aqueous humour dynamics
TRANSCRIPT

AQUEOUS HUMOR DYNAMICS
SIVATEJA CHALLASSSIHMS

INTRODUCTION• Is a clear, colourless, watery solution• Flows from posterior to anterior
chamber• In healthy eye flow against
resistance generates 15 mm hg

• Aqueous formation (F), facility of outflow (C), and episcleral venous pressure (P0) are the major intraocular determinants of IOP. These factors are related to one another by the Goldmann equation:
F = C (Po - Pv) P0 is IOP in undisturbed eye
With the discovery of pressure independent mech the equation is modified F = C (Po - Pv)+UU is the sum of pr independent pathways


FUNCTIONS• Nutrition to lens cornea and iris• Removes metabolically toxic
products• Refractive index 1.33• Inflates globe and maintains IOP• Ascorbate-anti oxidant-uv protection• Facilitates cellular and humoral
response of eye to inflammation And infection

DYNAMICS ICNCLUDE
• Anatomy of aqueous formation and
drainage structures• Aqueous humor formation• Aqueous humor outflow

ANATOMY• Primary ocular structures involved
are1.Ciliary body2.Posterior chamber3.Anterior chamber4.Angle of anterior chamber5.Aqueous outflow system

1.CILIARY BODY

• CILIARY PROCESS-70-80-2 mm length and 5mm width• Network of
capillaries• Stroma• Inner pigmented
epithelium• Outer non
pigmented epithelium


2.POSTERIOR CHAMBER 0.06ml

3.ANTERIOR CHAMBER-0.25ml

4.ANGLE OF ANTERIOR CHAMBER

AQUEOUS FORMATION
• Complex pathway• Ciliary processes are site of aqueous
humour formation• Mainly by three machanisms1.Ultra filtration 20%2.Active transfer 70%3.Diffusion 10%

1.ULTRAFILTRATIONProcess thru which fluids and solutes cross
through semi permeable membCapillary blood flow 150ml/min4%filters thru fenestrationsFavoured by hydrostatic pressure diff b/w
capillary and interstitial pr. Enough to move fluid to stroma but further
req active transportLeads to formation of stromal pool

2.ACTIVE TRANSPORT
Energy dependentMajority production by active secretionUses ATPAA:Decreased by hypoxia, hypothermia
and inhibitors of active metabolism.
Majority of investigators proposed that active transport of sodium is key in aq humor formation

• Sodium-70% is actively transported by specific secretary pump. Rest by diffusion, ultrafiltration.
• Chloride-dependent on sodium• Ascorbic acid- secreted against large
concentration gradient.• Amino acids-By 3 carriers.• Bicarbonate-by carbonic anhydrase
mediated reaction.

3.DIFFUSIONActive Transport of substances described
above lead to osmotic and electrical gradient
To maintain the balance small partices like water and small plasma constituents move in to post chamber by diffusion

AQUEOUS OUTFLOW SYSTEM
• Consists of two pathways
1.Trabecular or conventional outflow2.Uveoscleral or unconventional outflow

UVEOSCLERAL OUTFLOW Pressure independent,10-25% 0.3microl/min and independent of IOP
CILIARY BODY
SUPRA CHOROIDAL SPACE
CILIARY BODY VENOUS CIRCULATION
CHOROID
SCLERA
ORBITAL TISSUE

INCREASE• Prostaglandins-one of most potent
IOP reducing agents• Cycloplegics• Alpha agonists-
epinephrine,brimonidine,apraclonidine
• Atropine
DECREASE• Pilocarpine

TRABECULAR OUTFLOW• Pressure dependent,90%
TRABECULAR MESHWORK
SCHEMMS CANAL
INTRASCLERAL CHANNELS
EPISCLERAL AND CONJUNCTIVAL VEINS
CAVERNOUS SINUS


TRABECULAR MESHWORK


Mech of aq transport through trab meshwork
• VACUOLATION THEORY:- vesicles and vacuoles in endothelium open and close intermittently to transport aqueous from TM cells to Schlemm’s canal
Non Vacuolate
d state
Early stage of
basal infolding
Macrovacuole formation
Vacuolar
transecellula
r chann
el formation
Oclusion of basal infolding
SCHLEMMS CANAL
• Endothelial lined oval channel present circumferentially in Scleral sulcus.
• Cells irregular spindle shaped & contain giant vacuoles.
• Outer wall contains openings of collector channels.
• Torus or lip like thickenings near collector channel help to keep canal open.
• AA: Gaint vacuoles are lost with increasing age and this is implicated in POAG.


COLLECTOR CHANNELS• 25-30 intrascleral aqueous vessels• Valveless,wide at origin• Direct system• Indirect systemEPISCLERAL VEINS• drain ultimately in to cavernous sinus
via ant ciliary and sup ophthalmic veins

DIFFERENT MECHANISMS OF OUTFLOW OBSTRUCTION
• POAG - loss of trabecular endothelial cells. - collapse of schlemms canal. - obstruction of collector channels.• Infantile glaucoma – outflow structures not
developed properly (Trabeculodysgenesis).• Angle closure glaucoma – peripheral iris
pushed against meshwork.• Secondary open angle – obstruction by
RBCs, WBCs, tumor cells , pigment & lens particles.

AQ HUMOR COMPOSITION
• Rate: 2.4+/-0.6 microL/min• Volume: 0.31ml( 0.25ml AC, 0.06ml
PC)• Refractive index: 1.336• Viscosity:1.025-1.040• Osmotic pressure: 3-5mosm/L• pH:Acidic,7.2 • Turnover: 1.5-2hrs

• Water -99.9%.• IgM & IgG ,but no IgA and IgD.• Plasminogen and its activators but no
other clotting factors.• Most important- low protein content (200
times less) and high ascorbate (20 times).ascorbate acts as anti oxidant and protects ocular structures from uv light induced oxidative damage
• Comparision b/w PC and AC aqueous bicorb and ascorbate pc>Ac chloride ac>pc
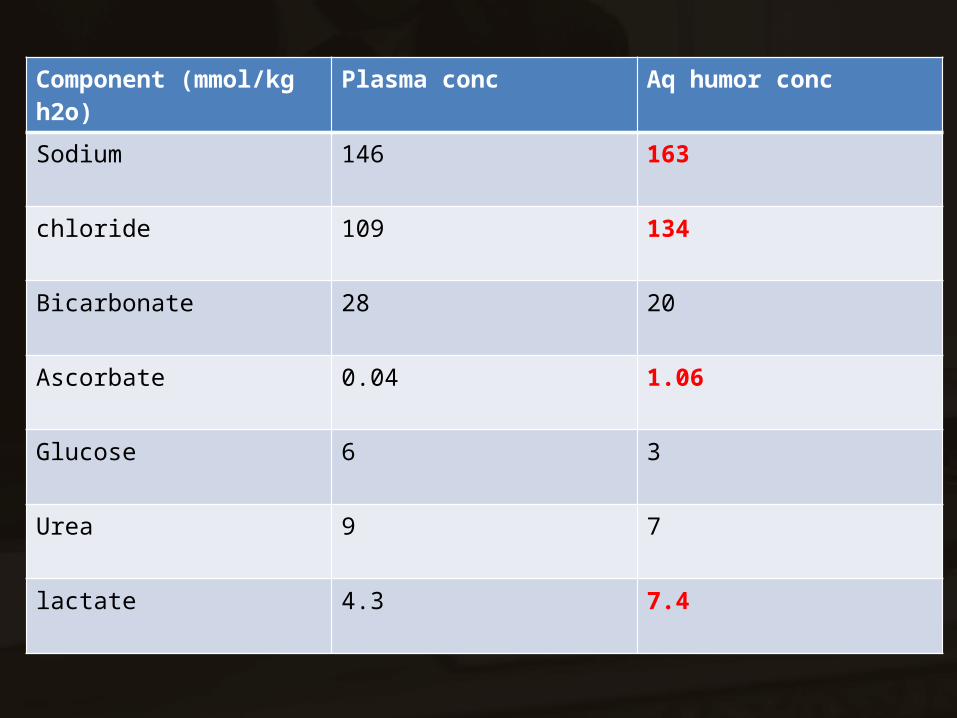
Component (mmol/kg h2o) Plasma conc Aq humor conc
Sodium 146 163
chloride 109 134
Bicarbonate 28 20
Ascorbate 0.04 1.06
Glucose 6 3
Urea 9 7
lactate 4.3 7.4

BLOOD AQUEOUS BARRIER
• The tight junctions connecting the apical portions of adjacent non pigmented epithelial cells forms the blood aqueous barrier.
• Responsible for maintaining the difference in chemical composition b/w aq and plasma
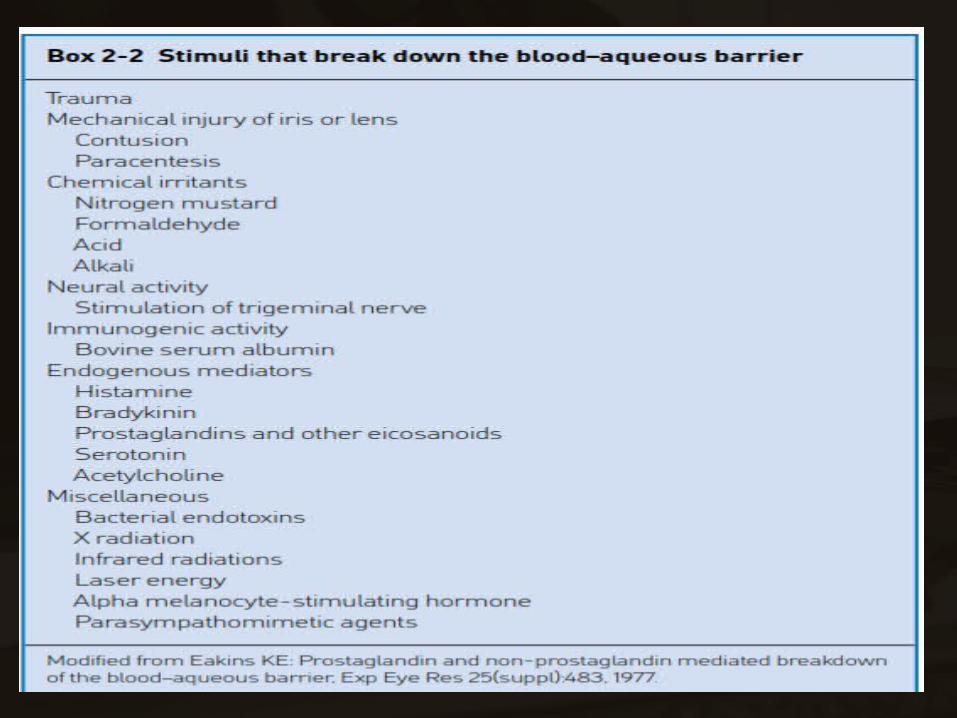

Break down• Proteins appear in aqueous humor: Plasmoid (Secondary )aqueous On SLE-Pronounced Tyndall beam >20mg / 100 ml ,phenomenon of FLARE.• Fibrinogen enters- clotting of aqueous.• INFECTIONS-brings mediators of cellular and
humoral immunity• UVEITIS AND TRAUMA-dev of cataract and
synechiae formation
AA: Rate of penetration of PAH, fluorescein, Evan’s blue increases-Diagnostic indicator.

FACTORS AFFECTING AQ HUMOR FORMATION
• Avg is 2.6-2.8 micro lit/min• Diurnal variation : maximum in morning hours
& min late at night, due to decreased stimulation of ciliary epithelium by catecholamines during sleep.
• Age and sex: similar in males & females , reduces with age.
• Ocular inflammation ,hypothermia ,systemic acidosis & anesthetics like halothane , barbiturates & ketamine decrease formation.

• Blood flow to ciliary body: profound vasoconstriction decreases formation.
• Sympathetic system: stimulation by β2 & inhibition via α2 receptors.
• Parasympathetic system: decreases via M3 receptors.
• Intracelluar regulators: cyclic AMP increases aqueous formation.

MEASUREMENT OF AQUEOUS
FORMATIONPHYSICAL METHODS-pressure dependent
• -When fluid is introduced in to a closed system there is intermediate increase in pressure in the system
• Can be calc using goldmans equation F = C (Po - Pv) F- Rate of aqueous outflow (mmHg) C- Coefficient of outflow facility
(microL/min/mmHg) Po -Baseline IOP (mmHg) Pv- Episcleral venous pressure (mmHg)

By1.Tonography2.Suction cup3.Perfusion
tonography• Non-invasive technique• Schiotz tonometer placed on eye for 4min ,
raises IOP.• Rate of flow calculated based on rate of rise
of IOP.• Normal: 0.28microl/min/mmHg• Most glaucoma patients have values less
than 0.17microl/min/mmHg.

TRACER METHODS• Measures rate of appearance or
dissappearance of various tracers in ac
• Any aq passing posteriorly to vitreous and retina cannot be detected
-Photogrammetric estimation -Radiolabelled isotopes -Fluorescein technique -PAH technique

CLINICAL ASPECTS• CLINICAL CONDITIONS-hypothemia and systemic acidosis decreases aq production and vice versa-IDDM decrease aqueous outflow

• PHARMACOLOGICAL AGENTSINCREASE PRODUCTION-beta adrenergic agents-hydrocortisone adm systemically-intracameral ANP
DECREASED PRODUCTION-CA inhibitors-Beta blockers_ouabain-cyclodestructive procedures


