptors. Other important effects are the activation of a subfamily of potassium channels (the two-pore domain K+ channels, reducing membrane excitability) and inhibition of excitatory NMDA receptors.

•Anaesthesia involves three main changes: unconsciousness, loss of response to painful stimulation and loss of reflexes (motor and autonomic)
•At supra-anaesthetic doses, all anaesthetic agents can cause death by loss of cardiovascular reflexes and respiratory paralysis.
Pharmacological effects of anaesthetic agents
•At the cellular level, anaesthetic agents affect synaptic transmission and neuronal excitability rather than axonal conduction.

Stage 1 - The "induction„ stageBefore loss of consciousness.
During this stage, the patient progresses from analgesia without amnesia to analgesia with amnesia. Patients can carry on a conversation at this time.
Stage 2 - The "excitement“ stageFollowing loss of consciousness , marked by excited and delirious activity.
During this stage, respirations and heart rate may become irregular. In addition, there may be uncontrolled movements, vomiting, breath holding. This may lead to airway compromise.Therefore rapidly acting drugs are used to minimize this stage.
Stages of anaesthesia
Stage 3 - "surgical anaesthesia„The patient is unconscious, with surgical anaesthesia, spontaneously breathing and ready for surgery.
It has been divided into 4 planes:
•eyes initially rolling, then becoming fixed•loss of corneal and laryngeal reflexes•pupils dilate and loss of light reflex•intercostal paralysis, shallow abdominal respiration
Stage 4 - "overdose„A cessation of respiration and potential cardiovascular collapse. This stage is lethal without cardiovascular and respiratory support.
Stages of anaesthesia (contd)

Even the fastest-acting inhalation anaesthetics take a few minutes to act and cause a period of excitement before anaesthesia is induced.
Intravenous anaesthetics act more rapidly, producing unconsciousness in about 20 s, as soon as the drug reaches the brain from its site of injection.
Therefore, intravenous anaesthetics are normally used for induction of anaesthesia.

Characteristics Induction/recovery Main adverse effects and disadvantages
Propofol Widely usedHas largely replaced thiopentaluseful for day-case surgery
Fast Cardiovascular and respiratory depression(hypotension and bradycardia)
Thiopental Still often used Fast induction, slow recovery (accumulation occurs, giving slow recovery)'Hangover'
Cardiovascular and respiratory depressionnarrow margin between anaesthetic dose and dose causing cardiovascular depression
Midazolam Little respiratory or cardiovascular depression
Slower than other agents
Few adverse effects
Etomidate Less cardiovascular and respiratory depression than with thiopental
Fast Excitatory effects during induction and recovery,risk of adrenocortical suppression
Ketamine Produces good analgesia and amnesia, produces 'dissociative' anaesthesia, in which the patient may remain conscious although amnesic and insensitive to pain
Slow Psychotomimetic effects (e.g.hallucinations) following recoveryPostoperative nausea, vomiting and salivationCan raise intracranial pressure
Intravenous anaesthetics
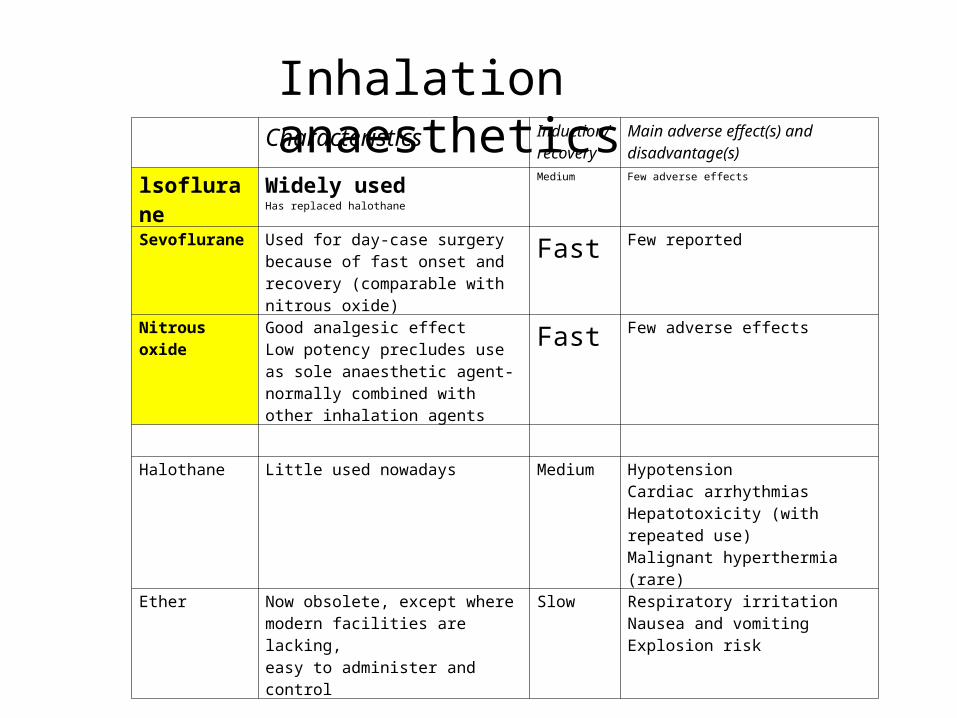
Characteristics Induction/recovery
Main adverse effect(s) and disadvantage(s)
lsoflurane Widely usedHas replaced halothane
Medium Few adverse effects
Sevoflurane Used for day-case surgery because of fast onset and recovery (comparable with nitrous oxide)
Fast Few reported
Nitrous oxide Good analgesic effectLow potency precludes use as sole anaesthetic agent-normally combined with other inhalation agents
Fast Few adverse effects
Halothane Little used nowadays Medium HypotensionCardiac arrhythmiasHepatotoxicity (with repeated use)Malignant hyperthermia (rare)
Ether Now obsolete, except where modern facilities are lacking,easy to administer and control
Slow Respiratory irritationNausea and vomitingExplosion risk
Inhalation anaesthetics

Relief from anxiety – benzodiazepines p.o.
Reduction of secretion (bronchial secretion) and vagal reflexes (bradycardia)
atropin i.m. or s.c.
PREMEDICATION:

neuromuscular-blocking drugs atracurium (vs neostigmin), suxamethonium (succinylcholin)opioid analgesics sufentanyl, fentanyl
antihypertensives to treat high blood pressure, ephedrine to treat low blood pressure, salbutamol to treat asthma or
laryngospasm/brochospasm epinephrine or antihistaminics to treat allergic
reactions,glucocorticoids or antibiotics to prevent inflammation and infection
PERIOPERATIVE MEDICATION

Analgesicsopioid and/or nonopioid
Antiemeticsmetoclopramide, ondansetron.
POSTOPERATIVE MEDICATION

•Intravenous anaesthetics are used for:- induction of anaesthesia (e.g. propofol or thiopental)- maintenance of anaesthesia throughout surgery ('total intravenous anaesthesia', e.g. propofol sometimes in combination with muscle relaxants and analgesics).
•Inhalational anaesthetics (gases or volatile liquids) are used for maintenance of anaesthesia.
Points to note are that:- volatile anaesthetics (e.g. isoflurane, sevoflurane) are delivered in air, oxygen or oxygen-nitrous oxide mixtures as the carrier gas- nitrous oxide must always be given with oxygen- because of its potential for inducing hepatotoxicity, halothane has largely been replaced by newer volatile anaesthetics such as isofluraneall inhalational anaesthetics can trigger malignant hyperthermia
Clinical uses of general anaethetics

Local anaesthetics

•Local anaesthetics block action potential generation by blocking sodium channels.
•Local anaesthetics are weak bases that must reach their site of action by penetrating the membrane as unionised species.
Action of local anaesthetics

Local anaesthetics are either esters or amides.
cocaine, procaine, tetracaine, benzocaine
lidocaine, trimecaine, articaine, bupivacaine
Esters are rapidly hydrolysed by plasma and tissue esterases while amides are less rapidly metabolised in the liver.
Local anaesthetic molecules consist of an aromatic part linked by an ester or amide bond to a basic side-chain :
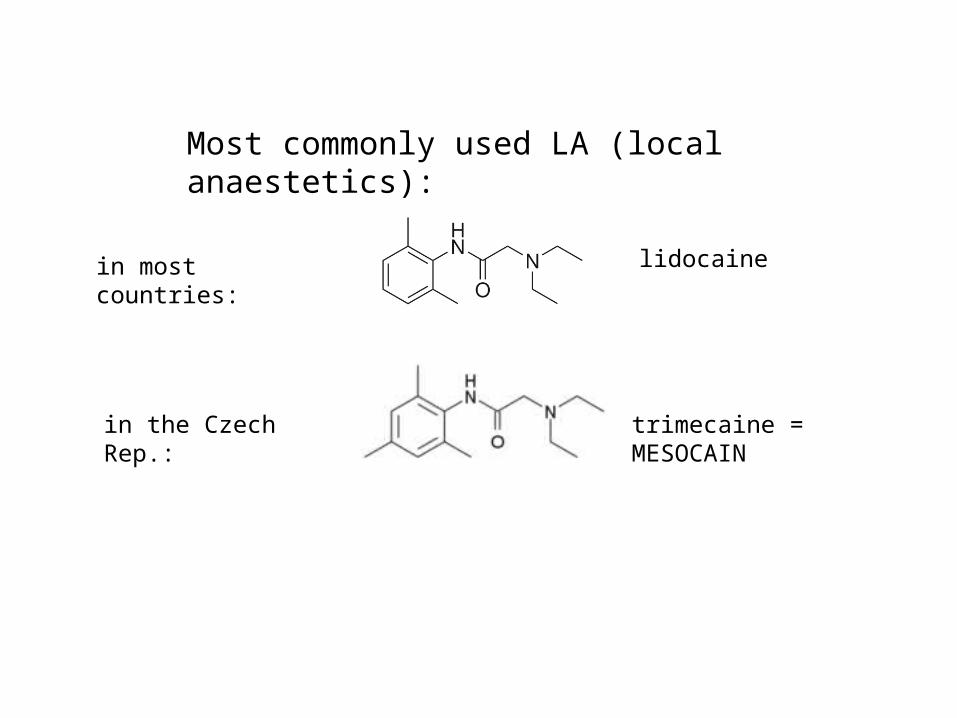
trimecaine = MESOCAIN
lidocaine
Most commonly used LA (local anaestetics):
in most countries:
in the Czech Rep.:
Local anaesthetic activity is increased at alkaline extracellular pH (i.e. when the proportion of ionised molecules is low) and reduced at acid pH.
Local anaaesthetic needs to penetrate the nerve membrane to reach the inner end of the sodium channel (where the local anaesthetic-binding site resides). Because the ionised form is not membrane permeant, penetration is very poor at acid pH.
This pH dependence can be clinically important, because inflamed tissues are often acidic and thus somewhat resistant to local anaesthetic agents.
Most local anaesthetics are weak bases. Therefore, their local anaesthetic activity is strongly pH dependent:

Main unwanted effects are:-central nervous system effects, agitation, confusion, tremors progressing to convulsions and respiratory depression
-cardiovascular effects, namely myocardial depression and vasodilatation, leading to fall in blood pressure
- occasional hypersensitivity reactions
UNWANTED EFFECTS of LA are due mainly to escape of local anaesthetics into the systemic circulation.
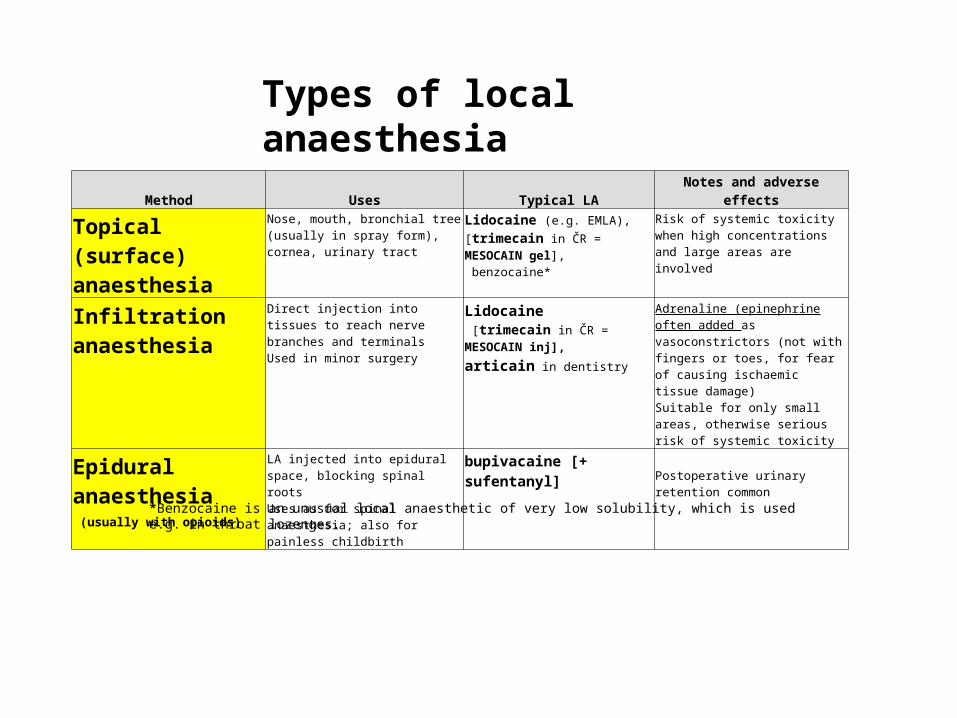
Method Uses Typical LA Notes and adverse effects
Topical (surface) anaesthesia
Nose, mouth, bronchial tree (usually in spray form), cornea, urinary tract
Lidocaine (e.g. EMLA),
[trimecain in ČR = MESOCAIN
gel], benzocaine*
Risk of systemic toxicity when high concentrations and large areas are involved
Infiltration anaesthesia
Direct injection into tissues to reach nerve branches and terminalsUsed in minor surgery
Lidocaine [trimecain in ČR = MESOCAIN
inj],
articain in dentistry
Adrenaline (epinephrine often added as vasoconstrictors (not with fingers or toes, for fear of causing ischaemic tissue damage)Suitable for only small areas, otherwise serious risk of systemic toxicity
Epidural anaesthesia (usually with opioids)
LA injected into epidural space, blocking spinal rootsUses as for spinal anaesthesia; also for painless childbirth
bupivacaine [+ sufentanyl]Postoperative urinary retention common
Types of local anaesthesia
*Benzocaine is an unusual local anaesthetic of very low solubility, which is used e.g. in throat lozenges.
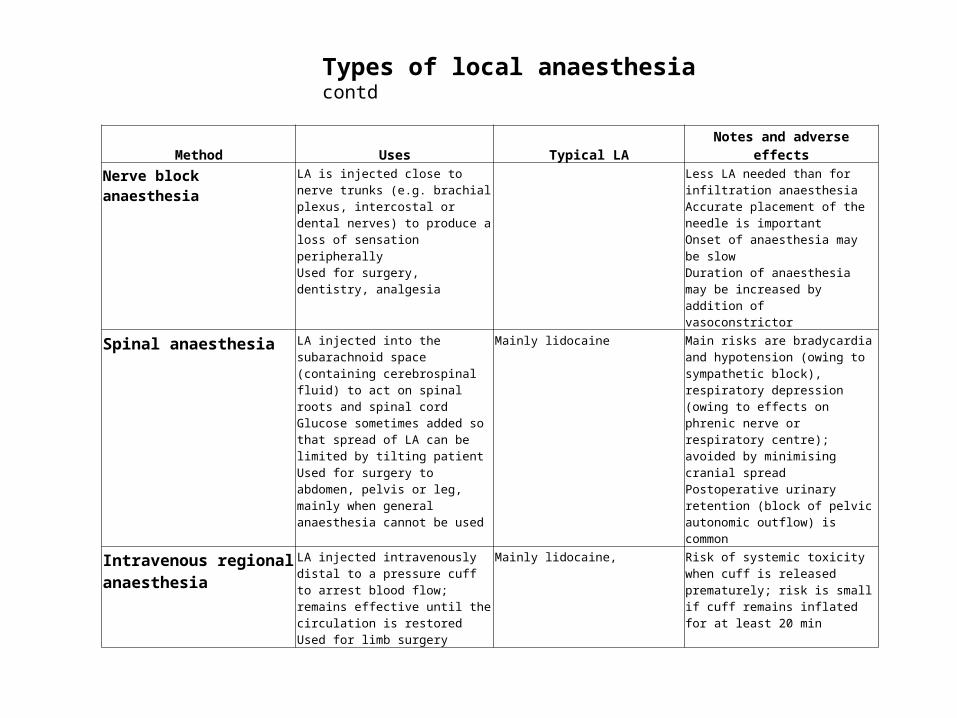
Method Uses Typical LA Notes and adverse effects
Nerve block anaesthesia LA is injected close to nerve trunks (e.g. brachial plexus, intercostal or dental nerves) to produce a loss of sensation peripherallyUsed for surgery, dentistry, analgesia
Less LA needed than for infiltration anaesthesiaAccurate placement of the needle is importantOnset of anaesthesia may be slowDuration of anaesthesia may be increased by addition of vasoconstrictor
Spinal anaesthesia LA injected into the subarachnoid space (containing cerebrospinal fluid) to act on spinal roots and spinal cordGlucose sometimes added so that spread of LA can be limited by tilting patientUsed for surgery to abdomen, pelvis or leg, mainly when general anaesthesia cannot be used
Mainly lidocaine Main risks are bradycardia and hypotension (owing to sympathetic block), respiratory depression (owing to effects on phrenic nerve or respiratory centre); avoided by minimising cranial spreadPostoperative urinary retention (block of pelvic autonomic outflow) is common
Intravenous regional anaesthesia
LA injected intravenously distal to a pressure cuff to arrest blood flow; remains effective until the circulation is restoredUsed for limb surgery
Mainly lidocaine, Risk of systemic toxicity when cuff is released prematurely; risk is small if cuff remains inflated for at least 20 min
Types of local anaesthesia contd
