appropriate response to patients in deterioration
DESCRIPTION
Dr Peter Morley delivered this presentation at IIR’s 10th annual Measuring & Reducing Avoidable Adverse Events conference. For more information about our wide range of medical and health events covering a broad range of industry issues, please visit www.healthcareconferences.com.auTRANSCRIPT

Responding Appropriately to Patients In Deterioration (RAPID)
The Royal Melbourne Hospital experience
A/Prof Peter MorleyFANZCA FRACP FCICM
Director of Medical EducationChair Deteriorating Patient Committee
Royal Melbourne HospitalUniversity of Melbourne




Conflict of interest disclosure
• Commercial/industry– Evidence Evaluation Expert (ILCOR/AHA)
• Potential intellectual conflicts– Deputy Chair Australian Resuscitation Council
(ARC)– Chair ALS Committee ARC– ARC rep on International Liaison Committee on
Resuscitation (ILCOR)– Director of Medical Education (RMH)– Chair Deteriorating Patient Committee (RMH)



Plan of attack• Where were we?
• Make your unknown unknowns known knowns!
• Medical Emergency Team: the answer?– Lessons from Surgery
– Lessons from Medicine
• Deteriorating patient project
• RAPID
• Improved education/training
• The future

Plan of attack• Where were we?
• Make your unknown unknowns known knowns!
• Medical Emergency Team: the answer?– Lessons from Surgery
– Lessons from Medicine
• Deteriorating patient project
• RAPID
• Improved education/training
• The future









Royal Melbourne Hospital
• 160 yr history of healing and teaching
• > 350 beds, plus
– Outpatient Units, Hospital-in-the-Home and
Emergency
• busiest hospital in Australia 2007/8/9
>100,000 inpatients
> 300,000 outpatients



Plan of attack• Where were we?
• Make your unknown unknowns known knowns!
• Medical Emergency Team: the answer?– Lessons from Surgery
– Lessons from Medicine
• Deteriorating patient project
• RAPID
• Improved education/training
• The future

Known knowns . . .
23

Unfortunately . . .
“[T]here are known knowns; there are things we know we know.
We also know there are known unknowns; that is to say we know there are some things we do not know.
But there are also unknown unknowns – the ones we don't know we don't know.”
Former US Secretary of Defense Donald Rumsfeld

Have we only just MET?
The Medical Emergency Team Experience at the City Campus

A “MET” process already existed
We needed to fine tune the response and publicise it better



Existing problems 2004
• Code Blue = CA and MET call
• debate and criticism regarding the appropriateness of the call
• confusion and reluctance to call a CBME
• 82 additional “MET” calls from the ICU CNC’s
• calls being rapidly stood down, without any assessment or intervention
• an inappropriate use of resources
• overcrowding

73
140
32
86
23
5
81
25
0
20
40
60
80
100
120
140
160
Resp Neuro Arrest Misc
Survived
Died
Patient outcome to hospital discharge
“Code Blue” calls 07/01 – 07/03
Arrest survival to discharge 32/113 = 28%
“Non-arrest” survival to discharge 299/352 = 85%


Medical Emergency TeamWorking Party
Progress Report
October 2004

Survival Comparisons of Cardiac
Arrests vs Medical Emergencies
208
7
55
37
0%
20%
40%
60%
80%
100%
Medical Emergencies Cardiac Arrests
Died
Survived
RMH Code Blue Outcome Graphs
Jan to Aug 2004

Trial of implementation of separate MET team 22/11/2004
• 3 months
• Smaller team for Code Blue: MET
• Full team for Code Blue (cardiac arrest)
• Assess number and outcome of various calls
• Assess logistics and quality of process
• Commenced weekly interdisciplinary MET/CA review meeting

Cardiac arrests not a horse ICU
Diagnosis
• broken leg
• bowel obstruction
• severe arthritis
Treatment
• shoot
• shoot
• shoot

Identify reversible causes!

CONSIDER and CORRECT
•Hypoxaemia
Hypovolaemia
Hypo/hyperthermia
Hypo/hyperkalaemia & other metabolic disorders
Tamponade
Tension pneumothorax
Toxins / Poisons / Drugs
Thrombus - pulmonary / coronary

Moitra, VK. Can J Anesth (2012) 59:586–603

Reversible causes of shock and cardiac arrest.
Not just potential causes, BUT conditions that may also develop
during cardiac arrest, . . . that if left uncorrected may
prevent successful resuscitation!





In-hospital extras
• Blood gas
• Electrolytes
• Echocardiogram
• Intra-arterial line, central line
• Good history (observed, documented) including drugs
• (ETCO2)

Can actually consider these!
• Hypoxaemia
• Hypovolaemia
• Hypo/hyperthermia
• Hypo/hyperkalaemia & metabolic disorders
• Blood gas
• Clinical, give fluids
• Measure, consider MH
• Blood gas/electrolytes

And these!
• Tamponade
• Tension pneumothorax
• Toxins/poisons/drugs
• Thrombosis-pulmonary / coronary
• Clinical/echo
• Clinical, can treat
• History known!
• ? Lipids with LA toxicity
• Clinical/thrombolytics

How on earth can I remember that?
W. G. J. Kloeck. A practical approach to
the aetiology of pulseless electrical
activity. A simple 10-step training
mnemonic. Resuscitation 1995;30:157-59.


10 step zig-zag sequence
W. G. J. Kloeck. A practical approach to
the aetiology of pulseless electrical
activity. A simple 10-step training
mnemonic. Resuscitation 1995;30:157-59.

Hypoxia (+ Lazarus)
ABG Test other pulses
IA lineTension
pneumothorax
EchoTamponade
EchoHeart attack
EchoToxins/therapeuti
cs
HistoryHypovolaemi
a Echo Hyper/HypoK, H+
ABGThromboembolism
Echo HypothermiaW. G. J. Kloeck. A practical approach
to the aetiology of pulseless electrical
activity. A simple 10-step training
mnemonic. Resuscitation 1995;30:157-
59.

So we put it on our Code paperwork!

Results of MET trial?

Outcome of MET & Cardiac ArrestsSurvival to hospital discharge: all
• 1 Jan - 21 Nov 2004• 415 Calls in 402 patients
279/342 pts with MET Calls (81.6%)8/60 pts with CAs (13.3%)
• 38.7 Calls/month26.1/32.0 MET pts survive (6D)0.7/5.6 C/A survive (5D)
• 22 Nov 04 - 2 May 06• 991 Calls in 868 patients
647/875 MET Calls (73.9%) 36/116 C/A (31.0%)
• 57.3 calls/month37.4/50.6 MET Calls survive (13D)2.1/6.7 C/A survive (5D)
0
10
20
30
40
50
60
70
80
90
Jan-
Nov 21
2004
Nov 22
04 to 2
May 05
% METsurvival
% CAsurvival
--
--
P = 0.005
P = 0.01
(31.0%)

2004
No code blues called for NFR patients

Outcome of MET & Cardiac ArrestsSurvival to hospital discharge: not NFR
• 1 Jan - 21 Nov 2004• 415 Calls in 402 patients
279/342 pts with MET Calls (81.6%)8/60 pts with CAs (13.3%)
• 38.7 Calls/month26.1/32.0 MET pts survive (6D)0.7/5.6 C/A survive (5D)
• 22 Nov 04 - 2 May 06• 868 Calls in non-NFR patients
611/783 MET patients (78%) 36/85 C/A (42.4%)
• 50.2 calls/month in non-NFR patients35.3/45.3 MET Calls survive (10D)2.1/4.9 C/A survive (3D)
0
10
20
30
40
50
60
70
80
90
Jan-
Nov 21
2004
Nov 22
04 to 2
May 05
% METsurvival
% CAsurvival
--
--
P = 0.18
P = 0.002

Outcome of MET & Cardiac ArrestsSurvival to hospital discharge: 2B
• 1 Jan - 21 Nov 2004• Calls in 17 cardiac patients
5/7 pts with MET Calls (71.5%)2/10 pts with CAs (20%)
• 1.6 Calls/month in cardiac patients0.5/0.7 MET pts survive (0D)0.2/0.9 C/A survive (1D)
• 22 Nov 04 - 2 May 06• Calls in 58 non-NFR cardiac patients
41/45 MET patients (91.1%) 17/33 C/A (51.5%)
• 3.4 calls/mth in non-NFR card. patients2.4/2.6 MET Calls survive (0D)1.0/1.9 C/A survive (1D)
0
10
20
30
40
50
60
70
80
90
100
Jan-
Nov 21
2004
Nov 22
04 to 2
May 05
% METsurvival
% CAsurvival
--
--
P = 0.18
P = 0.15
(51.5%%)

Outcome of MET & Cardiac ArrestsSurvival to hospital discharge: ward
• 1 Jan - 21 Nov 2004• Calls in 337 ward patients
239/299 pts with MET Calls (79.9%)6/38 pts with CAs (15.8%)
• 31.5 Calls/month in ward patients22.3/27.9 MET pts survive (6D)0.6/3.6 C/A survive (3D)
• 22 Nov 04 - 2 May 06• Calls in 776 non-NFR ward patients
573/724 MET patients (79.1%) 19/52 C/A (36.5%)
• 44.9 calls/mth in non-NFR ward patients33.1/41.9 MET Calls survive (10D)1.1/3.0 C/A survive (2D)
0
10
20
30
40
50
60
70
80
Jan-
Nov 21
2004
Nov 22
04 to 2
May 05
% METsurvival
% CAsurvival
--
--
P = 0.79
P = 0.03
36.5%

Summary outcomes 18/12 after MET
• More likely to die if arrest at night (reviewing staffing)
• More deaths on medical wards (reviewing)• Longer stay patients = Higher risk patients• Duration 30 min (up to 2 hrs)• > 70% arrests not shockable• 67% ROSC (all), 44% Discharge (all)
MET calls identify patients at high risk– 20% in-hospital mortality (2 X ICU!)

Plan of attack• Where were we?
• Make your unknown unknowns known knowns!
• Medical Emergency Team: the answer?– Lessons from Surgery
– Lessons from Medicine
• Deteriorating patient project
• RAPID
• Improved education/training
• The future

Seven alternatives to evidence based medicine
David Isaacs, Dominic Fitzgerald BMJ 1999;319:1618

BMJ 2003;327:1459-61


M.E.R.I.T Study
Medical
Early
Response
Intervention
Therapy

Us vs them (mean!)
• Cardiac arrests/1000 admissions– MERIT control 1.64
– MERIT MET 1.31 (Range 0.45-2.34)
– RMH 0.71
• Unplanned ICU admit/1000 admissions– MERIT control 4.68
– MERIT MET 4.18 (Range 0.30-10.87)
– RMH 2.5
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
Arrests UnexpICU
No MET
MET
RMH



City Campus Code Blue Medical Emergency Calls 2005 to
2011
709 699 825 918 974 1131 1513
0
200
400
600
800
1000
1200
1400
1600
Total Calls
2005 2006 2007 2008 2009 2010 2011

2005 - 2011 data
70
709 699
825
918
974
1131
1512
622 618
757
825
892
1056
1440
87 80 70 91 82 75 72
0
200
400
600
800
1000
1200
1400
1600
2005 2006 2007 2008 2009 2010 2011
Total Calls
MET
CA

Ward MET vs Cardiac Arrest
2005 to 2011
Ward patients =
excludes CCU,
Cath. Lab, non
patients and NFR
patients.
491 476 528599641
738 1051
34 43 29 50 40 45 29
0
200
400
600
800
1000
1200
MET CA
2005 2006 2007 2008 2009 2010 2011

Ward MET Survival to Hospital Discharge
2005 to 2010
382 384 457 500 533 604
9170 99 106 134109
0%10%20%30%40%50%60%70%80%90%
100%
2005
Ward
MET
2006
Ward
MET
2007
Ward
MET
2008
Ward
MET
2009
Ward
MET
2010
Ward
MET
Survived Died
Ward patients =
excludes CCU,
Cath. Lab, non
patients and NFR
patients.

Not alwaysstraight forward

Plan of attack• Where were we?
• Make your unknown unknowns known knowns!
• Medical Emergency Team: the answer?– Lessons from Surgery
– Lessons from Medicine
• Deteriorating patient project
• RAPID
• Team training
• The future

Antecedents to MET Calls in Surgical Patients
Adithya BalasubramanianMedical StudentUnivesity Of Melbourne

Methodology
• Retrospective review using patients’ histories and the RMH MET Database.
• January- March 2009
• Inclusion Criteria– Surgical patients who had their first MET call during
study period
• Exclusion Criteria– Patients who were in ICU at any time during the 24
hours preceding the MET call
• HREC approval as a Quality Assurance project

Results
• 49 surgical patients were subject to 65 MET calls
• Overall mortality was 24.5%

Systemic Factors (Significant)
• The odds of death were significantly higher in:
– Patients older than 80 years (OR: 6.40, p=0.01)
– NFR patients (OR: 55.00, p<0.0001)
– Patients admitted from Emergency Department (OR: 9.55, p=0.04)
– Neurosurgical patients (OR: 5.9, p=0.02)
– ASA Score 3-5 (OR: 18.36, p=0.01)

Pre-defined Scoring Systems: SOCCER Criteria Prevalence
• SOCCER: Signs of critical conditions and emergency responses, Jacques, T., et al. Resuscitation,2006 (Liverpool, NSW)
• In the 24 hrs preceding MET call the following signs were detected:– “SpO2 90-95%” (59.2%)
– “Alteration in Mentation” (38.8%)
– “Systolic BP 90-100 mmHg” (32.7%)
– “New Pain” (24.5%)

Pre-defined Scoring Systems: SOCCER Criteria Predictive Value
• Presence of certain physiological markers was associative of a statistically significant increase in death
– “Alteration in Mentation” (OR 15.56, 0.0005)
– New recording of “GCS 9-11 or alteration in GCS>2” (OR 8.75, 0.03)
– “Pulse Rate 40-49 or 131-140/min” (OR 5.89, p=0.03)

MET Breaches
“Met MET but no MET”
• Eighteen of the 49 patients (37%) had MET breach < 8hrs before MET
- 28% (5 of these 18) died
• Twenty (41%) had MET breach <24 hours before MET
- 35% (7 of these 20) died


Summary
• Mortality after MET call was higher in:– Neurosurgical patients
– Patients transferred onto general wards from the Emergency Department
– Patients who had displayed a number of “Early Signs” illustrating physiological instability
– Patients with an ASA Score of 3-5
– (NFR patients)
• Of concern, 41% of patients had a MET Breach

Conclusion
• Earlier calling and intervention may further decrease the mortality and morbidity of these patients.
• The use of the following red flags may facilitate earlier treatment and improve outcomes:– “Alteration in Mentation”
– “Pulse Rate 40-49 or 131-140/min”
– Age>80
– Admission from ED
– Neurosurgical patients
• Further research with increased patient numbers is needed.

What about “medical” patients?
Rachel Morgan, Zhongxiong Cai, Wei Chen, Emma Crawford, Anna Creelman,
Jennifer Burke, Peter Morley, Nick Santamaria

Medical MET review• 171 MET calls (Jan –May 2010)
• recorded clinical antecedents to these calls
• 26% breached MET call criteria in the 24 hours prior to the call
– HR>130 bpm (most frequent)
– oxygen saturation <90%,
– SBP<90 mm Hg,
– RR > 30 breaths per minute
– acute change in consciousness
– combinations of two MET call criteria.
• Junior staff appear more reluctant to call/not recognise as sick
• Follow up: none died during MET call, but 25% of these patients were known to be deceased Dec 2010.

Plan of attack• Where were we?
• Make your unknown unknowns known knowns!
• Medical Emergency Team: the answer?– Lessons from Surgery
– Lessons from Medicine
• Deteriorating patient project
• RAPID
• Team training
• The future


What about pre-MET!!!



Association between clinically abnormal observations & subsequent in-hospital mortality: a prospective study
Michael Buist, Stephen Bernard et al. Resuscitation 62 (2004) 137–141
• This study was a prospective, observational investigation at Dandenong Hospital, Melbourne, Victoria, Australia (320-bed, university affiliated teaching hospital).
• During the 7-month study period, 6303 patients were admitted to the study wards, with a total of 38,115 bed-days and a mean length of stay of 6 days. During this period, 1598 abnormal bedside observations were observed in 564 patients; making the incidence of abnormal bed observations 4.2 per 100 bed-days in 8.9% patients.

Michael Buist, Stephen Bernard et al. Resuscitation 62 (2004) 137–141

Resuscitation 2006


• The ‘top five’ ES and the odds (OR) for death were:
– base deficit −5to−8 mmol/L = 40.2 (95% C.I. 7.7—208.8)
– partial airway obstruction OR = 38.7 (3.9—64.4)
– poor peripheral circulation OR = 34.4 (6.8—174.0)
– >expected drain fluid loss OR = 30.1 (6.1—148.9)
– pH <7.3 >7.2 OR = 29.0 (3.1—268.3).




Respiratory rate• Respiratory rate higher than 27 breaths/minute was the most important
predictor of cardiac arrest in hospital wards.– Fieselmann JF, Hendryx MS, Helms CM, et al. Respiratory rate predicts cardiopulmonary arrest for
internal medicine patients. J Gen Intern Med 1993; 8: 354-360.
• 21% of ward patients with a respiratory rate of 25– 29 breaths/minute
assessed by a critical care outreach service died in hospital. Those with a
higher respiratory rate had an even higher mortality rate.– Goldhill DR, McNarry AF, Mandersloot G, et al. A physiologically-based early warning score for
ward patients: the association between score and outcome. Anaesthesia 2005; 60: 547-553.
• Just over half of all patients suffering a serious adverse event on the general
wards (such as a cardiac arrest or ICU admission) had a respiratory rate
greater than 24 breaths/minute. These patients could have been identified as
high risk up to 24 hours before the event with a specificity of over 95%.
– Cretikos M, Chen J, Hillman K, et al. The Objective Medical Emergency Team Activation
Criteria: a case–control study. Resuscitation 2007; 73: 62-72.

MET criteria
101

We can't solve problems by using the same kind of thinking we used when we created them.
Albert Einstein
14 March 1879 – 18 April 1955

Reducing Harm from Deterioration
Presenter: Peter Morley
Hospital: VulcanKey contact person: Dr Owen Bradfield.
(03) 9342 8937
Lisa McKenzie, Kylie Barnard, Caroline Cooper-Blair, Jenny Bell, Jenny Lumsden

104
AIM OF THIS PROJECT• What improvement was sought?
– Clear, consistent documentation of reportable limits
– Observations performed and documented as planned
– Improved communication/escalation process for deteriorating patients (pre-MET): EMPOWERMENT
– No preventable mortality and morbidity
• What areas?
– 1 Surgical ward, 28 acute surgical beds (130 admissions/month)
• By When?
– Implementation by 18/8/09. Final audit and evaluation 07/10/09.
• With what resources?
– Human – pre-existing staff Quality and Safety staff and Project Team
– Financial - $ 1,100 for printing of observation chart and ISBAR phone pads.
– Clinical Skills Centre – pre-existing low level simulation mannequin.

105
Stage 1: KEY CHANGES IMPLEMENTED • New observation chart
– coloured reportable parameters
– 24 hours fluid balance summary
– frequency of observations
– acceptable limits for reportable observations
– analgesic observations
– MET and Code Blue calling criteria
– escalation for medical review
• Introduction of ISBAR
– communication tool (with phone pad)
– R = requirement
• Empowerment
Adapted from chart developed by Western Health

Observation chart
106

Observation chart
107

108

109
ISBAR
• I – Identify
• S – Situation
• B – Background
• A – Assessment
• R – Request (Requirement)

• Small group education sessions (85% staff)
– regarding the project
– introduction of the new observation chart
– education regarding escalation process and ISBAR
• Small group simulation sessions (76% staff)
– deteriorating patient scenarios (pre MET criteria)
– ABCDE patient assessment approach
– ISBAR
– principles of Crisis Resource Management (now in all one day ALS courses)
111
KEY CHANGES IMPLEMENTED

112
Initial Responses
I feel confident to use ISBAR when treating a
deteriorating patient
1 2
21
9
00 0 0
13
20
0
5
10
15
20
25
Strongly
Disagree
Disagree Unsure Agree Strongly
Agree
Before
After
P<0.001
I feel comfortable with initiating treatment of the
deteriorating patient
0 0
9
19
4
0 0 1
16 16
0
5
10
15
20
Strongly
Disagree
Disagree Unsure Agree Strongly
Agree
Before
After
P<0.001
I feel comfortable with my ability to assess a
deteriorating patient
0 13
24
5
0 0 1
16 16
0
5
10
15
20
25
30
Strongly
Disagree
Disagree Unsure Agree Strongly
Agree
Before
After
P<0.001
• increased empowerment for nursing staff
– “ISBAR is an excellent communication tool”
• simulation training
– “Improved my assessment skills”
– “Improved my confidence when communicating with
Doctors”
– “Assertiveness when communicating with team”
– “Empowerment for staff”
113
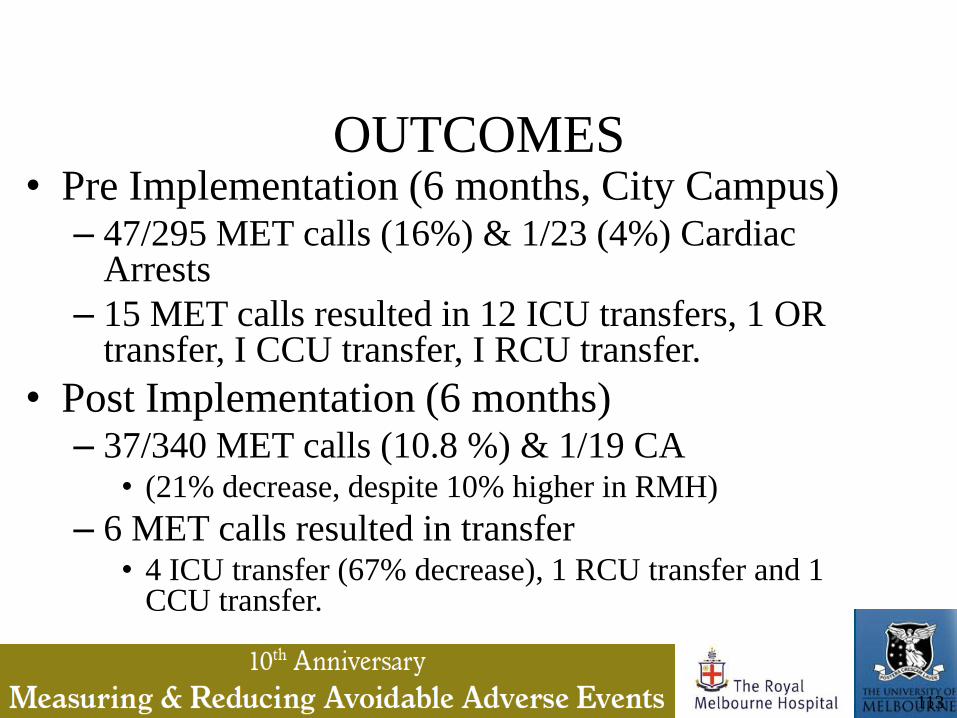
OUTCOMES• Pre Implementation (6 months, City Campus)
– 47/295 MET calls (16%) & 1/23 (4%) Cardiac Arrests
– 15 MET calls resulted in 12 ICU transfers, 1 OR transfer, I CCU transfer, I RCU transfer.
• Post Implementation (6 months)– 37/340 MET calls (10.8 %) & 1/19 CA
• (21% decrease, despite 10% higher in RMH)
– 6 MET calls resulted in transfer • 4 ICU transfer (67% decrease), 1 RCU transfer and 1
CCU transfer.

Progress since 3 South
• Roll out to 5th floor and 2 west
– Tailored program
• Over 50 medical and nursing instructors
trained
• Rebadged as RAPID
• Hospital wide roll out
114

Aims of RAPID
• “The aim of the RAPID Program is to improve
the documentation, communication and
escalation of patient care. Based on early
assessment and intervention we aim to
maximise opportunities to intervene during the
early phases of deterioration.”
115

Hierarchy of supports (all hours)
• Bedside nurse
• Team leader
• Nurse in charge
• Clinical nurse consultant ICU
• Intern/HMO
• Registrar surg/med/anaesth/ICU
• MET
• Code blue
116

117

Objectives of RAPID education
• Explain the aim of RAPID at Melbourne Health.
• Describe what is meant by the term “ABCDE” in relation to patient assessment.
• Assess the deteriorating patient, utilising the sequence of tasks “ABCDE”.
• Initiate treatment of the deteriorating patient.
• Call for help in the event of an emergency.
• Describe the ISBAR communication tool.
• Utilise the “ISBAR” tool when treating a deteriorating patient.
• Demonstrate the ability to deliver and integrate the ABCDE approach, ISBAR and Crisis Resource Management (CRM) in a low fidelity environment.
118
In order to form an immaculate member of a flock of sheep one
must, above all, be a sheep.Albert Einstein
14 March 1879 – 18 April 1955

Education in wards
• ABCDE
• Crisis Resource Management
• ISBAR
• paging
120

A…
B…
C…
D…
E…
airway
breathing
circulation
disability
exposure
The ABCDE approach to the critically ill patient
Recognition and treatment as problems detected

The ABCDE approach
• Personal safety (Danger)
• Patient responsiveness (Response)
• Send for help
• Vital signs
– respiratory rate, SpO2, pulse, BP, ECG, temperature
• Capable not just competent

Principles of Crisis Resource Management
How to work as a team in an emergency!

Three of the most important principles for successful team function in a crisis:
• Avoiding fixation errors
• Shared situational awareness
• Communication

“Mitigated speech”
• refers to any attempt to downplay or sugarcoat the meaning of what is being said. We mitigate when we're being polite, or when we're ashamed or embarrassed, or when we're being deferential to authority.
• Fischer and Orasanu found that captains overwhelmingly said they would issue a command in that situation: "Turn thirty degrees right." They were talking to a subordinate. They had no fear of being blunt. The first officers, on the other hand, were talking to their boss, and so they overwhelmingly chose the most mitigated alternative. They hinted.

Graded assertiveness• Opening
• Dr Williams
• State your concern
• I am worried that this man is hypoventilating and may need to be re-intubated
• State the problem
• He is sweaty and has a bounding pulse, but his neurological state is getting worse.
• Offer a solution(s)
• If you can assist his ventilation, I will get an arterial blood gas to check his CO2.
• State consequences
• If he is hypoventilating then he may actually go on to arrest unless we detect it and correct it.
• Obtain feedback
• Is that a reasonable plan of action?

127

Solution: Tools for Communication
• ISBAR
– I = Identify WHO?
– S = Situation WHERE?
– B = Background
– A = Assessment and Actions
– R = Request or Requirement WHAT? WHEN?
• Not complex at all. Abridged summary.

Other applications of ISBAR
• Writing a written referral
• Presenting a case on a ward round
• Handing over a complicated patient to cover staff
• Implemented in paging system



DOES
SHOWS HOW
KNOWS HOW
KNOWS
Performance integrated into practice:
Chart audit, direct observation
Demonstration of learning:
Clinical performance exams,
high fidelity simulations
Interpretation / Application:
Case presentations, essay
exams
Fact-gathering: Multiple
choice exams
Adapted from Miller GE. The assessment of clinical
skills/competence/performance. Acad Med. 1990; 65
(9);563-567
Capable

There are three kinds of men. The one that learns by reading. The few who
learn by observation. The rest of them have to pee on the electric fence for
themselves.
Will Rogers



Stage 2: Train-the-trainer education model 2010
• RAPID Instructors course to support and train medical and nursing clinical educators to facilitate a 90 minute Deteriorating Patient Simulation Session for medical and nursing staff
• The RAPID Instructors course duration was 3 hours and included– optimising educational experiences, – Crisis Resource Management (CRM) principles, – systematic assessment approaches (ABCDE), working
as a team and communication (ISBAR), and– how to facilitate low fidelity simulation training

RAPID - Responding Appropriately to Patients in Deterioration
Instructors Course
Pre & Post Evaluation
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
5.0
I understand the
background and
purpose of the
Deteriorating Patient
Project at
Melbourne Health
I am able to optimise
educational
experiences
I understand w hat
is meant by
“ABCDE” in terms of
patient assessment
I understand the
sequence of tasks
in assessment of
the deteriorating
patient (ABCDE)
I understand w hat
is meant by the term
“ISBAR”
I understand the
three main
components of
Crisis Resource
Management
I am able to deliver
and integrate the
ABCDE approach,
ISBAR and CRM in a
low fidelity
environment
Questions asked
Le
ve
l o
f u
nd
ers
tan
din
g/c
om
fort
1=str
on
gly
dis
ag
ree -
5 =
str
on
gly
ag
ree
Pre
Post
RAPID - Responding Appropriately to Patients in Deterioration
Instructors Course
Pre & Post Evaluation
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
5.0
I understand the
background and
purpose of the
Deteriorating Patient
Project at
Melbourne Health
I am able to optimise
educational
experiences
I understand w hat
is meant by
“ABCDE” in terms of
patient assessment
I understand the
sequence of tasks
in assessment of
the deteriorating
patient (ABCDE)
I understand w hat
is meant by the term
“ISBAR”
I understand the
three main
components of
Crisis Resource
Management
I am able to deliver
and integrate the
ABCDE approach,
ISBAR and CRM in a
low fidelity
environment
Questions asked
Le
ve
l o
f u
nd
ers
tan
din
g/c
om
fort
1=str
on
gly
dis
ag
ree -
5 =
str
on
gly
ag
ree
Pre
Post

Stage 3:
RAPID implemented at RMH May 2011• Change observation charts
• Nursing staff educated (90 minute sessions)
• Medical staff: broad education (Interns simulated cases: 2 X 0.5 days)
• Hospital wide support
• Reinforcement sessions Tuesday 1300-1400
• Evaluation in progress
• Medical staff to document reportable limits
138

Please document reportable limits!

MET criteria
140




Stage 4 Default reporting values
• Escalation of care to medical staff required if – Heart rate greater than 120 beats per minute.
– Respiratory rate greater than 24 per minute.
– Systolic Blood pressure less than 100 mmHg.
– Temperature ≥ 38C
• All patients at the RMH City Campus are to have a minimum of 6 hourly observations. These observations include heart rate, blood pressure, respiratory rate and temperature.

Where are we now?

RAPID
• Well embedded
• Standardised escalation criteria across hospital
• Deteriorating patient sessions
– Weekly in clinical skills centre
• About to start team training for mock codes


City Campus Code Blue Medical Emergency Calls
Sept 2011/2012
10941003
1036 960
58 43
0
200
400
600
800
1000
1200
Total Calls MET CA
Jan to Sept 11 Jan to Sept 12

Ward patients =
excludes CCU,
Cath. Lab, non
patients and NFR
patients.
763
713
23 17
0
100
200
300
400
500
600
700
800
MET CA
Jan to Sept 11 Jan to Sept 12
Ward Cardiac Arrest vs MET Calls
Sept 2011/2012

Comparison of 2011/12
MET calls- prior NFR and NFR at Call
763 713
110 94
3235
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Jan to Sept 11 Jan to Sept 12
Ward MET Prior NFR NFR at call

Ward MET Survival to Hospital Discharge
Sept 2011/12
644 621
92119
0%
10%20%
30%
40%50%
60%
70%
80%90%
100%
Jan to Sept 11 Ward MET Jan to Sept 12 Ward MET
Survived Died
Ward patients =
excludes CCU,
Cath. Lab, non
patients and
NFR patients.
2012 Ward MET survival to hospital discharge = 86%

Ward Cardiac Arrest
Survival to Hospital Discharge Sept 2011/12
7
3
9
8
76
0%10%
20%30%
40%50%60%
70%80%
90%100%
Jan to Sept 2011 Ward CA Jan to Sept 2012 Ward CA
Survived DDE DDA
Ward patients =
excludes CCU,
Cath. Lab, non
patients and
NFR patients.
2012 Ward CA survival to hospital discharge = 41%

Comparison of CA and NFR
Sept 2011/12
23 17
15 13
9 5
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Jan to Sept 11 CA Jan to Sept 12 CA
Total Ward CA Prior NFR NFR at call

Plan of attack• Where were we?
• Make your unknown unknowns known knowns!
• Medical Emergency Team: the answer?– Lessons from Surgery
– Lessons from Medicine
• Deteriorating patient project
• RAPID
• Improved education/training
• The future

ILCOR Treatment recommendation• In adult patients admitted to hospital, there is insufficient evidence to
support or refute the use of early warning/RRT/MET systems, compared with no such systems, to reduce cardiac and respiratory arrests and hospital mortality.
• However, it is reasonable for hospitals to provide a system of care that includes
– (a) staff education about the signs of patient deterioration;
– (b) appropriate and regular vital signs monitoring of patients;
– (c) clear guidance (e.g., via calling criteria or early warning scores) to assist staff in the early detection of patient deterioration;
– (d) a clear, uniform system of calling for assistance; and
– (e) a clinical response to calls for assistance.
• There is insufficient evidence to identify the best methods for the delivery of these components and, based on current evidence, this should be based on local circumstances.



ILCOR Treatment recommendation• Hospitals should use a system validated for their
specific patient population to identify individuals at increased risk of serious clinical deterioration, cardiac arrest, or death, both on admission and during hospital stay.

You need approximately 10,000 hours of deliberate practice with
feedback to become an expert in a field
(at least 40*50*5)

Education: “new” approaches• Brindley PG, Simmonds MR, Needham CJ, Simmonds KA. Teaching airway management to novices: a
simulator manikin study comparing the 'sniffing position' and 'win with the chin' analogies. Br J Anaesth. 2010 February 18, 2010:aeq020.
• Bollig G, Myklebust A, Ostringen K. Effects of first aid training in the kindergarten - a pilot study. Scandin J Trauma Resusc Emerg Med. 2011;19(1):13.
• Sutton RM, Niles D, Meaney PA, Aplenc R, French B, Abella BS, et al. Low-Dose, High-Frequency CPR Training Improves Skill Retention of In-Hospital Pediatric Providers. Pediatrics. 2011 June 6, 2011(Online first):June 6.
• Oermann MH, Kardong-Edgren SE, Odom-Maryon T. Effects of monthly practice on nursing students' CPR psychomotor skill performance. Resuscitation. 2011;82(4):447-53.
• Beckers SK, Biermann H, Sopka S, Skorning M, Brokmann JC, Heussen N, et al. Influence of pre-course assessment using an emotionally activating stimulus with feedback: A pilot study in teaching Basic Life Support. Resuscitation. 2012;83(2):219-26.
• Bobrow BJ, Vadeboncoeur TF, Spaite DW, Potts J, Denninghoff K, Chikani V, et al. The Effectiveness of Ultrabrief and Brief Educational Videos for Training Lay Responders in Hands-Only Cardiopulmonary Resuscitation. Circ Cardiovasc Qual Outcom. 2011(Online first March 8).
• Oulego-Erroz I. A popular song improves CPR compression rate and skill retention by schoolchildren: A manikin trial. Resuscitation. 2011;82(4):499-500.
161

Education: team training• Andersen P, Jensen M, Lippert A, Astergaard D. Identifying non-technical skills and barriers for
improvement of teamwork in cardiac arrest teams. Resuscitation 2010;81(6):695-702.
• Andersen PO, Jensen MK, Lippert A, Østergaard D, Klausen TW. Development of a formative assessment tool for measurement of performance in multi-professional resuscitation teams. Resuscitation. 2010;In Press, Corrected Proof.
• Cooper S, Cant R, Porter J, Sellick K, Somers G, Kinsman L, et al. Rating medical emergency teamwork performance: Development of the Team Emergency Assessment Measure (TEAM). Resuscitation. 2010;81(4):446-52.
• Siassakos D, Fox R, Crofts J, Hunt L, Winter C, Draycott T. The management of a simulated emergency: Better teamwork, better performance. Resuscitation 2011;82(2):203-6.
• Cheng J, Yan Z, Zhiqiao C, Sheng C, Xiaobo Y. Improving cardiopulmonary resuscitation in the emergency department by real-time video recording and regular feedback learning. Resuscitation. 2010;81(12):1664-9.
• Walker S, Brett S, McKay A, Lambden S, Vincent C, Sevdalis N. Observational Skill-based Clinical Assessment tool for Resuscitation (OSCAR): Development and validation. Resuscitation. 2011;82(7):835-44.
• Hunziker S, Johansson AC, Tschan F, Semmer NK, Rock L, Howell MD, et al. Teamwork and Leadership in Cardiopulmonary Resuscitation. J Am Coll Cardiol. 2011 June 14, 2011;57(24):2381-8.
• Hunziker S, Buhlmann C, Tschan F, Balestra G, Legeret C, Schumacher C, et al. Brief leadership instructions improve cardiopulmonary resuscitation in a high-fidelity simulation: a randomized controlled trial. Critical Care Medicine. [Randomized Controlled Trial]. 2010 Apr;38(4):1086-91.
162




Smart teaching
166

167
Compression depth
Ventilation volume

Plan of attack• Where were we?
• Make your unknown unknowns known knowns!
• Medical Emergency Team: the answer?– Lessons from Surgery
– Lessons from Medicine
• Deteriorating patient project
• RAPID
• Improved education/training
• The future






Plan of attack• Where were we?
• Make your unknown unknowns known knowns!
• Medical Emergency Team: the answer?– Lessons from Surgery
– Lessons from Medicine
• Deteriorating patient project
• RAPID
• Improved education/training
• The future


176


Unexpected problems?


Acknowledgements
• Deteriorating patient committee
• RAPID instructors
• Instructors deteriorating patient sessions
• Jennifer Burke (legend!)