app ped aw eti
TRANSCRIPT

Pediatrics
Pediatric Airway Management

Page 2
xxx00.#####.ppt 11/21/13 04:42 AMPediatrics Pediatrics
ObjectivesBy the end of this workshop, the learner will:
‐Recite at least 3 indications and 5 complications associated with orotracheal intubation
‐Derive the appropriate ETT size for orotracheal intubation using a formula and/or the patient’s age/weight/size
‐Determine the appropriate sized laryngoscopy blade according to the patient’s age/weight/size
‐Carry out the proper sequence of events involved in orotracheal intubation

Pediatrics
Preparing for Intubation

Page 4
xxx00.#####.ppt 11/21/13 04:42 AMPediatrics Pediatrics
Indications for Intubation
• Primary respiratory disorder
‐ Severe hypoxemia (pneumonia, ARDS)
‐ Severe hypoventilation (bronchiolitis, emphysema, CLD)
• Primary neuromuscular disorder
‐ Myopathy (DMD, SMA)
‐ Altered mental status with hypoventilation (TBI, intoxication)
‐ Lack of airway protection (TBI, severe HIE, intoxication)
‐ Need for sedation with risk of airway protection or ventilation
• Tight control of paCO2 or pH
‐ Severe increased ICP (paCO2)
‐ Severe pulmonary hypertension (pH)
• To reduce metabolic demands in severe shock

Page 5
xxx00.#####.ppt 11/21/13 04:42 AMPediatrics Pediatrics
Use SOAP to Prepare for Intubation
•Suction
‐Rigid catheter with constant suction (Yankauer)
•Oxygen
‐10-15 LPM 100% (make sure it is not on a blender)
•Airway
‐Appropriate sized tubes (estimated size and ½ size smaller)
‐Appropriate sized laryngoscope blades
‐Airway adjuncts
•Pharmacology
‐Based on disease
www.m
ountai nside‐medical. com
/products /Yankauer‐Suc tion‐Tip‐Hand le.htm
l

Page 6
xxx00.#####.ppt 11/21/13 04:42 AMPediatrics Pediatrics
Medications for Intubation
•Premedication for laryngoscopy
•Sedation +/- analgesia
•Neuromuscular blockade‐Make sure you can ventilate prior to neuromuscular blockade
‐Make sure you can ventilate prior to neuromuscular blockade
‐Make sure you can ventilate prior to neuromuscular blockade

Page 7
xxx00.#####.ppt 11/21/13 04:42 AMPediatrics Pediatrics
Premedication
•Atropine (neonates, infants)‐0.02 mg/kg IV (0.1 – 1 mg total dose)
‐Blunts the vagal response from laryngoscopy
‐Use if bradycardic/risk of bradycardia
•Lidocaine (TBI, elevated ICP)‐1 mg/kg IV
‐Anesthetizes airway to blunt the ICP spike from laryngoscopy

Page 8
xxx00.#####.ppt 11/21/13 04:42 AMPediatrics
Sedation•Midazolam (85% of routine patients)
‐ 0.1 – 0.2 mg/kg IV
•Fentanyl (85% of routine patients)
‐ 2 – 6 mcg/kg IV (slow infusion, may cause rigid chest)
‐ Give sedative with fentanyl (no sedative effect)
•Propofol
‐ 1 mg/kg IV (may cause hypotension)
•Ketamine (shock states, asthma)
‐ 1 – 3 mg/kg IV (may cause increased bronchorrhea)
‐ 2 mg/kg IV for RSI
•Thiopental vs. Etomidate (elevated ICP)
‐ Thiopental 3 – 5 mg/kg IV (high risk of hypotension)
‐ Etomidate 0.2 – 0.6 mg/kg IV (may cause adrenal suppression)

Page 9
xxx00.#####.ppt 11/21/13 04:42 AMPediatrics
Neuromuscular Blockade•Rocuronium vs. Vecuronium (85% of patients)
‐ Rocuronium 0.6 – 1.2 mg/kg IV (1.5 – 2 mg/kg IV for RSI)
‐ Vecuronium 0.1 – 0.4 mg/kg IV
‐ Effect may be prolonged in renal/hepatic failure
•Cisatracurium
‐ 0.2 mg/kg IV
‐ Cleared by Hoffman degradation (good for renal/hepatic failure)
•Succinylcholine
‐ 1 – 2 mg/kg IV; 4 mg/kg IM
‐ Patient will fasciculate, consider a defasciculating dose of rocuronium/vecuronium (1/10 dose)
‐ Beware of hyperkalemia in patients with neuromuscular disorders, burns, crush injuries, renal failure

Pediatrics
Orotracheal Intubation

Page 11
xxx00.#####.ppt 11/21/13 04:43 AMPediatrics Pediatrics
Laryngoscope and ETT Selection
•Match the patient! If the patient is smaller than stated age (or unknown age), ETT can be estimated by the patient’s 5 th finger size
Age Blade Size & Type ETT Size (mm; Uncuffed & Cuffed)
NB < 2 kg 0 Miller 2.5
NB > 2 kg ~ 6 mo 1 Miller 3.5 or 3.0 C
6 mo ~ 1 yr 1 ~ 1.5 Miller 4.0 or 3.5 C
1 yr ~ 2 yr 1.5 Miller 4.5 or 4.0 C
2 yr ~ 8 yr 2 Miller For UNcuffed tubes:
8 yr ~ 12 yr 2 Miller or 2 Macintosh
> 12 yr 3 Miller or 3 MacintoshAge(yrs)
4+ 4 Subtract 0.5 mm
for Cuffed tubes

Page 12
xxx00.#####.ppt 11/21/13 04:42 AMPediatrics
Choose Your Blades
Miller Blades Macintosh Blades

Page 13
xxx00.#####.ppt 11/21/13 04:43 AMPediatrics Pediatrics
http://utdol.com/utd/content/topic.do?topicKey=ped_res/2259
Head Tilt-Chin Lift Maneuver

Page 14
xxx00.#####.ppt 11/21/13 04:43 AMPediatrics Pediatrics
Alignment of The Airway:Children <3 years
McAllister J D and K A Gnauck. Pediatr Clin North Am. 1999. 46(6): 1249‐84
O: Oral axisP: Pharyngeal axisL: Laryngeal axis
Large occiput flexes head and neck Shoulder roll will
help line up the pharyngeal and laryngeal axes
Extension of atlantooccipital joint will line up oral axis with the other two

Page 15
xxx00.#####.ppt 11/21/13 04:42 AMPediatrics Pediatrics
Placement of the Laryngoscope Blade (< 3 years)
From: Foltin et al (eds). Teaching Resource for Instructors in Prehospital Pediatrics (TRIPP). 2001
Shoulder Roll for Infants

Page 16
xxx00.#####.ppt 11/21/13 04:42 AMPediatrics Pediatrics
Alignment of The Airway:Children >3 years
McAllister J D and K A Gnauck. Pediatr Clin North Am. 1999. 46(6): 1249-84
O: Oral axisP: Pharyngeal axisL: Laryngeal axis
Cushion under head will flex neck to line up pharyngeal and laryngeal axes
Extension of atlantooccipital joint will line up oral axis with the other two

Page 17
xxx00.#####.ppt 11/21/13 04:42 AMPediatrics Pediatrics
Placement of the Laryngoscope Blade (> 3 years)
From: Foltin et al (eds). Teaching Resource for Instructors in Prehospital Pediatrics (TRIPP). 2001

Page 18
xxx00.#####.ppt 11/21/13 04:42 AMPediatrics Pediatrics
Laryngoscopic View
From: Kakodkar et al. In: Harnick et al. (eds) Pediatric Airway Surgery 2012 (Left); Gray’s Anatomy 1918 (Right)

Page 19
xxx00.#####.ppt 11/21/13 04:42 AMPediatrics Pediatrics
ETT Insertion Depth – How Far?
•3 x ETT size
•Black marking or cuff past vocal cords

Pediatrics
Post-Intubation Care

Page 21
xxx00.#####.ppt 11/21/13 04:43 AMPediatrics
How Do You Confirm Intubation?
•Bilateral & equal breath sounds
- If decreased on one side?
- If absent on one side and hypertympanic
•Improvement of oxygenation
- If saturations rapidly decrease?
•EtCO2 confirmation
- Colorimetric: Yellow = Yes
- Waveform analysis/quantitative: > 15 mm Hg
•CXR confirmation
•Absent sounds over stomach
•Mist in ETT during bag-ventilation

Page 22
xxx00.#####.ppt 11/21/13 04:42 AMPediatrics Pediatrics
•Inability to ventilate (difficulty intubating and cannot BMV)
‐This can lead to death
‐Make sure you can ventilate prior to neuromuscular blockade
•Tube malposition (esophageal intubation)
‐What will you notice/see?
Potential Complications of Oral Intubation

Page 23
xxx00.#####.ppt 11/21/13 04:42 AMPediatrics Pediatrics
•Airway trauma
‐Teeth (check for loose or missing teeth before and after)
‐Vocal cord injury (ineffective paralytic/VC closed during insertion)
‐Subglottic edema/stenosis (incorrect tube size)
•Pulmonary disease
‐Mainstem (left or right) intubation
‐Pneumothorax (usually from over-exuberant bagging)
Potential Complications of Oral Intubation
Page 24
xxx00.#####.ppt 11/21/13 04:42 AMPediatrics Pediatrics
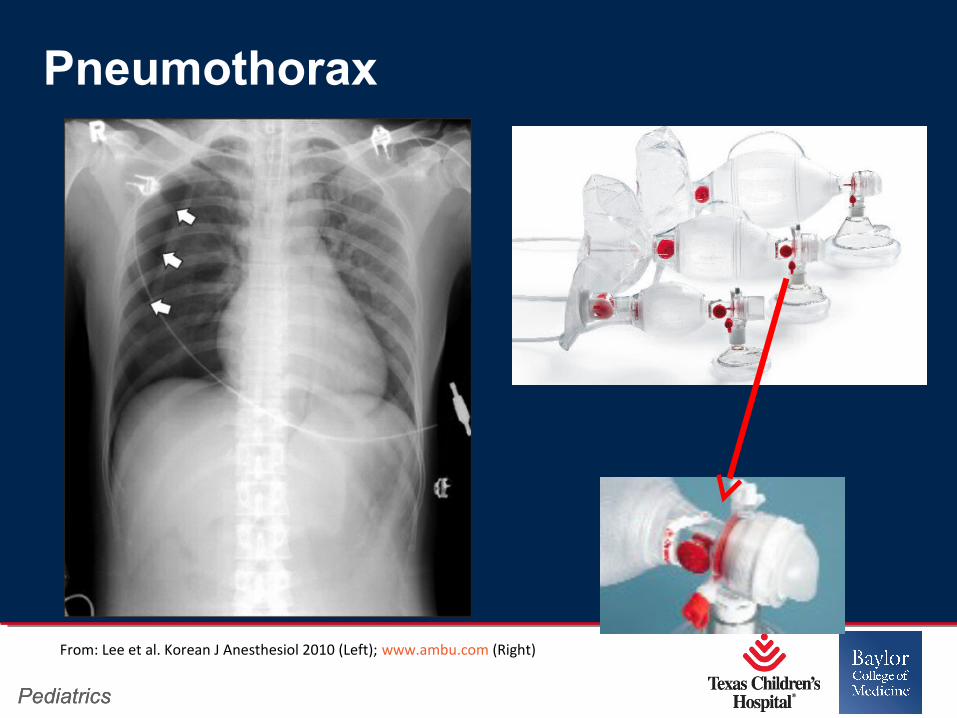
Pneumothorax
From: Lee et al. Korean J Anesthesiol 2010 (Left); www.ambu.com (Right)

Page 25
xxx00.#####.ppt 11/21/13 04:42 AMPediatrics Pediatrics
Dental Trauma (DON’T DO THIS)
From: Windsor and Lockie. Anaesth and Int Care Med. 2008

Pediatrics
NOW WATCH IT DONE