annual report 2009. leprosy mission nepal
DESCRIPTION
The 2009 Annual Report for the Leprosy Mission Nepal.TRANSCRIPT
Annual Report2009
LeprosyMissionNepal

Conte
nts
Te:l +977-1-4290545Email: [email protected]. tlmnepal.org
Anandaban Hospital,PO Box 151,Kathmandu, Nepal
Contact Anandaban Hospital
2
4
10
30
12
34
26
36
6 8
From the ED
Leprosy Basics
Labs
Anandaban
Clinical Dept
Training
Finances
Stories
Community Work
Cover Image: Ram Bahadur Thami and his wife Muni (see Stories section)
After being stranded in Kathmandu because of the 2010 Iceland Volcano eruption the kind people of
Anandaban Hospital put me up for an extra week. Allowing me to design this 2009 Annual Report.
Thanks Anandaban staff and patients, for being a great encoragement to myself.
God bless. Adam Howson. Email: [email protected]

A WORLD WITHOUT LEPROSY
Our VisionNepal without leprosy or other disabling conditions
Our GoalTo prevent disabilities or to restore and optimise function for people who have
experienced activity or limitation or participation restrictions as affects of
leprosy or trauma.
Our MissionTo work with communities disadvantaged by leprosy and other
disabling conditions; sharing the love of Jesus Christ through actions
to heal and restore dignity.
Our
Vis
ion
3
Cover Image: Ram Bahadur Thami and his wife Muni (see Stories section)

It is a great pleasure to have this opportunity to share with you about some of the major achievements of the Leprosy Mission Nepal (LMN) over the last twelve months towards transforming the lives of people affected by leprosy.
Elimination of LeprosyIn 2009 the Government of Nepal announced that the country had achieved the “elimination of lep-rosy”. This is a wonderful outcome resulting from the joint effort and contributions of many people at all levels to the national leprosy control program. When the Leprosy Mission Nepal began its program of additional technical support to the national leprosy control program the number of cases of leprosy in the Central Region of Nepal was very high. By working together we were able to bring the prevalence rate down to the level of elimination. Our work has not however come to an end. There are still many people in the community yet to be diagnosed, as well as people with disabilities related to leprosy who require ongoing care and services. Furthermore the Government of Nepal and the I/NGOs are now
focused on developing and imple-menting relevant and effective post elimination strategies to address the remaining challenges of leprosy and to see our ultimate goal achieved, that of eradicating the causes and consequences of leprosy in Nepal.
Meeting the needDespite the political instability and challenges in the country, the Leprosy Mission Nepal was able to meet the needs of more than 30,000 people throughout the work of Anandaban Hospital and many more people throughout its activities in the community. Anandaban Hos-pital, as a centre of excellence, has been delivering all types of medical,
From
the
Exec
utive
Direc
tors
Des
k
Shovakhar sheds some light
“Leprosy Mission Nepal was able to meet the needs of more than 30,000 people throughout the work of Anandaban.”
4

surgical and physical rehabilitation care to improve the quality of life of people affected by leprosy in Nepal and northern India as well. We have made significant progress in reducing readmissions through-out proper management of ulcers, reactions and self care teaching in the hospital. Our work is not only limited to the hospital, but we are also going out to the community through our satellite clinics, medical and surgical camps to ensure that basic leprosy services are available in the remote areas, especially to those who cannot afford to come to the hospital. Our expert reconstructive surgery team has also travelled to other regions of Nepal to offer their services to people in need and to im-part their skills to local doctors.
Five year strategic planOne of our major achievements has been the development of the hos-pital’s five-year strategic plan which
will guide us in our future work. Through this strategy we remain committed towards delivering qual-ity leprosy services and to expand-ing our orthopaedic and trauma related services in the hospital, thus enabling us to become financially self sufficient.
ResearchResearch has been an area of com-mitment of the Leprosy Mission in 2009 also. The team worked very hard to conclude the Skin Test Clinical Trial, in collaboration with Colorado State University, USA, alongside other research commit-ments. We are eagerly waiting to know the outcome of this study. We have been able to replace some old equipment and begin necessary renovation work done to provide a favourable environment to maintain international research standards. Our research laboratory facilities are also used for training research and
health professional students from across Nepal and abroad, in leprosy and research procedures.In 2005, through a small scale pilot program, we began to implement community based rehabilitation ac-tivities for people affected by leprosy. This was new work for us at the time. From this program came the vision of a bigger integrated community based program for people affected by leprosy and people with physical disabilities from marginalised com-munities. It was therefore with great excitement that in 2009 we launched the Community Empowerment De-velopment, Disability and Rehabilita-tion (CEDAR) and Socio-Economic Re-habilitation (SER) Projects. In a short period of time we have established very meaningful working partner-ships with the concerned authorities in the project areas. We are very thankful to the Lord for providing such a committed team to work with these projects.
Mr. Shovakhar Kandel, Sushil Khatiwada, Aathen Rongong and Hira Shrestha
5

When a patient first comes to Anandaban, an experienced clinician will discuss symptoms and evaluate the patient as a whole. The diag-nostic lab will test for the presence of leprosy bacteria in their skin, enabling the clinician to prescribe the proper dosages of medication. The physiotherapy department will evaluate nerve function in their eyes, hands and feet – carefully map-ping where sensation and function may have already been lost. Nurses dress and tend their wounds. If necessary, a surgeon will evaluate to determine if reconstruc-tive surgery is possible to reverse some of the effects.
The prosthetics and footwear department will assess their needs for customized shoes or prosthetic devices to help prevent or delay further injury development. A counselor will listen to the patient, help them to face their diag-
nosis and provide caring support on their journey to independent, healthy living. After immediate health issues are met, other teams are available within the Self-Care Unit to train in Prevention of Dis-ability methods in a Nepali-styled home setting. How can everyday farming tools be adjusted to re-duce injury to disabled or insen-sate hands? What methods should
Quick Tour of Anandaban
6
Anan
dab
an

vide empowerment for sustainability through education scholarships to leprosy-affected children, low cost housing and/or microloans to affected families to enable income generation and escape from the desperate poverty in which so many dwell.
The research lab will request volun-tary participation in ongoing leprosy
studies, so that future patients can benefit by what we can learn from today’s patients. All the while, the Training Unit hosts a steady flow of clini-cians, nurses, govern-ment and other health professionals in lep-rosy training programs utilizing experienced Anandaban staff and patients to increase awareness, proper di-agnosis and treatment across Nepal.
be added to daily routine home life for proper foot, eye and hand care?
Another team will assess patients for programs such as Socio-Economic Rehabilitation (SER) and Community Empowerment, Development, Disability and Rehabilitation (CEDAR) that will help to enable them to live on their own, participating in their communities. These programs pro-
Leprosy in NepalDuring 2009, the World Health Organizaton (WHO) declared lep-rosy eliminated in Nepal, a policy statement which means that <1 per 10,000 people in Nepal were registered as actively receiving antibiotic treatment for leprosy at the end of the year. During that year 4565 new cases were registered. 16 districts are still reporting higher than the WHO target. Most new cases were men, as women con-tinue to report less (32% of cases) and later, when symptoms can no longer be hidden. Evidence of recent transmission, children represent 8% of new cases in Nepal. While low infections require 6 months of treatment, 49% of Nepal’s new cases carry denser leprosy infections that require 1-2 yrs of antibiotics treat-ment. The majority of Anandaban’s hospital-based caseload are referrals of cases complicated by reactions, relapse, recurring wounds, prosthet-ics and surgical needs. Therefore, our experienced team of surgeons and clinicians provide specialized care to leprosy patients from across Nepal.

The figures worked out
8
Finan
ces
Base Hospital ExpensesTraining UnitMycobacterial Research LabCEDAR ProjectCAP Project ProgrammeSocio Economic RehabilitationTotal Programme Cost
377,211.38 5958,729.08 958,850.99 55,632.67 68,477.4125,623.05 644,524.58
59%9%9%9%11%4%100%
Project ‘09 Expenditure (GBP) Ratio %

2009 Leprosy Mission Nepal Expenditure 58%
9%
9%
9%
4%
11%
9Wheat harvest in the valley below Anandaban Hospital
Ratio %
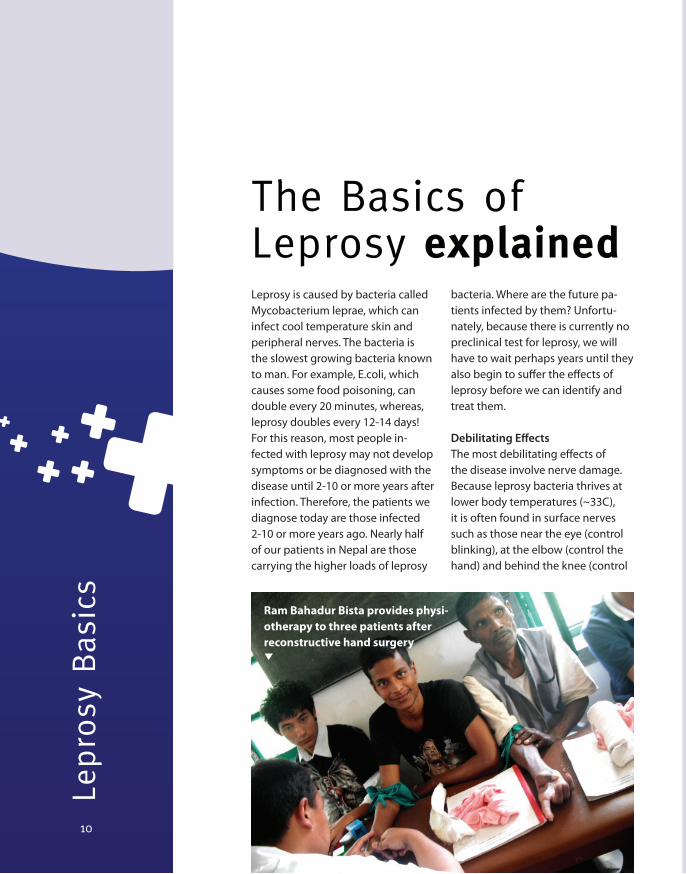
Leprosy is caused by bacteria called Mycobacterium leprae, which can infect cool temperature skin and peripheral nerves. The bacteria is the slowest growing bacteria known to man. For example, E.coli, which causes some food poisoning, can double every 20 minutes, whereas, leprosy doubles every 12-14 days! For this reason, most people in-fected with leprosy may not develop symptoms or be diagnosed with the disease until 2-10 or more years after infection. Therefore, the patients we diagnose today are those infected 2-10 or more years ago. Nearly half of our patients in Nepal are those carrying the higher loads of leprosy
bacteria. Where are the future pa-tients infected by them? Unfortu-nately, because there is currently no preclinical test for leprosy, we will have to wait perhaps years until they also begin to suffer the effects of leprosy before we can identify and treat them.
Debilitating EffectsThe most debilitating effects of the disease involve nerve damage. Because leprosy bacteria thrives at lower body temperatures (~33C), it is often found in surface nerves such as those near the eye (control blinking), at the elbow (control the hand) and behind the knee (control
The Basics of Leprosy explained
10
Lepro
sy B
asic
s
Ram Bahadur Bista provides physi-otherapy to three patients after reconstructive hand surgery

ence farmers, performing all work by hand. There is no option to change occupation due to disability. Eventually, a lesion or discolored patch of skin may form or the pa-tient may notice loss of sensation or pain associated with a nerve that is being damaged by leprosy infec-tion. Especially in rural areas (most of Nepal), leprosy patients can still face issues related to stigma. Leprosy diagnosis can cause rejection by spouse, family, communities and life-supporting employment. The majority of Anandaban’s patients are male. Females often do not come until they can no longer hide or deny their condition. By then, the nerve damage and other leprosy associ-ated problems can be substantial and irreversible.
Leprosy ReactionsAnandaban operates as the main referral center for complicated lepro-sy cases from across Nepal. Although a cocktail of antibiotic treatment can kill leprosy within the first few doses,
the foot). When these nerves begin to be irreversibly damaged, feeling and function can be lost. Cut off from communication with the rest of the body, muscles atrophy. Hands claw. Eyelids cease to blink. Feet no longer strike the ground properly. Muscles that support the foot arch
collapse. Placed under pressure they were never designed to bear, parts of the foot can wear ulcers to the bone while the patient may not even feel it. Nepal is a difficult place to live. Most Nepalese are subsist-
the bacterial corpses are made of a waxy substance that is not easily flushed from skin and nerve tissues. The dead bacteria can remain in skin and nerves for many years. The body may continue to fight with inflam-mation, swelling and fever called leprosy reactions that cause even further damage. Unpredictably, pa-tients can begin reacting with severe inflammation anywhere the leprosy bacteria are located. Leprosy reac-tions can occur before, during and even years after effective treatment is complete – requiring months of inpatient care. Reactions occur in 30-50% of leprosy cases and are a chief cause of morbidity and disability. Specialized clinicians experienced in leprosy reactions are required for complicated case management which can require months or even years of outpatient or recurring inpatient treatment. Steroids may cool inflammation briefly, but 50% of patients have recurrent reactions and repeated doses of steroids can induce other health problems.
“Most people affected with Leprosy may not develop the disease until 2-10 years after infection”
Bir Bahadur Tamang cleaning the wound of a patient.
11

Clinic
al
Dr Indra Napit with one of the patients12

Terai region as well. We also found that there was a need for outreach recon-structive surgery camps for patients from the Terai as they find it difficult to come to Kathmandu for surgery and to leave their families for several months. As such we conducted two such camps in government hospitals in 2009. We were able to perform one
camp in the Koshi Zonal hospital in East Nepal and another one in the Seti Zonal hospital in Far West Nepal in collaboration with the Netherlands Leprosy Relief. A total of 31 people affected by leprosy were operated on in these two camps. Another great achievement in 2009 was the regular visits of the hand surgeon Dr. Donald Sammut from the UK. His visits have
It has been two years since I joined Anandaban Hospital. It has been a great time for me to develop skills in leprosy work. The Government of Nepal declared the elimination of lep-rosy in November 2009. This does not mean however that there are no new cases of leprosy; it means that leprosy is no more a public health problem according to the WHO definition of elimination (less than 1 in 10,000). There are still new cases of leprosy diagnosed and there is a big need for holistic care for leprosy patients in a place like Anandaban Hospital, where patients can experience good care and love.
Given that most of the new cases of leprosy are from the Terai region of Nepal, in March 2009 Anandaban Hospital started a Satellite Clinic in Chandranigahapur in the district of Rautahat. Through this clinic we are providing free consultation and drugs for people affected by leprosy. New cases are diagnosed in this clinic every visit. A number of cases for reconstruc-tive surgery and rehabilitation are also referred from this clinic to Anandaban Hospital. We have come to realise that we may need to expand this type of outreach clinic to other districts of the
been a great opportunity for op-erations for many people requiring hand surgery and surgery to restore function following burn contractures of upper limbs, as well as a good learn-ing opportunity for all of the staff of Anandaban Hospital.
In 2009, as part of our newly developed strategic plan, we aimed to extend our general services for the local community. We were able to fulfill this aim by increasing the number of services on offer to people with trauma related injuries and increasing medical admissions. Our x-ray department now provides evening service. SIGN inter-locking IM nailing for femur and tibia fractures can now also be performed at Anandaban Hospital. This is the best and cheapest method of fracture treat-ment. We hope and pray that we will be able to continue our service to the people affected by leprosy for the long term and also to fulfill our strategic plan of extending our general services for the local community. I would like to thank all our prayer partners for their regular prayers and support to Anandaban Hospital.
Dr. Indra NapitMedical Director
A note from Dr.Indra
“I would like to thank all our prayer partners for their regular prayers and support to Anandaban Hospital”
13

1. Clinic Attendance2005 -2009 Total Clinic Attendances: Anandaban performs a weekly satel-lite leprosy clinic at a large hospital in Kathmandu. Patients come from the areas surrounding the valley for out-patient services and others are referrals from across Nepal. If a case needs inpatient care, we take them back to Anandaban with us.
2. Average Bed StaysAs a referral hospital, Anandaban receives complicated leprosy cases from all over Nepal. Reaction cases usually require a 2 month admission. Reconstructive tendon transfer sur-geries require 2 month stays to com-plete post-op physiotherapy. Some leprosy reactions and ulcer patients cases, however, are more difficult and require longer admissions.
3. Leprosy Case Admissions 2005-20092005-2009 Leprosy Case Admissions for Hospital Care: In 2009, there was a sharp increase in surgeries and surgical camps.
4. WHO Grade Disability for Anandaban Patients (2005-2009)The World Health Organization (WHO) uses a 3 grade scale for disability classifcation of patients. Grade 0 indicates no disability. Grade 1 indicates detectable nerve damage such as anesthesia but no outwardly visible signs of disability. Grade 2 indicates visible signs of disability (ie, clawed hands, inability to blink, foot drop).
Clinical department Statistics
Clinic
al
14Medical Records Department

Grade 0 44.5%Grade 1 17.2%Grade 2 38.3%
Total patients(including referrals, surgery,
ulcer and reactions)
Grade 0 59.9%Grade 1 19.7%Grade 2 20.4%
Newly diagnosed patients only
2. Average Bed Stays
1. Clinic Attendance
3. Leprosy Case Admissions 2005-2009
15
4. WHO Grade Disability for Anandaban Patients (2005-2009)

Nursing DepartmentThe nursing department aims to pro-vide high quality care across many hospital activities including surgery, wards, out patient clinic, and emer-gency care for general patients as well as support within Anandaban’s satellite and field health clinics performed elsewhere in Nepal. Anandaban also serves by collabo-rating with local nursing schools to provide training for nursing students in leprosy and general care,
during which the students stay onsite within the downhill Training Unit. In 2009, nursing schedules were reorganized to make 24hr nursing care available to patients rather than auxiliary duty with on-call nursing care. Several nurses also received ongoing professional development training in Nepal in X-ray, midwifery, “Practical Approaches to Lung Health”, Nursing Management and Basic Counseling Skills.
Clinical department Explained
Dr Pankaj Awale, Sr Usha Ghimire and Sr Niru Shrestha (Matron).
Clinic
al
16

SurgeryReconstructive hand surgery can make a dramatic difference for a lep-rosy patient not only in function but also in stigma-related appearance. After surgery and specialized physi-otherapy, fingers can be stretched out and are no longer clawed.
Eyes can blink. Feet no longer drop. In these photos, Dr. Indra Napit and Dr. Pradeep Sapkota perform recon-structive surgery on a patient with clawed hands. Later, as As Dr. Indra finished wrapping up the cast, he asked the patient, “Are you hungry?”
Since the anesthetist had used a local nerve block, the patient had been awake the whole time. In the last photo, another patient demon-strates the effects of surgery on his left hand as compared to right which is still awaiting surgery.
An operation in progress
17

Clinic
al
18
PhysiotherapyAnandaban’s physiotherapy department has important roles indiagnosing and monitoring progres-sive nerve damage caused by lep-rosy. Typically, leprosy nerve damage can result in hand, foot and blinkingdisability. All patients are evaluated upon diagnosis, during treatment and once a year after treatment is finished. Reconstructive tendon transfer surgery with specialized physiotherapy can make dramatic change for those affected by leprosy.
Tendons linked to muscles and nerves that are still functional are spliced and used to rewire adjacent hand, foot or blinking muscles that have been damaged to regain func-tion. While a surgeon can rewire the tendons of a hand, foot or eyelid in just a few hours, it is the weeks and months of exercises between a dedicated physiotherapist and
a committed patient that play the stronger role in outcome.
Without proper physiotherapy,surgery would yield little. After the cast and bandages are removed,the patient must relearn how to think to move the rewired areas.Muscles that had weakened or had not been used for years needstrengthening exercises.
Reconstructive surgery patients are typically referrals from across Nepal, and many are from areas with little to no access to health care. Some come from villages many days walk from the nearest road. In order for their surgery to be successful, consistent physiotherapy is critical. Therefore, most reconstructive sur-gery patients stay in the hospital for at least 2-3 months per procedure.
Apsara Ghimire assessing the finger mobilization of a boy

Out Patient Department (OPD) Dr. Deepa Shah checks a patient while his father watches. The father and brother walked from a distant hill area for more than a day taking turns carrying him on their backs to reach the hospital. In addition to leprosy services, Anandaban also provides ~20,000 general medical treatments annually - including surgery, outa-patient and inpatient care (25 beds). Anandaban is the closest hospital for almost 200,000 Nepalese living in the rural hill communities south of Kathmandu. Many people live hours or a day(s) walk from the nearest road.
19
X-RayMadan Mahat prepares to take an x-ray of one of the patients

Foot and Disability CampsFoot and disability camps are an effective method to identify hidden cases of leprosy in a community, with 8% more cases found this way than using other methods.
The camps aim to: • Reach out to the community to
identify people affected by leprosy early so as to avoid disability.
• Identify people who have not com-pleted their MDT treatment or who have reaction
• Provide education to people about prevention of disability.
• Provide appropriate footwear and supportive orthopaedic devices to both people affected by leprosy and people with other physical disabilities
• Assess the need for any surgical or other intervention.
Through the camps held in 2009, 163 people were seen (30 % people affected by leprosy and 70 % oth-ers). For instance, Sunderbasti is a self settled leprosy colony situated on the outskirts of the Kalaiya Municipality in the southern district of Bara. About 100 people live in the colony, including 22 people af-fected by leprosy, their children and other relatives. Many of the people affected by leprosy have severe foot disabilities, leaving them vulnerable to unnoticed injury and in need of ongoing medical and prevention of disability care to stop further deterioration. In 2009 we started running foot camps in the colony every six
Outreach Clinics
Clinic
al
20

and severe disabilities are referred to Anandaban Hospital for ulcer management and corrective surgery. In comparison to earlier camps more people were found to be practicing self care for their feet and there was a decline in the number of people with ulcers. We are thankful for the welcome we receive at the colony and the op-portunity to conduct these camps.
Medical CampsIn 2009, we performed 5 general health camps attended by a total of 2253 people at a total cost of 2883 GBP (4940 USD). Camps ranged from 158-593 patients with a cost of 323-817 GBP (553-1400 USD) per camp, including after care like surgery and inpatient services for severe cases.
months with the objective of preventing disability and recurrent damage to feet, as well providing necessary medical services to other people living in the colony.
During the camp everyone affected by leprosy, their close relatives and anyone else who has concerns about leprosy are thoroughly exam-ined. At a recent camp one young girl was newly diagnosed with leprosy. Unlike her parents who are also affected by leprosy she started treatment early and is now cured with no visible disability. During the camp those who need it also receive education about self care, protective footwear and supportive devices. People with complicated ulcers
The camps target areas accessible to impoverished people with limited or no access to health care. Private donations from individuals or groups like Traid-Nepal and Lush (UK) have allowed us to staff a bus with clinicians, medicines and volunteers. We provide free health and dental checks, donated clothing, referrals and medicines. Hundreds are seen in 4-6 hours by a relative handful of very busy staff and volunteers. Many are women, children or those who normally may not seek medical care because they cannot pay. Some of the most life changing opportunities occur when we discover people needing sur-gery – like bone fractures left untended or prolapsed uterus neglected for years. Our Nepali staff identify cases of need and then refer or treat as appropriate. Many thanks to all those whose donations helped!
21

CounsellingExplained
Clinic
al
22Counsellor, Ruth Strestha, with patients in the women’s ward.

ber, with fifteen participants from different organisations across Nepal. Comprehensive Leprosy Training was given to health post staff for counselling for people affected by leprosy as well as gen-eral patients. Medical needs are great in Nepal and counselling in general is not much emphasised.
Counselling is a new concept to some people. Some of the partici-pants understood the importance of counselling for patients only after participating in the training.
In January of 2009, I joined as the Anandaban patient counsellor. In the context of Nepal, if a person is affected with leprosy, he/she is affected badly and torn apart not only physically but also mentally and emotionally. That is why the role of counselling is vital.
In my experience, when someone is diagnosed with leprosy then he/she often feels rejected and worthless to society. Depression is common, some considering suicide to end a life not worth living. These are the experiences that people affected by leprosy share with me. In group discus-sions, people learn to share their problems with one another, offering and receiving encourage-ment themselves. When families remain involved, they also receive counselling.
In 2009, grief and counselling training was provided to hospital staff members. A Basic Counsel-ling Workshop was held in Novem-
In future, I will also incorporate field and home visits, which will allow for family and community counseling.
In the past year I had to counsel an older woman who was affected with leprosy, Nima Tamang. After long period of continuous counseling, visiting and caring, we see changes in her. Now she is more willing to talk to others. She smiles and feels she is an integral part of society. Although she has been staying in the hospital for five months, no one has come to visit her. This case is just one example of the many that receive care at Anandaban. There are so many cases like this, emotionally bearing the stigma attached with leprosy. There is such need for coun-seling and prayer. As the effects of leprosy can extend for years beyond medication, counselling work at Anandaban will continue for some time to come.
Ruth ShresthaCounselorAnandaban Hospital
“In group discussions, people learn to share their problems with one another, offering & receiving encouragement”
Ruth Shrestha with a patient
23

There are a quite a few non-clinical staff that make the day to day operations of running a hospital compound possible!
Non Clinical Support
Non-C
linic
al S
upport
24
Left Middle:Dil Bahadur Lama works to keep the hospital clean
Upper Middle:Raj Kumar Khadka wringing clothes in the (hand) laundry department.
Lower Left:Maintenance team builds a sidewalk in front of the laboratories
Lower Middle:Krishna Mahandhar handles important errands dealing with government, customs and other official agencies.

Men Maharjan, Maila Tamang, Kedar Kathet and Chandra Tamang, have helped with their safe driving
25
Tulsi Thapa delights our guests with delicious food

Sto
ries
Urmilla with her Grandmother26

During this time at Anandaban, Muni met Ram Bahadur Thami, a former leprosy patient that now cares for Anandaban’s small herd of pigs within the rehabilitation programme. They married and are now expecting their first child. See cover picture.
Maya’s StoryAt the age of 14, Maya’s clawed hands were diagnosed as an effect of leprosy. After receiving antibi-otic treatment at another hospital, she was referred to Anandaban for reconstructive surgery for her hands. Maya has had three reconstructive surgeries and the physiotherapy staff continue to help her with exercises to help regain more function in both of her hands. She had not been able to use her own hands to eat for seven years! Although her family is aware, none of her community knows that she has been diagnosed with leprosy. Maya worries about how they will respond when she returns home. Maya also would like to receive train-ing through Anandaban’s rehabilita-tion program so that she can support herself. She is determined to show people back home that she can live a dignified life and earn livelihood. See photo on page 29.
Urmilla’s StoryAt 11 years old, Urmilla is the young-est of three children. Three years ago, Urmilla’s mother left for employ-ment in the middle east. Her mother phoned once and has not been heard from again. Her father left them. The children now live with their maternal grandmother who sells vegetables in Chitwan. During the winter, red swollen patches of skin began to ap-pear on Urmilla’s face and body. Her grandmother took her to the district hospital which then referred her to Anandaban where she was diag-nosed with a leprosy reaction. The extent of the patches indicated that she has had leprosy for some time but was unaware. Urmilla was admit-ted, provided proper medications and stayed under doctor supervision for 2 months here at Anandaban. Un-like most other children that come to us, she had a family member with her. Her grandmother stayed at her side.
Muni’s StoryMuni remembers noticing the first signs of leprosy when she was 8 years old. She lived in the Morang District of Eastern Nepal. Fatherless, she lived with her mother, elder sister, younger sister and younger brother. She attended school until grade five, when her feet lost feel-ing and she was diagnosed with leprosy. She had travelled first to the district hospital and then was referred to a mission clinic in Biratnagar.
Muni faced discrimination from her village: she was not permitted to draw water from the local tap. Her elder married sister was even looked down by their community because they were related. When Muni finally completed the long treatment with leprosy antibiotics, the mission clinic referred her to Anandaban for surgical consulta-tion. Her hands and feet were marred and disabled by leprosy. In November 2009, Muni received corrective surgery for her hand and then later her foot.
Each surgery requires weeks in a cast followed by months of physiotherapy.
Patient Stories
27
Urmilla

Yadhav’s StoryAlthough medicine killed the leprosy bacteria in his nerves years ago, the nerve dam-age in Yadhav’s legs and feet is permanent. He can walk, but his foot strikes the ground awkwardly and has become deformed after years of problem-atic use. Altered pressure points on his feet make him vulnerable to the development of deep tissue ul-cers. Yadhav’s story is typical of many people affected by leprosy. The nerve damage also means that people can-not feel the pain of the ulcers, so the ulcers can grow deep and fester be-fore people even notice. Yadhav still comes to hospital for the treatment of recurrent foot ulcers. Sometimes they are so deep they require months of inpatient care. It’s a debilitating
cycle. If people work hard or walk far (which is what is demanded from the Nepali lifestyle and environment)
their disabilities worsen through foot wounds and altered wear-ing. Coming from across Nepal, sometimes people make it to hospital too late: infection sets in and amputa-tion must be performed. Then,
how will they work? Our footwear department can custom build them prostheses, but life becomes that much harder. Yadhav is one of the 50,000 cured but disabled people affected by leprosy in Nepal who still suffer from the effects of the disease. Our hospital seeks to provide holistic care. Multiple staff work with patients to determine how we can help. For patients with disabilities what lifestyle changes can be made to
Yadhav can walk, but his foot strikes the ground awkwardly and has become deformed after years of problematic use.
Sto
ries
28

prevent development of further disability and wounding? How can recurrent inpatient care be avoided? How can people be more self-sufficient and participatory in their own communities? The pastoral counsellor, Mrs. Ruth Shrestha, provided Yadhav with a listening ear. Yadhav pleaded, “Please, I need a toilet! Please give me a toilet. The nearest toilet is 25 minutes walk away.”
Can you imagine? Every time this man needs to use the toilet, he must walk roughly one hour. Could you picture the impact that would have on your family? In some ways, he is lucky. Only 50% of people in Nepal have access to a toilet. Combined with water short-ages and monsoon, this is a major contributing factor to the routine parasite, intestinal and stomach sicknesses that plague similar communities around the world. Through our socio economic reha-bilitation program (SER), Yadhav
29
can receive the supplies to build his own toilet, a simple outhouse. To encourage empowerment and responsibility, the Leprosy Mission requires that the receiver provide the necessary labour – either by hiring from their community or performing it themselves. Yadhav lives in a community that is so poor that there is often no money.
Peasants work landowner’s farms when work is available: food for the day becomes currency. This “small” but strategic gift of a simple toilet may allow Yadhav to escape developing foot ulcers as often as he currently does and thus to avoid inpatient care which means months away from home and the work he must perform to feed his family. Hospital staff processed the forms for him to re-ceive the toilet construction sup-plies. His ulcers are healing and he will soon depart the hospital. He will now be able to better care for his feet.
Maya (far right) with the counsellor, Ruth, and other patients in the women's ward

Maita Majhi’s StoryMaita Majhi’s hands danced as she talked about her children – she tapped her forehead to fashion a hat and then flashed the number two and a huge smile. “You have two sons,” Ruth Shrestha, Ananda-ban Hospital’s patient counsellor, mouthed back, also imitating her signs. Maita has had a speech-impairment since birth, but that has not prevented her from having much to say.
Her brown eyes sparkled as she communicated through her own form of sign language; as she held her hands away from her to describe the great distance she travelled from her home in Ra-mechhap in the North Eastern part of Central Nepal to Anandaban, the rigid clutch of the fingers on her right hand bore the trademark of leprosy, which causes loss of control of these muscles as the bacteria attacks the motor nerves in the fingers.
Sto
ries
30Maita Majhi

Maita’s expressions became sol-emnly emphatic as she described her daughter – “chori,” she signed, twisting her fingers in the shape of a tiny nose ring. “She fed her and fed her but her daughter was so tiny,” Ruth explains. Maita passes her hands over her face, and then tugs on Ruth’s white nursing coat – “her daughter turned very pale and then she died.”
Without words, the full meaning of Maita’s pain becomes lost in her folded hands. Like many Nepali women she has never been to school and cannot write to explain how she is feeling beyond what she can sign. Much of Maita’s per-sonal history has been lost to the daily grind of her role as mother and wife in rural Nepal; she is not sure how old she is. With some friendly debate, the other women in the open ward arrive at the community consensus that she is thirty-three because her sons are twelve and seven years old. As a
farmer’s wife, her life hinges on the success of her family’s crops and the cooperation of the weather; poor nutrition and disease pose a constant threat, and poverty can exacerbate simple health prob-lems by limiting proper medical
attention. As Anandaban’s coun-sellor, Ruth not only helps locate occupational and educational re-sources, but often takes on the role of friend and surrogate mother, listening to the many stories of heartbreak and loss caused not only by the stigma of leprosy, but
31
also by the difficulties of poverty and illiteracy in Nepal.
Still, the work-free stay at Anandaban makes Maita rest-less; she is looking forward to a visit from her husband as soon as rice-planting season is over. Maita laughed as she signed “water buffalo milk makes you grow large”– she is proud of her family and misses the daily activity of maintaining their farm. However, the development of clawing in her hands caused by her leprosy makes work difficult. At Anandaban she will loosen up her stiffened finger muscles through daily physiothera-py exercises, and will then undergo reconstructive surgery to regain control of those fingers. Because she has come to Anandaban, the clawing in her fingers can be im-proved; while here, she also gains a community of sisters, sharing their experiences as they are restored in a place providing physical, emotional, and spiritual support.
At Anandaban Maita will loosen up her stiffened finger muscles through daily physiotherapy exercises

Dia
gnost
ic &
Res
earc
h L
abs
Mr. Ishwor Shrestha performs routine lab tests on patient blood samples32
collaborations funded by grants from external agencies.
Can early leprosy be detected in patients before symptoms develop? In 2009, after 10 years work at Anandaban, data collection was completed for a Phase II clinical trial performed in collaboration with scientists at Colorado State University and the US National Institutes of Health. Similar to the
Anandaban Hospital is uniquely equipped with a strong research laboratory permitting investiga-tions relevant to leprosy patients around the world. Accessing leprosy patients from across Nepal, we investigate new diag-nostics, the basic science of how the disease affects patients as well as evaluate how well current control strategies are perform-ing in Nepal. Most projects are international
PPD or Monteux test for tubercu-losis, we tested a new diagnostic skin test to see if it was possible to detect leprosy exposure to leprosy in patients and household contacts. Results are currently under analysis, but may lead towards identification of leprosy patients before they develop clini-cal symptoms, irreversible nerve damage or disability. A presen-tation of findings will be given during the US-Japan Cooperative
Diagnostic & Research Labs Explained
33Saraswoti Khadge, Research Assistant

34
Tuberculosis and Leprosy Meeting held at Harvard University (USA) in July 2010.
Are current treatments sufficient to block ongoing nerve damage and resolve leprosy reactions? Another study was also completed in collaboration with Dr. Diana Lockwood and Dr. Steve Walker of the London School of Tropical Medicine and Hygiene that inves-tigated current steroid treatment regiments for reactions. Results
indicated that current global treatment recommendations only resolve reactions in 50% of patients and should be improved to provide better protection from ongoing nerve damage during the reaction episode. Findings will be developed into a manuscript for scientific journal publication in 2010.
Do genetic differences make some people more susceptible to leprosy? Why?
Dhurba Mahat and Kapil Neupane lookat samples in their microscopes.
Dia
gnost
ic &
Res
earc
h L
abs

While leprosy remains primarily a disease of the poor, susceptibil-ity to leprosy is a complex issue that is not well understood. In collaboration with Dr. Tom Hawn of the University of Washington (USA), we have investigated and compared the genes of Nepalese leprosy patients and healthy controls. We’ve identified several important genetic differences in patients that develop reac-tions and those who do not and between the different types of
“While Leprosy remains primarily a disease of the poor, succeptibility to leprosy is a complex issue ”
As specialized leprosy refer-ral centers dwindle in number, Anandaban provides an essential setting for performing these types of high caliber studies ap-plicable for leprosy care providers around the globe. Several other studies are currently in progress.
For more information on studies or publications, please contact Dr. Deanna Hagge at [email protected]
leprosy (MB and PB) – primarily in genes directing defense strategies against invading bacteria. Illumination of such vulnerabilities will help us better understand how the disease works and how we can more effectively combat it.
Ishwor Shrestha, Dr Min Thapa and Kapil Neupane looking at the injection site of one of the patients of the Skin Test Study
35

Trai
nin
g
36Field Training in Makawanpur

orientation sessions and workshops for other NGO’s, Government and private colleges. MD Dermatology students from the B.P. Koirala Insti-tute of Health, National Academy of Medical Science, Tribhuvan University Teaching Hospital and Bir Hospital also came for two weeks of training to develop their knowledge in holistic leprosy treatment and management.
In addition this year we started to train people who are directly involved in community work with people affected by leprosy. We particularly focused on the
training of Community Health and Development Facilitators who work with self help groups to implement a range of programmes aimed at improving group member’s quality of life. Facilitators also help to em-power people affected by leprosy to be a voice against discrimination they face in their communities.
The Training Unit is proud of the recognition it has received about the quality of our training both from the concerned government health institutions and trainees. Overall, the Training Department has had a successful year.
The Leprosy Mission Nepal’s Train-ing Unit aims to equip Basic Health Service Staff with the knowledge and skills necessary to provide high quality leprosy services within the integrated health system to people affected by leprosy in their own communities.
In 2009, 781 people in total, representing the 15 districts of the Central Development Region, participated in different courses, held either at the Training Unit or in the field. These courses included Comprehensive Leprosy Training (basic and refresher) and leprosy
Training Explained
20 Paramedics28 School Teachers198 Female Community Health Volunteers
12 Health & Development Workers135 Volunteers104 Paramedics
25 Medical Doctors131 Nursing Students131 Medical Students
Field Based Training
Anandaban Based Training
37
A previous Medical Director of Anandaban, Dr. Ruth Butlin, visited to help teach a medical officers training course

Com
munity
Work
38
Self help group member Sanjhariya having her first driving lesson after receiving a tricycle. She is watched closely by Dinesh Chaudhary on the far right, CEDAR Project volunteer, and the other members of her village.

self help groups in each VDC, bring-ing together people affected by leprosy and people with physical dis-abilities. There will be 40 groups in Rautahat and 25 groups in Ramech-hap, with 15 to 20 members each.
All the programs and activities of the project are being implemented through these groups.
There are six key programs in all:1) Capacity building program: Group members will decide on the changes/impacts they would like to see realised in their lives and their communities through being a part of their self help groups. A range of different workshops will be con-ducted to help group members to
In July 2009 the Leprosy Mission Nepal (LMN) launched a new project – the Community Empowerment Development, Disability and Rehabilitation (CEDAR) Project.
The goal of the project is to empower, increase the capacity and improve the quality of life of people affected by leprosy and people with physical disabilities, with attention to women and people who are marginalised. A team combining experienced LMN staff, with new local staff from the project area, has been put together to see this work carried out. This project is being supported by The Leprosy Mission in Australia. It will run for five years (until mid 2014) and will operate in the districts of Rautahat (on the Southern plains) where the prevalence rate of leprosy remains high, and Ramechhap (in the North Eastern hills) where disability is a major issue. Eight Village Development Committees (VDCs), composed of nine villages each, where the greatest number of people affected by leprosy are living were selected in each district.
Work began with the formation of
achieve these changes/impacts.
2) Economic program: This program will provide group members with training in the development of business plans, along with vocational and income generation skills in local industries. Each group will receive seed money that will form a revolving fund from which group members can take loans to start their own small busi-nesses.
3) Social participation program: To increase people’s participa-tion in social interactions and important community activities this program will offer group members the opportunity to undertake non-formal educa-tion literacy classes. We will also launch community awareness campaigns about leprosy and disability. In partnership with community leaders and other agencies we aim to identify how the needs of people with leprosy and physical disabilities can be met in the wider community e.g. the development of support services, enabling access to public places.
CEDAR
“The goal of the project is to empower, increase the capacity and improve the quality of life ”
39
The CEDAR Project team

Com
munity
Work
40
4) Disability program: This program will conduct training for group members on prevention of disability strategies. It will also provide rehabilitation services to group members aimed at enabling members to learn new ways to perform daily activities for their maximum independence and will provide members with assistive devices (e.g. wheelchairs, home modifications).
5) Health education program: To assist in reducing the incidence of waterborne and sanitation related diseases this program will
conduct health education training for group members. We will also build water and toilet facilities for group members most in need.
6) Housing program: This program will provide for the construction of low cost housing and repair of housing for those group members most in need.In the final phase of the project the self help groups in the same VDCs will join together to form cooperatives. These cooperatives will act to meet the ongoing needs of members once the project has come to a close.
Rautahat writing the meeting minutes.
Self help group members from Bhatauli VDC, Ramechhap participating in leadership training.

two week rolling programme where prior to going home people can learn everything they need to know about preventing disability when
performing their everyday activities e.g. cleaning, cooking, farming etc. Previously the unit was located in one of the new wards of Ananda-ban Hospital. Because a hospital ward bears little resemblance to the home environment that people are returning to on discharge, a new unit in the style of a Nepali village house was built on the hospital compound. This is now known as Rosa’s house.
In 2009 the Leprosy Mission Nepal initiated the Socio-Economic Rehabilitation (SER) Project. This project is supported by The Leprosy Mission Australia. The project brings together under one umbrella a number of activities that the Lep-rosy Mission Nepal has been imple-menting for several years, as well as adding some new activities.
One key focus of the project is to support both children affected by leprosy and the children of parents affected by leprosy to go to school. Starting in 2009 the parents of chil-dren receiving scholarships will also receive a matching grant for either vocational training or other income generation initiatives. In this way it is hoped that whole families will be empowered. Popular income gen-eration initiatives include buffalo and goat rearing, vegetable farm-ing, small businesses, mechanical and driving training and tailoring training.
The project also includes the Self Care Unit. The Self Care Unit offers a
The project will also continue to build low cost houses for people affected by leprosy, with a particular focus on women who have been abandoned by their families follow-ing a diagnosis of leprosy and other people who have been displaced. An additional activity will be the construction of toilets and drinking water facilities. The commencement of these activities was in response to the growing number of requests for these facilities from people attend-ing Anandaban Hospital.
While many of these activities are currently implemented on an individual basis, it is the aim of the project to increase the number of self help groups for people affected by leprosy. Currently there are 20 groups, and we hope to add another 20 groups. Self help groups are a great way of implementing many of these activities, and when combined with leadership and other capacity building training for members, they can be a means of meeting the sup-port and other needs of members for many years to come.
SER
“One key focus of the project is to support both children affected by leprosy and the children of parents ”
41
Mr Chanra B Thapa and Mrs Sulochana Shrestha attending to people for rehabilitation programme
Dr Hugh Cross, Country Representative of TLMI, inaugurating a Self Care House

Exec
utive
Mem
ber
s of
the
LMN B
oar
d
42
Board Executive Members of Leprosy Mission Nepal
Mr. B.B. Khawas Chairman (Ex-CEO of Patan Hospital, Pastor of NIM Lalitpur Church)
Mrs. Draupadi Rokaya Vice Chairperson (Women Activist, Social Worker)
Mr. Ashok Adhikari General Secretary (Pastor)
Mr. Surya Acharya Treasurer (Tutor, Ebenezer Bible College)
Mr. Kamal Shrestha Member (Executive Director, Nepal Leprosy Trust)
Mr. Krishna Man Shakya Member (Executive Director, Shanti Nepal)

Back row, Left to right:
Sushil Khatiwada (Finance manager) Kamal Shrestha, Dr. Hugh Cross (TLM Nepal Country Leader), Hem Thapa.Surya Acharya.Dr. Indra Napit (Medical Director), Dr. Narayan Maharja.
43
Dr. Narayan Maharjan Member (Chairman, Nepal Christian Fellowship)
Mrs. Gyanu Sodemba Member (Tutor, Nursing College)
Mr. Hem Thapa Member (Social Worker)
Front Row, Left to right:
Mrs. Draupadi Rokaya.Shovakhar Kandel (Executive Director)B.B. Khawas.Mrs. Gyanu Sodemba.
