apd vs capd - msn.org.my · t h e p a tie n t's h e lp e r w o u ld b e tr a in e d to r e m o...
TRANSCRIPT

Does APD vs CAPD plays a role in Better Outcome?
Dr Lily Mushahar
Department of Nephrology
Hospital Tuanku Ja’afar
PD Masterclass 2018
Le Meridien Putrajaya
6-7 October 2018

Outline
• APD vs CAPD: Any difference in patient outcome?• Solute clearance• Residual renal function• Quality of life• PD related infection• Technique survival• Patient survival

History of Peritoneal
Dialysis
Ebers Papyrus (1550 BC)

Successful History of Treating Acute Kidney injury
1946 – Seligman, Fine & Frank developed
closed PD system using 2 catheters

History of CAPD
1976 – first application of CAPD using glass containers by Moncrief & Popovich
1977 - exchanging with plastic bag was introduced by D. Oreopolous
1980’s – introduced in Malaysia - non-disconnecting
system
1990’s – Y disconnect system was introduced
6
The First CyclersThe First Cyclers
1962- Developed by Boen
The first automated peritoneal delivery system
S.T. Boen, C.M. Mion, F.T. Curtis and G. Shilipetar developed an automated
device to do peritoneal dialysis at home. It utilized a 40-liter bottle that was
filled and sterilized at the University of Washington. The bottles were delivered
to the patient's home and returned to the hospital after use.
A cam cycler timer was used to meter the peritoneal fluid into and out of the
peritoneal cavity. A heater plate heated the solution to body temperature and
the effluent from the peritoneum was measured.
Fred Boen, MD, used the "repeated puncture" method for access. This
required that a physician go to the patient's home and surgically place a 14F
trocar in the patient's abdomen. The patient's helper would be trained to
remove the trocar after the peritoneal dialysis treatment.
Boen ST, Mion CM, Curtis FK, Shilipetar G. Periodic peritoneal dialysis using
the repeated puncture technique and an automatic cycling machine. Trans Am
Soc Artif Intern Organs. 196; 10: 408-14.
In 1966 lasker introduced a simple gravity fed cycler. This device used sterile
dialysate in 2 l glass bottles, plastic tubing for delivery and a plastic bag for
collection of dialysate.This was the forerunner of all modern cyclers. This
system could deliver variable amout of warm dialysate.
6
History of APD
Introduced by Boen in 1964

Modalities of PD

ManualVs
Automation

CAPDAPD
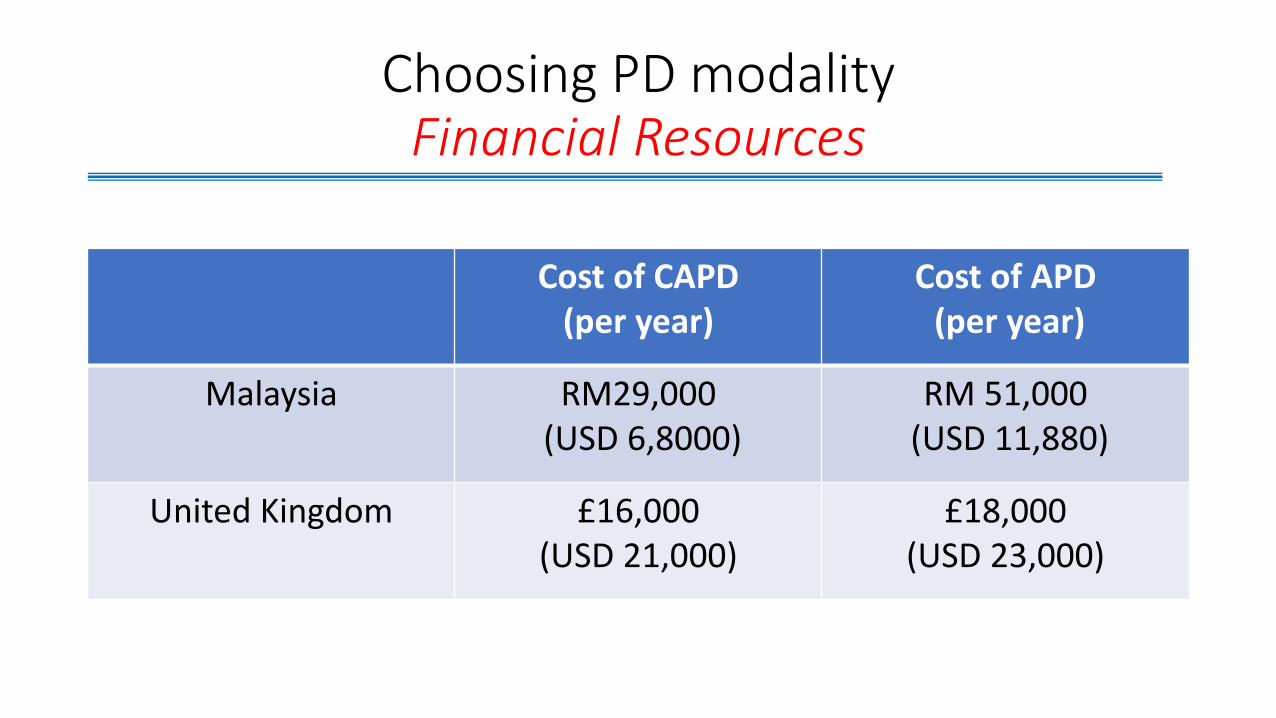
Choosing PD modalityFinancial Resources
Cost of CAPD (per year)
Cost of APD(per year)
Malaysia RM29,000(USD 6,8000)
RM 51,000(USD 11,880)
United Kingdom £16,000 (USD 21,000)
£18,000(USD 23,000)

CAPD vs APD Usage in Malaysia
1464
1662
1838
19962064
2178
2455
2773
3208
3746
88144 121
246296
371 404477 497
569
1552
1806
2083
2212
2360
2549
2859
3250
3705
4315
0
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Nu
mb
er
of
pat
ien
ts
CAPD APD Total

CAPD vs APD Usage in other Countries
Developing Country Developed Country
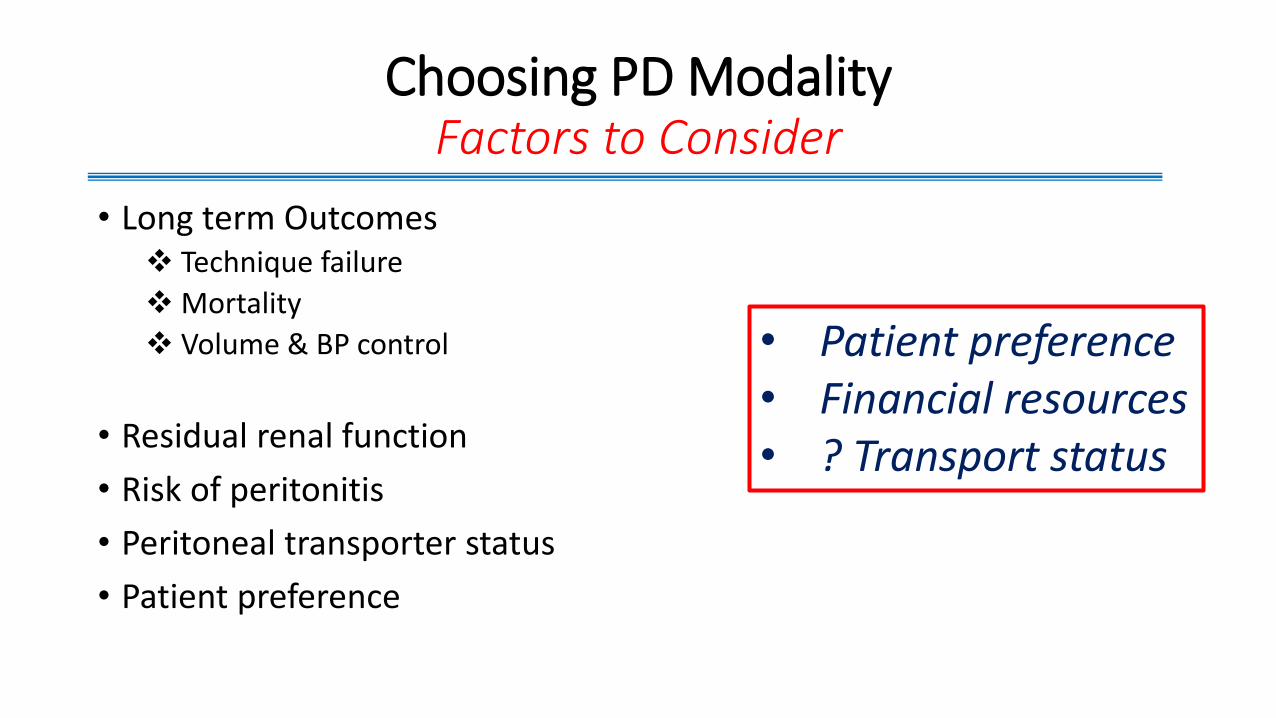
Choosing PD ModalityFactors to Consider
• Long term Outcomes Technique failure
Mortality
Volume & BP control
• Residual renal function
• Risk of peritonitis
• Peritoneal transporter status
• Patient preference
• Patient preference• Financial resources• ? Transport status

Traditional APD Indications
• Enhance small solute clearances
• Enhance ultrafiltration (esp high transport)
• Social reasons• Employment
• School
• Care of elderly/debilitated patients
• Mechanical problems• Hernias, leaks, back pain, body image
• Reduce peritonitis rates
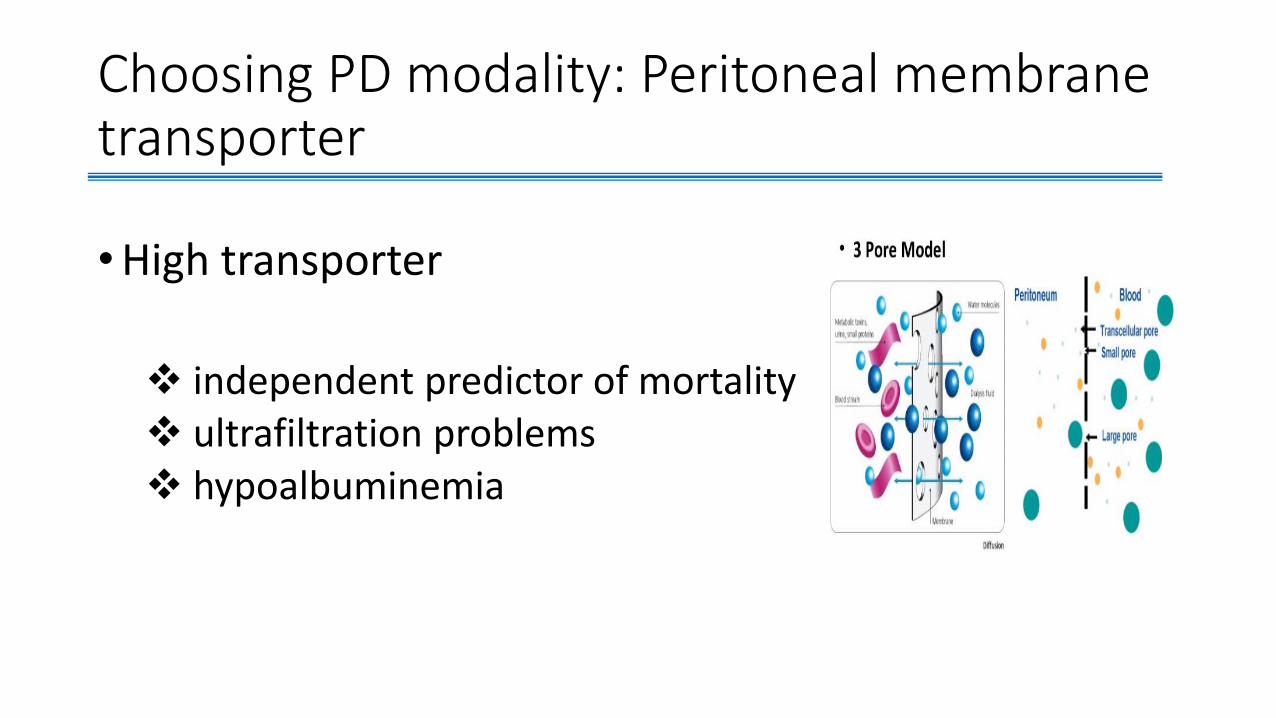
Choosing PD modality: Peritoneal membrane transporter
•High transporter
independent predictor of mortality ultrafiltration problems hypoalbuminemia


CAPD vs APDMortality & Technique failure
• Most studies are observational
• Significant reduction in mortality & technique failure for the past 20 years due to: improvement in connectology in both CAPD & APD
lower peritonitis rate
• 2 potential causal physiologic mechanism that affect mortality:
RRF and serum albumin level

21
The outcomes of continuous ambulatory and The outcomes of continuous ambulatory and
automated peritoneal dialysis are similarautomated peritoneal dialysis are similarMehrotra et al, Kidney Mehrotra et al, Kidney IntInt 2009; 76,972009; 76,97--107107
There were no significant differences
in adjusted mortality rates in patients
treated with CAPD or APD for virtually
all the time periods examined
There were no significant
differences in either time dependent
or overall relative risk for technique
failure between CAPD and APD
patients
21
No significant differences in adjusted mortality rate between CAPD vs APD patients Mehrotra et al, Kidney Int 2009
CAPD vs APDMortality & Technique failure
• 66,300 patients USRDS
• 1994-2004
---- APD__ CAPD


No significant differences in technique survival between CAPD vs APD patients
---- APD__ CAPD
CAPD vs APDMortality & Technique failure


CAPD vs APDSodium removal
• Management of sodium & water balance is crucial especially in anuric patients
• Sodium balance correlates strongly with fluid removal
APD patient tend to have poorer solute removal due to: sodium sieving overnight dwell

CAPD vs APDUltrafiltration
0
200
400
600
800
1000
1200
1400
1600
1800
UF
(m
l/d
ay)
P=NS
N=25
Bro et al Perit Dial Int 19:526-33,1999
CAPD APD
200
400
600
800
1000
0
1200
1400
1600
Ultrafiltration(mls)

• Recumbent position in APD:
increase peritoneal solute transport
associated with reduce ultrafiltration
capacity
hinder proper drainage of dialysate
increase likelihood of incomplete
emptying at the end of every
exchanges
CAPD vs APDUltrafiltration

CAPD vs APDNutrient Loss
•APD tends have more peritoneal protein loss compared to CAPD

CAPD vs APDResidual Renal Function (RRF)
• Each 250 mls of increase urine output associated with reduction in mortality risk by 36%
CANUSA study
• Each increase in RRF of CrCl 10 L/week/1.73 m2 was associated with an 11% decrease in mortality
ADEMEX study

CAPD vs APDResidual Renal Function (RRF)
0
1
2
3
4
5
6
7
0 6 12
Follow-up (months)
Resi
du
al
Cl C
r (m
l/m
in)
CAPD APD
Hufnagel et al Nephrol Dial Transplant 14:1224-8, 1999
* ** p<0.05
n=36

CAPD vs APDResidual Renal Function (RRF)
• Faster decline of RRF in APD compared to CAPD patients 4 longitudinal observational studies
confounded by patient selection bias & underlying renal disease, older
patients with more comorbid treated more with CAPD
• No difference in the rate of decline in RRF between CAPD and APD
No difference in the rate of decline in RRF between CAPD and APDMehrotra R, Perit Dial Int 2009

• CAPD and APD differ significantly in the frequency and method of making the connections and disconnections between the PD catheter & dialysate bags
• Improvements in PD connectology (Y-set, Luer lock technology, flush before fill) is the dominant reason for reduction in risk for peritonitis
CAPD vs APDPeritonitis

CAPD vs APDPeritonitis
• Data seems to suggest APD patients to have lower rates of peritonitis than CAPD
• However, most published studies do not include description of connecting system used by the CAPD & APD patients
** Need to be critical in interpreting the results from studies in different period

No association between PD modality & time to first peritonitis
episode


CAPD vs APDReduce pressure related symptoms
• Hernias• Leaks

CAPD vs APDQuality of Life (QOL)

Scale Scores Parameter
APD
(n=12)
CAPD
(n=13)
P Value
Social Time 3.21.2 1.20.5 0.0005
Physical discomfort 1.91.0 2.21.3 NS
Emotional discomfort 1.81.0 2.21.4 NS
Anorexia 2.81.3 2.90.6 NS
Sleep Problems 2.30.9 1.81.3 NS

Choosing PD modalityLifestyle & Patient Preference

CAPD vs APDPatient Preference
Advantage of CAPD• Cheaper
• Easier to be trained
• Undisturbed from alarms
Advantage of APD• More time available for work,
family and social activities

Conclusion
• The choice of the initial PD modality should be based on patient preference and available resources
• No difference between both modality in terms of: overall mortality and technique failure residual renal function peritonitis for APD compared with CAPD in incident dialysis patients.
• Thus, countries in which prescription of APD is limited because of limited resources do not provide an inferior therapy for their patients WHEN THEY prescribe

Thank You