anatomy arteries in transposition ofthe methods for in · anatomyofthecoronaryarteriesin...
TRANSCRIPT

Thorax, 1978, 33, 418-424
Anatomy of the coronary arteries in transpositionof the great arteries and methods for their transferin anatomical correctionMAGDI H YACOUB AND ROSEMARY RADLEY-SMITH
From Harefield Hospital, Middlesex, and the National Heart Hospital, London, UK
Yacoub, M I, and Radley-Smith, R (1978). Thorax, 33, 418-424. Anatomy of the coronary
arteries in transposition of the great arteries and methods for their transfer in anatomicalcorrection. For the success of anatomical correction of transposition of the great arteries (TGA)it is essential to transfer the coronary ostia to the posterior vessel without undue tension, torsion,or kinking of the proximal coronary arteries or their early branches. This requires thoroughunderstanding of the different modes of origin and early branching of the coronary arteries inTGA. Based on observations made during anatomical correction, a classification of the coronaryarteries in TGA is suggested. In type A the right and left coronary ostia arise from the middleof the right and left posterior aortic sinuses and curve forwards to reach the right atrioventriculargroove or anterior interventricular groove respectively. In type B both coronary arteries arise bya single ostium, while in type C the two coronary ostia are situated posteriorly, very close to eachother, in a position similar to that in type B. The origin of the coronary arteries in type D issimilar to that of type A. However, the right coronary artery gives origin to the circumflexcoronary artery that curves round the posterior (pulmonary) vessel to reach the atrioventriculargroove. In type E the right coronary artery arises in common with the left anterior descendingartery from the left posterior sinus, while the circumflex artery arises separately from the rightposterior sinus. Three techniques for the transfer of the different types of coronary arteriesduring anatomical correction are described.
Although anatomical correction of transpositionof the great arteries (TGA) is the logical andobvious method for treatment of this condition, itssuccessful application has been delayed until veryrecently (Jatene et al, 1976; Ross et al, 1976;Yacoub et al, 1976). This delay is partly due to thetechnical difficulties of transferring the coronaryostia, because these vary in position and courseand are closely related to the aortic valve. Forthe success of the operation it is essential to avoidundue tension, torsion, or kinking of the maincoronary arteries or their early branches. This canbe achieved only by a thorough understanding ofthe different modes of origin, early course, andbranching of the coronary arteries in TGA. Weshall attempt to define the different anatomicaltypes of coronary arteries in TGA and to describemethods for transfer of each type.
Material and methods
The anatomy of the coronary arteries wasexamined during operation for TGA both beforeand, whenever possible, after transection of theaorta in 18 patients in an attempt to characterise:(1) The location of each coronary ostium and itsrelation to the sinuses and commissures of theaortic and pulmonary valves.(2) The course, direction, and length of the maincoronary artery before branches are given off.(3) The mode of origin and course of the earlybranches.
ANATOMICAL TYPES OF CORONARY ARTERIES IN TGAUsing the criteria mentioned above, the followinganatomical types could be identified.
418
on 9 April 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.33.4.418 on 1 A
ugust 1978. Dow
nloaded from
Anatomy of the coronary arteries in transposition of the great arteries
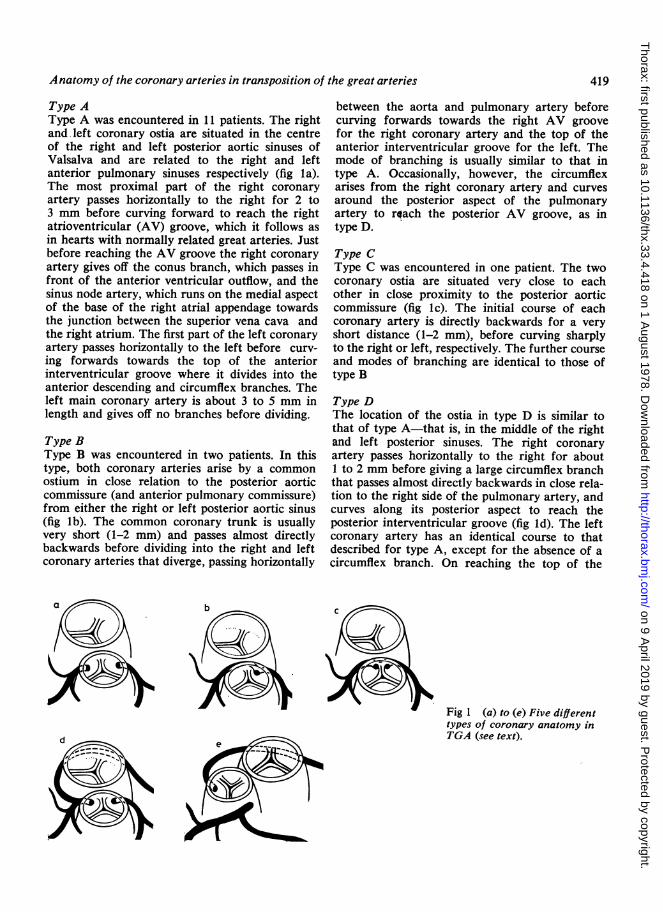
Type AType A was encountered in 11 patients. The rightand left coronary ostia are situated in the centreof the right and left posterior aortic sinuses ofValsalva and are related to the right and leftanterior pulmonary sinuses respectively (fig la).The most proximal part of the right coronaryartery passes horizontally to the right for 2 to3 mm before curving forward to reach the rightatrioventricular (AV) groove, which it follows asin hearts with normally related great arteries. Justbefore reaching the AV groove the right coronaryartery gives off the conus branch, which passes infront of the anterior ventricular outflow, and thesinus node artery, which runs on the medial aspectof the base of the right atrial appendage towardsthe junction between the superior vena cava andthe right atrium. The first part of the left coronaryartery passes horizontally to the left before curv-ing forwards towards the top of the anteriorinterventricular groove where it divides into theanterior descending and circumflex branches. Theleft main coronary artery is about 3 to 5 mm inlength and gives off no branches before dividing.
Type BType B was encountered in two patients. In thistype, both coronary arteries arise by a commonostium in close relation to the posterior aorticcommissure (and anterior pulmonary commissure)from either the right or left posterior aortic sinus(fig lb). The common coronary trunk is usuallyvery short (1-2 mm) and passes almost directlybackwards before dividing into the right and leftcoronary arteries that diverge, passing horizontally
b
between the aorta and pulmonary artery beforecurving forwards towards the right AV groovefor the right coronary artery and the top of theanterior interventricular groove for the left. Themode of branching is usually similar to that intype A. Occasionally, however, the circumflexarises from the right coronary artery and curvesaround the posterior aspect of the pulmonaryartery to roach the posterior AV groove, as intype D.
Type CType C was encountered in one patient. The twocoronary ostia are situated very close to eachother in close proximity to the posterior aorticcommissure (fig lc). The initial course of eachcoronary artery is directly backwards for a veryshort distance (1-2 mm), before curving sharplyto the right or left, respectively. The further courseand modes of branching are identical to those oftype B
Type DThe location of the ostia in type D is similar tothat of type A-that is, in the middle of the rightand left posterior sinuses. The right coronaryartery passes horizontally to the right for about1 to 2 mm before giving a large circumflex branchthat passes almost directly backwards in close rela-tion to the right side of the pulmonary artery, andcurves along its posterior aspect to reach theposterior interventricular groove (fig ld). The leftcoronary artery has an identical course to thatdescribed for type A, except for the absence of acircumflex branch. On reaching the top of the
Fig 1 (a) to (e) Five differenttypes of coronary anatomy inTGA (see text).
419
on 9 April 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.33.4.418 on 1 A
ugust 1978. Dow
nloaded from
Magdi H Yacoub and Rosemary Radley-Smith
anterior interventricular groove, the vessel con-tinues as the anterior descending artery. Thistype was encountered in three patients.
Type EType E appears to be a rare type that was en-countered in one patient in this series. The cir-cumflex artery arises from the right posteriorsinus and its further course is identical to thatdescribed in type D. Another coronary trunkarises from the anterior part of the left posteriorsinus and passes forward for 2 mm before dividinginto the right main and left anterior descendingarteries (fig le). The right coronary artery passesin front of the outflow tract of the anteriorventricle to reach the right atrioventricular groove.This type was associated with a different relation-ship of the great arteries that were almost side byside, with the aorta to the right and slightlyanterior. In addition, the mode of origin of theaorta from the anterior ventricle was unusual,arising from a recess to the right of the outflowtract, which ended blindly. The relation of theaortic valve to the tricuspid was similar to thatencountered in double outlet right ventricle withd-malposition of the great arteries.
TECHNIQUES FOR CORONARY TRANSFERThree techniques were evolved for transfer of thedifferent anatomical types of coronary arteries.
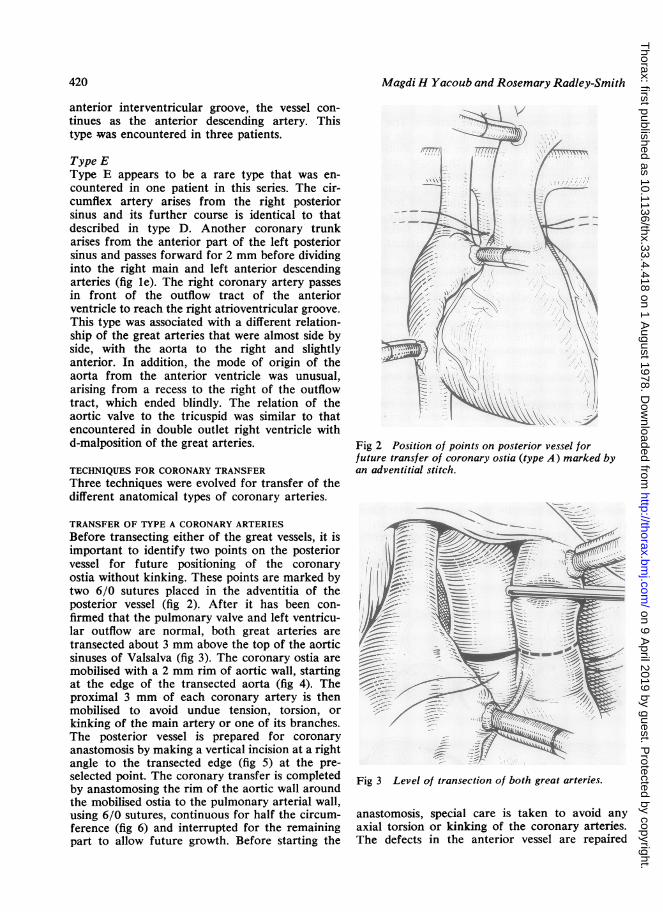
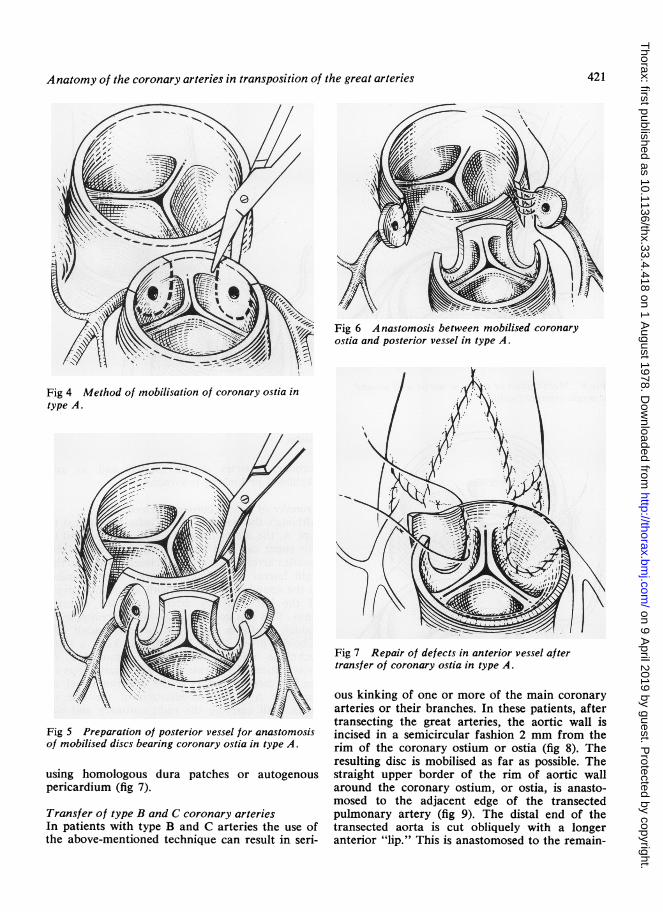
TRANSFER OF TYPE A CORONARY ARTERIESBefore transecting either of the great vessels, it isimportant to identify two points on the posteriorvessel for future positioning of the coronaryostia without kinking. These points are marked bytwo 6/0 sutures placed in the adventitia of theposterior vessel (fig 2). After it has been con-firmed that the pulmonary valve and left ventricu-lar outflow are normal, both great arteries aretransected about 3 mm above the top of the aorticsinuses of Valsalva (fig 3). The coronary ostia aremobilised with a 2 mm rim of aortic wall, startingat the edge of the transected aorta (fig 4). Theproximal 3 mm of each coronary artery is thenmobilised to avoid undue tension, torsion, orkinking of the main artery or one of its branches.The posterior vessel is prepared for coronaryanastomosis by making a vertical incision at a rightangle to the transected edge (fig 5) at the pre-selected point. The coronary transfer is completedby anastomosing the rim of the aortic wall aroundthe mobilised ostia to the pulmonary arterial wall,using 6/0 sutures, continuous for half the circum-ference (fig 6) and interrupted for the remainingpart to allow future growth. Before starting the
I1
I'K\
Fig 2 Position of points on posterior vessel forfuture transfer of coronary ostia (type A) marked byan adventitial stitch.
Fig 3 Level of transection of both great arteries.
anastomosis, special care is taken to avoid anyaxial torsion or kinking of the coronary arteries.The defects in the anterior vessel are repaired
420
on 9 April 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.33.4.418 on 1 A
ugust 1978. Dow
nloaded from
Anatomy of the coronary arteries in transposition of the great arteries
Fig 6 A nastomosis between mobilised coronaryostia and posterior vessel in type A.
Fig 4 Method of mobilisation of coronary ostia intype A.
Fig 7 Repair of defects in anterior vessel aftertransfer of coronary ostia in type A.
Fig 5 Preparation of posterior vessel for anastomosisof mobilised discs bearing coronary ostia in type A.
using homologous dura patches or autogenouspericardium (fig 7).
Transfer of type B and C coronary arteriesIn patients with type B and C arteries the use ofthe above-mentioned technique can result in seri-
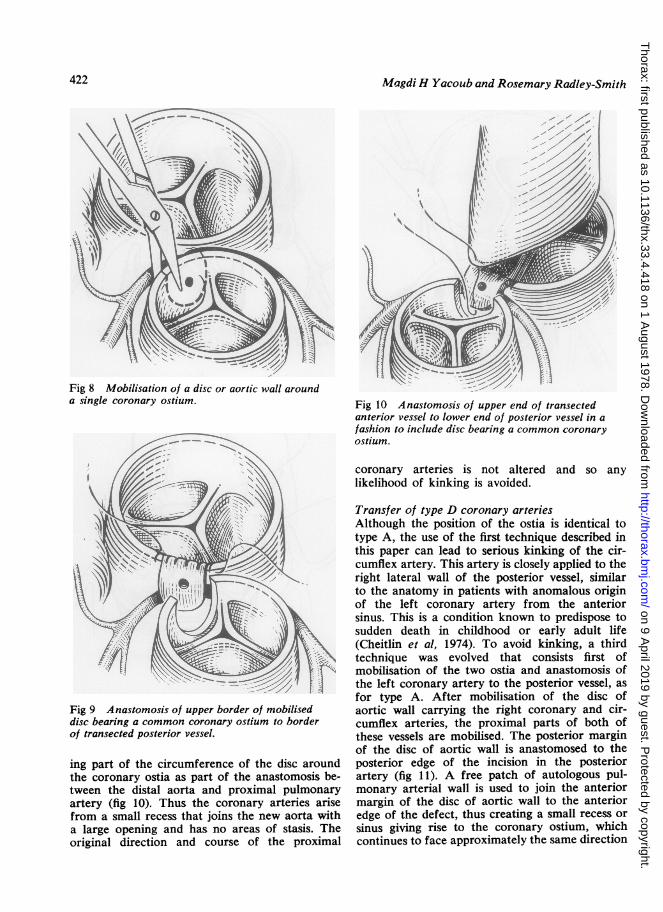
ous kinking of one or more of the main coronaryarteries or their branches. In these patients, aftertransecting the great arteries, the aortic wall isincised in a semicircular fashion 2 mm from therim of the coronary ostium or ostia (fig 8). Theresulting disc is mobilised as far as possible. Thestraight upper border of the rim of aortic wallaround the coronary ostium, or ostia, is anasto-mosed to the adjacent edge of the transectedpulmonary artery (fig 9). The distal end of thetransected aorta is cut obliquely with a longeranterior "lip." This is anastomosed to the remain-
421
on 9 April 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.33.4.418 on 1 A
ugust 1978. Dow
nloaded from
Magdi H Yacoub and Rosemary Radley-Smith
Fig 8 Mobilisation of a disc or aortic wall arounda single coronary ostium. Fig 10 Anastomosis of upper end of transected
anterior vessel to lower end of posterior vessel in afashion to include disc bearing a common coronary
- - ostium.
Fig 9 Anastomosis of upper border of mobiliseddisc bearing a common coronary ostium to borderof transected posterior vessel.
ing part of the circumference of the disc aroundthe coronary ostia as part of the anastomosis be-tween the distal aorta and proximal pulmonaryartery (fig 10). Thus the coronary arteries arisefrom a small recess that joins the new aorta witha large opening and has no areas of stasis. Theoriginal direction and course of the proximal
coronary arteries is not altered and so anylikelihood of kinking is avoided.
Transfer of type D coronary arteriesAlthough the position of the ostia is identical totype A, the use of the first technique described inthis paper can lead to serious kinking of the cir-cumflex artery. This artery is closely applied to theright lateral wall of the posterior vessel, similarto the anatomy in patients with anomalous originof the left coronary artery from the anteriorsinus. This is a condition known to predispose tosudden death in childhood or early adult life(Cheitlin et al, 1974). To avoid kinking, a thirdtechnique was evolved that consists first ofmobilisation of the two ostia and anastomosis ofthe left coronary artery to the posterior vessel, asfor type A. After mobilisation of the disc ofaortic wall carrying the right coronary and cir-cumflex arteries, the proximal parts of both ofthese vessels are mobilised. The posterior marginof the disc of aortic wall is anastomosed to theposterior edge of the incision in the posteriorartery (fig 11). A free patch of autologous pul-monary arterial wall is used to join the anteriormargin of the disc of aortic wall to the anterioredge of the defect, thus creating a small recess orsinus giving rise to the coronary ostium, whichcontinues to face approximately the same direction
422
on 9 April 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.33.4.418 on 1 A
ugust 1978. Dow
nloaded from

Anatomy of the coronary arteries in transposition of the great arteries
Fig 11 Technique for transfer of type C coronaryvessels. To avoid kinking of circumflex artery, a freepatch "P" of autogenous pulmonary artery is used tojoin anterior edge of disc to the anterior edge ofdefect created in posterior wall.
as before so preventing kinking of the circumflexartery (fig 11). In addition, this technique avoidsundue tension on the circumflex artery and itsostium when the future aorta dilates duringexercise.
Discussion
Although the basic abnormality in complete, ord-transposition of the great arteries is the originof the aorta and coronary arteries from morpho-logical right (anterior) ventricle, and the pul-monary artery from the morphological left(posterior) ventricle, the only available methodfor treating these patients, until recently, hasbeen by atrial septostomy followed by inflow "cor-rection" by the Mustard or Senning operation(Senning, 1959; Mustard, 1964). These operationshave given good early and moderately lateresults (Breckenbridge et al, 1972), but they are
not corrective, as the right ventricle continues toserve the systemic circulation, and there is some
concern about the incidence of late arrhythmias(El Said et al, 1972), tricuspid regurgitation(Tynan et al, 1972), and pulmonary or systemicvenous obstruction (Stark et al, 1972). The idealoperation, in theory, should consist of transposingthe aorta and pulmonary arteries to their appro-
priate ventricles and resiting the coronary arteries.This corrective procedure is still not widely used.Difficulties in applying this operation are becausein patients with intact ventricular septum regres-
sion of pulmonary vascular resistance after birthresults in rapid regression of left ventricular mass,rendering it incapable of supporting the systemiccirculation (Tynan, 1972; British Medical Journal,1976); added to this are the technical difficultiesof transferring the coronary arteries to theposterior vessel at a very young age. It ispossible to redevelop the posterior ventricle inpatients with intact ventricular septum by per-forming a first-stage operation consisting of band-ing the pulmonary artery and creating anaortopulmonary shunt proximal to the band(Yacoub et al, 1977). The technical difficulties oftransferring the coronary arteries can be solvedonly by accurate characterisation of the differentanatomical types. We have described five types ofcoronary artery anatomy and methods for thetransfer of each type. These methods are designedto avoid undue tension, torsion, or kinking of themain coronary arteries and their early branches.We hope that the anatomical classification andsurgical techniques described here will beof some value in helpina to establish the role ofanatomical correction in the management ofpatients with complete transposition of the greatarteries.
References
Breckenbridge, I M, Oelert, H, Stark, J, Graham,G R, Bonham-Carter, R E, and Waterston, D J(1972). Mustard's operation for transposition of thegreat arteries. A review of 200 cases. Lancet, 1,1140-1142.
British Medical Journal (1976). Transposition of thegreat arteries. British Medical Journal, 1, 1104-1105.
Cheitlin, M D, De Castro, C M, McAllister, H A(1974). Sudden death as a complication of anomal-ous left coronary origin from the anterior sinus ofValsalva. Circulation, 50, 780-787.
El Said, G, Rosenberg, H S, Mullins, C E, Hallman,G L, Cooley, D A, and McNamara, D G (1972).Dysrhythmias after Mustard's operation for trans-position of the great arteries. American Journal ofCardiology, 30, 526-532.
Jatene, A D, Fontes, V E, Paulista, P P, Souza,L C B, Negaer, F, Galantier, M, Sousa, J E M R(1976). Anatomical correction of transposition ofthe great vessels. Journal of Thoracic and Cardio-vascular Surgery, 72, 364-370.
Mustard, W T (1964). Successful two-stage correctionof transposition of the great vessels. Surgery, 55,469-472.
Ross, D, Rickards, A, Somerville, J (1976). Trans-position of the great arteries; logical anatomicalarterial correction. British Medical Journal, 1, 1109-1111.
Senning, A (1959). Surgical correction of transposition
423
on 9 April 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.33.4.418 on 1 A
ugust 1978. Dow
nloaded from

424 Magdi H Yacoub and Rosemary Radley-Smith
of the great vessels. Surgery, 45, 966-980. Anatomical correction of complete transposition ofStark, J, Tynan, M J, Ashcraft, K W, Aberdeen, E, the great arteries and ventricular septal defect inand Waterston, D J (1972). Obstruction of pul- infancy. British Medical Journal, 1, 1112-1114.monary veins and superior vena cava after Mustard's Yacoub, M H, Radley-Smith, R, Maclaurin, R (1977).operation for transposition of the great arteries. Two-stage operation for anatomical correction ofCirculation, 46, Supp 1, 116-120. transposition of the great arteries with intact inter-
Tynan, M, Aberdeen, E, and Stark, J (1972). Tricuspid ventricular septum. Lancet, 1, 1275-1278.incompetence after Mustard's operation for trans-position of the greater arteries. Circulation, 45,Supp 1, 111-116. Requests for reprints to: M H Yacoub, 24 Upper
Yacoub, M H, Radley-Smith, R, Hilton, C J (1976). Wimpole Street, London WIM 7TA.
on 9 April 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.33.4.418 on 1 A
ugust 1978. Dow
nloaded from