antifúngicos por onde começar? - aparcih · antifúngicos por onde começar? flávio de queiroz...
TRANSCRIPT

AntifúngicosPorondecomeçar?
FláviodeQueirozTellesMédicoInfectologista
ProfessorAssociadodeInfectologiaDepartamentodeSaúdeComunitária

Disclosures
Grants for Medical EducationAstellas, MSD, Pfizer, TEVA, United Medical
Grants for ResearchAstellas, MSD, Pfizer
Public Fundings - Brazilian AgenciesCNPq, CAPES, Fundação Araucária

Pathogenic Opportunistic
DermatophytesDimorphic Molds Yeasts
Aspergillus sp
Fusarium sp.
Mucorales
Scedosporium sp
Melanized(Dematiaceous)
Candida sp.
Cryptococcus sp
Trichosporon sp
Malasezzia sp
Rodotorula
Sacharomyces
P. brasiliensis / lutzii
H. capsulatum
B. dermatiditis
Coccidioides imitis / posdasii
P. marneffei
S. Schenckii / brasiliensis
Melanized (Dematiaceous)
Fungos deimportância médica noambientehospitalar
MicosessuperficiaisecutâneasMicosesendêmicasMicosesoportunísticas xAIDSDFI=raridadeecuriosidade
00.20.40.60.8
11.21.41.61.8
2
1969 1979 1989 1994
Candidíase
Aspergilose
Criptococose
Zigomicose
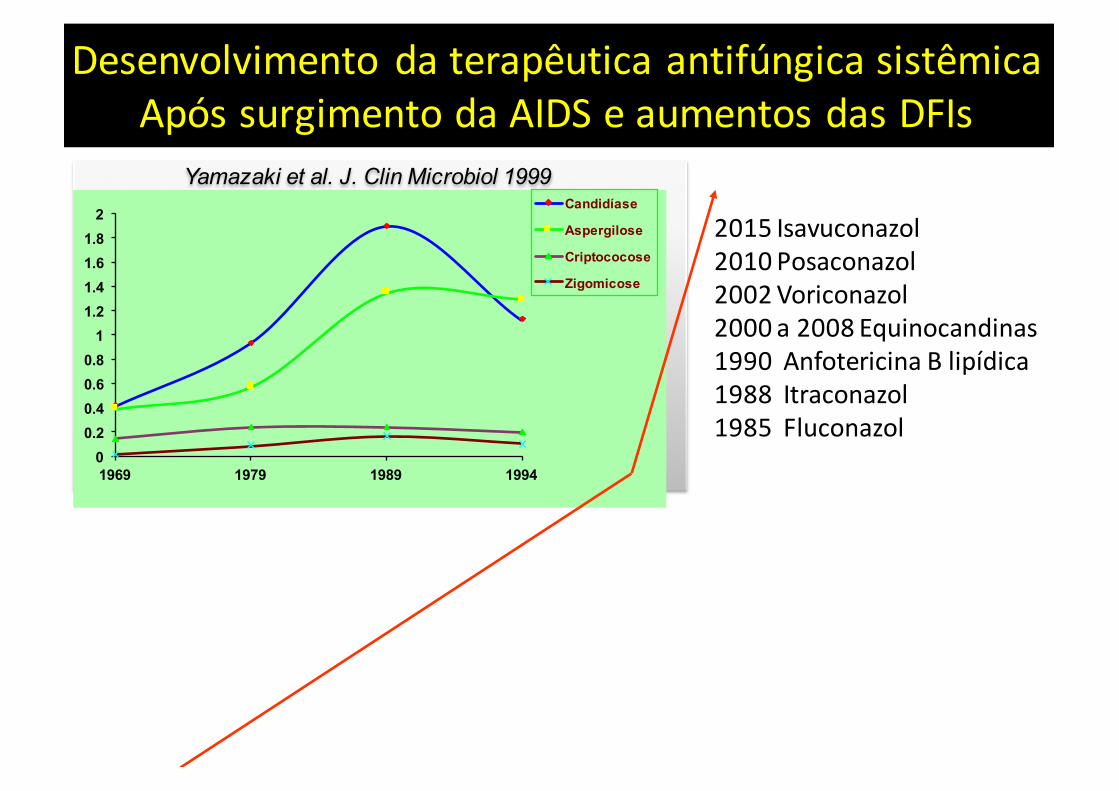
Yamazaki et al. J. Clin Microbiol 1999
Desenvolvimento daterapêutica antifúngica sistêmicaApós surgimento daAIDSeaumentos dasDFIs
2015Isavuconazol2010Posaconazol2002Voriconazol2000a2008Equinocandinas1990Anfotericina Blipídica1988Itraconazol1985Fluconazol

Highburdenoffungalinfectionsworldwide
Thelogicbehindtheseestimationsisanextrapolationfromincidenceratesreportedinriskpopulationsworldwide
BrownGP,Denning D,GowNARet al Sci Transl Med 4(165):1,2012
Disease (most common species) Location Estimated life-threatening
infections/year
Mortality rates (% in infected populations)
Cryptococcosis(Criptococcus neoformans)
Worldwide >1,000,000 20-70
Invasive Candidiasis(Candida albicans)
Worldwide >400,000(proved cases)
46-75
Invasive Aspergillosis(Aspergillus fumigatusand Aspergillus spp.
Worldwide >200,000(under diagnosed)
30-95
Mucormycosis(Rhizopus aryzae)
Worldwide >10,000 30-90
Pneumocystis(Pneumocystis jiroveci)
Worldwide >400,000 20-80

43%
28%
8%
21% Invasive aspergillosisInvasive candidiasisZygomycosisOthers
23 US transplant centers, 2001-2006983 IFI in 875 patients with HSCT
Incidência deDFIsem Receptores deTCH
Kontoyiannis DP, et al. Clin Infect Dis. 2010;50:1091-100.
● Aspergillus spp é o agente mais frequente (TRANSNET)
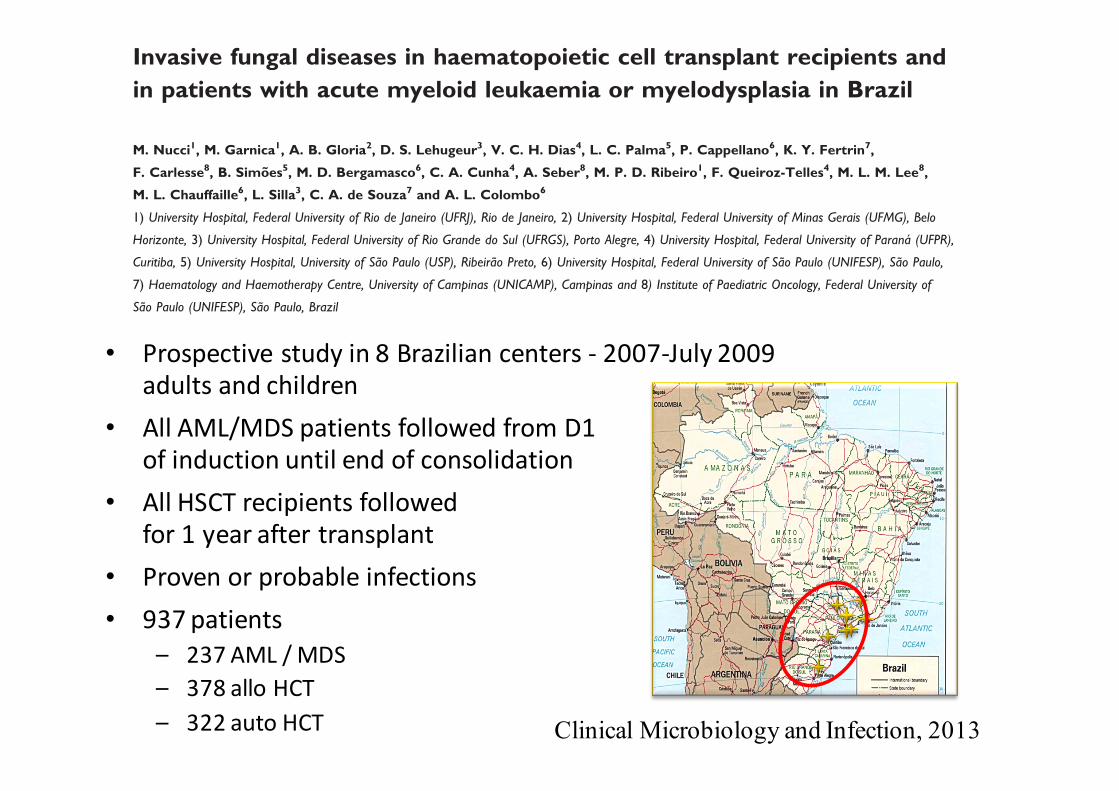
Invasive fungal diseases in haematopoietic cell transplant recipients and
in patients with acute myeloid leukaemia or myelodysplasia in Brazil
M. Nucci1, M. Garnica1, A. B. Gloria2, D. S. Lehugeur3, V. C. H. Dias4, L. C. Palma5, P. Cappellano6, K. Y. Fertrin7,
F. Carlesse8, B. Simoes5, M. D. Bergamasco6, C. A. Cunha4, A. Seber8, M. P. D. Ribeiro1, F. Queiroz-Telles4, M. L. M. Lee8,
M. L. Chauffaille6, L. Silla3, C. A. de Souza7 and A. L. Colombo6
1) University Hospital, Federal University of Rio de Janeiro (UFRJ), Rio de Janeiro, 2) University Hospital, Federal University of Minas Gerais (UFMG), Belo
Horizonte, 3) University Hospital, Federal University of Rio Grande do Sul (UFRGS), Porto Alegre, 4) University Hospital, Federal University of Parana (UFPR),
Curitiba, 5) University Hospital, University of Sao Paulo (USP), Ribeirao Preto, 6) University Hospital, Federal University of Sao Paulo (UNIFESP), Sao Paulo,
7) Haematology and Haemotherapy Centre, University of Campinas (UNICAMP), Campinas and 8) Institute of Paediatric Oncology, Federal University of
Sao Paulo (UNIFESP), Sao Paulo, Brazil
Abstract
Invasive fungal disease (IFD) shows distinct regional incidence patterns and epidemiological features depending on the geographic region.
We conducted a prospective survey in eight centres in Brazil from May 2007 to July 2009. All haematopoietic cell transplant (HCT)
recipients and patients with acute myeloid leukaemia (AML) or myelodysplasia (MDS) were followed from admission until 1 year (HCT)
or end of consolidation therapy (AML/MDS). The 12-month cumulative incidence (CI) of proven or probable IFD was calculated, and
curves were compared using the Grey test. Among 237 AML/MDS patients and 700 HCT recipients (378 allogeneic, 322 autologous),
the 1-year CI of IFD in AML/MDS, allogeneic HCT and autologous HCT was 18.7%, 11.3% and 1.9% (p <0.001), respectively. Fusariosis
(23 episodes), aspergillosis (20 episodes) and candidiasis (11 episodes) were the most frequent IFD. The 1-year CI of aspergillosis and
fusariosis in AML/MDS, allogeneic HCT and autologous HCT were 13.4%, 2.3% and 0% (p <0.001), and 5.2%, 3.8% and 0.6% (p 0.01),
respectively. The 6-week probability of survival was 53%, and was lower in cases of fusariosis (41%). We observed a high burden of IFD
and a high incidence and mortality for fusariosis in this first multicentre epidemiological study of IFD in haematological patients in Brazil.
Keywords: Aspergillosis, epidemiology, fusariosis, haematological malignancy, invasive fungal disease
Original Submission: 11 June 2012; Revised Submission: 7 August 2012; Accepted: 14 August 2012
Editor: E. Bottieau
Article published online: 31 August 2012
Clin Microbiol Infect 2013; 19: 745–751
10.1111/1469-0691.12002
Corresponding author: M. Nucci, Hospital Universitario
Clementino Fraga Filho, UFRJ. Rua Prof. Rodolpho Paulo Rocco 255
– 21941-913, Rio de Janeiro, Brazil
E-mail: [email protected]
Introduction
Invasive fungal disease (IFD) represents a major complication
in patients with haematological malignancies and in haemato-
poietic cell transplant (HCT) recipients [1,2]. The incidence
and epidemiology of such infections have been characterized
in various retrospective studies [3–17] and a few prospective
studies [18–22] conducted in Europe, the USA and Japan.
However, the incidence and epidemiology of IFD may differ
significantly depending on the geographic region. The knowl-
edge of these epidemiological differences is important to
implement appropriate strategies of prevention, diagnosis
and therapy, and also because of the globalization of the
world, with frequent travelling and migration.
In this paper we report the results of a study that
involved patients with acute myeloid leukaemia (AML) or
myelodysplasia (MDS) receiving intensive chemotherapy and
HCT recipients from eight major referring centres.
Patients and Methods
This is a prospective multicentre cohort study in eight cen-
tres located in seven cities in the south and south-east of
ª2012 The Authors
Clinical Microbiology and Infection ª2012 European Society of Clinical Microbiology and Infectious Diseases
ORIGINAL ARTICLE MYCOLOGY
Clinical Microbiology and Infection, 2013
• Prospective study in8Brazilian centers- 2007-July2009adults and children
• All AML/MDSpatients followed from D1of induction until end of consolidation
• All HSCTrecipients followedfor1year after transplant
• Proven or probable infections• 937patients
– 237AML/MDS– 378allo HCT– 322autoHCT

Invasive Fungal Infections
Todos Provadas+prováveis
Aspergillosis 58 18Fusariosis 18 17Candidiasis 15 12Hyalohyphomycosis 9 9Mucormycosis 3 3Mixed infection* 3 3Other**
* Fusarium+Candida(1),Aspergillus(1),Colletotrichium (1)**C.neoformans (1),Rhinocladiellaacquaspersa (1),Geotrichum sp.(1)
Nucci et al Clin Microbiol Infect 2013
1Limitações doestudo:GMnão realizado na rotina emalguns centros muitos “casos AIpossíveis”2– Aincidência de“casos AIprováveis ”pode ter sidosubestimada…
Rede Brasileira deVigilância em DFIsem PacientesOnco-Hematológicos

Rede Brasileira deDFIsem pacientes HematológicosAnálise de937casos em 08hospitais
17
2,2
0
2,3 1,7
0,5
2,3
1,3 0,5
0 0,8
0 0
2
4
6
8
10
12
14
16
18
LMA/MDS TCTH alo TCTH auto
Aspergilose Candidemia Fusariose Zigomicose
Prev
aleên
cia%
)
Nucci etal.Clin Microbiol Infec 2012
N=237 N=378 N=322

TheBrazilianNetworkofInvasiveFungalDiseasesinHematology:CumulativeIncidence
02468
101214161820
AML/MDS TCTH-ALLO TCTH-AUTO
CandidemiaFusariosisAspergillosis
(Inc =18.7%)
(Inc=11.3%)
(Inc=1.9%)
Nucci et al Clin Microbiol Infect. 2013

Aspergilose Invasiva em Países em Desenvolvimento
Aunaloke Charrabarti etal.MedMycol2011

General mortality = 92 (60%): IA and/or progression of underlying disease and septicemia
IA-related mortality = AI 62 (67%): Respiratory failure in 50/62 patients (80%) co-infections and co-morbilities: 20%Death within 14 and 21 days in 98% e 87% respectively
.
Garcia-Vidal, Plos One 2015within 14 and 21 days of presentation were 19.84-fold and 3.15-fold higher than that of an IA-unrelated death, respectively.
Factors associated with IA-related mortalityTable 3 shows the independent factors associated with IA-related mortality. After adjustment,chronic liver disease (HR 4.542; 95% CI, 1.69–12.23) was the only factor independently associ-ated with IA-related mortality. Conversely, receipt of voriconazole was independently associat-ed with reduced risk of IA-related death (HR 0.43; 95% CI, 0.20–0.93).
Fig 1. Frequency plot of IA-related and IA-unrelated mortality.
doi:10.1371/journal.pone.0120370.g001
Table 3. Independent risk factors for IA-related death.
Variable Adjusted
HR (95% CI) p
Patient-related factors
Chronic liver disease 4.54 (1.69–12.22) .003
Severe impairment on PFT1 2.46 (0.90–6.77) .081
Hematologic disease 0.99 (0.42–2.35) .992
Corticosteroid treatment 1.37 (0.61–3.06) .449
IA-related factors
Disseminated IA 2.12 (0.58–7.69) .253
Proven IA 2.23 (0.90–5.56) .986
Voriconazole treatment2 0.04 (0.20–0.93) .032
1Severe pulmonary function test abnormality.2 Voriconazole received for at least 5 days.
doi:10.1371/journal.pone.0120370.t003
Death in Patients with Aspergillosis
PLOS ONE | DOI:10.1371/journal.pone.0120370 March 24, 2015 6 / 10
Causesof Death related to Invasive AspergillosisBarcelona(03hospitals,152patients,2008-11)
Voriconazole TX wasassociated withreduced risk of death(HR 0.43; 95% CI,0.20–0.93).

Candidemia Na América Latina672 episódios (21 centros - 7 países)
Countries Rates per 1,000 admissionsColombia 1.96 (1 center)Argentina 1.95 (1.26-2.98)Venezuela 1.72 (1.04-2.90)
Brasil 1.38 (0.55-2.11)Ecuador 0.9 (0.30-1.10)
Honduras 0.90 (0.88-0.98)Chile 0.33 (0.21-0.47)Total 1.18
Nucci, Colombo, Queiroz-Telles et al; PLOS ONE, 2013

Characteristics of 672 Episodes of Candidemia in Latin America
No.Median age (range) 26 (0 – 98)Time from admission to candidemia
15 (0 – 176)
Median APACHE score (range)
18 (2 – 39)
Cancer 22%Renal failure 22%Cardiac disease 23%Lung disease 25%Diabetes 11%Surgery 44%
Nucci et al. PLoS ONE 2013;8:e59373

C.glabrata orCandidaMDR"Candidaproblema"
Fluco R
Equinocandinas R
Caspo
Ostrosky-Zeichner, CID 2013
Equinocandinas são “lowcostdrugs”Tratamento empírico é frequente!!!Profilaxia em pacientes hematológicos temsidousada….

Epidemiologia de candidemia em UTI no BrasilAnálise comparativa de 5 estudos multicêntricos
realizados entre 2003-2012
Espécies Período 12003-2007
Período 22008-2012
Valor de p
TOTAL 396 251
C albicans 44,7% 43% NS
C parapsilosis 18,2% 15,5% NS
C tropicalis 22,7% 20,3% NS
C glabrata 7,8% 13,1% ↑ <0.03
C krusei 1,3% 04,4%↑ <0.01
Colombo Al et al Intensive Care Medicine-Agosto, 2014

General characteristics related to the emergence of non-albicans Candida spp
Paramythiutou et al. Molecules, 2014

Kullberg & Arendrup, NEJM, 2015

Micafungina temimpactolimitadonacolonizaçãointestinalporCandidaspp
VanBurik etal.Clin InfectDis2004

Candidemia de escape durante a profilaxia com FCZ e CASPO
n engl j med 373;15 nejm.org October 8, 2015 1453
Invasive Candidiasis
removal at any time point was associated with a reduction in mortality and higher clinical suc-cess rates.39,40,58 In the pooled patient-level analy-sis of seven randomized treatment trials, treat-ment with an echinocandin and catheter removal were identified as the two modifiable manage-ment strategies associated with better survival.38 Because patients have to be alive to have a cath-eter removed, these types of analyses may not be free of bias. Although the debate about this issue will continue, it seems wise to remove all intra-vascular catheters in patients with candidemia, if logistically feasible.31,55,59
Emerging R esis ta nce
Resistance to antifungal treatment can emerge either by means of the selection of species with intrinsic resistance or an induction of resistance in isolates from species that are normally sus-ceptible. The former route is the most common, as illustrated by the emergence of C. glabrata after the introduction of fluconazole and of C. parapsilo-sis in settings in which there was increased use of echinocandins (Fig. 2).6,60 In addition, insuf-ficient dosing of azoles has been associated with the emergence of resistance.61
Figure 2. Distribution of Candida Species According to Duration of Prophylaxis and Antifungal Agent Used for Prophylaxis.
Panel A shows the distribution of candida species isolated from the bloodstream of patients with candidemia in a Danish study.6 From left to right, the graphs show the distribution in patients who had received no antifungal prophylaxis at the time of blood culture (258 patients), those who had received antifungal prophylaxis for less than 7 days at the time of culture (21 patients), and those who had re-ceived antifungal prophylaxis for at least 7 days at the time of culture (28 patients) (P = 0.007 according to the chi-square test). Antifun-gal prophylaxis included fluconazole in 37 patients (70%), voriconazole in 2 patients (4%), caspofungin in 6 patients (11%), and an am-photericin B formulation in 8 patients (15%) (some patients received more than one drug). Panel B shows the distribution of candida species isolated from the bloodstream of patients with candidemia in a French study.60 From left to right, the graphs show the distribu-tion in patients who had received no antifungal prophylaxis at the time of blood culture (2289 patients with no fluconazole exposure, and 2387 patients with no echinocandin exposure), those who had received fluconazole before the blood culture was performed (159 patients), and those who had received caspofungin before the blood culture was performed (61 patients).
B Distribution Based on Antifungal Agent Used for Prophylaxis
A Distribution Based on Duration of Prophylaxis
C. albicans
C. tropicalis
C. glabrata
C. krusei
C. parapsilosis
C. albicans
C. dubliniensis
C. tropicalis
C. glabrata
S. cerevisiae
C. krusei
C. parapsilosis
Other candida species
Other fungi
No Antifungal Prophylaxis Antifungal Prophylaxis <7 Days Antifungal Prophylaxis >7 Days
No Antifungal Prophylaxis Fluconazole Prophylaxis Caspofungin Prophylaxis
The New England Journal of Medicine Downloaded from nejm.org at UFPR on October 10, 2015. For personal use only. No other uses without permission.
Copyright © 2015 Massachusetts Medical Society. All rights reserved.
N = 2.289 N= 159 N = 61
Kullberg & Arendrup, NEJM, 2015

Herkert et al. RIAM 2015
Sensibilidade de 15 isolados sanguíneos de C. glabrata à EquinocandinasPeríodo: 2005 a 2012Susceptíveis: 03 (MIC 0,03-0,06)Intermediária: 11 (MIC ≥250) Resistência 01 (MIC ≥ 0,25)

Trichosporon breaktrhough fungemia duringechinocandin therapyN=14
YongLetal,ChinMedJ2012

Preventing invasive candida infections. Where couldwe do better?Philippe Eggimann*, Yok-Ai Que, Jean-Pierre Revelly, Jean-Luc PaganiAdult Critical Care Medicine and Burn Unit, Centre Hospitalier Universitaire Vaudois (CHUV), Lausanne, Switzerland
A R T I C L E I N F O
Article history:Received 28 October 2014Accepted 20 November 2014Available online 16 December2014
Keywords:Candida albicansCandidaemiaColonization indexEmpirical treatmentInvasive candidiasisNosocomial infectionsProphylaxis
S U M M A R Y
Invasive candidiasis is associated with high mortality rates, ranging from 35% to 60%, in therange reported for septic shock. The epidemiology and pathogenesis of invasive candidi-asis differ according to the patient’s immune status; the majority of cases in immuno-compromised hosts are candidaemia, whereas non-candidaemic systemic candidiasisaccounts for the majority of cases in critically ill patients. In contrast to candidaemia,non-candidaemic systemic candidiasis is difficult to prove, especially in critically ill pa-tients. Up to 80% of these patients are colonized, but only 5e30% develop invasiveinfection. The differentiation of colonization and proven infection is challenging, andevolution from the former to the latter requires seven to 10 days. This continuum fromcolonization of mucosal surfaces to local invasion and then invasive infection makes itdifficult to identify those critically ill patients likely to benefit most from antifungalprophylaxis or early empirical antifungal treatment. Early empirical treatment of non-candidaemic systemic candidiasis currently relies on the positive predictive value of riskassessment strategies, such as the colonization index, candida score, and predictive rulesbased on combinations of risk factors such as candida colonization, broad-spectrum an-tibiotics, and abdominal surgery. Although guidelines recently scored these strategies asbeing supported by limited evidence, they are widely used at bedside and have substan-tially decreased the incidence of invasive candidiasis.ª 2014 The Authors. Published by Elsevier Ltd on behalf of the Healthcare Infection So-
ciety. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/3.0/).
Introduction
Candida spp. colonization develops in up to 80% of criticallyill patients staying more than one week in intensive care,whereas invasive candidiasis is documented in only 5e10% ofthem.1!5 Early diagnosis of invasive candidiasis is difficult; it is
generally late in the course of the infection before microbio-logical evidence is found.6!8 This may delay appropriate anti-fungal treatment and may be in part responsible for its highcrude and attributable mortality rates, comparable to thosereported for septic shock.9!11
Antifungal prophylaxis and early empirical treatment ofsevere candidiasis has improved survival, but may result inoveruse of antifungal agents if indiscriminately prescribed toall patients colonized by Candida spp.12!14 Indeed, extensiveuse of antifungals has promoted a shift to Candida spp. withreduced susceptibility.15,16 Recent guidelines resulting fromexpert consensus provided no high-level recommendationsabout antifungal prophylaxis and empirical antifungal
* Corresponding author. Address: Department of Intensive CareMedicine, Centre Hospitalier Universitaire Vaudois (CHUV), Rue duBugnon 46, 1011 Lausanne, Switzerland. Tel.: þ41 21 314 2923;fax: þ41 21 314 3045.
E-mail address: [email protected] (P. Eggimann).
Available online at www.sciencedirect.com
Journal of Hospital Infection
journal homepage: www.elsevierheal th.com/journals / jh in
http://dx.doi.org/10.1016/j.jhin.2014.11.0060195-6701/ª 2014 The Authors. Published by Elsevier Ltd on behalf of the Healthcare Infection Society. This is an open access article under the CCBY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/3.0/).
Journal of Hospital Infection 89 (2015) 302e308

invasive candidiasis was 16.7% (14/84) in patients receivingplacebo and 9.8% (10/102) in patients receiving caspofungin(P ¼ 0.14). Treatment safety, length of stay, antifungal use,and mortality did not differ between groups. The authorsconcluded that caspofungin prophylaxis was safe, with a non-significant tendency to reduce invasive candidiasis. Twocurrently unpublished studies demonstrated no clinical use-fulness of predictive rules based on clinical factors in guidingempirical antifungal treatment. The first, entitled ‘Pilotfeasibility study with patients who are at high risk for devel-oping invasive candidiasis in a critical care setting’(ClinicalTrials.gov identifier: NCT01045798), was terminateddue to a low recruitment rate after the inclusion of only 15patients. The second study, entitled ‘An exploratory study tocompare the efficacy and safety of micafungin as a pre-emptive treatment of invasive candidiasis versus placebo inhigh risk surgical subjects e a multicentre, randomized,double-blind study’ (ClinicalTrials.gov identifier:NCT01122368), included only surgical critically ill patients.Preliminary results showed a high proportion of invasivecandidiasis cases at study entry. The overall rate of infectiondid not differ between patients receiving pre-emptive anti-fungal treatment (11.1%) and those receiving placebo (8.9%),but the number of patients excluded from the analysis resultedin insufficient statistical power.61
These three studies strongly suggest that despite betterpositive predictive value than colonization index and candidascore, predictive rules may not be feasible at the bedside.
The clinical paradox arising from the use of risk-basedstrategies
The laborious nature of the clinical use and the limitedavailability of solid clinical data explain the low level of evi-dence attributed by experts to these risk-based strategies inconsensus guidelines. Nevertheless, they are widely used atbedside and have succeeded in decreasing the incidence ofinvasive candidiasis.14,17,18,25,62 This picture reflects opposingstrategies: clinicians concerned by the worse prognosis ofdelayed treatment start antifungals early, even in low-riskpatients; whereas experts, more concerned by the negativeecological impact and cost of antifungals, recommend delayedprescription, which risks failing to identify patients requiringearly treatment.
New insight into risk-based strategies
We have emphasized that these diagnostic risk-based strat-egies result in the following paradigm: the most sensitivemethod (colonization index) increases the number of patientsreceiving useless treatment, whereas the most specific method(predictive rules) increases the number of patients notreceiving early antifungals and developing invasive candidi-asis.7,21,23 Objective analysis of the accuracy of the risk-basedstrategies shows that the NPVs of these strategies are muchhigher than their PPVs, for which they were developed(Table II).30,51"54,56 Among them, only the NPV of the candida
Antifungal treatment in critically ill patients ?
Surgical patient at very high risk
Colonization index (CI) Candida score (CS)
High risk of invasive candidiasis
CI ≥ 0.5 or CS ≥ 3 CI < 0.5 or CS < 3
Considerempiric antifungal treatment
Avoidempiric antifungal treatment
Low risk of invasive candidiasis
Antifungal prophylaxis-Anastomotic leakage
-Reopening of the digestive tract
-Surgery on ICU admission (1pt)-Total parenteral nutrition (1pt)-Severe sepsis (2pts)-Candida colonization (1pt)
No. of sites/no. of sites screened2x weekly
No Yes
Risk assessment evaluation
Figure 1. Risk assessment strategies for antifungal treatment.
P. Eggimann et al. / Journal of Hospital Infection 89 (2015) 302e308306
Risk assessment strategies forAntifungal treatment
Eggimann et al, 2015

Resumodasrecomedações paramanejodepacientescomCandidemia
IDSA 2009 ESCMID 2011 SBI 2012
Equinocandinas AI AI AI
L-Anfo B AI (alternativa) BI BI
D-Anfo B AI (alternativa) DI DI
Flu AI para pacientes estáveis???
CI BI (estáveis) ?
Vori AI BI
Combinação Não Recomendado Não recomendado Não Recomendado
> toxicidade que equinocandinas
Não use !!! Não use !!!

Recomendations forthe therapy forinvasiveaspergillosis - IDSA2008
Primary Alternative
Load Voriconazole 6mg/kgIV L-AMB3-5mg/kg/day(AII)*
followedby4mg/kg orABLC5mg/kg/dayororalvoriconazole or CASPO(BII)*200mgevery12h(AI) or MICA(BII)*
POSA(BII)*
WalshTJ,etal.ClinInfectDis.2008;46:327-360.
ChildrenLoad2to11yo,7-8mg/kgFollowedby6mg/kg/twodoses

Review article
Our 2015 approach to invasive pulmonary aspergillosis
B. Liss,1,2 J. J. Vehreschild,1,2,3 C. Bangard,4 D. Maintz,4 K. Frank,5 S. Gr€onke,5 G. Michels,5
A. Hamprecht,6 H. Wisplinghoff,6 B. Markiefka,7 K. Hekmat,8 M. J. G. T. Vehreschild1,2,3 andO. A. Cornely1,2,3,9,10
1Department I of Internal Medicine, University Hospital of Cologne, Cologne, Germany, 2Center for Integrated Oncology CIO K€olnBonn, University of
Cologne, Cologne, Germany, 3German Centre for Infection Research (DZIF), partner site Bonn-Cologne, Cologne, Germany, 4Department of Radiology,
University Hospital of Cologne, Cologne, Germany, 5Department III of Internal Medicine, Heart Centre of the University of Cologne, Cologne, Germany,6Institute for Medical Microbiology, Immunology and Hygiene, University Hospital of Cologne, Cologne, Germany, 7Institute of Pathology, University
Hospital of Cologne, Cologne, Germany, 8Department of Cardiothoracic Surgery, University Hospital of Cologne, Cologne, Germany, 9Cologne Excellence
Cluster on Cellular Stress Responses in Aging-Associated Diseases (CECAD), University of Cologne, Cologne, Germany and 10Clinical Trials Centre Cologne,
ZKS K€oln, University of Cologne, Cologne, Germany
Summary At the University Hospital of Cologne, in general two patient groups at high risk forinvasive aspergillosis receive posaconazole prophylaxis: Acute myelogenous leukaemiapatients during remission induction chemotherapy and allogeneic haematopoietic stemcell transplant recipients. Other patients at risk undergo serum galactomannan testingthree times weekly. At 72–96 h of persisting fever despite broad-spectrum antibiotics,or at onset of lower respiratory tract symptoms a thoracic computed tomography (CT)scan is performed. Without lung infiltrates on CT, IPA is ruled out. In lung infiltratesnot suggestive for IPA mycological confirmation is pursued. In patients without posa-conazole prophylaxis empiric caspofungin will be considered. CT findings typical forIPA prompt targeted treatment, and mycological confirmation. Bronchoalveolar lavage(BAL) is most important for cultural identification and susceptibility testing, and facili-tates diagnosing other pathogens. BAL performance is virtually independent of plateletcounts. If despite suggestive infiltrates BAL does not yield the diagnosis, CT-guidedbiopsy follows as soon as platelet counts allow. Surgery can also be beneficial in diag-nosis and treatment of IPA. If the diagnosis of IPA is not established, mucormycosis isa valid concern. In patients with breakthrough IPA during posaconazole prophylaxisliposomal amphotericin B is the drug of choice. If no posaconazole prophylaxis wasgiven, voriconazole is the treatment of choice for IPA.
Key words: Aspergillosis, mould pneumonia, neutropaenia, voriconazole, liposomal amphotericin B, caspofungin.
Introduction
Current guidelines and recommendations of professionalsocieties are important sources of information. As theymight not always be applicable to specific clinical
settings, we describe our institutional standard clinicalapproach to invasive pulmonary aspergillosis.1–4
Invasive pulmonary aspergillosis is a major challengein the management of immunocompromised patients,due to a unique combination of high attributable mor-tality of ~70% and notorious diagnostic difficulties.5
Incidence rates depend on the underlying disease andon treatments received. In solid organ transplant recipi-ents incidence rates are 1.8–2.7%,6,7 and in haemato-logical malignancy range from 4.7 to 13.1%.5 Despiteprotection of patients with long-term neutropaeniareceiving posaconazole prophylaxis, in general the inci-dence of invasive aspergillosis is increasing.4,8–10 This
Correspondence: Prof. O. A. Cornely, University Hospital of Cologne,
Kerpener Str. 62, 50937 Cologne, Germany.
Tel.: +49 221 478 6494. Fax: +49 221 478 3611.
E-mail: [email protected]
Submitted for publication 5 March 2015
Revised 9 March 2015
Accepted for publication 9 March 2015
© 2015 Blackwell Verlag GmbH doi:10.1111/myc.12319
mycosesDiagnosis,Therapy and Prophylaxis of Fungal Diseases

development may be due to rising patient numbers invulnerable populations,11 as well as more frequent useof aggressive therapies.12
Patients in intensive care units (ICU) apparentlyare at increased risk, but this is not yet understood,owing to the heterogeneity of their underlyingdiseases and the lack of a definition of ICU itself.Susceptibility in any of these patient groups isenhanced by factors as diverse as use of gluco-corticosteroids and other immunosuppressants,13 pre-existing structural lung damage14–16 and geneticpredisposition.17,18
Timely treatment reduces mortality rates,19 but isoften hampered by a lack of specific clinical signs andsymptoms,20 and by unreliable in vitro diagnosticassays.21 A standardised approach may increase physi-cian compliance and thus diagnostic yield allowingearlier targeted treatment and subsequently lead toimproved outcome.22–24 At our university hospital, wefollow standard operating procedures (SOP) for diagno-sis and treatment of infections in neutropaenic hosts.In an additional poster format the ‘febrile neutropae-nia SOP’ are readily available on our haematologyand stem cell transplant wards. In addition, they areweb-based 25 (Fig. 1 and Fig. 2) for easy reference.They follow published evidence and guideline docu-ments of professional societies, e.g. ECMM, ESCMID,DGHO and are frequently updated.1–4
Diagnostic strategy
Patients with acute myelogenous leukaemia, myelo-dysplastic syndrome (AML/MDS) or severe aplasticanaemia and recipients of allogeneic haematopoieticstem cell transplantation receive posaconazole prophy-laxis at our institution.4,9,10,26 Posaconazole prophy-laxis has been included into the appropriatechemotherapy regimes in our ordering software.Patients ineligible for azole prophylaxis, e.g. those withacute lymphoblastic leukaemia, undergo serum galac-tomannan screening three times weekly.27,28
The most prevalent, but unspecific sign of invasivepulmonary aspergillosis, is persistent fever despite broad-spectrum antibiotic treatment, reported in up to 100% ofpatients.20,29 A computer tomographic scan is orderedafter 72–96 h of persistent fever and is performed within24 h, usually on the same day. This thoracic CT scanwithout contrast enhancement is a rapid procedure,thus not interfering with planned examinations in ourradiology department. In any patient with lower respira-tory tract symptoms a CT scan is ordered independent ofthe presence and duration of fever.30 Diagnostic imagingis of utmost importance as all further diagnostic andtherapeutic decisions depend on CT findings. We broadlycategorise into no infiltrate, infiltrate not suggestive ofinvasive pulmonary aspergillosis, and infiltrate sugges-tive of invasive pulmonary aspergillosis, i.e.
No infiltrate
High probability of invasive aspergillosis
Unspecific infiltrate
Targeted therapy
No pathogen identified
Infiltrate suggestive of fungal infection (nodule, halo, cavity, air-crescent)
Microscopy with septate hyphaeor galactomannan
(≥0.5 BAL or 2x in serum)
Bronchoalveolar lavage – specific test:Galactomannan, PCPRespiratory viruses
Bacteria (including TBC)
Chest CT without contrast
NoYes
Invasive mold infection likely
Targeted aspergillosis therapy No targeted therapy
Other pathogenidentified
Figure 1 Diagnostic algorithm for persistently febrile patients at risk of invasive pulmonary aspergillosis.
© 2015 Blackwell Verlag GmbH2
B. Liss et al.

Primary Therapy forInvasiveAspergillosis in2015
Amphotericin B58%
PatientsS
urviving(%
)
Weeks
Voriconazole 71%
Herbrecht etal.NEngl JMed.2002;347:408-415.
13%Survivalbenefit
MortalityDuetoAspergillosis (%)
13%
29%
Voriconazole Ampho B
16%p>0.001

Fluconazole Voriconazole
Tablets (50-200 mg) e Intravenous (200 mg)
Hepatic metabolism (drug to drug onteractions)IV: solution may be not indicated ifCreatinine Clearence < 50
More toxic than FlucoErratic plasma levels: Montitoring is indicated
SpectrumofFlucoCandida,CryptococcusDermatophytes
In vitro activity of voriconazole
Aspergillus sp., Candida spp.
Fusarium spp,
S. apiospermum P. brasiliensis,
H. capsulatum, B. dermatitidisCoccidioides spp,
P. marneffey, C. neoformans, Black fungi
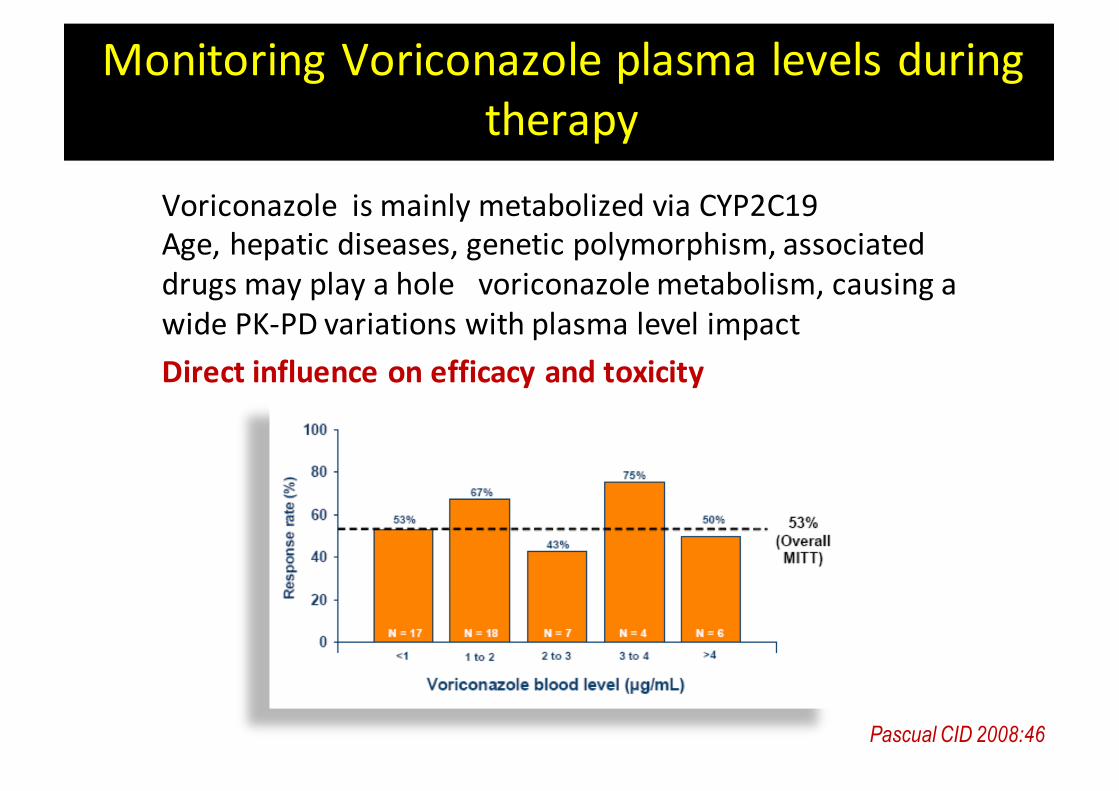
MonitoringVoriconazoleplasmalevelsduringtherapy
VoriconazoleismainlymetabolizedviaCYP2C19Age,hepaticdiseases,geneticpolymorphism,associateddrugsmayplayaholevoriconazolemetabolism,causingawidePK-PDvariationswithplasmalevelimpactDirectinfluenceonefficacyandtoxicity
Pascual CID 2008:46

• 459 patients were randomized, 454 received at least one dose of study medicationo 182 International sites (02 sites in Brazil)o 15 patients from our site
• 277 patients with confirmed proven or probable IA were included in the MITT o Voriconazole + Anidulafungin: 135o Voriconazole + placebo: 142
MarretalAnnInt Med2015

o Reduction in all-cause mortality at 6 weeks with voriconazole/anidulafungincombination compared to voriconazole monotherapy, but this difference did not meet criteria for superiority
o However, there was a 33% relative reduction in all-cause mortality at 6 weeks with voriconazole/anidulafungincombination compared to voriconazole monotherapy
voriconazole/anidulafungin CombinationStudy
Primary Endpoint (MITT)
Marr et al Ann Int Med 2015
39/142
26/135
All – Cause mortality at 6 weeksVORI + ANIDULA VORI monotherapy

Primary Endpoint and Post-hocAnalysis
Primary endpoint Sub-group analysis of patients with positive galactomannan at baseline
Marr et al Ann Int Med 2015

voriconazole/anidulafungin Combination Study All-Cause Mortality at 6 Weeks By Basis for Diagnosis
o All-cause mortality at 6 weeks was lowest in patients with GM-based diagnosis of probable IA, suggesting that the infection was identified at a relatively early stage.
4/9 14/50 47/218Marr et al Ann Int Med 2015
The benefit of antifungal combination treatment remains a matter of debate, despite increasing utilization and promising results in certain subgroups.
o All-cause mortality at 6 weeks was lowest in patients with GM-based diagnosis of probable IA, suggesting that the infection was identified at a relatively early stage.
o This is the patient group with the best opportunity for improved outcomes with combination treatment compared to monotherapy
BiofilmrelatedInfections

• SECURE Study – Invasive aspergillosis – compared to voriconazole
• ACTIVE study– Candidemia – compared to echinocandin followed by
azole• VITAL study (non-comparative)
– Mucormycosis, fusariosis, cryptococcosis, endemic mycosis (PCM, Histo, Cocci)and patients with renal impairment
Isavuconazole Clinical Trials

• SECURE Study - Invasive aspergillosis• 516 patients with hematologic malignancies, 66% neutropenic and 20%
allogeneic HSCT– About 50% were mycologically confirmed invasive aspergillosis
• Compared to IV/PO voriconazole• Primary endpoint: all-cause mortality through day 42 in the ITT population
• 18.6% (ISA) vs 20.2% (VRC)• DRC-assessed overall response (clinical, mycological and radiological
responses) at EOT (50 days)– 35.0% (ISA) vs 36.4% (VRC)
• statistically fewer adverse events– hepatobiliary (8.9% vs. 16.2%), skin (33.5% vs. 42.5%), eye disorders
(15.2% vs. 26.6%)
SECURE study (ISA x VORI in Invasive Aspergillosis

Posaconazole
Itraconazole
In vitro activity: Aspergillus sp., Candida sp., Fusarium sp*., MucoralesP. brasilensis, H. capsulatum, B. dermatitidis C. immitis, P. marneffey, C. neoformans, Dematiaceous, Secedosporium apiospermum
*Sensibility is species related
• Main indications for posaconazole• prophylaxis (LMA, MSD, GVHD)
• Refractory fungal infections• Several fungal infections• Formulations: Oral solution, Delayed-Release Tablets, IV solution

Antifungal Spectrumof Triazoles
Candida Aspergillus Fusarium Zigomycetes Cryptococcus
Fluco ++ - - - +++
Itra ++ +++ - - ++
Vori +++ +++ ++ - +++
Posa +++ +++ ++ ++ +++
Isavu +++ +++ + + +++

Epidemiologic changesofIFDinOncohematologic patients
0
0,5
1
1,5
2
2,5
3
3,5
4
4,5
5
1989 1993 1997
Year
Rat
e (p
er 1
,000
aut
opsi
es)
Candidiasis Aspergillosis
Kumeetal.Pathology International2003
Fluconazole 200-400 mg/day
EmergenceofCandidaspp - Fluco resistant(C.glabrata eC.krusei)EmergenceofInvasiveMoldInfections

Profilaxia com Posaconazol emNeutropênicos (LMA ou SMD)
Objetivo do estudo
Avaliar eficácia de posaconazol x fluconazol ouitraconazol em prevenir DFI.
População: 602 pacientes de alto risco (QT para LMA ou SMD)
Posaconazol solução oral 600mg/d (200mg 3x/dia) com alimentos x fluconazol (400mg/d) ou itraconazol(200mg 2x/dia)
Cornely OA et al. N Engl J Med. 2007;356:348-359.

Posaconazol Profilático em PacientesNeutropênicos
0 20 40 60 80 100DaysAfterRandomization
0.15
0.10
0.05
0.00
P =0,003*
Prob
abilityofInvasive
FungalInfection
Posaconazol
Fluconazol ou Itraconazol
CornelyOAetal.NEnglJMed.2007;356:348-359.
Resultados:TempoparaapresentarDFI
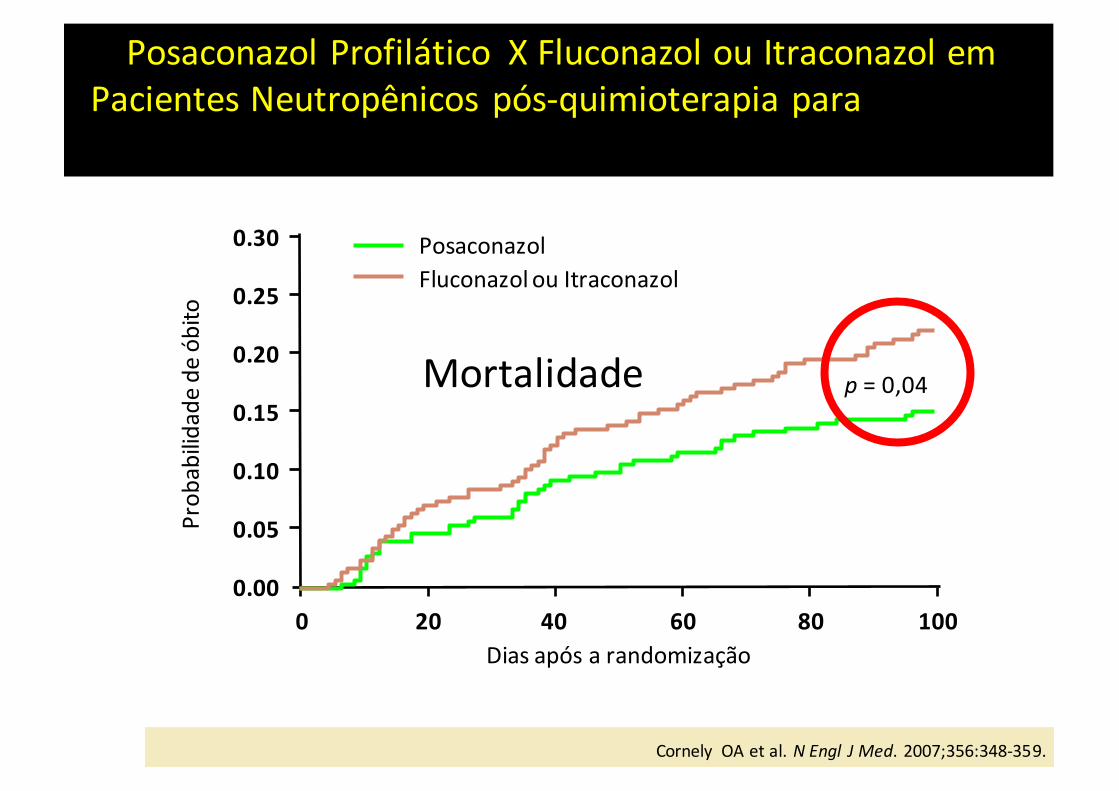
Posaconazol Profilático XFluconazol ou Itraconazol emPacientes Neutropênicos pós-quimioterapia para MDS/LMA
0 20 40 60 80 100Diasapósarandomização
0.30
0.20
0.10
0.00
Prob
abilid
adedeóbito
PosaconazolFluconazolouItraconazol
0.25
0.15
0.05
p =0,04
Cornely OAetal.NEngl JMed.2007;356:348-359.
Mortalidade

Response rate Mean plasma concentration
24% 0.13 mg/l
50% 0.85 mg/l
75% 1.48 mg/l
• Recommended to be taken with a full meal to maximise absorption
• Evidences for plasma levels variations (itraconazol <voriconazol< posaconazol)
Issues related to POSA plasma levels(oral solution)
Walsh TJ, et al. Clin Infect Dis 2007; 44: 2-12

DividingtheDoseofPOSAIncreasesAbsorption
Fasted Healthy Volunteers
800 mg once daily400 mg twice daily200 mg four times daily
050
100150200250300350400450
0 4 8 12 16 20 24 28 32 36 40Time (h)
Posa
cona
zole
Plas
ma
Conc
entra
tion (
ng/m
L)
44 48
Ezzet F et al. Clin Pharmacokinet. 2005;44:211-220.

POSAsol.oraleDRT(cáps deliberação prolongada)
PercivaletalCurr FungalInfectRep,2014

• Nodular shape, with or without halo (Fig. 3),
• Cavity within area of consolidation or ‘air-crescent’(Fig. 4).
A reversed halo sign demands immediate attention, too.Suggestive of mucormycosis it is beyond the topic of this per-spective article and has been dealt with elsewhere.3,31,32
Decision tree guided by CT findings
Persistent fever without infiltrate
This is the case in 34.5% of our patients at risk(Fig. 5). Invasive pulmonary aspergillosis is ruled out.If the patient received posaconazole prophylaxis, this
will be continued. No empiric antifungals are initiatedand this approach is safe and effective.33
In this clinical situation any single diagnostic testwill have a low yield, but identifying the cause of feverprevents polypragmatic treatment. In the absence oflocal symptoms during immunosuppression imaging ofthe paranasal sinuses rules out sinusitis. Repeatedblood cultures can help identify blood stream infectionby difficult to culture organisms or, e.g. Candida spp.34
Posaconazole serum concentration may be deter-mined if the oral suspension is used, although no un-controversial target level has been defined.35–38 Serumconcentration is difficult to predict despite the use ofcomplex models identifying correlating factors.39,40
Use of posaconazole tablets renders therapeutic drugmonitoring generally obsolete.41
If the patient was not receiving posaconazole pro-phylaxis, empiric antifungal treatment is consid-ered.42,43 Additional blood cultures are mandatorybefore the empiric antibiotic regimen may beswitched,43 and abdominal infection should be consid-ered.44,45 MRI can help identify aspergillosis of bonesand joints.46 If fever of unknown origin persists, tho-racic CT scans will be repeated weekly.
Infiltrate non-suggestive of invasive pulmonary
aspergillosis
This situation is encountered in 36.6% of our patients(Fig. 5). Invasive pulmonary aspergillosis is possibleand needs to be ruled out. If galactomannan screeningresults were negative, or not done, e.g. in the case ofposaconazole prophylaxis, bronchoalveolar lavage(BAL) is indicated. While we test BAL fluid for bacte-rial and viral infection, we in particular aim at
CT at d7 and d14
Voriconazole6 mg/kg BID d14 mg/kg BID i.v.
Liposomal amphotericin B3 mg/kg QD i.v.
Caspofungind1 70 mg QD50 mg QD i.v.
Posaconazole prophylaxis received?
YesNo
Consider oral treatment after at least 7 d i.v.
treatmentConsider biopsy
Respone/stable Progression at 14 d
Figure 2 Therapeutic algorithm for patient with high probabilityof invasive pulmonary aspergillosis.
Figure 3 Invasive pulmonary aspergillosis in a patient with mul-tiple myeloma: Two spiculated infiltrates in the left upper lobe,each with surrounding halo.
Figure 4 Invasive pulmonary aspergillosis in a patient withAML: Infiltrates in both lungs with ‘air-crescent sign’ in the larg-est infiltrate.
© 2015 Blackwell Verlag GmbH 3
Approach to invasive pulmonary aspergillosis
E quando ocorre DFI de escape durante a profilaxia?Liss et al Mycoses 2015

Stewardship dePosaconazol(POSA)emprofilaxiaeterapêuticade
resgateGrupo de Padronização de Antifúngicos (GPA)
Flavio de Queiroz Telles - InfectologiaClóvis Arns da Cunha – Infectologia e TMOFelipe Tuon – InfectologiaTony Tahan - InfectopediatriaRafael Mialski – InfectologiaFrancisco Beraldi Magalhães – InfectologiaHugo Morales – CCIHIzelândia Veronese – CCIHAdriana Elias de Souza – Unidade de FarmáciaGisela Lucas – Unidade de FarmáciaVaneuza Funke – Hematologia e TMOViviane Carvalho Hessel Dias – CCIH, HNGCarla Sakuma – Infectologia - UNIOESTE

PrincipaisindicaçõesdePOSA
• Profilaxia primária– Hematologia Clínica– Transplante de Cels Hematopoiéticas
• Terapêutica de DFI refratária– Micoses oportunísticas– Micoses endêmicas
• Idade ≥ 13 anos• < 13 anos, uso “off label” 04/mg/kg”
GPA

IndicaçõesdeprofilaxiaprimáriacomPOSAemHematologiaClínica
• Paciente com LMA em primeira indução, excluindo-se re induções e casos refratários. Previsão de Neutropenia prolongada
• Portadores de neoplasias hematológicas secundárias ou em recaída, principalmente de grupo citogenético desfavorável ou ainda que possuam mutações selvagens NPM1 ou FLT3/IDT.
• Portadores de co-morbidades que aumentem o risco para DFIs, como diabetes, DPOC, tabagismo crônico, sobrecarga de ferro ou doença viral pulmonar.
• Pacientes fatores de risco para DFI internados nas enfermarias de Hematologia Clínica, que não estão sob a proteção de filtro HEPA.
GPA

– Pacientes que irão receber transplantes com condicionamentos mieloablativos ou de sangue de cordão umbilical
– Neutropenia prolongada na indução de receptores de doadores haploidênticos ou não aparentados com incompatibilidade
– Pacientes que no período pós-transplante estejam recebendo altas doses de corticosteroides ou com DECH grave (III/IV)
– Pacientes com falha de pega do enxerto, DECH ou reativação de infecção por citomegalovírus (CMV)
– Pacientes portadores de co-morbidades que aumentem o risco para DFIs, como diabetes, DPOC, bronquiolite obliterante, tabagismo crônico, sobrecarga de ferro ou doença viral pulmonar
IndicaçõesdeprofilaxiacomPOSAemreceptoresdeTCH
GPA

IndicaçõesdePOSAemProfilaxiasecundáriadeDFIs
– Pacientes que anteriormente apresentaram DFI provável ou provada por fungos filamentosos (Aspergillus, Fusarium, Mucormicose, Hialohifomicoseou Feohifomicose)
– Pacientes que anteriormente apresentaram DFI possível por fungo filamentoso, com resposta a terapêutica antifúngica padrão
GPA

• Micosesoportunísticas*– Aspergilose invasiva,Fusarioseinvasiva,Mucormicose,Hialohifomicose eFeohifomicose
**considerarprognósticoedisponibilidadelocaldeANFO-Blipídica
• Micosesendêmicas**– Paracoccidioidomicose, Histoplasmose,CocciCromoblastomicose eEumicetomas
**considerarprognósticoeduraçãodotratamento
IndicaçõesdePOSAemMicosesRefratárias
GPA

RecomendaçõesgeraisparaprescriçãolocaldePOSA
• AvaliarocustolocaldeantifúngicossistêmicosdisponívelnaInstituição
• AnalisarosdadosdevigilânciaepidemiológicadasDFIs:incidência,etiologiaeresistência
• Semprequesolicitada,aprescriçãodePOSAdeveráservalidadapeloCCIHemconsonância comoServiçodeInfectologiadoHC-UFPR.
GPA