approach to vomiting
TRANSCRIPT

Approach to VomitingDr Nirav Dhinoja

Definition
Nausea: The unpleasant sensation of the imminent need to vomit, usually referred to the throat or epigastrium; a sensation that may or may not ultimately lead to the act of vomiting.
Vomiting: Forceful oral expulsion of gastric contents associated with contraction of the abdominal and chest wall musculature.
Regurgitation: The act by which food is brought back into the mouth without the abdominal and diaphragmatic muscular activity that characterizes vomiting.
Five classes of stimuli provoke nausea and vomiting:
(1) toxic substances within the lumen of the gastrointestinal tract, which initiate release of mediators by enteroendocrine cells (including 5-hydroxytryptamine, substance P, and cholecystokinin [CCK]);
(2) absorbed or parenterally administered toxins, which act directly on the area postrema (also referred to as the chemoreceptor trigger zone—a major lower brainstem center for coordination of drug-induced vomiting);
(3) pathologic processes in viscera (eg, gastrointestinal dilation or inflammation, renal failure);
(4) central nervous system (CNS) stimuli (eg, fear, anticipatory nausea, raised intracranial pressure);
(5) vestibular stimuli (eg, motion sickness) that result in nausea and vomiting by way of the autonomic nervous system.

Neurophysiology
Nausea and vomiting are innate responses that induce a learned and conditioned aversion to ingested toxins
There are four major pathways by which nausea and vomiting are induced.
Vagal afferents
Area postrema
Vestibular system
Amygdala

Vagal Afferents
Abdominal vagal afferents are involved in the emetic response.
Can be evoked by either mechanical or chemo-sensory sensations.
Examples of sensations that trigger this pathway include overdistension, food poisoning, mucosal irritation, cytotoxic drugs, and radiation.
Area Postrema
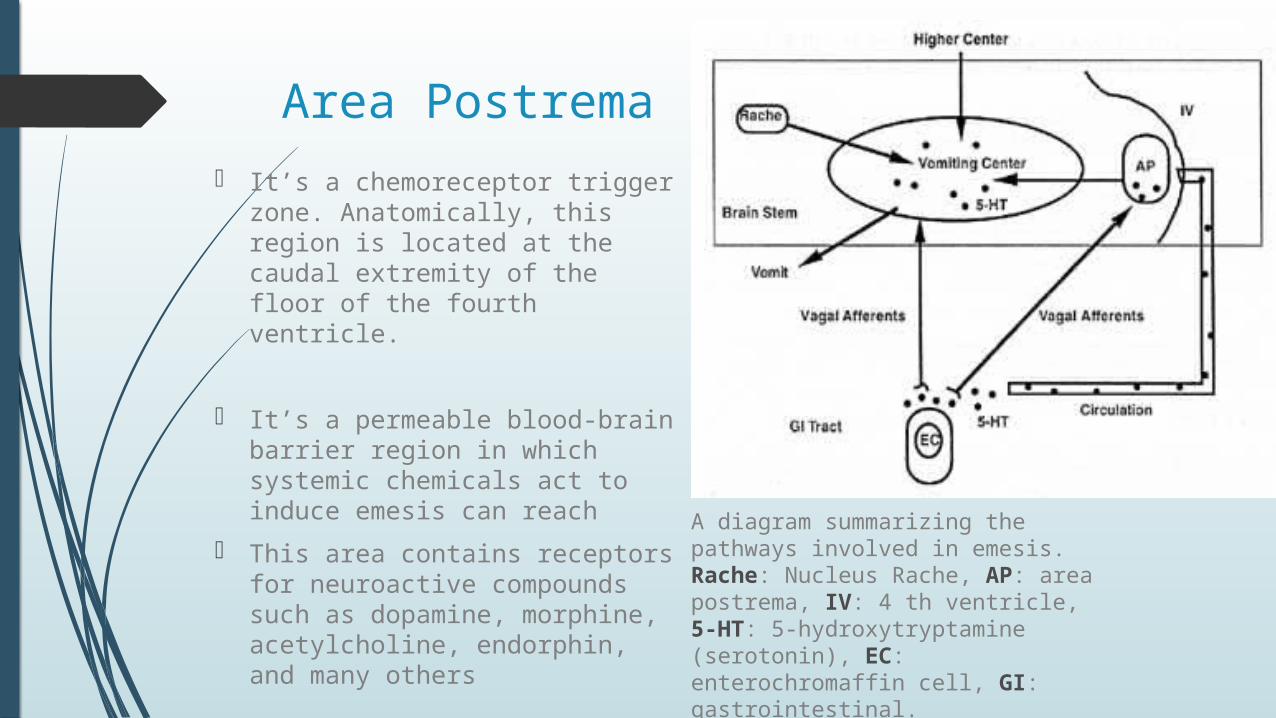
It’s a chemoreceptor trigger zone. Anatomically, this region is located at the caudal extremity of the floor of the fourth ventricle.
It’s a permeable blood-brain barrier region in which systemic chemicals act to induce emesis can reach
This area contains receptors for neuroactive compounds such as dopamine, morphine, acetylcholine, endorphin, and many others
A diagram summarizing the pathways involved in emesis. Rache: Nucleus Rache, AP: area postrema, IV: 4 th ventricle, 5-HT: 5-hydroxytryptamine (serotonin), EC: enterochromaffin cell, GI: gastrointestinal.

Vestibular System
It involved in the emetic response to motion
Exacerbated by visual sensations, Irritation or labyrinthine inflammation.
Somatomotor Events
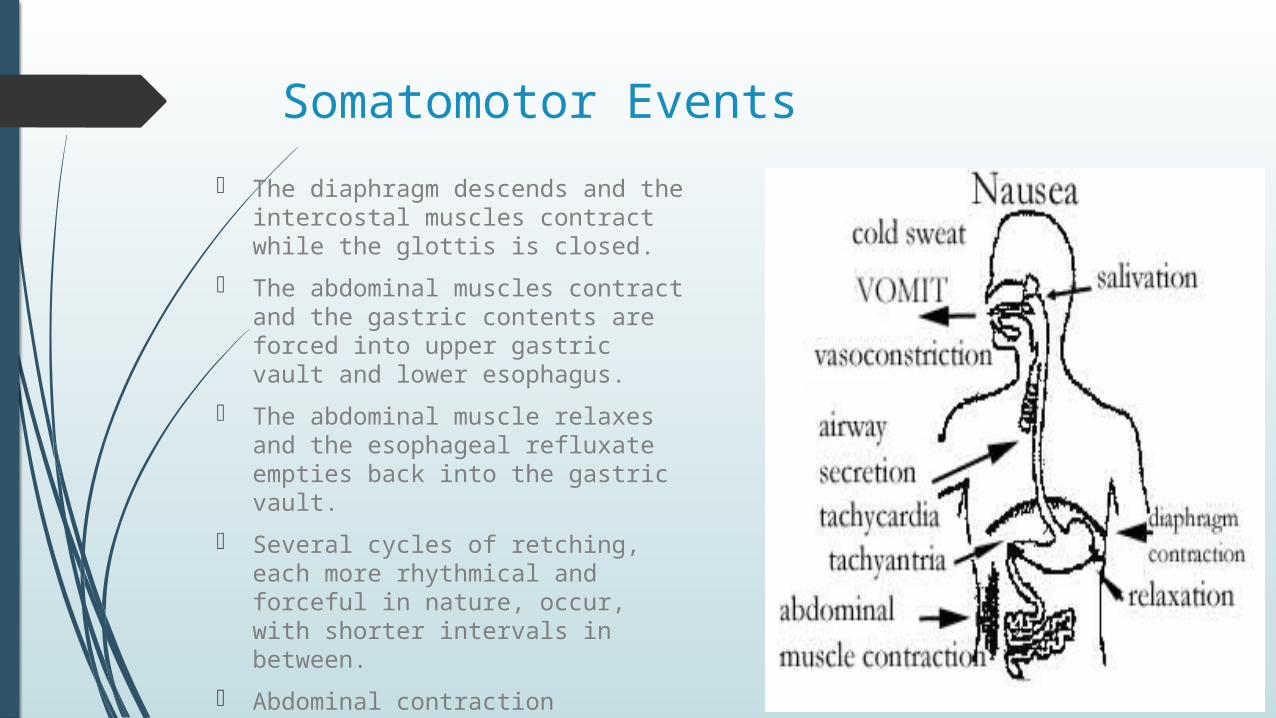
The diaphragm descends and the intercostal muscles contract while the glottis is closed.
The abdominal muscles contract and the gastric contents are forced into upper gastric vault and lower esophagus.
The abdominal muscle relaxes and the esophageal refluxate empties back into the gastric vault.
Several cycles of retching, each more rhythmical and forceful in nature, occur, with shorter intervals in between.
Abdominal contraction associated with elevation of diaphragms results in forceful expulsion of gastric contents.
Infancy/Early childhood - Congenital
• Regurgitation — gastro esophageal reflux
• Atresia— stenosis (tracheoesophageal fistula, antral web, intestinal atresia, annular pancreas)
• Gastrointestinal tract duplication
• Volvulus (secondary to an error in rotation and fixation or to Meckel diverticulum)
• Congenital bands
• Meconium ileus (cystic fibrosis), meconium plug
• Hirsch sprung disease

Infancy/Early childhood - Acquired
• Acute infectious gastroenteritis
• Food allergy, cow milk protein intolerance, eosinophilic gastroenteritis
• Eosinophilic esophagitis
• Pyloric stenosis
• Intussusception
• Celiac disease
• Incarcerated hernia—inguinal, internal secondary to old adhesions
• Postviral gastroparesis
• Adynamic ileus—the mediator for many nongastrointestinal causes of vomiting
• Neonatal necrotizing enterocolitis
• Chronic granulomatous disease with gastric outlet obstruction

Infancy/Early childhood - Nongastrointestinal
• Infectious—otitis, UTI, Pneumonia, URTI, Sepsis, Meningitis
• Metabolic— Aminoaciduria And Organic Aciduria, Galactosemia, Fructosemia, Adrenogenital Syndrome, Renal Tubular Acidosis, Hyperammonemia, Disorders Of Fatty Acid Oxidation(eg, Medium-chain Acyl Coenzyme A Dehydrogenase Deficiency), Mitochondrial Disease
• Central Nervous System — Trauma, Tumor, Infection, Increased Intracranial Pressure, Ventriculo-peritoneal Shunt Failure, Autonomic Responses (Pain, Shock).

Childhood/Adolscenes- Gastrointestinal
• Appendicitis
• Food poisoning (staphylococcal, clostridial)
• Peptic disease—ulcer, gastritis, duodenitis, Helicobacter pylori infection
• Trauma—duodenal hematoma, traumatic pancreatitis, perforated bowel
• Pancreatitis—viral, trauma, drug induced, cystic fibrosis, hyperparathyroidism, hyperlipidemia, hereditary pancreatitis,
• Gallbladder—cholelithiasis, choledochal cyst
• Crohn disease
• Adhesions—congenital or secondary to previous abdominal surgery
• Visceral neuropathy or myopathy.
• Superior mesenteric artery syndrome.

Childhood/Adolscenes- NonGastrointestinal
• Medications— anticholinergics, Alcohol, Idiosyncratic Reaction (Eg, Codeine), Chemotherapy, Radiation Therapy, Overdose(especially Aspirin Or Acetaminophen)
• Central Nervous System—cyclic Vomiting, Migraine, Anorexia Nervosa, Bulimia Nervosa
• Motion Sickness
• Metabolic—diabetic Ketoacidosis, Acute Intermittent Porphyria
• Pregnancy

History
Age of pt.
Duration/Frequency.
Onset
Associated with food intake.
Instantly : esophageal obstruction.
After a while : stomach or duodenal obstruction.
Nature (projectile/non-projectile)
Color & contents
Non digested – proximal obstruction.
Semi digested – distal obstruction.
Billious content – distal to 2nd part of duodenum
Fecal material – large intestinal obstruction.
History
RS : cough, chest discomfort.
Urinary : dysuria, hematuria.
CNS : irritability, altered sensorium, neck stiffness, headache, visual disturbance.
Past history :
Any known medical illness like IEM, cerebral palsy, down syndrome.
Drug & allergy history
Birth history
Nutritional history : recently changed to cow’s milk, food allergy.
Other history : recent travelling/eating outside, family members or friends having similar complaints.

Examination
General condition
Weight comparison before & after onset of illness.
Consciousness – GCS.
Hydration status.
Abdominal examination :
Distension/visible peristalsis.
Tenderness/hepatosplenomegaly.
Palpable mass.
Bowel sounds,

Examination
CNS ex. :
Tone, power, reflexes.
Change in vision.
Respiratory ex.
Otoscopy & fundoscopy.

Investigations
TC, DC – Leukocytosis (infections)
S.electrolytes, urea, s.creatinine – effect of vomiting on electrolytes.
RBS – DKA
ABG – Acidosis – organic acidemias.
Alkalosis- pyloric stenosis.
Urine C/S.
Imaging : CXR, abdominal xray, barium meal, barium follow-through, Cranial CT. Upper endoscopy.
Esophageal ph monitoring.
Metabolic workup in suspected IEM.

Management
Asses the severity of dehydration.
Rehydrate accordingly.
Correct electrolyte imbalances.
Encourage oral intake.
Treat underlying cause.

Treatment should be directed toward the underlying etiology.
Electrolyte abnormalities, metabolic abnormalities, or nutritional deficiencies should be corrected.
Cognitive-behavioral interventions are useful for vomiting associated with functional dyspepsia, adolescent rumination syndrome, and bulimia.
Prokinetic medications such as metoclopramide, domperidone (where available), and erythromycin are beneficial when there are abnormalities in esophago-gastric motility.
Antiemetics, which are useful in persistent vomiting to avoid electrolyte abnormalities or nutritional sequelae, typically have not been recommended in the case of vomiting of unknown etiology. These agents are contraindicated in infants .
Likewise, they are not indicated for anatomic abnormalities or surgical abdomen


Complications
Dehydration and electrolyte imbalance, especially when the vomiting is persistent.
Aspiration pneumonia.
A tear at the gastro-esophageal junction (Mallory-Weiss syndrome)
Rupture of the esophagus (very uncommon in children).
Feeding refusal may follow persistent vomiting.