aortic dissection, and its complications dominik fleischmann department of radiology stanford...
TRANSCRIPT

Aortic Dissection, and its Complications
Aortic Dissection, and its Complications
Dominik FleischmannDepartment of RadiologyStanford University
Dominik FleischmannDepartment of RadiologyStanford University
20th Annual Summer Practicum, Masters in Body ImagingJackson Lake Lodge, Moran, Wyoming
August 8-11, 2010

Research support: General ElectricSpeaker's board: Bracco
Siemens
Dominik FleischmannDepartment of RadiologyStanford University
Dominik FleischmannDepartment of RadiologyStanford University
Conflicts of Interest Disclosure
20th Annual Summer Practicum, Masters in Body ImagingJackson Lake Lodge, Moran, Wyoming
August 8-11, 2010

Background & Clinical Context
Acute aortic syndrome:
acute life-threatening abnormalities of aorta assoc. with intense chest or back pain, traditionally include:
Aortic dissection (AD), Intramural hematoma (IMH), Penetrating atherosclerotic ulcer (PAU)
RARE: 2.6-3.5 /100k/yr in US
(440 /100k/yr for myocardial infarction)
LIFE THREATENING
DIAGNOSIS/MANAGEMENT: IMAGING BASED

• 40% die immediately (~50% within 48 hrs) mainly from rupture
• 2% per hour mortality (1-3% die in hour before surgery)
• end-organ malperfusion occurs in 16-30%, dramatically reduces survival
• short term (in-hospital and 30 day) mortality: 3.4% - 25%
Acute aortic syndromes
Natural History of Type A Dissection(approx 60% of dissections are Type A)

Acute Aortic Syndromes Imaging Strategy
Precontrast series • mandatory in acute setting
CTA series• CTA chest-abdomen-pelvis scanning range: thoracic inlet femoral a. bifurcation !!
• Gated chest + (abd.-pelv. non-gated CTA)
3mm/3mm
Thick./Rec.-Int.
1mm/0.7mm

Acute aortic syndrome: MUST HAVE non-contrast acquisition
• 62 year old man with hypercholesterolemia and hypertension;
• in morning squeezing chest pain, back pain
non contrast CT
Intramural Hematoma

Acute Type B DissectionEvaluation of femoral artery access for
intervention
left femoral a.: true lumen
right femoral a.: false lumen

Clinical 3D and 4D Imaging of the Thoracic Aorta
49 year old man
acute chest pain;
RR 170 / 20
Gated CTA of chest (+ abd pelv)
• r/o aortic disease

CT of the Thoracic Aorta
with ECG gating

Copyright ©1999 American Heart Association
Sven
sson
, L.
G.
et
al. C
ircu
lati
on 1
999;9
9:1
331-1
336
Top, TEE of patient 2 whose initial clinical presentation was suspicious for aortic dissection but in whom no dissecting flap or hematoma was found, although aortic aneurysm was noted
Dissection variant: Limited Intimal Tear

72 y.o. man, aneurysmal ascending aorta, chest pain

lumenAdventita
MediaIntima
Aortic Dissection: Manifestation of a Diseased Media
‘cystic medial necrosis’• elastolysis (elastic & collagen fiber loss)
• mucoid degeneration • smooth-muscle cell loss and
dedifferentiation Fedak, P. W.M. et al. Circulation 2002
Elastic Lamina of Aortic Wall
• Marfans (fibrillin)• Ehlers Danlos IV (collagen)• familial TAA• severe hypertension !!!!• normal aging
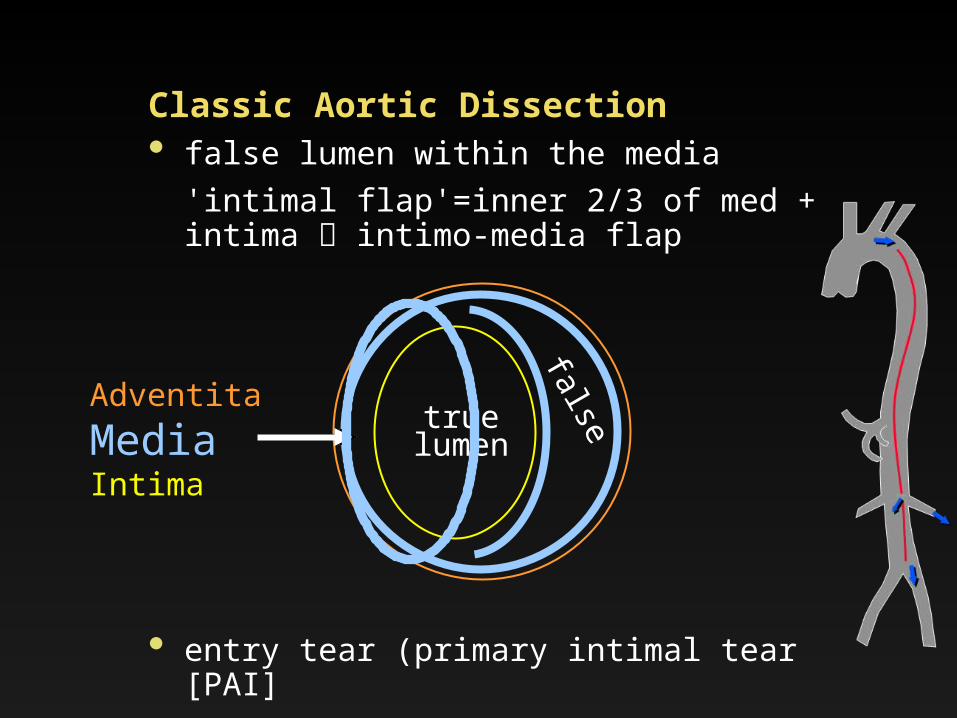
Classic Aortic Dissection• false lumen within the media
'intimal flap'=inner 2/3 of med + intima intimo-media flap
truelumen
falseAdventita
MediaIntima
• entry tear (primary intimal tear [PAI]• exit tear(s) ['reentry tear',
fenestrations]

Acute Type–A Dissection
CTA
primary intimal tear true / false lumen (DSA)
DSA
IMH BI^V
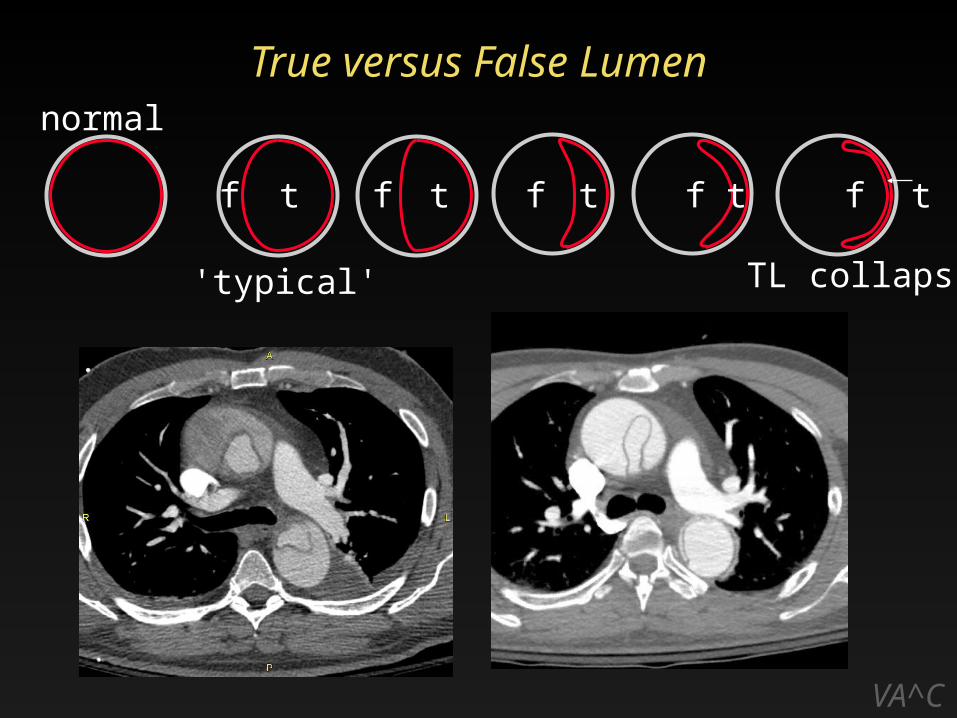
True versus False Lumen
VA^C
tttt t
normal
f f f f f
'typical' TL collaps

True versus False Lumen
VA^C
tttt t
normal
f f f f f
intima-intussusception
'typical' TL collaps
'complex' ‘pseudonormal’
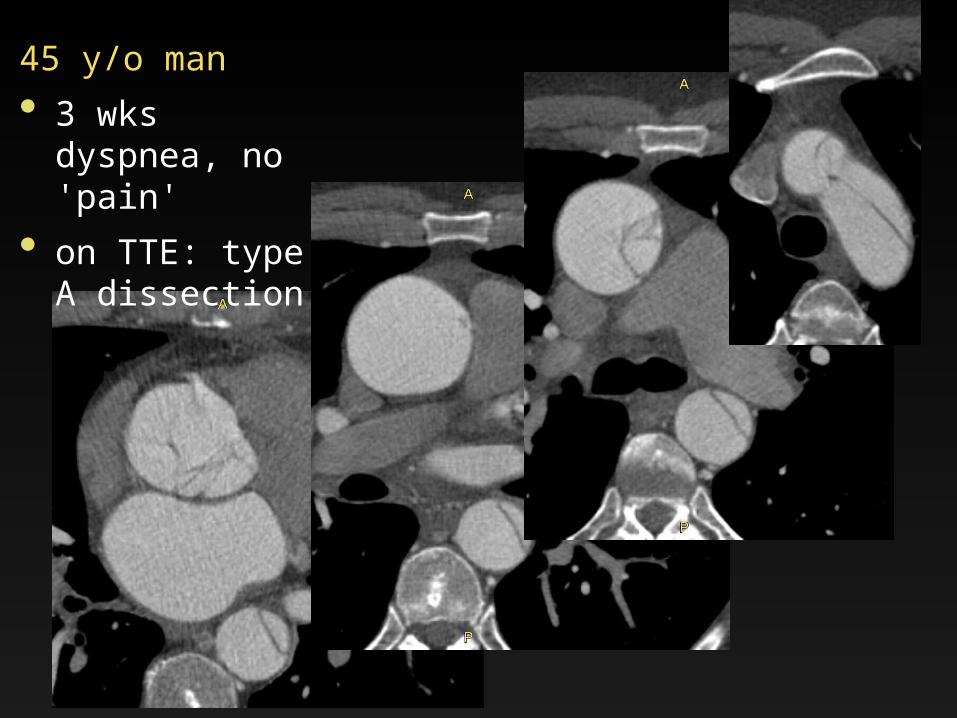
45 y/o man
• 3 wks dyspnea, no 'pain'
• on TTE: type A dissection

45 y/o man
• 3 wks dyspnea, no 'pain'
• on TTE: type A dissection

Small PIT
Prolapse
Primary Intimal Tear (PIT)
Large / Circumferential PIT
Intimal intussusception

48 yo man
• hx of crack cocain use;
• outside hx of type-A IMH which was evacuated, but not repaired
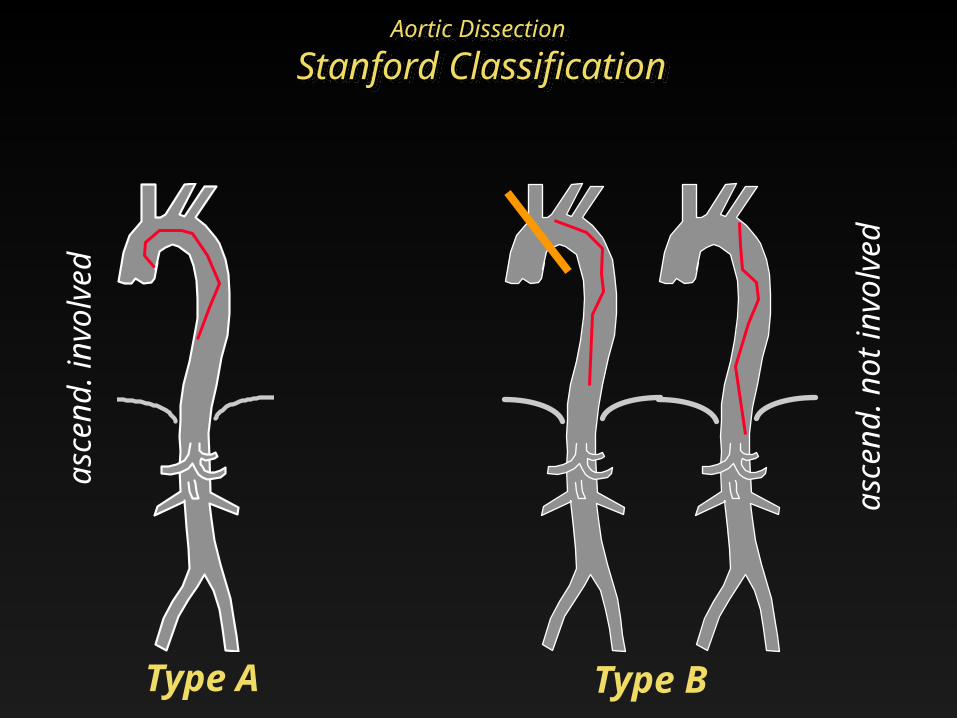
Aortic Dissection
Stanford ClassificationAortic Dissection
Stanford Classification
Type A Type B
asce
nd.
invo
lved
asce
nd.
not
invo
lved

Type A dissection/IMH
75 y/o hypertensive man, acute chest pain,
and left hemothorax
05-Dec
Treatment with descending ao. Stentgraft
desc.ao. intimal tear
17-Dec

Aortic Dissection
Stanford Classification Subclass. site of tear)
Type A: intimal flap involving ascending ao.
immediate surgery
subtype: asc / arch / desc / other [no])
Type B: no involvement of asc.ao.
conservative, unless complicated
subtype: arch / desc / other [no])Daily PO et al, Ann Thorac Surg. 1970;10:237-247
Primary intimal tear important !
endovasc. treatment target

Aortic Dissection – Stanford Subclassification
168 patients operated for acute dissections
(* arch in 10 of 11)(Lansman, Griepp; Ann Thorac Surg 1999;67:1975–1978)
Asc. Arch Desc. Mult.* None
TYPE A (n=139)
83 (60%)
31 (22%)
8 (6%)
11 * (8%)
4 (3%)
TYPE B (n=29) n/a 1 21 0 2
Sta
nfo
rd T
YPE
Subclass. site of tear)
1/3rd 'retro-A'

Acute Aortic Dissection
Complications
• (contained) rupture, leakage tamponade; aortic regurgitation (Type A)
• side branch malperfusion syndromes:
(in approx. 1/3rd of acute type A diss), substantially reduces survival
Type A: coronary, cerebral + ...
Type A&B: renal, mesenteric, peripheral, paraplegia

Aortic DissectionSide-branch Malperfusion
Mortality coronary arteries ~ 25% cerebral arteries/parapl. ~ 45%
renal (ATN, hypertens.) ~ 50-70 % mesenteric ~ 50-95 % peripheral (extremity) ~ 45 %
Diagnosis• clinical• labs
CT cannot diangose mal-perfusion !!

Aortic DissectionSide-branch Malperfusion
Possible mechanisms• local obstruction at branch ostium• limited in- (out-)flow into true (or false)
lumen
Role of CT in side branch malperfusion once diagnosis is established/suspected
• identify detailed anatomy to infer and• explain mechanism ('flow')
treatment consequence !
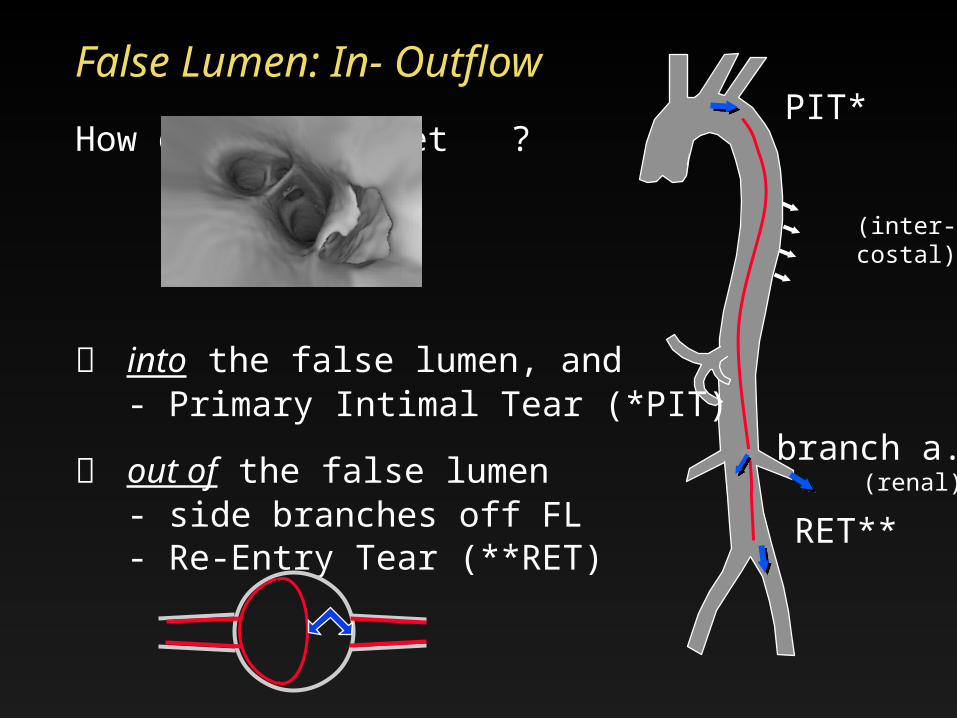
False Lumen: In- Outflow
How does blood get ?
into the false lumen, and - Primary Intimal Tear (*PIT)
out of the false lumen - side branches off FL
- Re-Entry Tear (**RET)
PIT*
RET**
branch a.(renal)
(inter-costal)
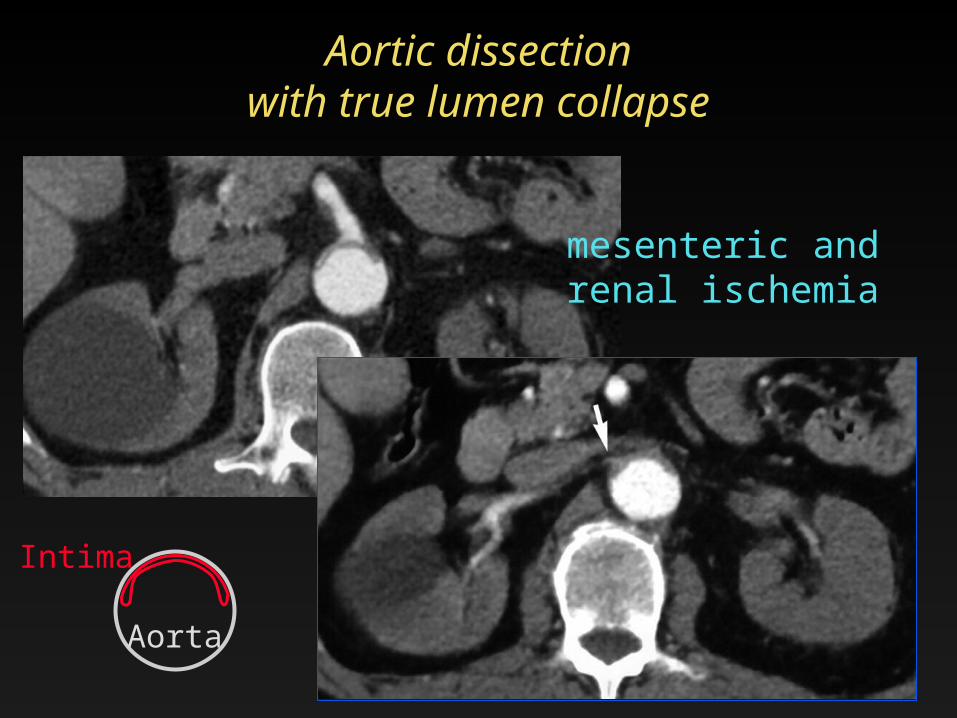
Aortic dissectionwith true lumen collapse
mesenteric and renal ischemia
Intima
Aorta

Type B dissection with TAAA

Type B dissection
• true lumen collapse,left renal artery occlusion with stent-placement

Local Side Branch Involvement in Dissection
natural fenestration('reentry tear', if large)
loca
l flow
-lim
itin
g lesi
on
s
diss. ext. into branch(es) /w stenosis
torn flap within branch /w stenosis
windsock in branch /w stenosis/occlusion
un
com
pli-
cate
d
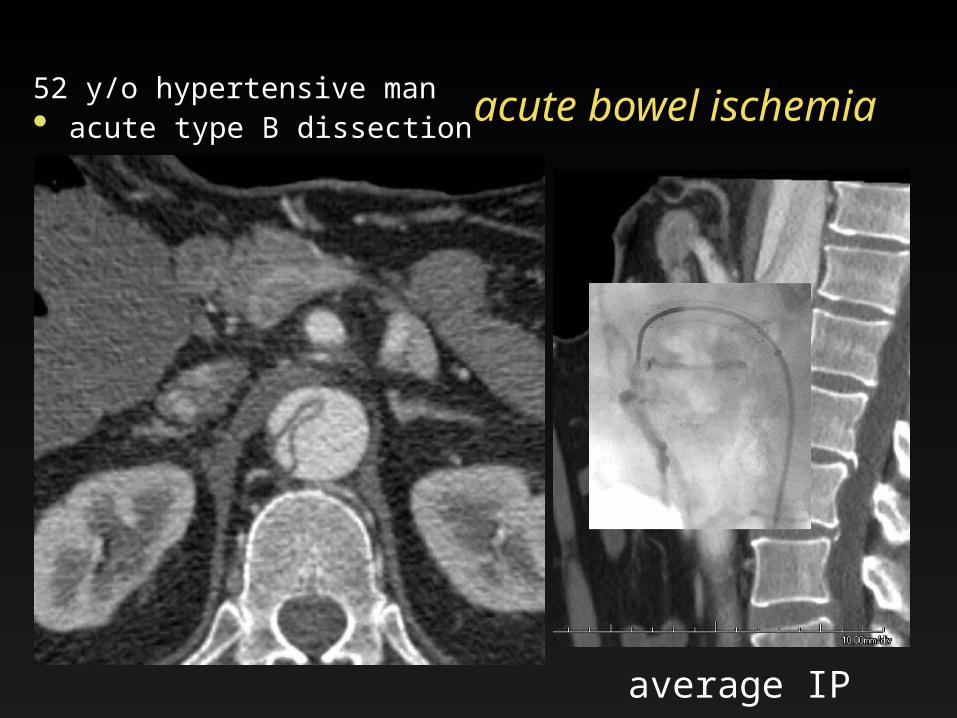
average IP
acute bowel ischemia52 y/o hypertensive man• acute type B dissection
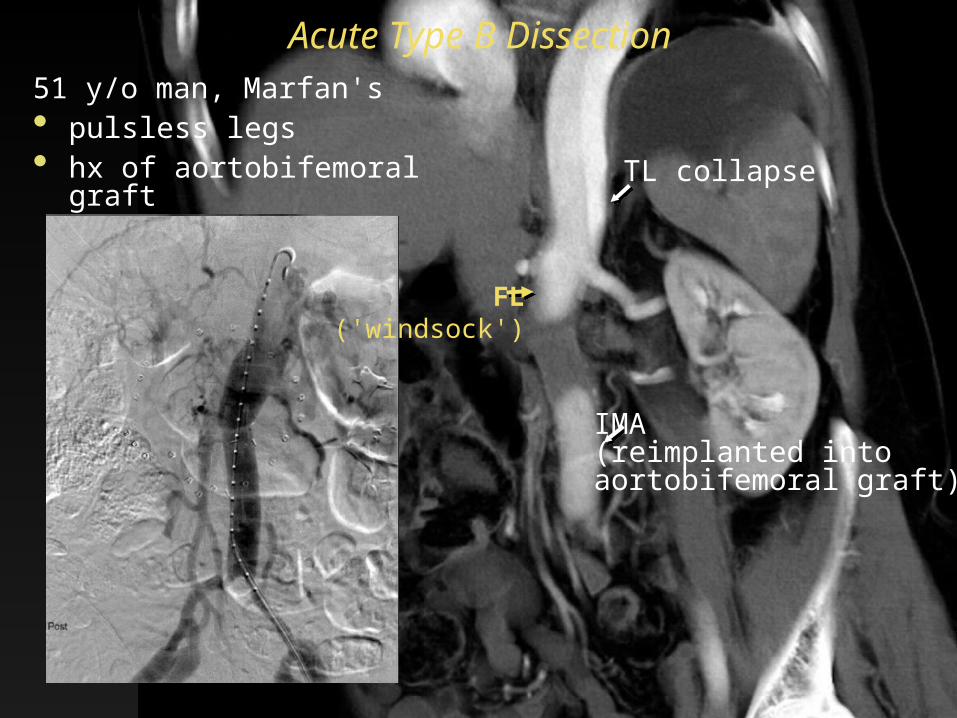
51 y/o man, Marfan's• pulsless legs• hx of aortobifemoral graft
Acute Type B Dissection
False lumeninjection
TL collapse
IMA(reimplanted into aortobifemoral graft)
FL('windsock')

Diagnostic information sought in patients Acute Aortic Syndromes
SUMMARY
• lesion detection, characteriz. (AD, IMH, PAU) incl. signs of leakage / rupture
• involvement of ascending aorta (type A vs B) pericardial effusion involvement of coronary arteries / aortic valve
apparatus
• location of entry tear (or ulcer, if PAU)
• distal extent (anatomic) for roadmap
• side branch involvement / mechanism

Acute aortic syndromes
Aortic dissectionClassic aortic dissection Intramural hematomaDissection variant 'limited tear with aortic bulge' = 'dissection without intimal flap' = 'subtle/discrete dissection
Intramural hematoma (NO DISEASE)
Penetrating atherosclerotic ulcerwith intramural hematoma
(Traumatic transection)(Rupturing/leaking aneurysm)
Dise
ase
d m
ed
iaD
isease
d
intim
a
Semin Thorac Cardiovasc Surg 2008 (Dec) 20:340-347